
Abstract
Introduction
Loneliness, which significantly impacts physical and mental health, quality of life, and longevity, is recognized as a global concern among older adults. Although home care services are generally viewed as beneficial, they may also fall short in addressing the psychosocial needs of older adults. This study aims to assess loneliness and its associations with well-being and personal characteristics in older adults in Lithuania receiving long-term home care services.
Methods
A cross-sectional quantitative study was conducted between September and November 2024. A translated version of validated scales of loneliness as well as sociodemographic and quality-of-life factors was administered to the homes of older (65 years or older) participants receiving home care services. The chi-square test was used to determine the dependence of the attributes. Spearman's rank correlation coefficient (rs) was used to assess the associations between variables.
Results
Of the 111 participants, 56.8% did not feel lonely, and 43.2% reported feeling lonely. The results revealed no statistically significant differences between loneliness and gender, age, or educational level. However, there was a significant difference between loneliness and living situation (p = .003), restricted physical activity (p = .028), difficulty meeting daily needs (p = .005), and negative emotional well-being (p < .05).
Conclusions
The main and most common indicators of loneliness were living situation and quality of life. Taken together, the results highlight that loneliness is a multifaceted issue involving physical, social, and emotional factors. Addressing loneliness in older adults requires not only meeting physical needs but also providing meaningful social support within home-based services.
Introduction
Loneliness is recognized as a global concern among older adults (Tomstad et al., 2021). Approximately one in four older adults experience loneliness or social isolation, both of which significantly impact physical and mental health, quality of life, and longevity (World Health Organization [WHO], 2021). Thus, among the aims of the United Nations Decade of Healthy Aging (2021–2030) are increased political awareness of the issue of loneliness, promotion of research in this field, and encouragement of the implementation of effective interventions (WHO, 2020). Objective indicators of social isolation include a lack of support from one's social network and a lack of social interactions. In contrast, loneliness is a subjective experience that represents a distinction between desired and actual social relationships, regardless of the number of social connections (Veazie et al., 2019). These distinctions are especially important in Lithuania, where the population is aging rapidly and a growing proportion of senior citizens require long-term care. Home-based services, which help older people in maintaining their independence, have become an essential component of care delivery in this setting with the backing of social and health institutions.
Review of Literature
Both social isolation (an objective lack of social contacts) and loneliness (a subjective perception of inadequate social relationships) have been associated with a range of adverse health outcomes, including stroke, cardiovascular disease, dementia, anxiety disorders, and suicidal thoughts (Qiao et al., 2022; Sharma et al., 2021; Valtorta et al., 2016; WHO, 2021). Individuals with mobility impairments, difficulties performing activities of daily living (ADL), or sensory impairments such as vision and hearing loss are at increased risk of experiencing loneliness (Gyasi et al., 2022; Tomstad et al., 2021; Zhang et al., 2023). Loneliness and physical health changes among older adults are closely connected and mutually influential. Research shows that loneliness and social isolation increase the risk of mortality related to health problems and contribute to a decline in functional ability (Nakou et al., 2025; Perissinotto et al., 2012). Physical health changes, such as frailty or limited mobility, can lead to feelings of loneliness and social isolation, while loneliness, in turn, increases the likelihood of physical frailty (Kojima et al., 2022). Therefore, social isolation and loneliness have a profound impact on overall quality of life (Beridze et al., 2020). Research indicates that engaging in basic activities such as playing card games, watching TV, or listening to the radio can significantly reduce feelings of loneliness (Teh & Tey, 2019). Encouraging older people to participate in social activities and expand their social networks is equally important for reducing social isolation (Reiner & Steinhoff, 2024). Additionally, social isolation and loneliness can be decreased by promoting emotional well-being, and the risk is increased by signs of anxiety or depression, sadness, exhaustion, or trouble sleeping (Liu et al., 2024).
