
Abstract
Background
A review of the literature on geriatric care assessment tools revealed no specific tools for assessing caregivers’ abilities in terms of seven major diseases—acute myocardial infarction, stroke, falls, diabetes, hypertension, osteoarthritis, and dementia—particularly in the context of rural community of Thailand as well as the need of the psychometric tested instrument for caregivers about knowledge, attitudes, and practice domain.
Objective
This cross-sectional study aimed to develop an assessment tool for knowledge, attitudes, and practices in continuity care for older adults with significant diseases.
Method
The sample consisted of 400 randomly selected caregivers and community health volunteers who cared for older adults with significant diseases. The instruments used incorporated 280 items of a questionnaire assessing knowledge, attitudes, and behaviors in continuity care for older adults with significant diseases and were reviewed by five experts, with a Content Validity Ratio (CVR) of over 0.99 and a Content Validity Index (CVI) of 0.98. All instruments were examined for reliability, with the knowledge assessment scoring a KR-20 of 0.71, the attitude assessment a Cronbach's alpha of 0.96, and the behavior assessment a Cronbach's alpha of 0.99. Data were analyzed using the factor analysis process, where exploratory factor analysis (EFA) was first performed by extracting elements using the principal component analysis method and Varimax rotation, followed by confirmatory factor analysis (CFA).
Results
The final version of the geriatric care competency instrument consists of a 60-item knowledge, a 28-item attitude, and a 177-item practice domain, along with models for measuring knowledge, attitudes, and behaviors in the continuous care of elderly individuals with suitable construct validity.
Conclusions
The results suggest that healthcare agencies can use the standardized assessment tool for continuous care competency in community caregivers.
Introduction
With an increasingly aging worldwide population, many countries have faced challenges. This rising older adults proportion could affect the healthcare system by improving its effectiveness in continuity care (Jones & Dolsten, 2024). In the context of developing countries and the increasing number of older adults, along with the rate of chronic diseases and accidents that impact serious illnesses and dependency in these countries, there is an urgent need for continuous long-term care to monitor complications in various diseases (Higo & Khan, 2015). Thailand has several limitations in its provision of health services, and this obstacle creates barriers to accessing comprehensive care for older adults. Although Thailand has launched an initiative to establish a primary healthcare system aimed at providing care to the entire population (Tejativaddhana et al., 2018), caring for older adults remains a challenge (Sumriddetchkajorn et al., 2019). For this reason, community health care volunteers collaborate with health officials to provide care to the local population (Woldie et al., 2018). While these efforts demonstrate how community health care volunteers have been developing their potential in various dimensions—including knowledge and skills in primary health care—caregivers have not been adequately assessed for their ability to care for older adults (Kowitt et al., 2015; Nawsuwan et al., 2025).
Literature Reviews
Thailand is currently experiencing an increase in the number of older individuals and is on track to become a completely age-inclusive society (Tantirat et al., 2020). The physical qualities of older persons, which deteriorate with age, can lead to a loss of function in numerous organs, resulting in illness and chronic diseases (Dombrowsky, 2023). This situation compels the public and private sectors to focus on and adjust their operations to enhance the quality of life of older people in the community (Şahin et al., 2019) by enabling older adults to access welfare and services for rehabilitation from chronic diseases and to achieve self-care abilities, among others (Zhou, Zhang, et al., 2025).
The older adult population in Surat Thani province has experienced a substantial and increasing burden of chronic diseases. The provincial health data indicate that older adults are progressively impacted by new cases of stroke, cardiovascular disease, diabetes, and hypertension (Surat Thani Provincial Public Health Office, 2024a, 2024b). A similar pattern is evident in Ban Na Derm district, where these same chronic illnesses are prevalent among older adults. These diseases are frequently accompanied by high rates of musculoskeletal problems, knee pain, and fall risk (Surat Thani Provincial Public Health Office, 2024b, 2024c, 2024d, 2024e). These district reports reflect broader national trends in which chronic diseases among Thai older adults are increasing continuously. The evidence has also revealed that the elderly half of the population is experiencing multiple conditions simultaneously (Department of Older Persons, 2023). The incidence of falls is approximately 20%, showing that Ban Na District has an elderly population structure at greater risk of degenerative diseases and falls than the national average. Overall, the evidence underscores the growing health challenges of multimorbidity and functional decline in the aging population at both the provincial and national levels. Therefore, it is necessary to focus on preventive measures and look at specific areas more directly (Pardoel et al., 2024; Rickles, 2011) to improve the healthcare system for older people (John et al., 2017).
