
Abstract
Introduction
Certain cultural practices after childbirth can significantly harm the health of both mothers and their babies. The impact of these practices can differ from one region to another.
Objective
This study explored the harmful cultural customs that occur during the postpartum period, as well as the reasons behind them, among women with infants younger than 12 months.
Methods
This study employed a phenomenological qualitative approach to explore instances of cultural malpractice during the postpartum period. Data were collected through in-depth interviews conducted between July 1 and 7, 2024. Nine postpartum individuals were purposefully selected to participate, ensuring representation of a range of experiences and perspectives relevant to the research question. The sample size was determined by the point of data saturation. An interview guide was used to structure the interviews.
Results
The study highlighted important postpartum practices and beliefs that shape care for newborns and mothers. Postpartum women usually shower for the first time three or four days after delivery. Sexual activity typically resumes around the same time. Cultural beliefs influence showering practices, and spicy chillies are avoided. The study highlighted the impact of cultural beliefs, traditional rituals, and the significance of community support.
Conclusions
Actively engaging families and communities to enhance health education and support is strongly recommended to prevent the adverse effects of risky postpartum malpractices.
Introduction
Since 2000, maternal deaths worldwide have dropped from 339 to 223 in 2020, a 34% reduction. However, sub-Saharan Africa and southern Asia account for 87% of these deaths, with 70% in sub-Saharan Africa. Ethiopia has 267 maternal deaths per 100,000 people. Urgent action is needed to meet the 2030 goal of 70 deaths per 100,000 live births (World Health Organization, UNICEF, 2023).
One of the contributing causes of maternal death is cultural malpractice, which causes 5% to 15% of deaths (Hailu et al., 2023; Melesse et al., 2021; Say et al., 2014).
Cultural malpractice refers to the shared practices or beliefs within a society that adversely affect maternal health. This phenomenon is seen in various forms across different countries and regions around the globe (Diro & Fufa, n.d.; Hailu et al., 2023; Melesse et al., 2021).
Ethiopia has a long history, a unique culture, and many cultural practices that continue to be observed today. However, it is a nation where many cultural customs surrounding childbirth, pregnancy, and postpartum care are popular (Kitila et al., 2018).
Cultural practices that are harmful to the health of pregnant women and their unborn babies include taboo food, drinking “Telba,” giving abdominal massages, and consuming “Kosso” (Abebe et al., 2021; Gedamu et al., 2018; Hailu et al., 2023); childbirth (abdominal and uterine massage); giving birth at home supported by untrained traditional birth attendants; using an unclean blade to cut the umbilical cord; and using an unclean thread to tie the umbilical cord (Abebe et al., 2021; Gedamu et al., 2018; Hailu et al., 2023; Melesse et al., 2021).
In Ethiopia's Amhara regions, childbirth traditions to expedite labor involve practices such as opening items found in the home, losing the husband's belt, reflecting in a mirror, carrying the laboring woman over water, roasting barley three times, preparing coffee multiple times, circling a white chicken around the mother's head three times, and massaging the mother's belly with butter, among others (Aynalem et al., 2023).
Review of Literature
After childbirth, women focus on caring for their babies and healing while also engaging in practices that may affect their health and their infants’ health (Moola et al., 2020).
The common harmful cultural practices that are also exercised during the postpartum period are the restriction of certain foods that may be nutritious, the provision of prelacteal feed (commonly honey and sugar water), delayed initiation of breastfeeding, discarding of colostrum, unhygienic practices related to cord care and personal hygiene, limiting exercise, and washing the baby immediately (Gedamu et al., 2018; Moola et al., 2020; Venkateswarlu et al., 2019).
In Northwest Ethiopia, women have unique beliefs about childbirth. They think placing cow dung under them and using a butter-smeared spindle helps deliver the placenta. Husbands shooting guns is believed to reduce postpartum bleeding (Aynalem et al., 2023).
Harmful cultural practices during pregnancy and after birth are common in Ethiopia. These practices differ across regions, but a study in Meshenti Town found that 76.1% of mothers practiced them (Gedamu et al., 2018). In Dire Dawa, 41.5% of women reported harmful practices (Hailu et al., 2023); in Wonago, 29% admitted the same (Kassahun et al., 2019). In the Gurage Zone, 71.4% of respondents acknowledged engaging in some form of harmful cultural practice during the perinatal period (Abebe et al., 2021). These results highlight the need for specific interventions to tackle these issues.