Global demographic shifts are increasing the need for long-term care services (European Commission, Directorate-General for Economic and Financial Affairs, 2018). Home care is a more sustainable solution in the context of a growing older population and the limited capacity of institutional care to meet all needs (Young et al., 2017; Wang et al., 2022). Moreover, home-based services tend to be emotionally closer and more familiar to older adults than hospital-based services are, making home care a more favorable environment for addressing the issue of loneliness (Haex et al., 2019). The type and frequency of care provided also influence an individual's social well-being. The services that have the greatest impact on reducing loneliness are those that include not only personal and medical care but also social and community-based support; therefore, home- and community-based services are more favorable for older adults than home care services alone (Sun & Shen, 2023; Zhang et al., 2023). Services that are provided regularly and for longer than 3 months have a greater positive impact on reducing loneliness (Chua et al., 2023; Kadowaki et al., 2014).
In Lithuania, home care refers to nursing and social services provided at the individual's home by multidisciplinary teams, including nurses, nurse assistants, social workers, physiotherapists, and occupational therapists, to address assessed health, functional, emotional, and social needs. These services, which are offered daily based on each person's needs, became first available nationwide in 2021. They focus on professional healthcare and social support but do not include household help. According to Order No. V-1026 of the Minister of Health of the Republic of Lithuania, home-based outpatient care services are delivered by healthcare institution specialists and include assessment, treatment, and care procedures performed in the patient's home. These services are financed by the Compulsory Health Insurance Fund if the patient is insured and has a referral from a family physician (Lithuanian Ministry of Health, 2007).
Although home care services are generally viewed as beneficial, they may also fall short in addressing the psychosocial needs of older adults (Bölenius et al., 2017). Individuals receiving home care often report feeling lonely and socially isolated (Pollak et al., 2025). This is partly because home care tends to focus on persons’ physical and functional needs, whereas psychosocial aspects receive comparatively less attention (Bölenius et al., 2017; Tomstad et al., 2021). High caseloads and limited time for each visit further constrain home care professionals’ ability to provide holistic care that includes psychosocial support (Ernsth Bravell et al., 2020). Older adults often use home care visits as opportunities to discuss not only health problems but also memories, social issues, and personal values. This reflects a desire to extend the conversation with health professionals and alleviate feelings of loneliness (Hafskjold et al., 2016). In this context, home care nurses play a crucial role in reducing loneliness among older adults living at home by prioritizing social engagement and addressing their social needs (Tomstad et al., 2021). Given that home-based healthcare is often long-term, it is essential for healthcare professionals to maintain effective communication and regular contact to build trust and support well-being (Gan et al., 2015).
Identifying loneliness in older adults is critical, as social isolation and loneliness have a profound impact on overall quality of life. Understanding the key factors that contribute to loneliness can help tailor services that are more responsive to an individual's needs. Such insights are essential for ensuring high-quality, holistic care that addresses not only physical and emotional needs but also social and spiritual needs.
Over the next 5–15 years, Lithuania's older adult population is expected to increase significantly as more baby boomers reach retirement age (Economic Policy Committee – Ageing Working Group, 2023). Even with the existence of professional home care services and social safety nets, family assistance is still an important part of older people's everyday life. The majority of older individuals depend on friends, family, neighbors, and volunteers for support due to strong family care traditions (WHO, Regional Office for Europe, 2024). In addition to family care, medical professionals are gradually taking over caregiving responsibilities due to the recently implemented home care services (which have been in place since 2021) (Organisation for Economic Co-operation and Development [OECD], 2022). The significance of examining loneliness and well-being among the nation's older adults receiving long-term home care is made clear by these contextual factors.
The aim of this study was to assess loneliness and its relationships to well-being and personal characteristics in older adults in Lithuania who were receiving long-term home care services.
Method
Study Design
A cross-sectional quantitative research design was employed in meeting the study aims with older adults from the family medicine clinic of a large hospital in Lithuania. This clinic was selected as the study site because a home care unit was established there in 2021, following the implementation of national legislation requiring each primary health care center to either establish its own home care unit or partner with an existing one (Lithuanian Ministry of Health, 2007). The legislation also mandated that home care services should be provided by a dedicated team of professionals – such as nurses, nurse assistants, and physiotherapists – rather than by health workers who normally work with family doctors.
