
Abstract
Introduction
Nurses’ ability to understand and manage emotions may offer insight into why certain aspects of care are missed, alongside operational aspects, including staffing and workload. The current body of nursing literature has examined the structural and procedural dimensions of missed nursing care (MISSNCARE), frequently neglecting the significant influence of emotional factors in the provision of healthcare. Specifically, emotional intelligence (EI) may influence clinical decision-making by enhancing prioritization, stress management, and interpersonal communication, thereby reducing care omissions.
Objectives
This study aimed to examine the relationships and differences between the perceived types and reasons for MISSNCARE and registered nurses’ (RNs) levels of EI. In addition, predictors of MISSNCARE were identified.
Methods
A quantitative cross-sectional design was used in the current study. A convenience sample of 285 RNs was recruited from different hospitals. Descriptive and inferential statistics were applied to analyze the data.
Results
The most frequent type of MISSNCARE activities was patient ambulation, and the most common reason for MISSNCARE was related to labor resources. Nurses perceived that they had higher-than-average levels of EI. A statistically significant, strong negative correlation was found between the perceived EI levels and types of MISSNCARE. The results also indicated that 42.90% of the variance in MISSNCARE was explained jointly by the role of EI, hospital type, gender, and marital status. Single and female nurses with higher EI levels and who worked in private hospitals reported lower incidences of MISSNCARE compared to their counterparts.
Conclusions
Nurses with higher levels of EI reported a lower incidence of MISSNCARE. Future research should consider more robust methods to enhance a more comprehensive understanding of the relationship between MISSNCARE and nurses’ EI. The findings underscored the potential for strategic improvement in EI as a means to reduce instances of MISSNCARE and enhance the overall quality of patient care.
Introduction
Healthcare systems are inherently unpredictable due to emerging diseases, technological advances, staffing challenges, economic pressures, and changing social dynamics (Aminabee, 2024). Nurses, as the backbone of healthcare, play a critical role in ensuring effective care through continuous monitoring. Any MISSNCARE can compromise patient safety and quality, leading to complications and adverse events (Larsson et al., 2022; Willis & Brady, 2022).
MISSNCARE refers to necessary nursing tasks that are partially or completely omitted or delayed (Kalisch et al., 2009). Key contributing factors include poor workplace conditions, dissatisfied staff, insufficient personnel, frequent patient admissions and discharges, unexpected critical events, inappropriate work schedules, high workload, and burnout (Cho et al., 2021; Da Silva et al., 2021; Kiekkas et al., 2021). Kirwan and Matthews (2020) noted that MISSNCARE leads to increased patient mortality and negatively affects nursing staff through burnout and dissatisfaction, which impede organizational growth and increase turnover rates.
Emotional intelligence (EI) is the ability to recognize and manage one's own and others’ emotions to guide thinking and behavior (Salovey & Mayer, 1990). It includes five learnable skills: self-awareness, self-regulation, motivation, empathy, and social skills (Castelino & Mendonca, 2021). Effective patient care depends on understanding patients’ emotions, managing oneself, and maintaining relationships (Larsson et al., 2022; Willis & Brady, 2022). Managing stress and dissatisfaction from multitasking is also essential for high-quality care.
Given the emotional demands of nursing, understanding the role of EI in mitigating MISSNCARE is increasingly important. Despite growing recognition of EI and MISSNCARE in healthcare, research has predominantly focused on structural and procedural aspects, often overlooking emotional and psychological factors (Albsoul et al., 2023). Few studies explore the connection between EI and MISSNCARE within specific cultural and institutional contexts, such as Jordan (Albsoul et al., 2023; Alfuqaha et al., 2023). To address this gap, this study uniquely examined the relationships and differences between the perceived types and reasons for MISSNCARE and registered nurses’ (RNs) levels of EI, while also identifying predictors of MISSNCARE. By incorporating hospital type and nurses’ demographic characteristics, and focusing on northern Jordan, the research offers culturally specific insights that contribute original evidence to regional nursing literature and fill a gap in nursing leadership scholarship.
Furthermore, EI, with its emphasis on understanding emotions, may help clarify the complexities inherent in MISSNCARE (Alfuqaha et al., 2023). The existing literature has largely investigated the structural and procedural aspects of MISSNCARE, often overlooking the profound impact of emotional aspects in healthcare delivery (Albsoul et al., 2023; Hosseini et al., 2023; Khrais et al., 2023). For example, nurses with higher levels of EI tend to make more accurate and timely clinical decisions, effectively prioritize patient needs, and collaborate with interdisciplinary teams, highlighting EI's role in enhancing clinical judgment and reducing care omissions, such as minimizing medication errors and ensuring timely ambulation (Ayed, 2025).
Theoretical Framework
This study was guided by the MISSNCARE Model (Kalisch et al., 2009), which explains how both organizational and individual factors contribute to the omission of essential nursing care. The model identifies three main domains: (a) care environment antecedents (e.g., staffing, resources, and communication); (b) the nursing process (assessment, planning, implementation, and evaluation); and (c) nurses’ internal processes (team norms, decision-making, values, and habits). These elements interact to shape whether care is delivered, delayed, or missed, ultimately affecting patient outcomes. The present study focuses particularly on the internal processes domain, examining EI as a potential factor influencing MISSNCARE.
Specifically, EI is seen as a blend of cognitive and emotional skills that significantly impact how nurses understand, interpret, and react to both people and situations in their professional setting. By influencing how decisions are made, how teams work together, and how emotions are managed, EI can affect the internal processes described in Kalisch's model—especially regarding the values, routines, and team agreements that dictate how care is prioritized and delivered (McManus, 2021).
