
Abstract
The aim of this study was to examine the relationship between hydration status as measured by salivary osmolality and personal hydration habits, selected demographic characteristics, and performance on a walking and balance test in older community-dwelling adults. This study used a descriptive observational design in a convenience sample of multiethnic, community-dwelling older adults (N = 53). We collected saliva for analysis on 3 days both in the morning and early afternoon, along with a hydration habit questionnaire, get up and go test and demographic information. An exploratory factor analysis of the hydration habit questionnaire revealed a two-factor solution including physical barriers and psychological barriers to drinking fluids. A linear mixed-model approach revealed that time of day (p < .01), race (p = .015), mobility (p < .01), and cognitive barriers (p = .023) are all significant predictors of salivary osmolality among noninstitutionalized seniors. There is also a significant interaction between psychological barriers to drinking fluids and time of day (p < .01). Average salivary osmolality was higher in this group of older adults than has been reported in younger adults. Controlling for all other variables, salivary osmolality is higher in the morning than in the afternoon, lower among Black or African American seniors than among White or Caucasian seniors, and higher among seniors with decreased mobility. An interaction between psychological barriers and salivary osmolality showed that those participants with more psychological barriers to drinking had higher salivary osmolality in the morning and an inverse relationship in the afternoon.
Dehydration continues to be a costly, underappreciated precipitating, or comorbid condition leading to excess and prolonged hospitalizations for older adults. Although dehydration has been designated as one of 13 ambulatory-care sensitive conditions (Agency for Healthcare Research and Quality [AHRQ], 2004); it has resulted in a 5% increase in preventable emergency department visits in adults between 2008 and 2012 (Fingar, Barrett, Elixhauser, Stocks, & Steiner, 2015). Further, adults older than 65 years continue to have the highest rates of admissions for dehydration as a primary diagnosis, with those older than 75 years having the highest rates at 750 per 100,000 (AHRQ, 2015). The cost estimate for a primary diagnosis of dehydration is more than 1.14 billion dollars (Xiao, Barber, & Campbell, 2004) with secondary dehydration raising the cost of a hospitalization (Mentes & Aronow, 2016) suggesting that the cost of dehydration is underestimated.
Dehydration can have an acute onset, but an insidious onset usually associated with on-going failure of individuals to replace lost fluids is a more common presentation in older adults. Several population studies have shown that as one ages intake of all fluids including water decreases (Volkert, Kreuel, & Stehle, 2005; Zizza, Ellison, & Wernette, 2009), leaving the individual underhydrated. Some investigators term the precursor condition associated with insidious onset as mild-dehydration (Stookey, 2005), impending dehydration (Hooper et al., 2015), or chronic underhydration (Mentes, 2006; Mentes, Wakefield, & Culp, 2006) the term used in this investigation. It is estimated that as many as 40% of community-dwelling older individuals may be chronically underhydrated (Stookey, 2005; Stookey, Pieper, & Cohen, 2005) which can lead to dehydration with serious sequelae such as life threatening infections (Mentes & Aronow, 2016).
While there are multiple measures to approximate dehydration including biologic measures (serum: osmolality, BUN, creatinine, and sodium; urine: osmolality, specific gravity, and color), none serve as a gold standard. Further the measurement of dehydration is particularly difficult in older adults because of age-related changes in body composition and renal function. The measurement and clinical significance of chronic underhydration is even more difficult to capture; however, in order to prevent the often life-threatening complications of dehydration, it is important to explore. Each biologic measure has some limitations, for example, although serum indices are used most frequently, getting a serum specimen is invasive and the result is not helpful in detecting underhydration. In addition, while urine color and specific gravity have been studied as early indicators of underhydration in frail older adults (Mentes & Culp, 2003; Mentes et al., 2006), they are valid indicators only when renal function is adequate and a single value from these tests is difficult to interpret. Conversely, salivary osmolality, a noninvasive measure, has been shown to be a valid indicator of progressive dehydration, with values rising earlier than serum osmolality in younger populations (Oliver, Laing, Wilson, Bilzon, & Walsh, 2008). Although promising, the validity of salivary osmolality to detect water loss and water and solute loss dehydration with individuals in older age-groups requires further testing (Fortes et al., 2015; Mentes, 2008).