Data were collected through the outpatient home care unit, with assessments carried out in the homes of older adults receiving care. At the time of the study, the outpatient home care unit served 333 individuals. This research is part of a larger regional study titled “Analysis of the impact of integrated long-term care at home methods on the health and well-being of older adults.”
Participants
The study targeted older adults (65 years and older) receiving long-term home care services. Multidisciplinary teams provide nursing and social support at home as part of home care services, which meet patients’ physical, functional, and psychological requirements (OECD, 2022). In Lithuania, those 65 and older are considered to be as older adults, which is in line with global demographic and health research standards (OECD, 2023). Eligible individuals were identified on the basis of specific inclusion criteria:
Receipt of long-term care services at home. The classification of low, medium, or high nursing needs as determined by the Nursing Needs Assessment Questionnaire (Lithuanian Ministry of Health, 2007). In addition to confirming study eligibility, the home care team used this tool to assess participants’ care needs at the beginning of receiving home care services. This questionnaire was neither scored or evaluated by the researchers themselves. This tool scores care needs on a scale from 0 to 93 points: 0–19 points: No need for outpatient home care services 20–33 points: Low need 34–49 points: Medium need 50+ points: High need Age 65 or older.
The exclusion criteria included individuals undergoing active medical treatments (e.g., chemotherapy or recent surgery), those residing in institutional care facilities, those receiving palliative care, adults with dementia or other cognitive impairments that would affect their ability to understand the questions in the questionnaire, and incapacitated adults.
Among the 333 individuals receiving home care services, 111 met the inclusion criteria and participated in the study. Out of 333, 134 were not included because they had not received services in the past year due to improved health or other reasons. Additionally, 20 individuals did not meet the specified age criteria (older than 65 years), 19 were hospitalized at the time of the study, 27 were unable to participate due to dementia or other illnesses, and 22 refused to participate. All 111 participants who met the inclusion criteria were included in the final analytical sample, as the questionnaires were completed with the researcher present, resulting in no missing data.
Data Collection
Data collection was conducted by the lead researcher, who also works directly with individuals receiving home care. Each potential participant was contacted in advance by phone and informed about the opportunity to take part in the study. During the home visit, the researcher verbally explained the study details and provided written informed consent.
The quantitative survey was administered in person by the researcher, who recorded responses and monitored participants’ engagement during questionnaire administration and offered short breaks if needed. This approach was chosen to accommodate participants who required clarification or repetition of certain questions. Additionally, in-person administration was chosen over telephone interviews, as it is important to assess the participants’ actual health status during the survey.
The questionnaire took approximately 30 min to complete and did not interfere with the participants’ normal activities or care services. As the questionnaire was carried out in the participants’ own homes, care was taken to create a nonthreatening atmosphere and to preserve privacy by keeping all personal identifying information (e.g., name, address, contact details) separate from the questionnaire data, ensuring anonymity. The study's data collection period took place between September and November 2024, with a total of 111 older adults receiving home care completing the questionnaires, which were deemed valid and included in the final analysis.
Research Instrument
This study is part of a larger regional project titled “Analysis of the impact of integrated long-term care at home methods on the health and well-being of older adults,” which uses the ICHOM toolkit, generally including both clinical and patient-reported data, as well as multiple questionnaires (Akpan et al., 2018; International Consortium for Health Outcomes Measurement [ICHOM], 2023). Only three patient-reported questionnaires were used in this analysis: the University of California, Los Angeles (UCLA) three-Item Loneliness Scale (Hughes et al., 2004), the Medical Outcomes Study: 36-Item Short Form Survey Instrument Version 1 (SF-36) (RAND Corporation, 1992) and the Canadian Study on Health & Aging Clinical Frailty Scale (Rockwood et al., 2005). Sociodemographic information was also collected including gender, age, living situation, and level of education. Participants were categorized into two groups according to educational level: low education (up to higher education – primary/secondary/vocational) or high education (holding a university degree). Regarding living situation, “living with others” refers to living with a spouse, other family members (children, grandchildren, siblings), or close relatives (e.g., daughter-in-law), based on the living arrangements observed in this study. This analysis does not include other clinical or project-wide data that were gathered as part of the bigger project.