Literature Review
MISSNCARE negatively impacts both patient outcomes and organizational stability. To address this, interventions like adequate staffing, supportive environments, and teamwork have shown effectiveness (Alasmari et al., 2023; Ghezeljeh et al., 2021). Building on this, Kalisch et al. (2009) highlighted nurses’ internal processes, values, beliefs, and habits in the MISSNCARE model. Emotions are integral to nursing practice (Dugué et al., 2021). As frontline caregivers in constant contact with teams, patients, and families, nurses need emotional competence to handle daily challenges, which can otherwise affect their professional commitment (Hoeve et al., 2020; Soto-Rubio et al., 2020).
In addition to emotional competence, several factors, such as gender, can influence EI. Nursing has traditionally been a female-dominated field, with assumptions that women possess greater empathy and emotional sensitivity (Laskowski et al., 2024). However, recent studies challenge this view. For example, a study of nursing students in Poland found that both male and female students had proficient EI, but standardized scores showed that males had higher EI than females (Laskowski et al., 2024). This result may reflect a self-selection effect, where men entering nursing already exhibit higher EI to compensate in a female-dominated profession.
Beyond gender differences, EI has many positive outcomes; it positively impacts nursing by enhancing communication, critical thinking, problem-solving, time management, and teamwork (Ahmed et al., 2023; Li et al., 2021). It also strengthens nurses’ caring abilities, which are crucial for quality care (Lee & Kim, 2021), and has been shown to improve patient satisfaction, a key indicator of care quality and organizational effectiveness (Nair, 2023). Given these benefits, nurses’ emotions, thoughts, and perceptions shape their behaviors and clinical practice (Kalisch et al., 2009), highlighting the importance of examining the link between MISSNCARE and EI. EI is significantly related to job well-being (Li et al., 2021), while MISSNCARE is associated with lower job satisfaction (Bragadóttir et al., 2020). Nurses’ caring behaviors, influenced by EI, reduce omitted care and adverse events, thereby improving the quality of patient care (Labrague et al., 2020; Taylan et al., 2021).
In light of this, the present study aimed to examine the relationships and differences between the perceived types and reasons for MISSNCARE and RNs’ levels of EI. In addition, predictors of MISSNCARE were identified. The results of this study could be used to inform targeted interventions aimed at reducing MISSNCARE by enhancing EI among nurses. Training programs that focus on emotional competencies serve as a strategic tool to improve patient outcomes (Mao et al., 2021). The study provides evidence-based insights that can be used to foster emotionally intelligent nursing environments, reduce care omissions, and elevate the overall quality of healthcare services (Alasmari et al., 2023).
Methods
Study Design
A quantitative, cross-sectional design was used to study the variables of interest. This design was selected for its efficiency in terms of time, cost, and effort (Polit & Beck, 2017). However, because data were collected at a single point in time, causal relationships between variables cannot be established.
Research Questions
This study aimed to answer the following research questions:
What are the perceived types and reasons for MISSNCARE and the levels of EI among nurses? What is the relationship between perceived MISSNCARE types and levels of EI? What are the relationships and mean differences between background variables and the study's main variables?. What are the predictors of MISSNCARE?
Settings and Sample
Jordan's healthcare system comprises 121 hospitals across various sectors: 33 governmental (27%), 15 military (12%), 71 private (59%), and 2 university-affiliated (2%) (Private Hospitals Association, 2023). This study was conducted in three hospitals representing key sectors—governmental, private, and university-affiliated—all located in northern Jordan. The target population included all RNs in Jordanian hospitals; the accessible population consisted of RNs working in the selected facilities. Inclusion criteria required RNs with at least one year of experience who were willing to participate. Nurses in administrative positions were excluded. It should be noted that the study's findings are limited in generalizability due to the inclusion of only three hospitals and the exclusion of military hospitals.
Using the rule of thumb by VanVoorhis and Morgan (2007), the sample size was calculated as: (7 demographic + 4 MISSNCARE + 7 EI variables) × 10 + 50 = 230. To offset potential non-response, the sample size was increased to 300. A convenience sample of eligible, on-duty RNs was recruited. Of the 300 distributed questionnaires, 288 were returned; 3 were incomplete and excluded, yielding 285 valid responses (95% response rate). While this approach facilitated timely data collection, it may introduce selection bias and limit the representativeness of the findings.
Ethical Considerations and Data Collection Procedures
This study followed the STROBE guidelines for observational research. Ethical approval was obtained from the Institutional Review Board (IRB) at the Jordan University of Science and Technology (JUST) (IRB No. 3/163/2023 dated August 30, 2023), the Ministry of Health (MoH) (IRB No. MOH/REC/2023/396 dated October 11, 2023), and the selected hospitals. Data were collected from September 26 to October 25, 2023.
Prior to participation, nurses received a full explanation of the study's purpose and provided informed consent. Questionnaires were distributed and collected by the researchers using sealed envelopes. Participation was voluntary, and nurses could withdraw at any time without consequence. Confidentiality and anonymity were maintained, with responses reported in aggregate form. All data were securely stored in a locked cabinet and on a password-protected computer accessible only to authorized researchers.
Instruments
A demographic data form was developed by the researchers, including nurses’ gender, age, marital status, level of education, years of experience as a nurse, years of experience in the current position, and the working unit.
The Cronbach’s alpha for the MISSNCARE Survey was 0.86 (Kalisch et al., 2009). Pearson's correlation coefficient for test-retest reliability was 0.87 for part A and 0.86 for part B (Kalisch & Williams, 2009). The MISSNCARE tool was translated into many languages; therefore, the Arabic version of the MISSNCARE survey was used, as it was valid and reliable; the Cronbach’s alpha was 0.98 for part A and 0.90 for part B (Saqer & AbuAlRub, 2018) and was 0.94 for part A and 0.90 for part B in another study (Al-Faouri et al., 2021). In this study, the Cronbach’s alpha was 0.97 for part A and 0.92 for part B of the MISSNCARE Survey.