In addition to risk for dehydration, chronic underhydration may cause excess disability by contributing to functional impairment such as impaired mobility resulting in increased likelihood of falls. Because underhydration may not cause easily identifiable symptoms and older persons often do not pay attention to their fluid intake, noninvasive monitoring of hydration status may be beneficial in curbing dehydration episodes. Monitoring hydration status over time may be advantageous for self-management and early detection of changes in hydration status associated with chronic diseases including congestive heart failure, diabetes, and renal disease by providing an individual referent of hydration status for an older adult. Therefore, the purpose of this exploratory study is twofold: (a) To examine the relationship between hydration status as measured by salivary osmolality and personal hydration habits in a community-dwelling population of older adults and (b) to examine the relationship of hydration status as measured by salivary osmolality to hydration habits, selected demographic information, and performance on a walking and balance test in older community-dwelling adults.
Method
This observational study was designed to evaluate profiles of salivary osmolality as a measure of hydration status in a community-dwelling older adult population and characterize fluctuations in salivary osmolality in relationship to hydration habits. We also examined the relationship between functional performance and hydration status as measured by salivary osmolality averaged over 3 days. We received institutional review board approval from our university’s office of human research protection program and the three program directors of participating sites.
Setting and Participants
We recruited a convenience sample of 53 multiethnic community-dwelling older adults at two senior centers and one adult day care center throughout Los Angeles County, who are 65 years or older, can speak and read English or Farsi and who could give informed consent by a human subjects protocol. Exclusion criteria included being medically unstable; that is, hospitalized within the past month, unable to drink fluids, receiving dialysis, or terminally ill.
Measures
Demographic data and health characteristics collected included age, gender, marital status, ethnic background, medications, and medical diagnoses (comorbidities) were retrieved by self report or from the resident chart (available at adult day care center), using a structured review form used in previous studies. All written materials were translated into Farsi by a formal translation service experienced in medical or nursing terminology and were administered by a research assistant proficient in English and Farsi.
Salivary osmolality was measured using a freezing point depression salivary osmometer (Fiske Model 210 Micro-osmometer) to characterize fluctuations in hydration status. This device requires 100 μl of saliva, about the volume of a teardrop. The validity of the osmometer measurement has been strongly correlated with percent of loss of body water by weight in healthy young- to middle-aged subjects (Stewart, Reed, Zhong, Morton, & Porter, 2007).
Oral Hydration Habits
Participants’ hydration habits were classified based on answers to a hydration habit questionnaire developed from an oral hydration typology (Mentes, 2006). This questionnaire has face validity based on evaluation by two expert geriatric nurses. The first three categories of (a) “can drink” with subcategories, “independent” and “forgets” (b) “can’t drink” with subcategories of “physically dependent” and “dysphagic” and (c) “won’t drink” with subcategories of “sipper” and “fears incontinence” were the focus of this assessment.
Functional Performance
Functional performance was operationalized as the ability to attend and concentrate in order to accomplish the everyday task of ambulating safely and efficiently. Since decreased ability to attend to performance on a task has been demonstrated in younger persons who have mild dehydration (Armstrong et al., 2012; Ganio et al., 2011) and middle-aged persons who have participated in a hiking exercise (Ainslie et al., 2002); we wanted to use an age-appropriate measure to evaluate the effect that levels of hydration may have on functional performance of older adults. Therefore, for this variable, we used the Timed Get-up-and Go (TGUG) test which is a test used to screen older persons for ambulation and balance problems (Podsiadlo & Richardson, 1991). The material required for this test was an armless chair with a seat height of 46 cm, positioned at the edge of a walkway marked with electrical tape measuring 8 m long and with a turnaround area at the end. For this test, the participant must wear regular footwear and is given the following instructions: (a) Sit with your back against the chair and your arms in your lap, (b) on the word go stand, then walk at your normal pace to the end of the walkway, (c) turn around in the box at the end of the walkway, and (d) return to your chair and sit down (Wall, Bell, Campbell, & Davis, 2000). The test is considered normal if the participant completes it in ≤10 s, with > 20 s correlating with poor functional independence and higher risk of falls (Podsiadlo, & Richardson, 1991). We timed the test with the use of a smart phone stopwatch feature. We chose this physical performance test as an easy, not burdensome test that is likely to vary depending on the participant’s physical state and would be directly linked to the participant’s overall functional ability (Quan et al., 2017; Van Kan et al., 2009).
