
Abstract
Introduction
The most common type of nosocomial infection among neonates on mechanical ventilation in neonatal intensive care units (NICUs) was ventilator-associated pneumonia (VAP). An Evidence-Based Practice Module for preventing VAP was highly recommended and crucial for enhancing nurses’ knowledge levels and improving their practices in this domain.
Objective
This study was designed to examine the impact of the Evidence-Based Practices Module on nurses’ knowledge and their practices for preventing VAP among high-risk neonates in NICUs.
Methods
This research employed a quasi-experimental (pre/post-test) design at two NICUs in Egypt—Banha Specialized Children's Hospital (Banha City) and Ain Shams University Hospital (Cairo)—to recruit a convenience sample (consisting of 200 male and female nurses) that served as a pre-/post-test group. The researchers employed three specific tools: a pre-test interview questionnaire (which was also utilized post-test), an Evidence-Based Practices Module for preventing VAP questionnaire, and an observational checklist concerning the nurse participants’ knowledge and practices in preventing VAP (pre- and post-demonstration of an Evidence-Based Practices Module).
Results
Participants’ general knowledge improved significantly with VAP (p < .001) across all areas evaluated: the participants’ performance improved markedly from a mean score of 9.010 ± 2.894 (pre-intervention) to 13.640 ± 1.285 (post-intervention) (t = −18.954, p < .001). Furthermore, the participants’ pre-intervention mean score for an Evidence-Based Practices Module (related to VAP prevention) was 9.300 ± 0.997, reflecting an almost total lack of knowledge; however, their post-intervention scores increased significantly to 17.745 ± 1.268. Additionally, their performances on an Evidence-Based Practices Module (related to VAP prevention) before intervention were 12.280 ± 3.143, which increased to 21.620 ± 1.615 post-intervention (t = −31.009, p < .001).
Conclusions
This study highlighted how the introduction of an Evidence-Based Practice Module positively impacted the nursing staff's knowledge and practices regarding the prevention of VAP in NICUs. It was recommended that the nursing staff implement the Ventilator-Associated Pneumonia Evidence-Based Practices Module to enhance their professional development, promote safe and proper practices, and improve the quality of care provided to high-risk neonates.
Introduction
Nosocomial infection, which can occur after 48 hours of a neonate being placed on a mechanical ventilator (MV), is a significant health problem associated with mechanical ventilation that has the potential to increase neonate mortality rates (Mohamed et al., 2023). Tracheal secretions, gastric fluid, and nasopharynx or oropharynx are the most common routes by which microorganisms can enter the lung; therefore, aspirating fluids contaminated into the lungs is a common cause of ventilator-associated pneumonia (VAP) (Osman et al., 2020).
VAP is the third most prevalent healthcare-associated infection among neonates in neonatal intensive care units (NICUs); therefore, updating healthcare providers’ knowledge concerning the incidence of VAP among neonates and methods of prevention is critical. In developed countries, the rate of VAP incidence is between 1.5 and 6 cases (per 1000 ventilators) per day; however, in developing countries, VAP incidence is between 17.2 and 90 cases (per 1000 ventilators) per day (Rangelova et al., 2024).
Literature Review
High-risk neonates who are hospitalized in NICUs are the most vulnerable demographic due to their susceptibility to a range of upper and lower respiratory tract infections, both of which contribute significantly to nosocomial infections (RM Abu-Elenen & BS Mehany, 2024). In recent decades, the utilization of MVs in NICUs has significantly enhanced the survival rates of newborns, particularly premature infants (Shivananda & Yashoda, 2021). While using a supportive MV in the intensive care unit (ICU) is a particularly humane approach, it is associated with several risks and complications, the most serious of which is pneumonia linked to the device. These complications had a substantial impact on the outcomes of critically ill newborns and staff (RM Abu-Elenen & BS Mehany, 2024). Typically, Associated Pneumonia linked with mechanical ventilation is classified as either early-onset (in the first 3 to 4 days of MV) or late-onset, a difference which is microbiologically necessary (Abad et al., 2021).
According to Rangelova et al. (2024), VAP is the third most common cause of increased morbidity and mortality rates among neonates on mechanical ventilation. Globally, there are between one and 73 cases of VAP (for every 1000 ventilators) per day in NICUs (Klompas et al., 2022; Rangelova et al., 2024). The low immunity of high-risk neonates, combined with their undeveloped lungs and prematurity, means that they may require mechanical ventilation for respiratory support. Nurses provide 24-h care for ventilated high-risk neonates at the NICU; therefore, adequate knowledge and practices regarding strategies of VAP prevention could contribute to decreasing the incidence of VAP. In Egypt, hospital infections (such as pneumonia, meningitis, and septicemia) among high-risk neonates account for 30% of deaths during the neonatal stage (Abou Zed & Mohammed, 2019). This study was designed to examine the potential knowledge level of nurses and their implementation of VAP preventative practices.
According to the Centers for Disease Control and Prevention (CDC) (2013), the risk factors for VAP include aspirating oropharyngeal secretions that may contain microorganisms, the extended use of ventilator support, contaminated ventilator equipment (such as ventilator tubing), the improper use of aseptic techniques by newly hired nurses, and inadequate oral hygiene (Abdel-Hamed et al., 2024). Bundled care, an approach which can be utilized by nursing staff responsible for infection control in NICUs, has been proven to minimize the ratio of nosocomial infections (such as pneumonia). When staff nurses follow the care bundle for every neonate, it has been established that the risk of VAP could be eliminated (Ali & Ahmed, 2023).
VAP is a serious healthcare-associated infection which can cause increased morbidity and mortality rates among neonates in NICUs (Ergenekon & Çataltepe, 2020). Additionally, it can result in extended periods of hospitalization for neonates while, according to Elsaeed et al. (2025), escalating the costs of healthcare. VAP is considered the most prevalent healthcare-associated sepsis in NICUs. Consequently, updating the nurses’ performances and knowledge regarding the incidence of newborn VAP is considered to be a critical preventative method (El-Sayed et al., 2023). After applying mechanical ventilation, neonates were found to be more susceptible to hospital-acquired pneumonia (which occurs more than 48 h after NICU hospitalization), which resulted in increased neonate mortality rates (Amin et al., 2021). Furthermore, endotracheal intubation for mechanical ventilation increases the risk of neonatal acquired pneumonia (Jeengar et al., 2024); therefore, the most acute complication of putting neonates on mechanical ventilation is VAP (Dipanjali et al., 2020).