The Genos Emotional Intelligence Inventory was used because it assesses EI as a set of workplace-related behaviors rather than as an abstract trait, which makes it particularly relevant for nursing practice. Compared to other EI instruments, the Genos scale emphasizes how emotions are expressed, managed, and utilized in professional interactions. This focus aligns well with the study's context, where nurses’ emotional skills directly affect teamwork, communication, and patient care outcomes.
The Cronbach’s alpha for the subscales fluctuated between 0.71 and 0.93, which indicates that the instrument is reliable (Palmer et al., 2009). The Arabic version was used, as it was shown to be valid and reliable (Al-Hamdan et al., 2019), with an adequate level of internal consistency (Cronbach's alpha = 0.89). In this study, the Cronbach's alpha for the whole EI scale was 0.95. For the subscales, Cronbach’s alphas were 0.63 for ESA, 0.76 for EE, 0.70 for EAO, 0.85 for ER, 0.79 for ESM, 0.71 for EMO, and 0.70 for ESC. Although the ESA subscale showed slightly lower reliability, it has been validated in previous research and captures a theoretically important aspect of EI. Therefore, including this subscale is essential for a comprehensive assessment of EI in the study.
Data Analyses
The Statistical Package for Social Sciences software (SPSS version 26) (IBM Corp., 2019) was used to analyze the collected data. The level of significance was set at 0.05. Data were coded, cleaned, and checked for statistical assumptions. The normality of continuous variables was assessed using the Shapiro-Wilk test and by examining skewness and kurtosis values, ensuring the assumptions for parametric tests were met. Listwise deletion was applied for cases with missing data, meaning that incomplete records were excluded from the analyses.
Descriptive statistics of frequencies, percentages, means, and standard deviations were used to describe the demographic data and variables according to the level of measurement (Polit & Beck, 2017). Pearson's correlation coefficient was used to assess the relationships between continuous variables. Furthermore, independent t-tests, the analysis of variance (ANOVA) tests, and the Tukey post hoc tests were used to test differences in categorical background variables and the continuous variables of the study. Moreover, multiple linear regression was utilized to determine the predictors of MISSNCARE (Polit & Beck, 2017). While the analysis offers meaningful findings, the reliance on self-report measures carries the risk of response bias, which could influence the accuracy of how EI and MISSNCARE were reported.
Results
Sample Characteristics
Most participants were female (63%) and aged 23–51 years (M = 34.53). In terms of background, 70% were married and 92.6% held bachelor's degrees. Professionally, nurses averaged 11.2 years of experience, with 6.3 years in their current roles. Participants worked across sectors, including governmental (41%), university-affiliated (35%), and private hospitals (24%). More details are listed in Table 1.
Group Differences in Missed Nursing Care, Reasons for Missed Nursing Care, and Emotional Intelligence by Demographic Variables (n = 285).

The Perceived Types of MISSNCARE
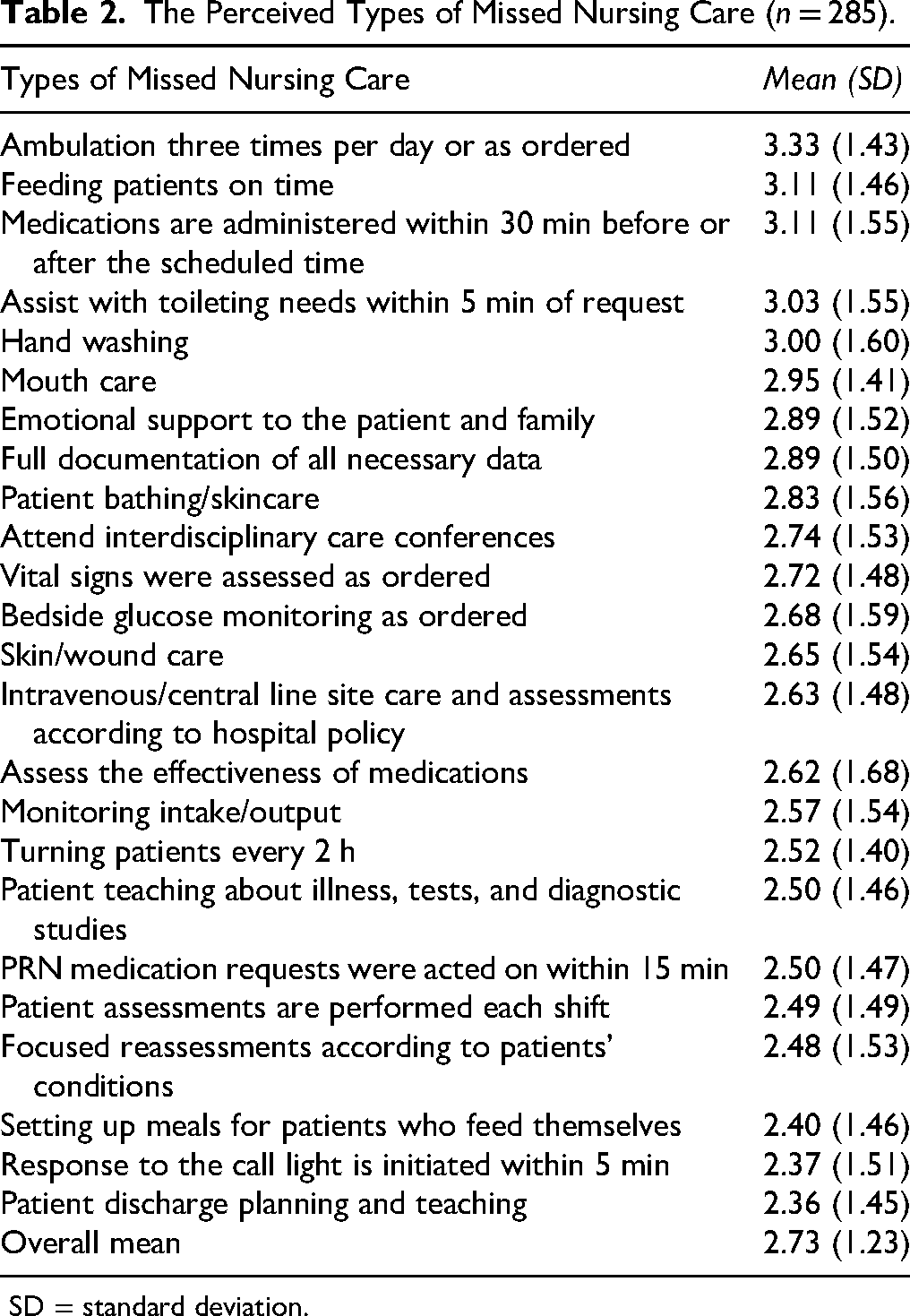
The three most frequently reported MISSNCARE types were as follows: ambulating patients three times per day or as ordered, feeding patients on time, and administering medications within 30 min before or after the scheduled time. On the other hand, the top least frequently reported MISSNCARE types were patient discharge planning and teaching, responding to call lights initiated within 5 min, and setting up meals for the patients who feed themselves. Detailed means and standard deviations for each type of MISSNCARE are listed in Table 2.