Procedure
After obtaining informed consent, trained research assistants collected two saliva (morning and early afternoon) specimens per day more than 3 days (total 6), asked participants to fill out a hydration habit profile, a brief health history form and complete a “get up and go test.” An unstimulated saliva specimen was required for the analysis, and the collection procedure was as follows: A participant must not have eaten for at least 30 min before specimen collection. She or he must be seated and first clear the mouth by swallowing all saliva one time, then sit quietly for 2 min to allow saliva to collect passively, not chewing, talking, or moving the jaw. After 2 min, the participant should tilt the head forward and use the straw provided or drool all saliva into the collecting vial for ∼ 5 s. Two specimens per day were collected, first as the participant arrived at the center and in the early afternoon. The saliva was transported to the university laboratory and tested by a trained research assistant for osmolality within an hour of collection using the freezing depression point osmometer (Fiske Model 210 Micro-osmometer).
Data Analysis
Data analyses were performed using SAS software, version 9.4 (SAS Institute, Cary, NC). For the first aim of the study to identify underlying determinants of elderly people’s oral hydration habits, an exploratory factor analysis was performed on the 11 variables corresponding to the hydration habits questionnaire in order to reveal any inherent clustering of related variables and to compare this latent variable structure to a newly developed typology of hydration habits among older adults. A promax rotation method was used to perform the factor analysis, which produced factor scores for each participant.
For the second aim of this investigation, a mixed-model approach was used to develop a model to examine the effect of the hydration habits factor scores, selected demographic factors, and get up and go scores on average salivary osmolality at the two specified time points.
Results
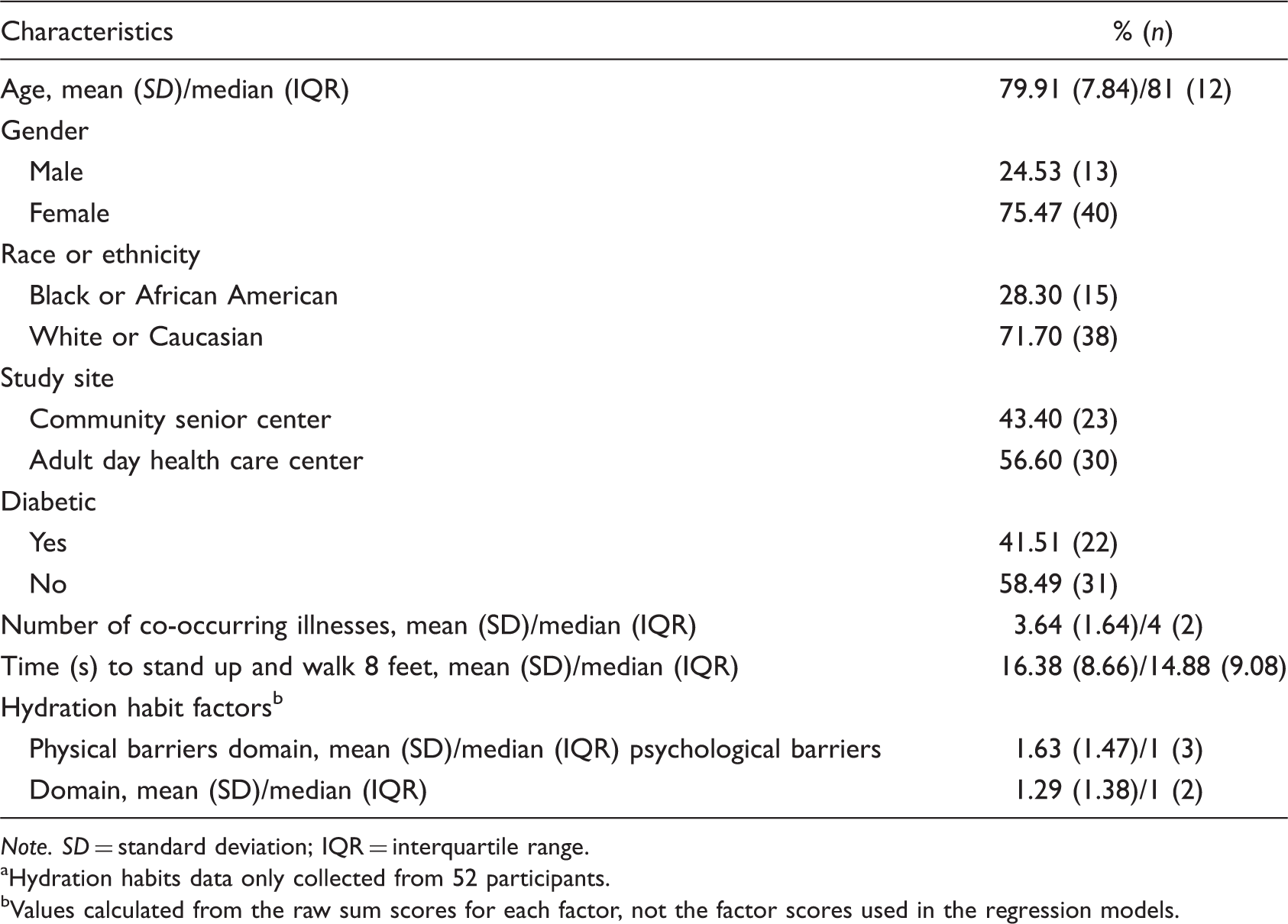
As shown in Table 1, the mean age of participants in the study was 79.91 years (SD = 7.84). Just more than 75% of the participants were female, and nearly 72% were White or Caucasian. More than half of the participants were recruited from a single adult day health care center, while 43% were recruited from two community senior centers. The mean number of co-occurring illnesses was 3.64 (SD = 1.64), and the mean or median time to stand and walk 8 feet was 16.38 s (SD = 8.7) and 14.88 s (interquartile range = 9.0), respectively. The average osmolality values for the participants in the morning was 143.6 mOsm/kg (SD = 65.8) and in the afternoon 125.3 mOsm/kg (SD = 56.8; Figure 1). Median values were 125 and 110.25 mOsm/kg, respectively.
Boxplot of salivary osmolality by time of day. Participant Demographics and Characteristics (N = 53a). Note. SD = standard deviation; IQR = interquartile range. Hydration habits data only collected from 52 participants. Values calculated from the raw sum scores for each factor, not the factor scores used in the regression models.