The Evidence-Based Practices Module involves keeping the endotracheal intubation equipment for neonates as sterile as possible (via hand washing and the sterilization of intubated equipment), positioning the newborn to prevent reflux, and reassessing the newborn's readiness for routine tube removal (Khalfallah et al., 2024). Since the primary strategy used to reduce VAP incidence among high-risk neonates was the Evidence-Based Practices Module, this approach requires the simultaneous application of several preventive measures to each neonate, via the frequent use of checklists and other tools (Abdel-Hamed et al., 2024). Although the effectiveness of one or more Evidence-Based Practices Modules may be supported only by theoretical evidence or, in some cases, biological plausibility, the utilization of Evidence-Based Practices Modules has increased in popularity and success in recent years (Allari et al., 2025). The bundle strategy and the implementation of an Evidence-Based Practices Module for NICU nurses can prevent VAP and statistically reduce its frequency (Abohadida et al., 2025).
Most high-risk neonates in ICUs require respiratory support (mechanical ventilation); therefore, neonatal intubation is one of the primary contributors to the risk of neonatal VAP. Staff nurses may lack the required knowledge, which may hinder their ability to implement the Evidence-Based Practices Module for VAP prevention. Given that VAP is preventable and several practices have been proven to decrease its incidence and associated disease burden, educating nurses who care for mechanically ventilated, high-risk neonates about the causes and manifestations of VAP, its pathophysiology, potential risk factors, and preventive measures will enhance their knowledge, improve their practice, and reduce the incidence of VAP among high-risk neonates in NICUs.
However, the current literature for nurses concerning Evidence-Based Practices Modules related to the prevention of VAP is limited, highlighting the need for context-specific research to address the gap between the general lack of knowledge of NICU nurses and the demands for Evidence-Based Practices Modules for VAP. This research aimed to examine an Evidence-Based Practices Module concerning nurses’ knowledge and their practices for preventing VAP among high-risk neonates in the NICU. Sustainability in healthcare encompasses social and economic sustainability alongside environmental considerations, and an emphasis on long-term enhancements in workforce competency, resource efficiency, and care quality. This research encouraged environmentally friendly medical procedures via several routes: human resource sustainability (enhancing nurses’ abilities through education grounded in facts); economic sustainability (preventing diseases linked to healthcare - such as VAP - which reduces the demand for antibiotics, intensive care stays, and medical expenses); and social sustainability (enhanced results for a disadvantaged group and elevated standards of safety for newborn care).
Methodology
Study Design
For this study, a quasi-experimental approach was employed to conduct a pre- and post-test intervention study. This design lacked random assignment to groups, often using naturally occurring groups instead. The objective of this research is to infer a cause-and-effect relationship between the intervention and any observed changes in the dependent variable.
Study Hypotheses
Post-Evidence-Based Practices Module implementation: Nursing staff demonstrate improved knowledge concerning the prevention of VAP among high-risk neonates in NICUs.
Post-Evidence-Based Practices Module implementation: Nursing staff demonstrate improved practices concerning the prevention of VAP among high-risk neonates in NICUs.
Settings and Sampling
This study was conducted in the NICUs of two hospitals in Egypt: Banha Specialized Children's Hospital (Banha City) and, for review purposes, Ain Shams University Hospital (Cairo). According to Gray et al. (2016), the G*Power of 0.95 (β = 1–0.95 = 0.5) at α = 0.05 (one-tailed) with a large effect size (0.5) was utilized as the significance level, while 0.001 was utilized as the high significance level (considering the requirement for 200 nurses working within the aforementioned settings). Therefore, the convenience sample was utilized in the current study, as all 200 nurses (from different educational categories) were enrolled in this research. As a single group, this sample served as a pre-/post-test design. All of the participants in this study were volunteers who were selected according to the predetermined inclusion criteria. The participant group consisted of males and females with a range of educational backgrounds, some of whom had 1 year of experience in the NICU. Due to their limited knowledge and inexperience in caring for high-risk neonates in NICUs, assistant nurses (a rank of sub-nurses working under the direct supervision of a Registered Nurse) were excluded from this study. Before the study began, each participant nurse was supplied with information concerning the study's objectives and data confidentiality and was required to provide their written informed consent.
Instruments
First Instrument
Following a comprehensive review of the relevant literature (Elward et al., 2002; Sinuff et al., 2013), the researchers developed an Arabic language interview questionnaire consisting of two sections:
Part I contained questions concerning the demographic data of the nurse participants (such as age, gender, and educational qualifications) and their experiences of Evidence-Based Practices Modules concerning the prevention of VAP (For example, how many training courses have you attended and what was their duration?). Part II contained seven questions concerning nurses’ knowledge about VAP (such as definition, indicators, symptoms, diagnostic procedures, the importance of MV, different MV modes, and laboratory investigations).
Second Instrument
The nurses’ knowledge concerning Evidence-Based Practices Modules for preventing VAP was assessed pre- and post-implementation of an Evidence-Based Practices Module via the use of a multiple-choice questionnaire—adapted from Labeau et al. (2007)—containing 22 validated questions. The 22 questions covered the following areas: Positioning of high-risk neonates (2 questions), humidifier airway types (2 questions), standard or kinetic beds (1 question), endotracheal intubation oral or nasal demonstrations (4 questions), open or closed suction systems (6 questions), number of changes of ventilator equipment (1 question), frequency of humidifier changes (2 questions), extra-lumen tracheal tubes for subglottic drainage (2 questions), and suction system changes (2 questions). The nurses were interviewed individually, both pre- and post-implementation of the Evidence-Based Practices Module, to assess their knowledge. The scoring system awarded 1 mark for a correct answer and 0 marks for an incorrect answer; therefore, the highest possible score for the knowledge questions was 22. The same questionnaire items were used pre- and post-intervention. The level of each nurse's knowledge was assessed as follows: ≥ 80% = good; 60 to <80% = average; and <60% = poor.
Third Instrument
Adapted from Tolentino-DelosReyes et al. (2007), the third instrument was an observational checklist concerning nurses’ practices regarding the VAP preventive Evidence-Based Practices Module. The checklist consisted of nine items: hand washing frequency and infection control maneuvers, raising the head of the bed to 30° to 45°, monitoring gastric residuals in enteral feed to prevent neonatal aspiration, use of chlorhexidine and an oral swab every 4 hours to enhance oral care, performing intubation and oral suction with a separate suction catheter, performing in-line endotracheal tube suction, maintaining end of ventilator equipment and suction devices and removing the manual ventilation bag and mask from the bed, draining the ventilator fan capacitors repeatedly without opening the circuit, and suctioning the pharynx before repositioning neonates and repositioning the endotracheal tube. The researcher observed each participant while they conducted the aforementioned procedures. The Evidence-Based Practices Module for preventing VAP was implemented (taking 12 to 15 min per procedure), and the observers were blinded to minimize bias.