Harmful cultural practices during pregnancy, childbirth, and postpartum are linked to several factors. Older women (35+) are twice as likely to engage in them compared to younger women. Cultural endorsement significantly increases the likelihood, as does a lack of formal education. Absence of health education sessions and rural residency also contribute. Key predictors include low awareness of negative consequences and lack of antenatal care during pregnancy (Abebe et al., 2021; Hailu et al., 2023; Kassahun et al., 2019). These combined factors highlight vulnerable groups needing targeted interventions to reduce harmful practices.
The separation of beneficial cultural practices (feeding mothers with a special type of sugar tea or porridge) should be promoted, whereas harmful cultural practices (restrictions of some food items, cutting of umbilical cords with unsterile materials, delaying breastfeeding, and avoiding colostrum feeding) should be discouraged (Aynalem et al., 2023; Moola et al., 2020).
Despite their significant harm to both mothers and newborns, few investigations have attempted to identify the significant reasons why women practice these harmful practices. Owing to the practice's magnitude, type, and cultural variations among different regions, few studies (Abebe et al., 2021; Aynalem et al., 2023) have explored the beliefs behind cultural malpractice during the postpartum period in this area. As a result, the goal of this study was to explain cultural malpractices during the postpartum period in the Shebedino District, as well as the factors that contribute to them.
Methods
Study Setting and Period
The study was conducted between July 1 and 7, 2024, in Shebedino District, which is located in the Sidama Regional State of Ethiopia. It is located 27 km from Hawassa, the regional capital. Shebedino District comprises 25 rural kebeles and five urban kebeles. With a population of 241,581 and a significant reproductive-age population of 56,288, the majority of Shebedino residents are Sidama, speaking the Sidamu Affoo language. The district boasts one primary hospital, six health centers, and 23 health posts.
Study Design, Participants, and Sampling Procedure
This study used a phenomenological qualitative approach to explore and understand cultural practices during the postpartum period in the Shebedino districts of the Sidama region in Ethiopia. The study focused on women who had given birth at least once in the past 12 months. The participants were purposefully selected, meaning that they were chosen because they represented the range of experiences and perspectives relevant to the study. Women who had given birth within the past year and lived in the study area for at least 6 months were included, whereas women who had a serious medical illness and were in the immediate postpartum period (right after giving birth) were excluded.
The number of participants (nine) was determined on the basis of “saturation,” meaning that the researchers continued interviewing participants until they were no longer receiving new information. The participants were carefully chosen on the basis of their ability to represent the study's focus on cultural practices. Before the interviews, the researchers ensured that each participant understood the study and agreed to participate (informed consent). The interviews were conducted in a conversational style, moving from general to specific questions and from easier to more difficult topics. The participants were encouraged to speak freely, and the wording and order of the questions were adjusted to be culturally appropriate and sensitive to the participants’ feelings.
Operational Definition
Cultural malpractice means the common beliefs or practices in a community that negatively impact the health of mothers and newborns (Hailu et al., 2023).
Data Collection Tools and Procedures
Data were collected through in-depth interviews. These interviews were guided by a semistructured interview guide, allowing for some flexibility in the conversation. The interviewer and a note-taker discussed each question before the interview to ensure that they were both on the same page. Face-to-face interviews were conducted in person, allowing the interviewer to observe nonverbal cues from the participants and providing a richer understanding of their responses. The interview guide included questions with probes to help steer the conversation in a specific direction while still allowing for a natural flow.
The interviews were recorded to ensure accurate transcription for analysis. Additional notes were taken to capture important information that might not be captured on audio. The interviews were conducted at times and locations that were convenient for the participants, ensuring that they felt comfortable and at ease. The interviews were conducted by three public health experts trained in qualitative research. Each interview lasted between 30 and 60 min and took place in the morning in stable areas at the home of participants.
Trustworthiness
Credibility: To preserve data source triangulation, in-depth, and key informant interviews were conducted in a confidential and comfortable setting among those participants who had a history of childbirth within the past 12 months and their husbands. The audiotape was transcribed word-for-word in Amharic before being translated into English. On the same day, data transcription and analysis were completed.