Factor Analysis
Summary of Exploratory Factor Analysis Results for Nine Hydration Habits Variables With Promax Rotation (N = 52).

Note. Factor loadings more than 0.30 appear in bold.
Since nearly all of the off-diagonal entries in the residual correlation matrix were less than or equal to 0.10, it approximates a null matrix, indicating that the two retained factors (psychological barriers and physical barriers) were sufficient to explain the correlations among the nine hydration habits variables included in the analysis.
These results from the exploratory factor analysis were well matched to Mentes’ (2006) developed typology of hydration problems in older adults. This typology categorizes the drinking behaviors of older patients into four categories: “can drink,” “can’t drink,” “won’t drink,” and “end of life.” For the purposes of this investigation, the first three categories were included in the factor analysis, with the “can’t drink” category represented by the physical barriers factor and the “won’t drink” category corresponding to the psychological barriers factor. The “can drink” factor of not knowing how much to drink was eliminated from the factor analysis because of small factor loadings.
Mixed-Model Analysis
Results From Mixed-Effects Model With Repeated Measures and Participants as Random Effects (N = 46).

Controlling for all other covariates in the model, salivary osmolality was 18.80 mOsm/kg higher in the morning, on average, than in the early afternoon. Figure 1 illustrates the relationship between salivary osmolality and time of day. All else held constant, salivary osmolality is 42.40 mOsm/kg lower among Black or African American participants, on average, than among White or Caucasian participants (Figure 2). Adjusting for the other covariates in the model, salivary osmolality increases by 2.39 mOsm/kg, on average, for each additional second, it takes an individual to stand and walk 8 feet.
Boxplot of salivary osmolality by race.
In the morning, a participant with more psychological barriers has, on average, higher salivary osmolality than a participant with fewer psychological barriers. In the afternoon, the direction of this relationship appears to change such that an individual with more psychological barriers has a lower salivary osmolality.
Discussion
Quantifying the effects of hydration status in older community-dwelling adults remains a daunting task. Clinicians need an accurate, noninvasive, quantitative measure with which to assess hydration in older adults. This effort includes using an appropriate biologic measure of hydration, such as salivary osmolality, while trying to account for individuals’ characteristics that include drinking behaviors. This study provides beginning evidence that the latent factors underlying the oral hydration habits of community-dwelling older adults include physical barriers, such as difficulty getting or drinking fluids, and psychological barriers, such as fear of incontinence, aversion to drinking fluids, or forgetting to drink. Examining older adults’ hydration habits offers a way for nurses to intervene to minimize underhydration and prevent dehydration.