The maximum obtainable marks for the observational checklist were 11: one mark was given for each step completed, and zero marks were awarded for each incomplete step. Participants who received a score of ≥85% were judged as competent; a score of less than 85% was assessed as incompetent. An identical observational checklist was employed pre- and post-intervention.
Data Collection Procedure
The researchers reviewed a range of historical and contemporary literature, following which the data collection instruments were approved. Five experts from the pediatric nursing staff specialty were selected to establish face validity, convenience of the content, sentence sequence, and clarity, following which some minor language modifications were made according to their recommendations. A pilot study was conducted to assess the feasibility, applicability, and clarity of the selected instruments. Five participants from the nursing staff were included in the pilot; therefore, they were excluded from the study sample. Furthermore, the time taken to administer each tool was evaluated after the pilot study. A panel of experts (including five professors who specialize in pediatric nursing) reviewed and corroborated the content and validity of the study tools based on their expert opinions and feedback. For reliability, the results were assessed using Cronbach's alpha coefficient (r = 0.83 for the first tool), which demonstrated a significant difference across all items; however, the correlation coefficients were above the acceptable level of significance for the knowledge instrument. The alpha value for the performance checklist in the study sample was (r = 0.85). In contrast, Cronbach's alpha coefficient for the newborn assessment was (r = 0.79), indicating the high reliability of the study instruments.
Ethical Considerations
Ethical approval was gained from the Faculty of Nursing at the South Valley University (SVU-NUR-ADM: # 01-8-4-2024). Additionally, approval was sought from the hospital administrators at the aforementioned study settings. The participants received a comprehensive description of the study's objectives and the expected outcomes. The researchers obtained written consent from each participant, and their data were safeguarded by ensuring anonymity and confidentiality. Participants had the right to withdraw from the research at any time without any penalty.
Fieldwork
The current study was conducted between January 2025 and June 2025 to collect data concerning the use of Evidence-Based Practices Modules for the prevention of VAP in NICUs. By rotation, the researchers were available at the study settings; they visited each setting twice a week, through three shifts (morning, afternoon, and night), to observe routine MV procedures in NICUs.
Study Intervention
In the present study, an Evidence-Based Practices Module was meticulously shown to function as a fundamental intervention. Before the instructional presentation, the selected participants (staff nurses at NICUs) were divided into two groups (n = 100 for each group). This grouping facilitated a comprehensive understanding of each participant's knowledge, their practices during each session, and the structured system as a whole.
Pre-Intervention
The researchers assessed the nurses’ knowledge level and their practices in a pre-test to establish a baseline and then compared their scores with the post-test results. Pre-test questionnaires were conducted and evaluated after implementing the Evidence-Based Practices Module. The observation process involved the following basic nursing procedures: hand washing, infection control precautions (according to hospital polices), use of suction system, bed positioning, oral hygiene (swab & chlorhexidine), maintenance of MV accessories, and ventilator equipment changes. Each procedure took approximately 12 to 15 min per high-risk neonate.
Evidence-Based Practices Module Implementation
The researchers organized ten in-person group discussions, involving 20 nurses per session. Each session lasted approximately 30 minutes and used audiovisual aids (such as pictures, posters, handouts, flip charts, and data shows) for clarification. The procedures were conducted at NICUs, initially demonstrated by the researchers, and then re-demonstrated by researchers in front of the nurses. The training was conducted over 6 months. The performance segment included demonstrations of proper handwashing, implementation of infection control policies, suction system handling, bed positioning, oral hygiene with swabs and chlorhexidine, MV accessories maintenance, and ventilator equipment changes. Childcare procedures (such as the Evidence-Based Practices Module concerning neonatal VAP prevention) were repeated during and after each training session, demonstrated and re-demonstrated at the bedside, and routine neonatal care tasks (such as oral care and gastric residual checks) were repeated every 4–5 h.
Evaluation Phase
Five days after implementing an Evidence-Based Practices Module, the post-test questionnaire and observational checklist tools were used to assess the impact of an Evidence-Based Practices Module on the nursing staff's knowledge level and their practices.
Results
Table 1 shows the distribution of the participants’ demographic characteristics. The results revealed that the majority of participants (78.5%) were females, and that the mean age of the group was 28.41 ± 6.91. Additionally, the table shows that 66.6% of the participants had a bachelor's degree in nursing science, 4.0% had a master's degree, and 29.4% had a diploma. The majority of the study participants (80.4%) had not attended any training courses concerning VAP prevention; however, the remaining participants (19.6%) had previously attended VAP prevention training courses. 80.0% of the participants had only attended training courses on one occasion; however, 20.0% had attended more than once. When considering the duration of the training courses attended, 70.0% attended courses that lasted for one day, and the remaining 30.0% attended training courses that lasted for two or more days.
Participants’ Distribution About Their Demographic Characteristics (n = 200).