The Perceived Types of Missed Nursing Care (n = 285).
SD = standard deviation.
The Perceived Reasons for MISSNCARE
The results showed that the reasons for MISSNCARE were prevalent. The MISSNCARE scale had three subscales and was ranked as follows: 1: the labor resources (M = 3.40, SD = 0.60), 2: the material resources (M = 3.06, SD = 0.80), and 3: the communication reasons (M = 3.00, SD = 0.70). More specifically, the most important contributors to the labor resources were the inadequate number of staff and an occurrence of urgent patient situations. In contrast, the least contributor was the heavy admission and discharge activities and the inadequate number of assistive personnel.
Regarding the material resource reasons, the most crucial contributor was the unavailability of medications when needed, while the malfunctioning of supplies and equipment when needed was the least crucial contributor. Unbalanced patient assignments were the major contributor to the communication reasons, while the least influential factor was the failure of assistive personnel to communicate that care was not provided. Detailed means and standard deviations for each reason for MISSNCARE are listed in Table 3.
The Perceived Reasons for Missed Nursing Care (n = 285).

SD= standard deviation.
The Perceived Levels of EI
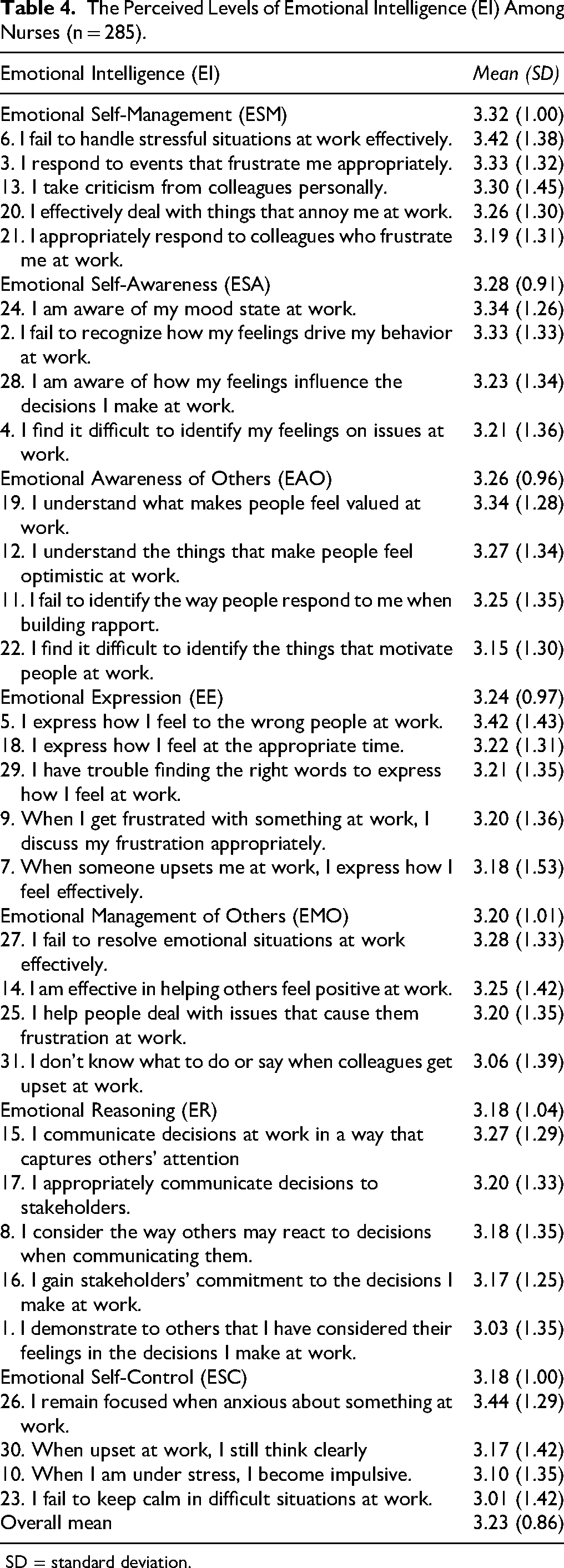
Descriptive statistics revealed that the total mean level of nurses’ EI was (Mean = 3.23, SD = 0.86 on a scale from 1 to 5). This result means that Jordanian nurses have a higher-than-average level of EI. Moreover, the highest mean for the subscales was observed in the ESM subscale (Mean = 3.32, SD = 1.00). Conversely, the ER and Emotional Self-Control (ESC) were shown to have the lowest means (Mean = 3.18, SD = 1.04) and (Mean = 3.18, SD = 1.00), respectively. Detailed means and standard deviations of items of RNs’ EI are listed in Table 4.