Dependability: Reviewing the audio recording and writing notes helped to confirm the manual transcription. The procedures for data collection, processing, and study findings were assessed by people who did not participate in the data analysis.
Transferability: The investigator provided many details to explain the entire research procedure, from data collection to the final report.
To achieve conformability to eliminate bias throughout data collection, coding, and analysis, the researcher reflected on and examined prior personal expectations and experiences. The participants’ words were used instead of the researchers’ opinions and biases.
Data Analysis and Management
Data collection and analysis were carried out concurrently. To discover new concepts and categories, the data were evaluated immediately after the key informant interview. After frequently listening to the tape recorder to grasp each respondent's concepts, the audio record data were transcribed verbatim in Amharic for each interview at the same time. The data are translated into English and written down. The translated data were imported into qualitative data analysis via the value-coding method. The data were analyzed via the inductive approach, and an interpretive phenomenological analysis was performed. Twenty-one codes were grouped together on the basis of their resemblance, subthemes and categories were created, and a sample quotation was selected for reporting.
Results
Mothers’ Sociodemographic Characteristics
A total of nine female key informants were recruited for this study. The mean age of the informants was 28.8 years, with a standard deviation of 1.51, ranging from 23 to 35 years. Five participants were between 20 and 30 years old. Six participants were rural residents. All participants were married and Sidamu in their ethnicity (Table 1).
Sociodemographic Characteristics of Participants in Sidama, Ethiopia.

Cultural Malpractice During the Postpartum Period
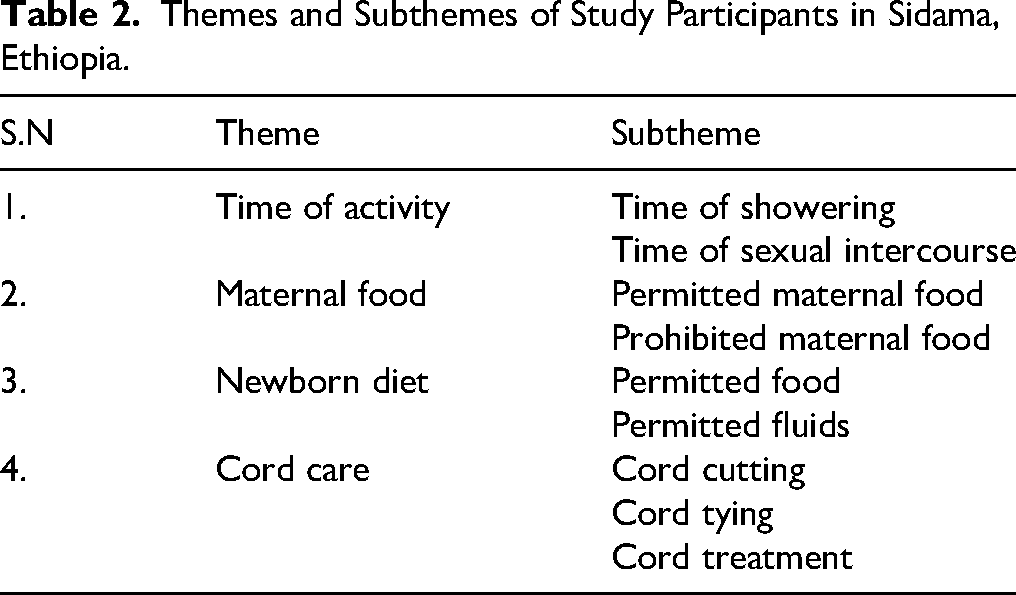
The study was conducted among nine women in the Sidama region, Ethiopia, using a qualitative study. The study categorizes these practices into four main themes and nine subthemes (Table 2).
Time of showering and sexual intercourse
Showering: postpartum women typically take their first shower on the third or fourth day following delivery. Sexual intercourse: sexual activity is generally resumed on the third or fourth day following delivery. Permitted and prohibited maternal food
Permitted foods: common postpartum foods for mothers include telba, atimit, blood from goats or other animals, a glass of butter, sweet foods, and dry foods. Prohibited foods: some homemade foods are restricted during the postpartum period. Newborn diet
Permitted foods and fluids: newborns are typically given Amessa, butter, cow milk, and water. Cord care
Cord tying: the umbilical cord is typically left untied. Cord cutting: the cord is often cut with unsterile materials. Cord treatment: various substances are applied to the cord.