With the authors’ consent, the questionnaires were linguistically adapted from English to Lithuanian in accordance with the International Society for Pharmacoeconomics and Outcomes Research (ISPOR) principles of good practice, as outlined in the ICHOM Guide to Data Collection in Older Adults, “The Cross-Cultural Adaptation Process for Patient-Reported Outcome Measures” (Hughes et al., 2004; ICHOM, 2023). The original translation was translated from English into Lithuanian. Back-translation into English was then performed to detect inconsistencies and ensure accuracy. The adapted Lithuanian version was pilot tested with older adults to assess comprehensibility and alignment with the original questionnaire. The comparison revealed no differences between the original version and the translated versions, indicating that the questionnaires were appropriately adapted to the Lithuanian context.
Loneliness was measured using the UCLA three-Item Loneliness Scale (Hughes et al., 2004). The three items on the scale ask about how often one feels alone, excluded, and lacks companionship. Each item is rated on a three-point scale: “almost never” (1) “some of the time” (2), and “often” (3). The responses are summed up to produce an original total score ranging from 3 to 9, with higher scores indicating greater loneliness. For the purposes of this study, and to improve interpretability in the descriptive analyses, the original total scores (3–9) were re-coded to a 0–6 range by subtracting 3 from each participant's score. Based on this re-coded scale, loneliness was dichotomized as follows: 0–2 = not lonely, 3–6 = lonely. This dichotomization was used only for descriptive and group comparisons, while the continuous re-coded score (0–6) was used in all bivariate correlations to maintain the entire variability of the measure. The UCLA three-Item Scale is a viable measure for evaluating loneliness in older people and has demonstrated acceptable reliability (Cronbach's α = 0.72).
Health-related quality of life was assessed using Medical Outcomes Study: The 36-item Short Form Survey Instrument Version 1 (SF-36). Physical functioning, role limits caused by physical health, bodily pain, general health, vitality, social functioning, role limitations due to emotional difficulties, and mental health are the eight areas covered by the 36 items in this popular standardized test. Higher scores indicate better health condition, and scores are converted to a 0–100 scale (RAND Corporation, 1992). The majority of the SF-36's domains demonstrate strong internal consistency (Cronbach's α > 0.80), making it a dependable instrument for older individuals.
Frailty was measured using the Canadian Study on Health & Aging's Clinical Frailty Scale (CFS) (Rockwood et al., 2005). The CFS uses a 9-point rating system, with 1 indicating very fit and 9 indicating terminally ill, based on a clinical assessment of the person's functional condition and degree of dependence. Since none of the participants in this study were identified as level 1 or 9, they were grouped into levels 2–8. The CFS demonstrates strong predictive validity and inter-rater reliability for adverse results like hospitalization and mortality.
Ethical Consideration
The study obtained ethical approval in compliance with ethical standards and national regulations. Participation in the study was entirely voluntary. The study protocol ensured that individuals were fully informed about the study, its duration, and the importance of their participation. All information was provided in an informed consent form to be signed by the participants. As the study took place in the participants’ homes, all personal data were kept separate from the questionnaire data, which were coded to ensure anonymity. All the data collected were handled securely, in strict compliance with ethical guidelines and data protection rules.