The Perceived Levels of Emotional Intelligence (EI) Among Nurses (n = 285).
SD = standard deviation.
The Relationships Between the Perceived Types of MISSNCARE and Levels of EI
Pearson's correlation test was used to investigate the relationship between the perceived types of MISSNCARE and levels of EI. The strength of correlations was assessed using Cohen's (1988) guidelines: correlations with r < .30 were classified as weak, those with r > .30 and < .50 as moderate, and those with r > .50 as strong in magnitude. The findings revealed a statistically significant, strong, negative correlation between the two variables (r = −.626, p < .05). This finding implies that nurses who perceived higher levels of EI reported lower levels of MISSNCARE activities. Because both EI and MISSNCARE were assessed through self-report measures, there is a risk of common method bias, which could overstate the strength of associations, even though statistical checks were applied to minimize this concern.
The Relationships Between the Perceived Types and Reasons for MISSNCARE, EI, and Background Variables
Significant positive weak correlations were found between nurses’ age and the perceived types of MISSNCARE activities (r = .120, p < .05) and the perceived reasons for MISSNCARE (r = .140, p < .05). Older nurses tended to perceive a higher frequency of MISSNCARE activities and reported more prevalent reasons for such occurrences. However, no significant correlations were observed between the age of nurses, years of experience in nursing, or years of experience in their current position and their levels of EI (p > .05).
In addition, there were positive weak correlations between the number of years of experience in nursing and the current position and the perceived reasons for MISSNCARE (r = .140, p < .05; r = .190, p < .05), indicating that nurses with greater experience in nursing and their current role tend to report more reasons for MISSNCARE.
The Differences in the Perceived Types and Reasons for MISSNCARE and EI
A statistically significant difference in the perceived MISSNCARE types was found based on nurses’ gender. Males significantly reported a higher incidence of MISSNCARE activities than females (t (283) = 3.544, p < .001). However, the ANOVA test found no differences in the perceived MISSNCARE activities based on marital status, level of education, or working unit (Table 1).
There were no statistically significant differences in the perceived reasons for MISSNCARE concerning gender, marital status, and level of education (Table 1). The perceived reasons for MISSNCARE differed regarding working units, as shown by the ANOVA test (F (7,277) = 3.601, p < .001). The Tukey post hoc test indicated that nurses working in intensive care units, operating rooms, pediatric units, surgical units, and other units reported more prevalent reasons for MISSNCARE than nurses working in the gynecology/obstetrics departments. In addition, nurses working in intensive care units reported more prevalent reasons for MISSNCARE than those who are working in emergency departments (Table 1). Furthermore, no significant differences were found between the groups regarding the perceived levels of EI based on gender, marital status, level of education, and working units (Table 1).
Predictors of MISSNCARE
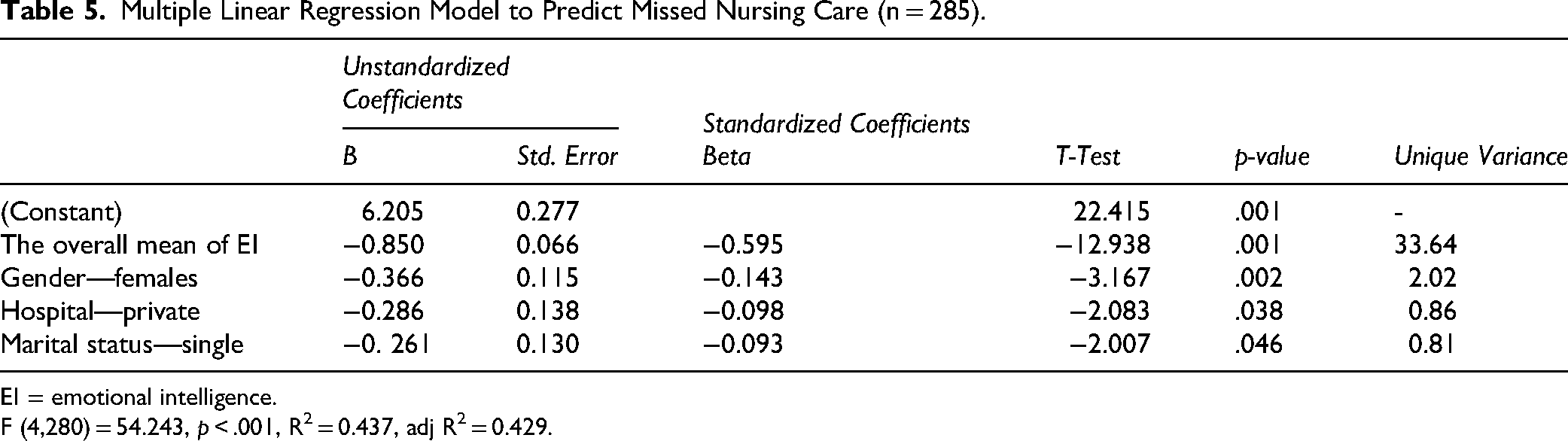
To assess the predictors of MISSNCARE, a backward multiple linear regression analysis was conducted. This method begins with all candidate variables and removes the least significant predictor at each step to produce a parsimonious model (Polit & Beck, 2017). The initial model included 19 predictors, including hospital type, gender, age, marital status, education level, nursing experience, experience in the current position, clinical unit, EI, and reasons for MISSNCARE. Dummy coding was applied to categorical variables using the most frequent category as the reference. Furthermore, the squared part correlation was computed to illustrate the unique variance explained by each factor. The final regression model was significant (F (4,280) = 54.243, p < .001) (Table 5), with 42.90% of the variance in MISSNCARE explained jointly as a function of EI, hospital type, gender, and marital status. It is essential to estimate the variance explained by EI alone; thus, the best way is to look at its standardized beta coefficient in Model 16. EI (MeanAll.E) has a standardized beta of −0.595, meaning that it has the largest effect among the predictors. The R² value for Model 16 is 0.437 (43.7%), which accounts for EI, hospital type, gender, and marital status. A reasonable estimate of EI's contribution is obtained by squaring its standardized beta coefficient: [\text{Variance explained by EI} = (−0.595)^2 = 0.354 (35.4%)]. Therefore, EI alone explains approximately 35.4% of the variance in MISSNCARE, while the remaining 8.3% (43.7%–35.4%) is attributable to hospital type, gender, and marital status.