Themes and Subthemes of Study Participants in Sidama, Ethiopia.
Time of Showering and Sexual Intercourse
The practice of showering after childbirth is deeply rooted in cultural beliefs. “After delivery, neighbours come together on the third or fourth day for a ceremony. They prepare water for a shower and “Sherko” or “Porridge” for the mother. A 31-year-old woman.” (31-year-old woman) “Waiting up to the third or fourth day to take a shower has cultural importance, as it is not allowed to do so earlier due to norms of culture.” (35-year-old woman)
Maternal Diet for Postpartum Mothers
Foods claimed to assist postpartum moms include porridge, a glass of filtered butter, and blood from goats and cows collected during their slaughter. “The butter will be produced in a glass and filtered before being consumed. It is thought to fortify her and replenish the blood lost during childbirth.” (36-year-old participant) “Postpartum women use telba and sinafic to avoid bleeding after birth; despite being prohibited during pregnancy, telba and atimit are said to minimize vaginal bleeding after birth.” (27-year-old woman)
Traditional foods like “Kolo,” “Kita,” “Bulla,” and “Baso” are often avoided during the postpartum period; they are believed to cause constipation, decreased breast milk production, and abdominal pain in both mothers and infants. Additionally, spicy chillies are also believed to cause burning sensations in the abdomens of both mothers and newborns. “In our culture, foods such as cabbage are prohibited because they cause abdominal pain in babies if mothers eat them.” (25-year-old participant) “Foods such as ‘chilli’ are not allowed after delivery since they cause a burning sensation for both the mother's and newborn's abdomens.” (26-year-old participant) “It is not recommended for postpartum mothers to consume ‘Kolo’ or ‘Kita’ since they are believed to induce constipation and reduce the amount of breast milk.” (21-year-old woman)
Diet for Newborns and Infants
“Amessa” is a popular traditional remedy given to newborns in the region, with almost all respondents highlighting its importance. The primary reason for administering “Amessa” is to prevent “Fancho,” a condition characterized by symptoms such as changes in bowel sounds, bulging fontanels, weight loss, abdominal pain, skin rash, bloating, and decreased appetite. “There are around seven types of ‘Amessa’ species. The preparation involves heating the ‘Amessa’ leaves with water and then giving the neonate three cups per day, starting from the first day of delivery.” (29-year-old participant) ‘‘(Fancho) is a disease that can be prevented by giving ‘Amessa’. It manifests as a change in bowel sounds, bulging fontanels, weight loss, abdominal pain, skin rash, bloating, and decreased appetite.” (29-year-old participant) “Fancho is a hereditary disease that can appear in neonates if the parents have a history of using ‘Amessa’ and the baby does not receive it.” (Another description of a 33-year-old participant) “If the parents have a history of using ‘Amessa’, giving it to the baby is mandatory to prevent Fancho. The feared complication of Fancho syndrome is death.” (27-year-old participant)
Colostrum, the first milk produced after delivery, is often prohibited because of concerns about its potential negative effects on baby health. It is believed to cause a loss of appetite and decreased weight gain. “Colostrum should not be given to the baby because it is yellow. It makes the baby lose his appetite and makes him thin.” (33-year-old participant said)
Cord Care
Many participants reported that they often use unsterile materials to cut cords because they don’t see a link between infection and the unclean blades purchased from stores. Additionally, some individuals reuse blades before cutting the cord. “In some emergency cases, if the new blade is not available at home, we will use the blade that was used before to cut the cords.” “We didn't tie the cord because bleeding will stop quickly. Various substances such as Vaseline, butter, dung, and soil are applied on the cord, believed to dry and remove the remaining cord.” (27-year-old woman) “Different types of substances, such as Vaseline, butter, dung, and soil, which are very common on the cord because they are believed to dry rapidly and prevent cord infection.” (29-year-old participant)
Discussion
Harmful cultural practices during pregnancy, childbirth, and the postpartum period contribute to maternal deaths and endanger newborns. These practices, particularly those occurring after childbirth, can negatively impact a mother's mental health, violate her human rights, and lead to infections and even death in newborns. The complexity arises from the variation of these practices across different communities. Therefore, identifying and understanding harmful practices in various regions is crucial. This study aimed to explore cultural malpractices and their underlying rationales in the Shebedino district of the Sidama region, Ethiopia.