Statistical Analysis
The survey data were analyzed via the Statistical Package for Social Sciences (SPSS for Windows 30.0) (IBM Corp., 2023). The study data are presented as absolute (n) and percentage frequencies (%) or means ± standard deviations. Nonparametric methods of analysis were used to compare variables. Correlation tables were constructed to assess the relationships between attributes, and the chi-square criterion was used to determine the dependence of the attributes. Spearman's rank correlation coefficient (rs) was chosen to assess the relationships between loneliness and other variables among older adults. Since the main goal of the study was to look into correlations between certain pairs of variables, bivariate tests were used for the analysis. This kind of test makes it possible to clearly and immediately illustrate the key relationships that are most relevant to the research problem. The chosen level of statistical significance was set at p < .05.
Results
A total of 111 participants receiving care at home took part in the study. Approximately three-quarters were women, four-fifths were over the age of 80, and 40% of the participants lived alone. Table 1 shows the characteristics of the participants.
Characteristics of the Participants.

More than half of the participants were identified as having a medium level of care needs. The participants’ physical capacity is reflected in the Clinical Frailty Scale. The highest proportion corresponds to level 6, indicating that the individuals live with a moderate level of frailty, requiring assistance with activities inside and outside the home. At home, they often need help with climbing stairs and bathing and may need minimal help (reminders, support) while being dressed.
Statistical analysis was carried out to investigate the loneliness of older adults and revealed that 56.8% of the adults did not feel lonely and that 43.2% reported feeling lonely. Perceived loneliness was compared with sociodemographic factors, such as gender, age, educational level, and living situation (Table 2). There were no significant differences between loneliness and gender, age, or educational level; however, there was a significant difference between loneliness and living situation.
Relationships Between Loneliness and Sociodemographic Factors.

Note. p < .05 indicates statistical significance.
The association between loneliness and each of the following wellbeing factors was examined using Spearman's rank correlations: physical wellbeing (physical activity, meeting daily needs), social factors (socialization, living situation), and negative emotional wellbeing (mental health: exhaustion, fatigue, sadness; physical health: lack of strength and energy; mood-anxiety: restlessness, irritability, nervousness, depression) (Table 3).
Associations Between Loneliness and Emotional and Physical Wellbeing and Social Factors.
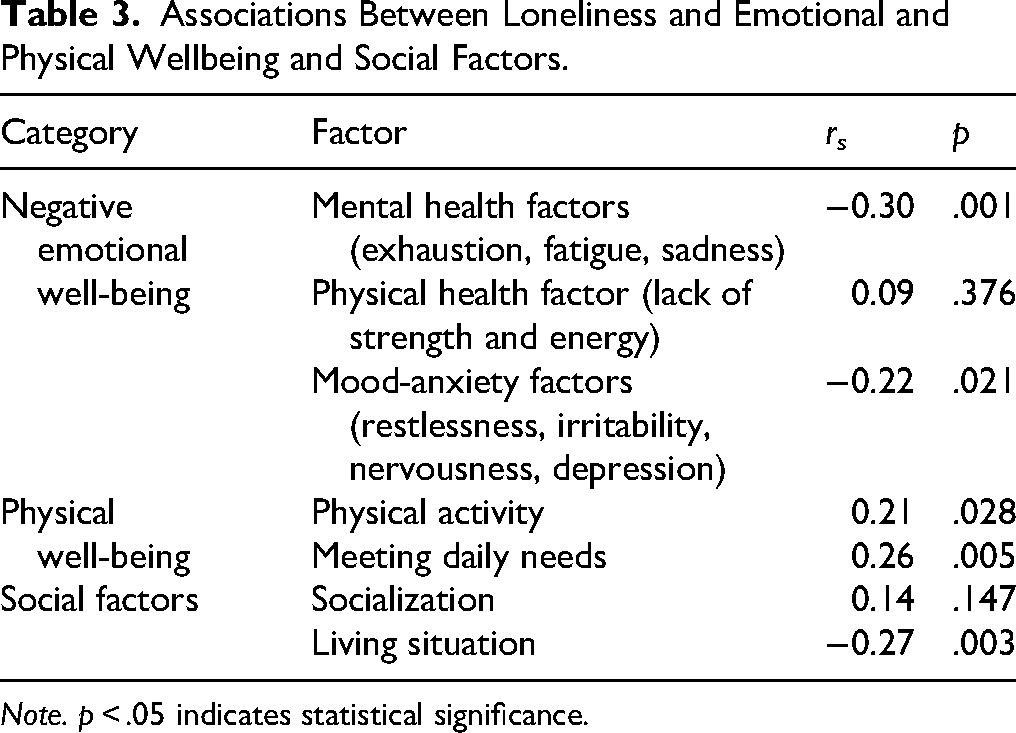
Note. p < .05 indicates statistical significance.