Multiple Linear Regression Model to Predict Missed Nursing Care (n = 285).
EI = emotional intelligence.
F (4,280) = 54.243, p < .001, R2 = 0.437, adj R2 = 0.429.
To elucidate the contribution of each significant predictor, the results in Table 5 demonstrate that the most significant predictor was EI; this factor explains around 35% of the unique variance in MISSNCARE. In the same line, gender was ranked in second place, as the females reported lower MISSNCARE compared to male nurses, with 2.02% of the unique variance explained. Moreover, the hospital type demonstrated a significant predictor, revealing that the private hospitals reported lower MISSNCARE than the governmental hospitals, with 0.86% of the unique variance explained. Finally, marital status ranked the lowest, yielding that single nurses reported lower MISSNCARE than married nurses, with 0.81% of the unique variance explained (Table 5). A detailed analysis of the backward regression model predicting MISSNCARE was reported, as well as the detailed statistics of the initial model and the full regression model results, including the coefficients and p-values for all variables. All these details were provided as Supplemental Tables 6–8.
Since both variables were self-reported, raising the potential for common method variance (CMV), Harman's single-factor test was conducted using principal component analysis. The unrotated first factor accounted for 33.95% of the total variance, which is below the 50% threshold, suggesting that CMV was not a major concern (Podsakoff et al., 2003). A detailed analysis of the total variance explained from principal component analysis (Harman's single-factor test) is provided as Supplemental Table 9.
Discussion
This study studied the relationships between and differences in the perceived types and reasons for MISSNCARE activities and nurses’ levels of EI. Predictors of MISSNCARE were also measured.
The Perceived Types of MISSNCARE
The most frequently reported MISSNCARE activities were ambulating patients, feeding patients on time, and administering medications within the recommended time frame. These findings suggest that basic but time-consuming aspects of nursing care are the first to be compromised when workload increases, highlighting how task prioritization under pressure may unintentionally shift attention away from fundamental patient needs. The findings of the current study, especially regarding missed ambulating patients, are in line with previous research conducted in Jordan. Alfuqaha et al. (2023) and Al-Faouri et al. (2021) demonstrated a similar trend, indicating that patient ambulation had the highest mean score across all MISSNCARE items, pointing to the significance of the issue to nursing practice in Jordan. This finding may be justified by Jordanian nurses’ perception that patient ambulation is a less important task among their numerous responsibilities. Given RNs’ time and effort requirements, it underscores the crucial role of nursing assistants in carrying out such activities. Hosseini et al. (2023) identified patient education as the most frequently performed MISSNCARE activity, which is inconsistent with the current study findings but adds a broader context to the results.
The Perceived Reasons for MISSNCARE
Labor resources were the most common reason for MISSNCARE, followed by material and communication factors. This order aligns closely with the findings of Jordanian studies conducted by Alfuqaha et al. (2023), Al-Faouri et al. (2021), and Saqer and AbuAlRub (2018). The consistency in ranking across these studies underscores the significance of addressing challenges related to labor resources in the context of MISSNCARE, emphasizing its relevance for effective healthcare delivery in Jordan.
An inadequate number of staff was the predominant contributor to labor reasons, which is consistent with the findings of the Jordanian studies by Albsoul et al. (2023) and Alfuqaha et al. (2023), who found that the inadequate number of staff was the major contributor to labor reasons for MISSNCARE. Furthermore, these results are in line with the findings of the Iranian study by Hosseini et al. (2023), who found that the inadequate number of staff and urgent patient situations were the two major reasons for MISSNCARE. This result highlights that the issue of the nursing shortages is a global concern that needs to be addressed. Contrastingly, Khrais et al. (2023) found that communication reasons were the major contributor to MISSNCARE in their study, followed by labor resources and material resources. This discrepancy emphasizes the importance of considering communication patterns to enhance healthcare delivery across organizations, not only relying on labor and material resources.
The Perceived Levels of EI
The majority of the participants have high levels of perceived EI, which is consistent with Al-Oweidat et al.'s (2023) findings. Earlier investigations into Jordanian nurses’ EI by Al-Hamdan et al. (2021) revealed moderate levels, suggesting a noteworthy increase in EI perceptions among Jordanian nurses. A reasonable explanation for this progression is the potential evolution of training programs and educational curricula, possibly emphasizing the enhancement of EI skills among nurses. As indicated by Mao et al. (2021), training programs have been recognized as instrumental in enhancing EI. Additionally, individual differences regarding personal characteristics, as highlighted by Castelino and Mendonca (2021), may play an important role in the observed increase, emphasizing the significance of considering the unique attributes of each nurse in understanding the development of their EI.