What is striking about the salivary osmolality values in the morning is that half of the participants had values of 125 mOsm/kg or higher which was only slightly lower than the mean values that Fortes et al. (2015) found in older adult acute care patients with water and salt and water dehydration. The salivary osmolality values decreased with the afternoon values to a median value of 110.25 mOsm/kg. This suggests that many community-dwelling older adults are chronically underhydrated and are at risk for many poor outcomes such as medication side-effects, falls, increased susceptibility to infections to name a few. Given that the values are higher in the morning, issues of events such as early morning falls should be considered.
Concerning hydration barriers, it is interesting to note that it is the psychological barriers that are significantly related to increased salivary osmolality signaling poorer hydration status, rather than physical barriers. Since physical limitations for drinking are more visible, it is likely that the participant and his or her caregiver are sensitive to the need for assistance with drinking. Psychological barriers are more personal in nature and not as easily remedied; for example, older adults may be less likely to reveal to health-care providers that they are limiting fluid intake related to issues with urinary incontinence. The reversal of the relationship between salivary osmolality and psychological barriers in the afternoon is intriguing. Perhaps being in a social setting, such as a senior center or adult day health center provided an incentive for those individuals to drink given that drinking can be considered a social activity and those individuals who forget to drink maybe encouraged to drink by friends. In addition, for those who have concerns about incontinence, they would be in a known setting where access to toilet facilities would be easy.
Further, the results of this small study revealed that those community-dwelling older adults with a higher average salivary osmolality were more likely to take longer to perform the TGUG (mean was 16.88 s), where the normal value is ≤10 s, with >20 s correlating with poor functional independence and higher risk of falls (Podsiadlo & Richardson, 1991). Of the participants, 10 were able to complete the TGUG within the 10 s and 12 took longer than 20 s to complete with the remaining participants falling into the ambiguous area of completing the TGUG between 11 and 20 s. Taken together this suggests that older community-dwelling adults who have questionable hydration as evidenced by a higher salivary osmolality have more difficulty performing the TGUG test which could place them at risk for falls.
African American participants who attended a typical senior center comprised 28% of the sample, which is a fair representation of this ethnic group. The mixed-method analysis controlled for age, race, number of comorbidities, and function as measured by the get up and go test; therefore, the ethnic differences between Black or African American and White or Caucasian participants seen in the sample are particularly striking. In the limited literature on racial or ethnic differences available, Black or African American community-dwelling older adults were more likely to be hospitalized for dehydration than Caucasian older adults, independent of diuretic use (Lancaster, Smiciklas-Wright, Heller, Ahern, & Jensen, 2003). There is no literature on community-dwelling Black or African American older adults with respect to hydration status; in fact, most studies examining fluid intake in older adults have been conducted with Caucasian older adults (IOM, 2005; Volkert et al., 2005; Zizza et al., 2009). An explanation for these striking differences may be that a majority of the African American participants were recruited from one senior center.
Although a small observational study, the representation of community-dwelling older adults from an ethnic perspective is a strength of this project. Issues of missing saliva data are a known difficulty in conducting research with older adults, and although most participants were able to provide saliva specimens there were others who were unable. Together with the collection of repeated measurements over several days, the linear mixed-model technique was able to control for this missing data and we are reasonably sure that the resulting analysis is accurate.
Nursing Implications
Given the results of this study, nurses should monitor and encourage older adults to consume adequate amount of fluids throughout the day in order to promote optimal functioning of older adults. It would be important to educate the older adult to be particularly careful in the morning and to have a glass of water nearby to drink before starting the day. Many older adults restrict their fluids in the evening to prevent nocturnal incontinence or having to get up to the bathroom at night, and this leads to underhydration and may cause the older adult to fall. Family caregivers should be made aware of this possibility and educated on fall prevention. Further, educating family members about adequate intake spread throughout the day is also recommended. It could be helpful to assess personal hydration habits of older adults as psychological barriers to drinking can significantly affect their intake.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Gamma Tau Chapter, Sigma Theta Tau small grant program.