Higher scores on mood-anxiety variables (rs = −0.22, p < .05) and mental health factors (rs = −0.30, p < .01) were linked to higher levels of loneliness, according to Spearman's correlations. Higher levels of loneliness were also associated with less physical activity (rs = 0.21, p < .05) and trouble satisfying daily needs (rs = 0.26, p < .01). Among social characteristics, socialization was not statistically significant (rs = 0.14, p = .147), while living alone was significantly associated with higher levels of loneliness (rs = −0.27, p < .01). Negative correlations reveal that higher factor scores are linked to higher levels of loneliness, and higher scores suggest greater negative influence on mental, physical, or mood-anxiety related well-being.
Discussion
This study, which explored loneliness among community-residing older adults receiving home care services, identified key factors associated with loneliness. While home care services are important for meeting the physical and psychological needs of older adults, they often prioritize the assessment of clinical complaints, inadvertently overlooking a significant issue: loneliness (Zhang et al., 2023). Recent research among home-care professionals suggests that meeting social needs and promoting social involvement through home care visits might reduce loneliness and increase overall wellbeing (Nordin et al., 2023).
Older adults generally view home care services positively and regard home visits as an opportunity for social interaction. However, these visits alone are insufficient to fully address their social needs. Although home care services provide essential health-related support, they do not adequately meet the emotional needs associated with loneliness (Hemberg et al., 2018). Previous studies have additionally highlighted that while delivering essential care, home visits often fail to fully address emotional needs; additionally, the quality and frequency of nurse interactions can increase feelings of loneliness (Niemann & Million, 2023; Sya'diyah et al., 2020).
Identifying loneliness and its underlying causes can be challenging. Nurses and other healthcare professionals often feel ill-equipped to manage the psychological dimensions of care, including loneliness and other emotional concerns (Hauger et al., 2025). Our results bring attention to certain factors linked to loneliness in older adults receiving home care. This highlights the necessity of focused training and support for nurses in order to properly meet their physical and psychological needs. These findings have significant effects on the nursing profession. Home-care nurses are often the first point of contact, and their responsibilities go beyond clinical assessment to include psychosocial support. Training in understanding and dealing with loneliness is critical. Nurses can identify early indicators of social and emotional discomfort and carry out interventions such as promoting social interaction or organizing multidisciplinary assistance. Qualitative research among home-care nurses highlighted loneliness as a complex need commonly ignored in everyday care. Many nurses feel they lack suitable tools and organizational support to address this issue (Tomstad et al., 2021). Strengthening nurses’ competencies in this area may result in better holistic care and overall quality of life for older people. Systematic reviews and quality improvement projects show that structured interventions, including social engagement programs and coordinated multidisciplinary support, can reduce loneliness among older adults receiving home care (Dove et al., 2022; Sepúlveda-Loyola et al., 2020).
Sociodemographic Factors
This study revealed that sociodemographic factors, which are often considered influential, did not have a significant effect on loneliness among older adults receiving home care. While previous research has examined gender differences in experiences of loneliness, the findings remain mixed. Some studies suggest that women may report higher levels of loneliness due to greater emotional openness, a need for more social contact (Boehlen et al., 2023; Zhou & Wu, 2023), or because of their longer life expectancy and increased likelihood of widowhood (Yu et al., 2024). However, other research suggests that loneliness does not consistently differ by gender; rather, individual personality traits and communication styles may play a more critical role (Lin et al., 2021; Parlapani et al., 2020). A study conducted in Spain also explored the associations of loneliness with sociodemographic factors. Although no significant associations were found between gender and emotional loneliness, the authors concluded that women who were single or widowed and did not have children were more likely to report social loneliness (Ibáñez-Del Valle et al., 2022).