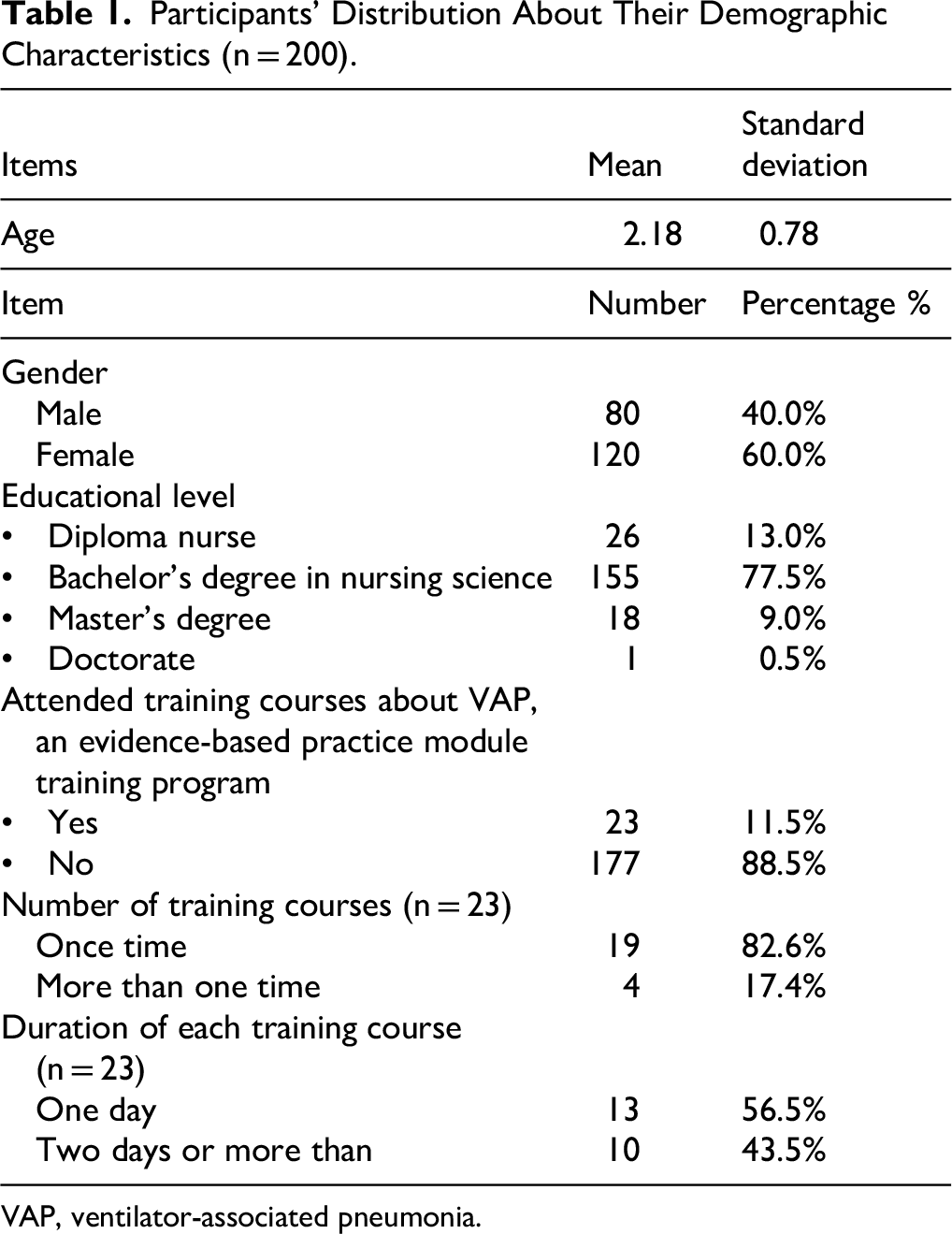
VAP, ventilator-associated pneumonia.
Table 2 presents a comparison between the participants’ level of knowledge about VAP before and after the demonstration of an Evidence-Based Practices Module. The assessment covered key foundational topics, including definition, clinical manifestations, causes, diagnostic approaches, laboratory investigations, and MV. A McNemar test was employed to detect statistically significant modifications in knowledge between the two points in time. Before the educational intervention, the proportion of correct responses across all items was notably low, ranging from 25.0% to 42.5%, indicating inadequate baseline knowledge among participants. The lowest pre-intervention scores were observed in items such as clinical manifestations (25.0%), modes of MV (25.5%), and causes of VAP (26.0%). Before the intervention, even basic concepts (such as the definition of VAP) demonstrated only 26.8% correctness. After implementing an Evidence-Based Practices Module, a significant improvement in knowledge was observed across all items. Correct responses rose dramatically, reaching 94.0% to 97.5% for all assessed domains. For example, participant knowledge concerning the clinical manifestations of VAP increased from 25.0% to 97.5% and participant understanding of the causes of VAP improved from 26.0% to 97.5%. Correspondingly, participant awareness of diagnostic procedures increased from 28.0% to 96.0%, and participant understanding of laboratory investigations improved from 27.5% to 94.0%. The importance of mechanical ventilation was the only item with a marginally higher baseline (42.5% correct); however, this domain also experienced a substantial post-intervention increase to 95.5% correctness. Statistical analysis was employed, and the McNemar test revealed highly significant improvements (p < .001) for all items. Chi-square values ranged from 90.369 to 135.529, supporting the conclusion that the implemented educational module had a robust and statistically significant effect on enhancing nurses’ general knowledge of VAP (see Table 2).
Comparison Between Nurses’ General Knowledge About Ventilator-Associated Pneumonia Pre- & Post-Evidence-Based Practice Module Implementation.

**Highly significant difference at p-value ≤.001.
MV, mechanical ventilator.
Table 3 presents a comparative analysis of participants’ knowledge level about the Evidence-Based Practices Module for preventing VAP before and after implementation of a targeted educational module. The McNemar test was utilized to assess the statistical significance of changes in knowledge across nine core clinical items. Before the intervention, the knowledge level was notably low across all items, with correct response rates ranging between 0.0% and 8.0%, reflecting a widespread lack of familiarity with Evidence-Based Practices Module VAP prevention measures. Contrastingly, the post-intervention results exhibited a substantial improvement: correct responses increased to between 96.4% and 98.5%, and incorrect responses decreased dramatically to 1.5%–3.6%. For example, participant understanding of the appropriate route for endotracheal intubation (oral vs. nasal) improved markedly: correct responses increased from 7.6% to 96.4%. Correspondingly, participant knowledge concerning the types of airway humidifiers increased from 6.0% to 98.5%, and correct answers related to suction systems (open vs. closed type) increased from 6.5% to 96.5%. Items that had 0% correct answers pre-interventions (such as standard vs. kinetic beds, neonatal positioning, and frequency of suction system changes) exhibited post-intervention gains of more than 98.0%. Notably, even items with slightly higher pre-intervention knowledge, such as subglottic drainage tubes (8.0% correct), displayed significant post-training improvement (96.5% correct). These results suggest that the implementation of an Evidence-Based Practices Module had a robust impact on areas of low- and moderate knowledge. All observed improvements were statistically significant, with McNemar chi-square values ranging from 163.894 to 195.005 and p < .001, indicating highly significant enhancements in nurses’ knowledge following an Evidence-Based Practices Module training intervention. These findings reinforced the importance and efficacy of structured educational modules in bridging knowledge gaps in critical care nursing practices (as shown in Table 3).
Comparison Between Nurses’ Knowledge About an Evidence-Based Practice Module for Preventing Ventilator-Associated Pneumonia Pre- & Post-Implementation.