In this study, the practice of bathing after childbirth typically occurred after 3 or 4 days. While a qualitative study in Uttarakhand, India (Saxena et al., 2020), suggested a delay of 6 days for baby girls and 5 days for baby boys, this practice is based on cultural acceptance. However, health recommendations encourage mothers to bathe anytime they feel ready. Community health workers play a crucial role in raising awareness about the importance and timing of postpartum bathing.
A common practice observed in this study is the recommendation of porridge for postpartum mothers. This aligns with findings from studies in northern Maputaland, South Africa (Ramulondi et al., 2021), and East Gojjam Zone, Ethiopia (Aynalem et al., 2023). Porridge is believed to help restore strength, increase blood volume, and promote lactation.
Additionally, postpartum mothers are encouraged to consume filtered butter and blood from goats and cows collected during slaughter. This practice, also observed in East Gojjam, Ethiopia (Aynalem et al., 2023), aligns with the belief that the postpartum period is a time of celebration for the mother, family, and community, often marked by the slaughter of a sheep, goat, or hen for cultural ceremonies. One participant explained, “If the postpartum woman's family is well-off, they may slaughter a goat or cow, collecting the blood that flows from the animal's neck for the mother to drink as soon as possible.” This practice is believed to help strengthen the mother after childbirth, replenishing the blood lost during delivery. A previous study supported this belief, emphasizing the importance of strengthening postpartum mothers (Withers et al., 2018).
In this study, there was a practice of prohibiting foods such as banana, cabbage, potato, kita, bulla, and baso. This aligns with findings from a study in India, which restricted certain foods on the basis of their perceived temperature, classifying them as “hot” (e.g., papaya) or “cold” (e.g., oranges, bananas, buttermilk, and beans) (Moola et al., 2020; Saxena et al., 2020). The belief is that consuming certain foods can lead to colds or excessive body heat in women.
Colostrum feeding was avoided or not practiced in this study, aligning with findings from the Gurage Zone, Southern Ethiopia, where nearly one-third of participants discarded colostrum (Abebe et al., 2021). Some practices even delay the early initiation of breastfeeding, believing that colostrum becomes indigestible and causes vomiting (Moola et al., 2020).
However, colostrum is an essential form of breast milk that is rich in nutrients and is recommended for use within the first hour after childbirth. The International Federation of Gynaecology and Obstetrics (FIGO) encourages breastfeeding during the first hour of life, known as the “golden hour,” as a protective and life-saving intervention (FIGO, 2023). Community and healthcare facility workers require counseling about the importance of colostrum feeding and the early initiation of breastfeeding.
This study identified practices related to umbilical cord care, highlighting two key areas of concern. Some participants used old razor blades to cut the cord, echoing findings in the Gurage Zone of Southern Ethiopia, where 44.6% of mothers employed unclean blades (Abebe et al., 2021). While current practice often delays cord clamping, scientific evidence strongly recommends delaying it for 60 to 120 s, even in emergencies, to significantly reduce neonatal mortality and morbidity and improve hematological outcomes (McDonald et al., 2022). Behavioral change messages and counseling are crucial to address these practices.
Additionally, the participants applied various substances, such as dung, soil, and Vaseline, to the umbilical cord. While these practices differ across cultures and even within regions, they are generally intended to promote healing, accelerate cord separation, or protect the baby from perceived harm, such as “bad spirits,” the cold, or the air (Coffey & Brown, 2017).
A prevalent indigenous practice in this community involves administering “Amessa” to newborns. “Amessa” is a local term for an herbal remedy prepared from the leaves of a specific tree. Experienced women, known as “Amessama,” crush the leaves and mix them with cold water, giving the newborn a cup three times a day for at least 6 months, sometimes up to 12 months if the newborn has health problems. The community believes that “Amessa” prevents “Fancho,” a local term for a condition characterized by changes in bowel sounds, bulging fontanels, weight loss, abdominal pain, and skin rash.