In the present study, while most sociodemographic indicators were not significantly associated with loneliness, one factor, living situation, emerged as particularly important. Living alone, especially in the absence of a close family, is linked to a greater sense of loneliness. Nevertheless, this relationship is nuanced; some older adults living alone do not experience loneliness, which may be related to engaging in meaningful activities. This study concentrated on perceived loneliness, which reflects the subjective sense of unmet social needs, despite the fact that loneliness and social isolation are associated. As in findings from other countries, maintaining an active social network remains one of the most effective strategies for preventing loneliness among older adults living alone. In contrast, other factors, such as income, level of education, or health status, were not found to influence feelings of loneliness (Zebhauser et al., 2014).
Quality of Life Factors
Limiting physical activity due to health problems is closely associated with perceived loneliness and may relate to reduced quality of life. This study revealed that greater restrictions in physical activity, such as difficulty moving around, walking outdoors, bending, or climbing stairs, were correlated with higher levels of loneliness. In addition, reduced physical activity interferes with the ability to perform daily tasks such as daily hygiene, bathing, cooking, and housekeeping.
These results suggest that loneliness is not only influenced by social and emotional factors but is also linked to health factors. Other studies have shown that lower physical activity is more strongly associated with social isolation than loneliness is. When older adults’ activity levels decrease, they are inherently socially isolated (Schrempft et al., 2019). Another study also supports this connection, indicating that mobility impairments are strongly associated with feelings of loneliness. These feelings reflect a broader sense of loss associated with aging, particularly the loss of independence associated with physical decline (Moeyersons et al., 2022). A recent study of older adults receiving home-based care showed the link between frailty and loneliness. Frail patients had significantly greater loneliness levels than robust ones (Klesiora et al., 2024). These findings highlight the importance of nurses coordinating interdisciplinary support, involving other specialists such as physiotherapists, to address physical activity limitations and frailty that contribute to loneliness. It may enhance holistic wellbeing and reduce feelings of loneliness among home-care recipients.
Negative Emotional Well-Being Factor
Loneliness is clearly strongly linked to both social factors and overall quality of life, particularly physical health. However, emotional health remains another very important aspect. This study revealed a strong association between negative emotional well-being and increased feelings of loneliness. The key emotional indicators identified in this study were exhaustion, fatigue, sadness, restlessness, irritability, nervousness, and depression.
The connection between loneliness among older adults and mental health is well documented. Loneliness has a direct effect on mental health, exacerbating emotions such as anxiety or depression that contribute to long-term mental health concerns (Trybusińska & Saracen, 2019). This was the case during the COVID-19 pandemic, when prolonged social isolation negatively affected the psychological state of older adults (Sepúlveda-Loyola et al., 2020; Dove et al., 2022). A Swedish study found that home-care recipients had increased loneliness and anxiety during the COVID-19 pandemic, emphasizing the significance of integrating psychosocial support into home care (Johansson-Pajala et al., 2022). However, these issues persist after the pandemic, as older adults continue to face loneliness and social isolation.
Contextual Considerations
When interpreting these findings, the Lithuanian context should be taken into account. Strong family care traditions mean that many older people still rely on family members for daily help, but recent policy changes and demographic changes – like the introduction of formal home care services in 2021 – are gradually changing the way care is delivered. This transitional period may affect how loneliness is felt as the growing significance of professional care combines with reliance on family support. Therefore, this study provides important insights into the psychosocial needs of older adults in a country where formal home care is still developing.