The Relationships Between the Studied Variables
The negative correlation between EI and MISSNCARE suggests that EI can buffer against staffing shortages by enabling nurses to manage stress, prioritize tasks effectively, and maintain patient-centered care even under pressure, indicating that nurses with higher EI are more effective at handling stress, balancing workload pressures, and staying attentive to patient needs despite limited resources. Practically, nurses with strong EI are likely to handle high-pressure situations more effectively. They can use emotional regulation to keep their cool, show empathy to build strong relationships with patients, and employ social skills to work well with their colleagues. This adaptability can help offset staffing shortages by fostering more resilient behaviors (Powell et al., 2024; Singh, 2025). This positions EI as more than an individual attribute; it serves as a protective factor that can help mitigate the impact of broader systemic issues such as staff shortages, thereby reinforcing previous research that associates higher EI with enhanced caregiving (Lee & Kim, 2021) and increased job satisfaction (Qin et al., 2023).
Drawing on Salovey and Mayer's (1990) model, EI encompasses the ability to perceive, regulate, and use emotions effectively. These skills enable nurses to cope with stress, prioritize tasks, and stay responsive to patient needs. In this way, EI can act as an intermediary against the pressures of limited staffing and high workload, thereby reducing the likelihood of MISSNCARE. The observed correlation reinforces the idea that EI is tied to fewer care omissions, underscoring its importance in both individual and organizational efforts to enhance nursing outcomes (Zhang et al., 2025). This research contributes to the existing body of literature by emphasizing the role of EI in minimizing care omissions. The model proposed by Kalisch et al. (2009) supports this relationship, highlighting the impact of nurses’ internal processes on the quality of care.
Older nurses indicated a higher incidence of MISSNCARE, which is consistent with findings from Al-Faouri et al. (2021) and Khrais et al. (2023); however, Labrague et al. (2022) did not observe such a correlation in the Philippines. This result could reflect adaptation challenges to current work demands, heavier workloads, or slower adjustment to technological or procedural changes in the healthcare settings. In line with previous studies (Al-Faouri et al., 2021; Labrague et al., 2022), no significant relationship was identified between MISSNCARE and either the number of years of experience or the current job position.
Differences in the Perceived Types and Reasons for MISSNCARE
Despite similar experience levels, nurses vary in their ability to manage workload and prioritize tasks. In this study, male nurses reported more MISSNCARE than females, a finding inconsistent with previous research (Al-Faouri et al., 2021; Labrague et al., 2022). This finding may reflect differences in task perception, reporting behavior, or cultural norms around caregiving roles.
Contrary to earlier findings, no variation was observed based on marital status, education, or unit type, although Al-Faouri et al. (2021) reported higher MISSNCARE among married nurses and lower rates in critical units. This result suggests that organizational factors, such as workload and time constraints, may be more influential than personal demographics. Unit-specific differences were noted, with gynecology/obstetrics nurses reporting fewer reasons for MISSNCARE, possibly due to the unique demands of their specialty.
Regarding EI, no correlation with age was found, aligning with Al-Hamdan et al. (2021). However, Raeissi et al. (2019) found higher EI among older nurses, likely due to greater life experience. In Jordan, limited career advancement and challenging work conditions may hinder EI development among older nurses.
Differences in the Perceived EI
Consistent with prior Jordanian studies, no significant correlation was found between nurses’ experience and EI levels (Al-Oweidat et al., 2023; Al-Hamdan et al., 2020, 2021). In contrast, international studies reported higher EI among more experienced nurses, suggesting that workplace challenges in Jordan may hinder EI development (Mansel & Einion, 2019; Mao et al., 2021; Raeissi et al., 2019). Similarly, gender showed no significant differences in EI across studies (Al-Hamdan et al., 2021; Ma et al., 2022), implying that individual and social factors may be more influential (Ireland, 2022).
Regarding marital status, findings were mixed. While this study and others found no impact (Al-Hamdan et al., 2020, 2021), some reported higher EI among widowed or married nurses, possibly due to contextual factors (Al-Oweidat et al., 2023; Moradian et al., 2022).
Educational background also showed inconsistent results. Some studies found no differences (Moradian et al., 2022; Raeissi et al., 2019), while others reported higher EI among more educated nurses (Al-Oweidat et al., 2023; Al-Hamdan et al., 2020, 2021), potentially due to variations in measurement tools and interpretation. Finally, no significant differences in EI were found across working units in this study and others (Moradian et al., 2022), though some reported higher EI in emergency and pediatric departments, highlighting the role of unit-specific demands and organizational support (Al-Hamdan et al., 2021; Ma et al., 2022).
Predictors of MISSNCARE
Regression analysis revealed that EI, hospital type, gender, and marital status jointly explained 43% of the variance in MISSNCARE, with EI alone accounting for 35%. This result underscores the critical role of emotional skills in reducing care omissions and suggests that EI training could enhance patient care alongside organizational improvements. Consistent with prior studies, female, single nurses and those in private hospitals reported fewer MISSNCARE incidents (Al-Faouri et al., 2021; Saqer & AbuAlRub, 2018). Conversely, married nurses reported more, possibly due to competing personal responsibilities. However, lower MISSNCARE rates in private hospitals may reflect underreporting due to fear of repercussions (Albsoul et al., 2023). These findings highlight the need for open communication and trust to foster safe, transparent care environments.
Strengths and Limitations of the Study
The present study showcases several significant strengths that enhance its contribution to nursing research and practice. By investigating the connection between EI and MISSNCARE within the context of Jordanian healthcare, the study provides culturally pertinent insights that are frequently neglected in international literature. It utilizes validated tools with high reliability, ensuring thorough data collection. The inclusion of a substantial sample size with an impressive response rate of 95% enhances the credibility of the findings. Additionally, the study recognizes EI as a key predictor of MISSNCARE, accounting for 35.40% of the variance, and emphasizes the potential benefits of EI training in enhancing patient outcomes. Guided by the MISSNCARE Model, the research incorporates both organizational and individual elements, presenting practical recommendations for nursing education, leadership, and policy formulation.