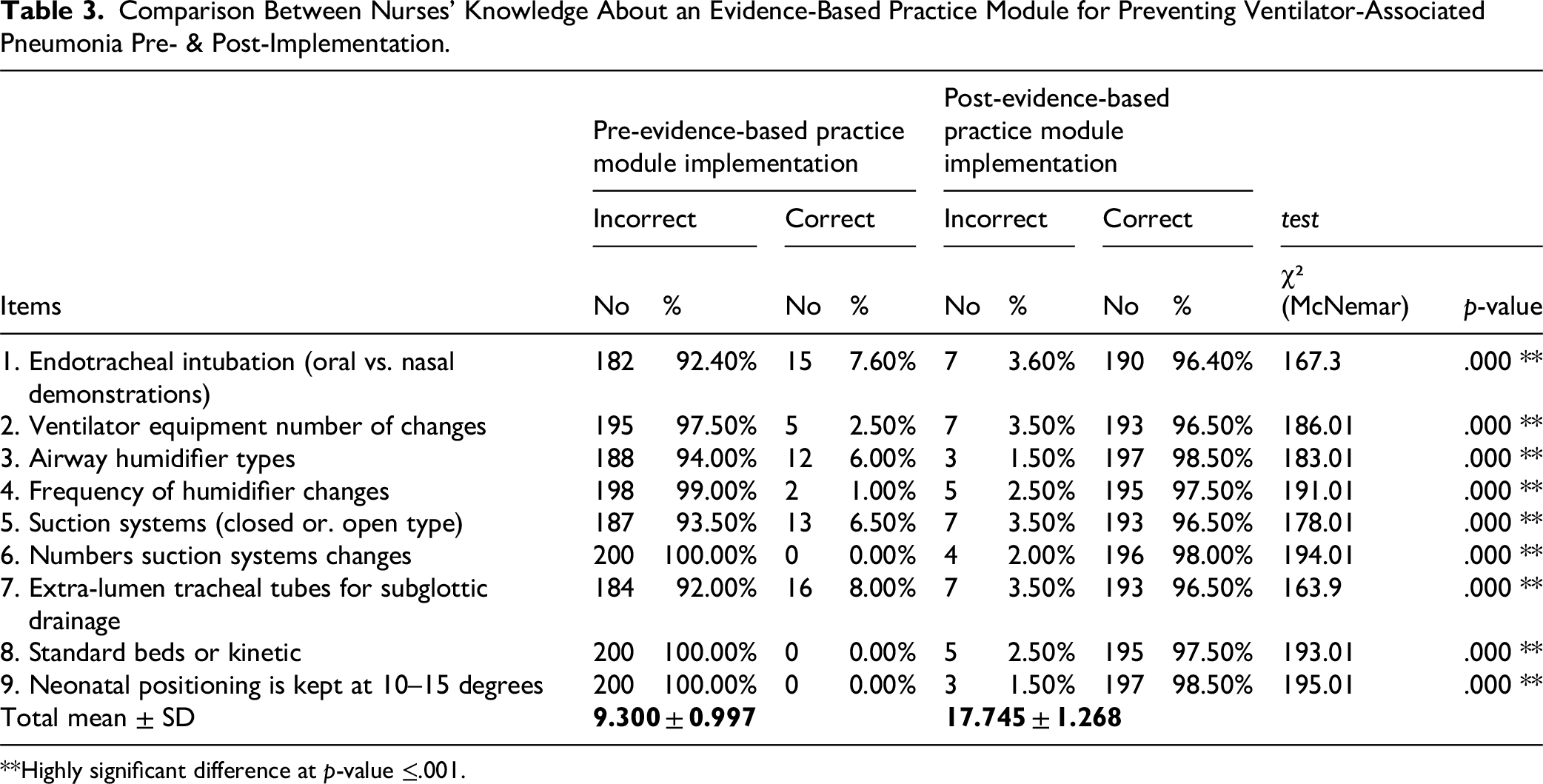
**Highly significant difference at p-value ≤.001.
Table 4 illustrates the effect of an Evidence-Based Practices Module on nurses’ adherence to VAP prevention strategies (as measured before and after implementation of the module). The practices were evaluated using a paired approach, and statistical significance was assessed using McNemar's test for correlated proportions. Across all 11 practice items, the results demonstrate highly significant improvements (p < .001) following an Evidence-Based Practices Module. These findings underscore the Evidence-Based Practices Module's effectiveness in translating knowledge into practical behavioral change. Frequent hand hygiene and infection control adherence rose from 15.5% pre-intervention to 95.0% post-intervention, with McNemar's χ² = 139.464 (p < .001), reflecting substantial improvement in basic infection prevention practices. Elevating the head-of-bed to between 30 and 45 degrees, a well-known VAP prevention measure, increased from 15.0% to 98.0%, with an extremely high χ² value of 156.466, highlighting strong uptake post-intervention. Monitoring of gastric residuals every 5 h improved from 15.5% to 93.5%, while oral care with chlorhexidine every 4 h increased from 8.5% to 93.0% adherence (χ² = 149.333, p < .001), indicating improved compliance with Evidence-Based Practices Module oral hygiene protocols. Significant changes were also observed in more technical procedures, such as the use of separated suction catheters for intubation and oral suctioning (15.5% to 98.0%), inline endotracheal suction systems (9.0% to 98.0%), and removal of manual ventilation bags from the bedside (10.0% to 98.0%). Equipment handling practices (such as draining ventilator fan condensate without circuit interruption) increased from 7.0% to 98.0%, indicating a dramatic adoption of best practices (χ² = 176.134, p < .001). Adherence to pharyngeal suctioning before key procedures, such as endotracheal intubation (15.5% to 98.5%), neonate repositioning (7.5% to 98.5%), and endotracheal tube repositioning (9.0% to 93.5%), also exhibited statistically and clinically significant improvement. Collectively, these results revealed a consistent and robust enhancement in clinical practices post-intervention. The exceptionally high chi-square values in each domain further reinforced the magnitude of behavioral change, driven by the structured Evidence-Based Practices Module (as shown in Table 4).
Comparison Between Nurses’ Practices About an Evidence-Based Practices Module for Preventing Ventilator-Associated Pneumonia Pre- & Post-Implementation.