Postpartum recovery is unique; thus, personalized medical advice is crucial for resuming sexual activity safely. Conversely, some cultural practices disregard a woman's autonomy and physical readiness, dictating sex as early as day 3 or 4 postpartum. This timing, sometimes vary by the newborn's sex, primarily aims to confirm the father's paternity as an act of ownership, often publicly announced. These deeply ingrained norms regrettably promote harmful stereotypes and violate women's consent and bodily autonomy. Crucially, such practices contradict scientific evidence, which recommends 4 to 6 weeks abstinence for healing and up to 6 months for full recovery. This period prevents potential sexual dysfunctions like pain or decreased desire and satisfaction. Empowering women to make informed decisions about their bodies and sexual health is paramount (Grussu et al., 2021).
Postpartum sexual intercourse, while a specific event, significantly impacts an individual's lifelong sexual and reproductive health. Comprehensive sexual education, as recommended by UNFPA for people at all stages of life, plays a crucial role in ensuring positive outcomes during and after this period (Population, U. (United) N, 2022).
Strengths and Limitations
As a qualitative study, it offers a more profound understanding of cultural malpractices in the area. However, these studies may have limitations, including reliance on the accuracy of participant recall and small sample sizes that limit the generalizability of the findings to broader populations.
Implications for Practice
This study helps policymakers consider the useful and harmful aspects of cultural practices. Therefore, a multifaceted approach, including health education, policy re-evaluation, and community engagement, is crucial for mitigating the negative impacts of harmful cultural practices.
Conclusion and Recommendations
Childbirth practices in Sidama, Ethiopia, reveal concerning cultural practices that put mothers and newborns at risk. Practices like withholding colostrum, providing inappropriate foods and fluids to newborns, and risky postpartum practices like early sexual intercourse, delayed showering, unsterile cord care, and substance application to the umbilical cord are rooted in cultural beliefs. These practices often lack scientific evidence and can negatively impact health.
In order to improve maternal and child healthcare, the zonal health bureau should provide nutrition education and encourage early and exclusive breastfeeding. In order to support comprehensive healthcare services that improve maternal health outcomes by empowering women, bringing intersectoral collaboration, and implementing individualized services, active stakeholder engagement, including that of women, families, community leaders, donors, and healthcare providers, is advised. It is recommended that other researchers conduct further studies.
Supplemental Material
sj-docx-1-son-10.1177_23779608251393761 - Supplemental material for Cultural Malpractice During the Postpartum Period: A Qualitative Study in Sidama, Ethiopia
Supplemental material, sj-docx-1-son-10.1177_23779608251393761 for Cultural Malpractice During the Postpartum Period: A Qualitative Study in Sidama, Ethiopia by Misgana Desalegn Menesho, Abebaw Abeje Muluneh, Belda Negesa Beyene and Andergachew Kassa Biratu in SAGE Open Nursing
Supplemental Material
sj-docx-2-son-10.1177_23779608251393761 - Supplemental material for Cultural Malpractice During the Postpartum Period: A Qualitative Study in Sidama, Ethiopia
Supplemental material, sj-docx-2-son-10.1177_23779608251393761 for Cultural Malpractice During the Postpartum Period: A Qualitative Study in Sidama, Ethiopia by Misgana Desalegn Menesho, Abebaw Abeje Muluneh, Belda Negesa Beyene and Andergachew Kassa Biratu in SAGE Open Nursing
Footnotes
Acknowledgments
The authors would like to express our special thanks to Hawassa University, supervisors, study participants, and data collectors for their continuous support throughout the work.
Ethical Approval
Ethical approval was obtained from the Hawassa University Research and Community Service Directorate (Ref no: IRB/194/14). The study was ethically approved by the research organizing and approving committee of the health science college. All methods were carried out following the relevant guidelines and regulations of Hawassa University. Written informed consent was obtained from the study participants, and the respondents were informed about the purpose of the study and the confidentiality of all the information, with no personal identification left on the questionnaire.
Author Contributions
MDM was involved in conceptualization, methodology, software, formal analysis, investigation, and writing of the original draft. AKB and AAM contributed to the conceptualization, methodology, supervision, and investigation of the paper. BNB contributed to the methodology, writing review, and editing of the research.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of Data and Materials
The data sets used and analyzed during the current study will be available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.