Our findings, which are based on data gathered at a specific point in time, show correlations between variables rather than causes. Contextual factors, such as the relatively recent introduction of home care services in Lithuania and cultural or demographic characteristics, particularly family structures, may have an impact on some of the differences between our results and those reported in other studies. Variations in findings may also result from differences in home care delivery in other countries, since the type, frequency, and focus of services might influence older individuals’ feelings of loneliness and social support.
Strengths and Limitations
One of the key strengths of this study is the selection of a specific group of participants – older adults receiving home care services. Since each individual was visited personally, it was possible to assess their actual situation. This is particularly important in the Lithuanian context, as very few studies have been conducted in this field.
Although the study yielded significant results, it also has certain limitations. It was carried out in only one institution in Lithuania, and some older adults receiving services in this facility did not participate in the study because of their health status. Thus, the study findings may not be representative of the whole population of older adults receiving home care services. The study's small sample size was another limitation, as it precluded the use of multivariable models with any degree of reliability. Bivariate tests were therefore used in the analysis. Multivariable models should be used in future research with a bigger sample size to account for any confounding factors and produce more comprehensible findings.
Implications for Practice
The results of this study emphasize that when providing home services to older adults, it is important to address not only physical but also psychosocial needs. Psychosocial issues are often overlooked or inadequately identified. To tackle this practical problem, service integration is necessary, involving social workers and/or psychologists. Since these services in Lithuania are new and still evolving, attention should be paid to team composition and interprofessional collaboration. This is important not only for primary health care centers providing these services but also for policy makers. Crucially, this study shows in an original manner how loneliness among older individuals in Lithuania who are receiving recently introduced home care services is related to living situation, physical ability, and specific aspects of emotional well-being. These findings are also relevant in the international context, as they can help other countries understand how newly implemented home care models may affect the well-being and feelings of loneliness among older adults. From a nursing point of view, this study emphasizes the significance of integrating psychosocial assessments into routine home visits. Nurses should be provided with resources and instruction on how to recognize loneliness and provide or coordinate appropriate interventions, such as promoting social activity, connecting people with community services, or consulting mental health professionals. Policies that support nurses’ increased roles in addressing psychological issues may improve the effectiveness of home care services and enhance the well-being of older adults.
Conclusions
The findings of this study provide valuable insights into one of the most important issues facing older adults: loneliness. While sociodemographic factors are often assumed to influence loneliness, this study revealed that they have little impact. The main and most common factor for loneliness is the living situation, where the person spends time alone, not only emotionally but also physically. The strongest associations were found between loneliness and quality-of-life factors. A decrease in physical health that limits activity and the ability to perform daily tasks is associated with greater feelings of loneliness. These limitations affect not only daily activities but also quality of life. In addition to physical and social dimensions, emotional well-being is also important. Feelings such as exhaustion, sadness, anxiety, or depression are associated with a greater sense of loneliness.
Taken together, the results highlight that loneliness is a multifaceted issue involving physical, social, and emotional factors. Addressing loneliness in older adults requires not only meeting physical needs but also providing meaningful social support within home-based services. Interventions in home care services are therefore crucial for improving the overall quality of life of older adults by increasing their daily functioning, promoting physical activity, and maintaining emotional well-being.
Footnotes
Acknowledgment
We extend our gratitude to all who participated in the study and to the team that helped collect the data.
Ethics Approval and Informed Consent Statements
All ethical principles were respected in the conduct of the study. The participants were provided with an informed consent form, verbal and written explanations of the importance of the study, and the possibility of withdrawing at any time. All information was provided in an informed consent form to be signed by the participants. Ethical permission was granted by the Kaunas Regional Committee on Biomedical Research Ethics (bioethics authorization number of this study: P1-BE-2-55/2024).
Author Contributions
Arūnė Česonienė: conceptualization, data curation, formal analysis, investigation, methodology, visualization, and writing–original draft. Lina Jaruševičienė: validation, data curation, and writing–review and editing. Elizabeth A. Capezuti: writing–review and editing. Aurelija Blaževičienė: conceptualization, methodology, supervision, validation, and writing–review and editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.