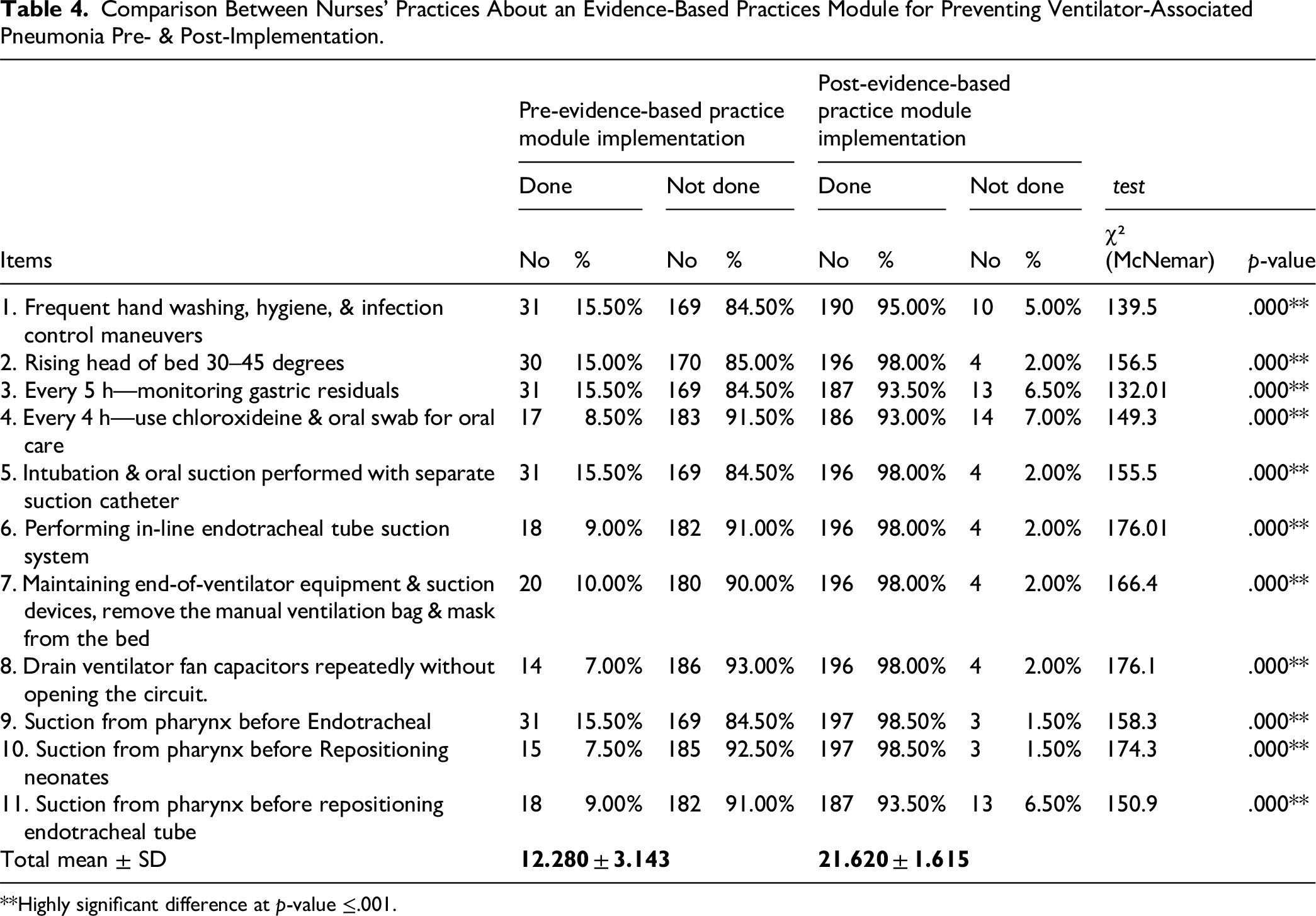
**Highly significant difference at p-value ≤.001.
Table 5 shows a comparison of mean scores for participants’ overall knowledge concerning VAP, their understanding of an Evidence-Based Practices Module for VAP prevention, and their actual practices related to the module, as measured before and after its implementation. A paired sample t-test was utilized to assess the intervention's effectiveness. The results revealed highly significant improvements (p < .001) in all of the areas evaluated. General knowledge concerning VAP increased markedly from a pre-intervention mean score of 9.010 ± 2.894 to 13.640 ± 1.285 after the intervention (t = −18.954, p < .001), where the Confidence Interval was 3.99–5.27, with an effect size of 0.518. This indicates that an Evidence-Based Practices Module significantly enhanced basic understanding among the nursing staff. Knowledge regarding VAP prevention and the Evidence-Based Practices Module demonstrated the most notable improvement. The pre-implementation score was 9.300 ± 0.997, reflecting an almost complete lack of knowledge, which rose significantly to 17.745 ± 1.268 post-intervention (t = −67.574, p < .001), where the Confidence Interval was 8.75–8.13 with an effect size of 0.932. This demonstrated the Evidence-Based Practices Module's effectiveness in delivering targeted information. Additionally, practice related to Evidence-Based Practices Module concerning VAP prevention measures experienced substantial gains: the mean score increased from 12.280 ± 3.143 (before the module) to 21.620 ± 1.615 (after implementation) (t = −31.009, p < .001), where Confidence intervals were 8.55–10.12 with an effect size of 0.778. These results indicate a robust positive change in participants’ application of the knowledge learned during the Evidence-Based Practices Module. Overall, the analysis of this study's findings confirms the statistical and practical significance of the module in improving nurses’ knowledge and practice concerning VAP prevention.
Mean Score for Nurses’ General Knowledge About VAP, an Evidence-Based Practice Module Knowledge & Their Practices About Evidence-Based Practice Module Pre- & Post-Implementation for VAP Prevention.

**Highly significant difference at p-value ≤.001.
VAP, ventilator-associated pneumonia.
Discussion
The management, treatment, and prevention of nosocomial infection among neonates on mechanical ventilation are essential tasks performed by the participant nurses in the NICU. To decrease the risk of VAP and minimize the morbidity and mortality rate of neonates on mechanical ventilation in the NICU, staff nurses must be appropriately trained and educated regarding VAP prevention (Elsaeed et al., 2025). Implementing an Evidence-Based Practices Module could enhance the commitment of nurses to VAP prevention efforts, leading to enhanced neonatal outcomes and improved nursing care (Abohadida et al., 2025). To reduce the incidence of VAP among newborns in NICUs, this study focused on assessing the impact of using an Evidence-Based Practices Module to improve participant nurses’ knowledge and application of VAP prevention techniques (Amin et al., 2021). This aligns with Khalfallah et al. (2025), who noted that improving the knowledge of nurses who care for neonates on MV could reduce the VAP ratio.
The findings of the current study clarified that more than half of the participant nurses (66.6%) held a bachelor's degree in nursing science, and the majority of the participant nurses (80.4%) had not attended any training courses concerning VAP prevention, which may explain the participants’ limited knowledge about the causes of VAP. This finding aligns with Shivananda and Yashoda (2021), who noted that nurses who had not attended any VAP prevention training courses had a lower knowledge level and performed at a lower level than nurses who had attended such courses. The current study revealed that an Evidence-Based Practices Module improved nurses’ overall understanding of VAP prevention in NICUs and enhanced their knowledge regarding the importance of mechanical ventilation, diagnostic criteria, and specific VAP prevention measures (Khalfallah et al., 2024). Simultaneously, the participants’ knowledge of the causes of VAP and the importance of laboratory investigations for neonates supported by mechanical ventilation was positive and stable pre- and post-demonstration of an Evidence-Based Practices Module. The results of the current study reflected high significance between nurses’ general knowledge pre- and post-implementation of an Evidence-Based Practices Module, with a mean score of (9.010 ± 2.894 to 13.640 ± 1.285, respectively), which reflected the effectiveness of an Evidence-Based Practices Module for preventing VAP. This result was confirmed by Elkalashy and Attia (2017), who noted that improving nurses’ knowledge and their ability to provide effective care would enhance the quality of neonatal health care and reduce the incidence of morbidity among newborns.