Notwithstanding the importance of the study, it is essential to acknowledge several methodological limitations. Additionally, nurses’ self-reported EI scores may be influenced by cultural norms in Jordan regarding the expression and regulation of emotions, which could affect the interpretation of the findings. Furthermore, the self-reported nature of MISSNCARE raises questions about the accuracy of recall. The cross-sectional design restricts the ability to draw causal conclusions between MISSNCARE and EI. At the same time, the use of convenience sampling from a single region in Jordan and the omission of the military sector diminish the generalizability of the findings. Moreover, the emotional self-awareness subscale exhibited low internal consistency (α = 0.63), which may impact the reliability of the EI assessment. Additional research is necessary to determine whether this low consistency indicates content-related issues or difficulties in evaluating emotional self-awareness.
Implications and Recommendations for Practice and Education
Future studies ought to implement more stringent methodologies, such as randomized controlled trials, and expand inclusion criteria to encompass experienced nurses and those working in military hospitals, thereby enhancing the generalizability of the results. Given the strong negative correlation between EI and MISSNCARE, investing in EI development is essential. Targeted training, such as workshops on emotional self-awareness and regulation, can help nurses manage stress and reduce care omissions. At the same time, broader EI education supports clinical decision-making and interpersonal effectiveness (Mao et al., 2021).
Operational improvements are also needed. Structured ambulation schedules and additional personnel could address the frequent omission of patient ambulation. Addressing labor shortages through optimized nurse-to-patient ratios and recruitment initiatives is vital to reducing systemic barriers to care (Kalisch et al., 2009). Leadership plays a key role. Nurse managers can foster EI through peer-led seminars, and emotionally intelligent leadership can promote a healthier work environment. Finally, integrating EI into nursing curricula prepares future nurses with essential interpersonal skills. Recognizing gender differences in EI may further guide targeted training and professional development, fostering resilience, collaboration, and improved patient outcomes.
Conclusions
Although nurses reported elevated levels of EI, they also indicated higher-than-average instances of MISSNCARE, with the ambulation of patients being the task most often neglected. This observation underscores significant opportunities for enhancement in research, clinical practice, administration, and education. Labor shortages were identified as the primary factor contributing to this issue, which may help in pinpointing the necessity for policy-level interventions to bolster workforce capacity. The pronounced negative correlation between EI and MISSNCARE may imply that improving EI can reduce care omissions, indicating its potential as a modifiable factor in improving nursing practice, thereby promoting more effective and attentive nursing practices, which may help reduce MISSNCARE events, promote more effective nursing practices, and enhance patient outcomes.
Supplemental Material
sj-docx-1-son-10.1177_23779608251394291 - Supplemental material for The Perceived Types and Reasons for Missed Nursing Care Activities and the Levels of Emotional Intelligence Among Nurses: A Cross-Sectional Study
Supplemental material, sj-docx-1-son-10.1177_23779608251394291 for The Perceived Types and Reasons for Missed Nursing Care Activities and the Levels of Emotional Intelligence Among Nurses: A Cross-Sectional Study by Thara’ S. Bani-Baker, Majd T. Mrayyan, Ibrahim G. Al-Faouri and Raeda F. AbuAlRub in SAGE Open Nursing
Supplemental Material
sj-docx-2-son-10.1177_23779608251394291 - Supplemental material for The Perceived Types and Reasons for Missed Nursing Care Activities and the Levels of Emotional Intelligence Among Nurses: A Cross-Sectional Study
Supplemental material, sj-docx-2-son-10.1177_23779608251394291 for The Perceived Types and Reasons for Missed Nursing Care Activities and the Levels of Emotional Intelligence Among Nurses: A Cross-Sectional Study by Thara’ S. Bani-Baker, Majd T. Mrayyan, Ibrahim G. Al-Faouri and Raeda F. AbuAlRub in SAGE Open Nursing
Supplemental Material
sj-docx-3-son-10.1177_23779608251394291 - Supplemental material for The Perceived Types and Reasons for Missed Nursing Care Activities and the Levels of Emotional Intelligence Among Nurses: A Cross-Sectional Study
Supplemental material, sj-docx-3-son-10.1177_23779608251394291 for The Perceived Types and Reasons for Missed Nursing Care Activities and the Levels of Emotional Intelligence Among Nurses: A Cross-Sectional Study by Thara’ S. Bani-Baker, Majd T. Mrayyan, Ibrahim G. Al-Faouri and Raeda F. AbuAlRub in SAGE Open Nursing
Footnotes
Acknowledgments
The researchers would like to thank all participants for their input in the current study.
Ethical Approval
The study was conducted according to the guidelines of the Declaration of Helsinki. The ethical approvals for this study were obtained from multiple authorities, including the Institutional Review Board (IRB) committee at the Jordan University of Science and Technology (JUST) (IRB No. 3/163/2023 dated August 30, 2023), as well as the Ministry of Health (MoH) (IRB No. MOH/REC/2023/396 dated October 11, 2023) and the selected hospitals.
Consent for Publication
This article includes data obtained from individual participants. Written informed consent for publication was obtained from all participants. All authors hereby give their consent for the publication of the article, including all associated data published by Sage Publications.
Authorship Statement
The authors listed meet the authorship criteria according to the latest guidelines of the International Committee of Medical Journal Editors, and the authors agree with the content of the manuscript. The authors have approved the content before submission or resubmission.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability and Materials
The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Reporting Method
The authors of this manuscript have adhered to the STrengthening the Reporting of OBservational Studies in Epidemiology (STROBE) checklist, which was used to guide the study.
Use of AI Software
During the preparation of this work, the authors used Grammarly and Copilot for editing and condensing paragraphs to decrease the number of words, paraphrasing, and plagiarism checks. After using these tools, the authors reviewed and edited the content as needed and took full responsibility for the content of the publication.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.