Given the general statistics and health conditions of older people, particularly in Surat Thani and Ban Na Derm district, it is clear that chronic illnesses and the risk of falling are significant concerns (Paliwal et al., 2017) that require ongoing care and prevention strategies to enhance their quality of life (Tang et al., 2022) However, a review of the literature on geriatric care assessment tools revealed no specific tools for assessing caregivers’ abilities in terms of seven major diseases—acute myocardial infarction, stroke, falls, diabetes, hypertension, osteoarthritis, and dementia—particularly in the context of rural community of Thailand as well as the need of the psychometric tested instrument for caregivers about knowledge, attitudes, and practice domain. (Murali et al., 2022). Although several recent studies have provided evidence of tool development for caregiver evaluation across various dimensions and purposes, a limitation remains in the accuracy of the instrument validation process and in the confidence of implications (Doungjan, 2017; Klinjun et al., 2023; Sari et al., 2022; Thana et al., 2022). Moreover, there is a need for reporting to adopt a systematic and transparent approach, particularly in terms of its cultural and educational relevance among tool development (Zarei et al., 2024; Zhou, Gu, et al., 2025). The instrument in this study was designed for both family caregivers and community health volunteers who support daily care and basic health activities. At the same time, healthcare professionals deliver clinical care for older adults.
The research team has been on a crucial mission to develop an assessment tool for continuous geriatric care competencies. The main concepts of the geriatric care competency measurement were developed based on a literature review related to caregiver competency in geriatric care, focusing on three key domains: knowledge, attitudes, and practices for continuity of care for older adults in the community.
This instrument, which is tailored to the unique healthcare issues of a rural community, covers this gap by offering a complete and context-specific evaluation of carers’ competencies in the seven disease domains and will appropriately evaluate caregiving skills and connect them to learning processes that improve geriatric care. The ultimate objective is to improve older individuals’ quality of life, minimize hospitalizations and readmissions, and provide comprehensive and accessible healthcare services free of chronic illness consequences. These findings will directly and significantly affect geriatric care and public health.
Research Objectives
To develop an assessment tool for knowledge, attitudes, and practices in the continuity of care for older adults with significant diseases.
To validate the Thai version of geriatric care competency in significant diseases among caregivers in the continuity of care for older adults
This study hypothesizes that the instrument will demonstrate acceptable psychometric properties in terms of content validity, reliability, and construct validity in the rural Thai community context, at p < 0.05.
Methods
Design
Based on a cross-sectional study, this research represents a comprehensive effort to develop and validate an instrument to assess the continuity of geriatric care with seven significant diseases. The research methods involved a psychometric assessment of the nursing instrument for evaluating community health care volunteers across three dimensions: knowledge, attitudes, and behaviors. This study formed the first part of the project titled “Enhancing Quality of Care and Health Outcomes in Significant Illness Toward Geriatric Comprehensive Health Care Innovation within Integrating the Health Eco-System Platform: Suratthani Model.”
Research Question
How valid is the psychometric development of the Thai version of geriatric care competency in significant diseases among caregivers in a rural Thai community?
Samples
The research sample consisted of 400 caregivers and community health volunteers (CHVs) who cared for older adults with significant diseases across four primary healthcare units in Surat Thani, Thailand.
Inclusion and Exclusion Criteria
The research samples were selected through a random sampling process that recruited participants who met the following inclusion criteria: 1) over 18 years of age; 2) voluntary participation; and 3) able to read and write in Thai. The exclusion criteria included physical issues that arose during questionnaire completion, such as dizziness.
Sample calculations were performed by Hair et al. (2010), who suggested that the appropriate sample was between 10 and 20 times the number of variables studied. The researcher determined the sample size to be 20 times the 19 variables studied, which is the larger ratio selected to ensure greater statistical power and stability of parameter estimates in the confirmatory factor analysis (CFA) (Wolf et al., 2013). The total number of research samples was 380. To prevent dropout, the researcher increased the sample size to 400 cases. Both caregivers and Community Health Volunteers (CHVs) play complementary roles in supporting older adults in primary care and rural communities within the Thai context. Despite the role of these subgroup differences, they share competencies in providing supportive and continuous care, which can be evaluated using the validated measure instrument of this study.