According to Elkalashy and Attia (2017), the educational program had an appropriate impact on the level of knowledge of nurses and was instrumental in influencing performance, particularly regarding VAP prevention. This study emphasized the need to maintain an adequate level of knowledge among nursing staff to achieve superior outcomes for newborns. Previous findings were supported by the current study, which found that participant nurses’ knowledge level of certain areas (such as changes in humidifiers, suction systems (closed or open type), extra-lumen tracheal tubes for subglottic drainage, and standard beds vs kinetic beds) was lower before implementing an Evidence-Based Practices Module than after.
Furthermore, the findings of the current study clarified that most participants had limited knowledge regarding intubation via the endotracheal method. They emphasized that physicians typically demonstrated the oral method; however, on some occasions, both methods were demonstrated after physicians had made their decisions, without identifying the causes or which route is superior for VAP prevention. After completing an Evidence-Based Practices Module, 90.2% of participants judged the oral method as superior to the nasal route. Invasive procedures (such as intubation lasting more than 48 h) were considered a risk factor for hospital-acquired infections involving VAP; therefore, ventilation cannot be provided without intubation (Dipanjali et al., 2020). Additionally, the same study found that, compared to a nasotracheal tube, an oral endotracheal tube was associated with a lower incidence rate of VAP. Finally, regarding nurses’ knowledge about the Evidence-Based Practices Module, the present study revealed a highly significant difference between nurses’ scores before and after implementing the module: the mean score increased from (9.300 ± 0.997) to (17.745 ± 1.268). This reflects the effectiveness and importance of the Evidence-Based Practices Module in preventing VAP in NICUs.
A Saudi Arabian study by Corpuz-Pulido (2023) noted that one of the primary risk factors for VAP in NICUs concerns gastric secretions, which are considered the initial method of bacterial entry into the respiratory system and a significant contributor to the increase in VAP. In the current study, the lowest scores achieved in any category concerned the use of intubation with an extra-lumen for the drainage of subglottic secretions; however, following the implementation of an Evidence-Based Practices Module, the participants’ scores increased from 2% to 70.6%.
When comparing the participants’ knowledge level concerning the frequency of humidifier changes and the utilization of the suction system (opened vs closed), the participants’ scores were low 6%; however, following the implementation of an Evidence-Based Practices Module, they increased. The implementation of a low-outcome evidence-based practice module may be influenced by the performance of the nursing staff responsible for managing this care. These findings align with those reported by Ali and Ahmed (2023), who reported that changing humidifiers is the responsibility of respiratory therapists, who may be influenced by manufacturers’ recommendations to change heat and moisture exchange filters every 72 h. A study reported that infrequent changes to heat and moisture exchange filters may be considered with a lower incidence of mechanical VAP, as well as the use of proximal suction systems, which were changed for each newborn and based on clinical indications (Afroze & Shahidullah, 2022).
When considering the participant nurses’ performances in a Caring and Evidence-Based Practices Module for VAP prevention, significant differences were reported in participants’ hand washing performance pre-contact with neonates: less than half of the participants (45.1%) completed this task successfully; however, following the Evidence-Based Practices Module intervention, this figure increased to 98%. This result aligns with Abu-Elenen and Mehany (2024), who reported modifications in participants’ hand washing performance that reflected improved levels of professionalism and increased awareness about appropriate hand hygiene. Furthermore, these findings correspond with Barden (2021), who identified that the use of gloves—before and after direct or indirect contact with neonates—was vital to reducing infection.
Neonatal positioning (raising the head of the bed to between 30 and 45 degrees to minimize neonatal oral aspiration or peptic secretions) was found to decrease the incidence of VAP (Mohamed et al., 2023). The current study found that, before an Evidence-Based Practices Module intervention, raising the head of the bed was utilized at a rate of 7.7%; however, following the intervention, this rate increased to 86.3%. Participants considered that neonatal positioning may be a risk for some neonates. Several factors may have contributed to the significant improvement in this domain: Firstly, the participants’ significantly low baseline scores suggested that they had little prior knowledge or experience, which made it possible for them to make significant, quantifiable improvements following the intervention; secondly, the intervention's high level of structure, interaction, and direct targeting of the identified knowledge gaps facilitated learning; and thirdly, the participants were encouraged to put what they had learned into practice immediately, thereby improving both performance and retention. These results align with Corpuz-Pulido (2023), who reported that the mean elevation of the bedhead for neonates with MV was always less than 30 to 45 degrees.
The findings of one study, which investigated critically ill patients to assess the correlation between dental issues and respiratory infection, revealed that dental problems could act as sources of microorganisms; therefore, oral care is a proper technique for lowering VAP (Klompas et al., 2022). In the current study, before the implementation of an Evidence-Based Practices Module, 3.9% of participants performed oral care every 4 hours; however, post-implementation, this figure increased to 70.6%. A different study found that the use of a staff nursing self-reporting system increased the frequency of oral hygiene: the documented mean frequency of oral hygiene for patient intubation was 4.5 episodes in 24 h, while the self-report frequency was 5.3 episodes (Ali & Ahmed, 2023). For critical care patients, brushing teeth with a soft toothbrush twice a day, utilizing oral swabs, maintaining mouth moisture every 2 to 4 h, frequent oral suction, and changing oral suction catheters every 24 h were highly recommended by the American Association of Critical Care Nurses manual procedures (Ali & Ahmed, 2023). The present study reported that, pre-implementation of an Evidence-Based Practices Module, 33.3% of subjects used a separate suction catheter for oral suctioning (compared to 78.4% post-intervention); however, this may be attributed to a lack of equipment (Corpuz-Pulido, 2023).
Subglottic deep suctioning could be performed as a routine task during neonatal assessment and for repositioning the endotracheal tube (Meintjes, 2021). In the present study, there was a marked change in participants’ performances post an Evidence-Based Practices Module compared to pre-intervention of suctioning via repositioning for endotracheal tube neonates. This study clarified that the participant nurses had improved their performance in draining the ventilator fan capacitors repeatedly without opening the circuit (2.0% before the implementation of an Evidence-Based Practices Module compared to 94.1% after). This aligns with Meintjes (2021), who stated that maintaining a closed circuit reduces the possibility of infection from external microorganisms.
The findings of this study confirm a highly significant improvement between participant nurses’ performances pre- and post the implementation of an Evidence-Based Practices Module for VAP prevention. The mean score increased from 12.280
In summary, this study found that the mean score level for the participants’ general knowledge, knowledge regarding VAP, and their performance were enhanced following the implementation of an Evidence-Based Practices Module (t = −18.95**, −67.57**, and −31.01** respectively at p = 0.00).
Strengths and Limitations
This study's strengths were based on its results, which are directly applicable to the enhancement of patient care because they address VAP, a serious and recurrent issue in NICUs. The intervention makes use of an Evidence-Based Practices Module to guarantee that the information is based on proven methodologies rather than intuition. The study design strengthened the connection between the implementation of an Evidence-Based Practices Module and improvements in nurses’ knowledge and practices following the intervention. Moreover, the combination of an observational checklist, a knowledge questionnaire, a large sample size, and an interview questionnaire facilitated data triangulation, thereby improving the study's validity.
The primary limitation, according to the Hawthorne effect, is the length of development, which did not allow for a long-term assessment of the effectiveness of an Evidence-Based Practices Module and whether knowledge and practice levels remained adequate several months later. Therefore, future research should assess knowledge retention and long-term practice changes by conducting follow-up evaluations at 3, 6, or 12 months. Additionally, the current study failed to address all the factors that may have contributed to the incidence of nurse-associated pneumonia among neonates (such as the nurse-to-neonate ratio, reduced number of nursing staff, and increased workload). This study utilized a single-group pre-/post-design without a control group, which limited its ability to attribute observed changes solely to the intervention; therefore, future studies should include a control or comparison group to strengthen internal validity and allow for causal inferences. Furthermore, the use of a convenience sample in this study may have limited the generalizability of its findings; therefore, it is recommended that future studies should include all of the factors that may contribute to VAP prevention.
Implications for Clinical Practice
This study has demonstrated that participation in an Evidence-Based Practices Module for VAP prevention improved nurses’ professional development, ensured safe and competent practice, and enhanced the quality of care for high-risk neonates. All hospitals should organize ongoing educational sessions for NICU nurses to refresh and update their knowledge and skill set. Additionally, workshops that verify an Evidence-Based Practices Module related to the VAP module should be established, and these instructional sessions should be provided to nurses. Instructional brochures and handouts concerning VAP prevention should be distributed to all NICU nursing staff as part of the protocol. Furthermore, efforts should be made to enhance the knowledge and practices of all nursing staff regarding factors influencing an Evidence-Based Practices Module in pediatric ICUs.
Conclusion
The current study revealed inadequate knowledge and incompetence among nurses regarding VAP prevention in NICUs. However, following the implementation of an Evidence-Based Practices Module, there was a significant and notable improvement in nurses’ knowledge and practices concerning VAP prevention among high-risk neonates. This research highlighted the positive impact of implementing an Evidence-Based Practice Module on nurses’ knowledge of VAP prevention in NICUs. The implementation of an Evidence-Based Practice Module significantly enhanced the knowledge and performance of nurses in preventing VAP. The introduction of VAP as an Evidence-Based Practice Module for nursing staff promoted their professional development, ensured safe and proper performance, and improved the quality of care provided to high-risk neonates in NICUs.
Supplemental Material
sj-docx-1-son-10.1177_23779608251408925 - Supplemental material for The Impact of an Evidence-Based Practice Module on Nurses’ Knowledge and Practices for Preventing Ventilator-Associated Pneumonia Among High-Risk Neonates: A Quasi-Experimental Study
Supplemental material, sj-docx-1-son-10.1177_23779608251408925 for The Impact of an Evidence-Based Practice Module on Nurses’ Knowledge and Practices for Preventing Ventilator-Associated Pneumonia Among High-Risk Neonates: A Quasi-Experimental Study by Amira Adel Mohammed, Rabia S. Allari and Mahmoud H. Alrabab’a in SAGE Open Nursing
Supplemental Material
sj-docx-2-son-10.1177_23779608251408925 - Supplemental material for The Impact of an Evidence-Based Practice Module on Nurses’ Knowledge and Practices for Preventing Ventilator-Associated Pneumonia Among High-Risk Neonates: A Quasi-Experimental Study
Supplemental material, sj-docx-2-son-10.1177_23779608251408925 for The Impact of an Evidence-Based Practice Module on Nurses’ Knowledge and Practices for Preventing Ventilator-Associated Pneumonia Among High-Risk Neonates: A Quasi-Experimental Study by Amira Adel Mohammed, Rabia S. Allari and Mahmoud H. Alrabab’a in SAGE Open Nursing
Supplemental Material
sj-docx-3-son-10.1177_23779608251408925 - Supplemental material for The Impact of an Evidence-Based Practice Module on Nurses’ Knowledge and Practices for Preventing Ventilator-Associated Pneumonia Among High-Risk Neonates: A Quasi-Experimental Study
Supplemental material, sj-docx-3-son-10.1177_23779608251408925 for The Impact of an Evidence-Based Practice Module on Nurses’ Knowledge and Practices for Preventing Ventilator-Associated Pneumonia Among High-Risk Neonates: A Quasi-Experimental Study by Amira Adel Mohammed, Rabia S. Allari and Mahmoud H. Alrabab’a in SAGE Open Nursing
Supplemental Material
sj-doc-4-son-10.1177_23779608251408925 - Supplemental material for The Impact of an Evidence-Based Practice Module on Nurses’ Knowledge and Practices for Preventing Ventilator-Associated Pneumonia Among High-Risk Neonates: A Quasi-Experimental Study
Supplemental material, sj-doc-4-son-10.1177_23779608251408925 for The Impact of an Evidence-Based Practice Module on Nurses’ Knowledge and Practices for Preventing Ventilator-Associated Pneumonia Among High-Risk Neonates: A Quasi-Experimental Study by Amira Adel Mohammed, Rabia S. Allari and Mahmoud H. Alrabab’a in SAGE Open Nursing
Footnotes
Acknowledgment
The researchers thank the neonatal intensive care unit nursing staff and all members who supported the current study.
Ethics Approval and Consent to Participate
Ethical approval was obtained from the Faculty of Nursing at the South Valley University (SVU-NUR-ADM: # 01-8-4-2024). Approval from hospital administrators was also sought in the previously mentioned study settings, which conform to the provisions of the Declaration of Helsinki in 1995 (as revised in Edinburgh 2000). Further, informed consent to participate was obtained from all the participants.
Author Contributions
AA contributed to methodology, data analysis, conceptualization, writing, and review & editing. MA contributed to validation and supervision. RA contributed to review, editing, and validation.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
All data that were analyzed during this study are available to the corresponding author upon request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.