Research Instruments
The original 280 items of measured development of seven significant diseases comprise 13 steps:
Step 1: Defining the variable for the literature review Step 2: Defining the concept of the study Step 3: Defining the operational definition Step 4: Designing the measurement into a five-level rating scale in the attitude and practice dimension, and two choices in the knowledge dimension Step 5: Defining the domain and subdomain content that aligns with the operational definition Step 6: Drafting the item contents with the sub- and main concepts of measurement Step 7: Sequencing the questions by difficulty Step 8: Examining the content validity reported by five experts Step 9: Modifying and adjusting the measurement according to expert recommendations Step 10: Conducting item analysis and component analysis Step 11: Testing out the instrument in 30 cases Step 12: Reanalyzing all measurement items Step 13: Finalizing the psychometric properties
The included research instruments were as follows. First, a personal characteristic questionnaire included items on gender, age, occupation, education level, role in elderly care in the community, and training experience in elderly care. Second, a knowledge assessment of the continuity care of older adults with significant diseases focus on signs, symptoms, and assessment knowledge that consisted of 70 items with a two-choice format (yes/no), for which correct answers scored 1 point and incorrect answers scored 0 points, with a maximum score of 70 points. The assessed knowledge included myocardial infarction (10), stroke (10), falls (10), osteoarthritis (10), dementia (10), diabetes mellitus (10), and hypertension (10). These diseases and conditions were selected based on their high prevalence among older adults and their significant impact on older adults’ quality of life and healthcare needs. Third, an attitude assessment for the continuous care of older adults with significant diseases consisted of 28 items divided into three aspects—confidence in self-efficacy (12), attitudes toward patient and family care (9), and social support (7)—measured using a five-point Likert scale (1 = least, 5 = most). Fourth, a behavior and practice assessment for the continuous care of older adults with significant diseases consisted of 177 items divided into seven aspects: assessment and data collection (34), care planning (21), care implementation (27), communication (25), consultation (23), technology use in care (23), and continuous care evaluation (24). These aspects were selected based on their importance in providing comprehensive and effective geriatric care. The assessment was measured using a five-point Likert scale (1 = least, 5 = most). In this study, the psychometric development of the Thai version of geriatric care competency in significant diseases among caregivers underpins Bloom et al. (1956) learning theory, which focuses on the development of knowledge, attitude, and skill. Moreover, skill measurement methods are framed by the nursing process—including assessment, planning, implementation, and evaluation—about the continuity of care for the seven diseases and the ability to use technology in care.
Instrument Validity
After the researcher created the research instruments, content validity was reviewed by five experts who are registered nurses and nursing instructors. These experts were selected based on their qualifications in geriatric nursing, nursing research, and measurement development. Their professional experience ranged from 10 to 25 years. This showed a Content Validity Ratio (CVR) of over 0.99 and a Content Validity Index (CVI) of 0.98, indicating a high level of agreement among the parts. Reliability was examined by piloting each questionnaire set with 30 participants similar to those in the sample and calculating the reliability coefficients. The knowledge assessment achieved a Kuder-Richardson Formula 20 (KR-20) of 0.71, the attitude assessment a Cronbach's alpha of 0.96, and the behavior and practice assessment a Cronbach's alpha of 0.99, indicating the high internal consistency and reliability of the instruments.
Data Collection
This research collected data between August and September 2023. A representative from each service unit carried out data collection using a developed questionnaire and reviewed the data for completeness prior to the analysis process.
Data Analysis
The data analysis presented in this article includes descriptive statistics, including frequency, percentage, minimum, maximum, mean, and standard deviation. Exploratory factor analysis (EFA) was used with principal component analysis and varimax rotation to clarify the structure of the multi-item questions. Confirmatory factor analysis (CFA) was used to confirm alignment between the developed assessment tool and empirical data using indices and criteria suggested by Hair et al. (2013)—namely, χ2/df. ≤ 5, CFI ≥ 0.90, TLI ≥ 0.90, RMSEA ≤ 0.10, and RMR ≤ 0.05.
Ethical Considerations
This research has been approved by the Human Research Ethics Committee of Surat Thani Provincial Public Health Office (No: STPHO2023-186). This phase of research strictly considers the sample's privacy and confidentiality rights. The sample received sufficient information before deciding to participate in the research and signed the informed consent to participate in the research project. However, the sample group can withdraw from the research at any time without affecting any contribution to the service in the local healthcare unit.
Results
Data were collected from questionnaires completed by caregivers and CHVs who cared for elderly individuals with significant diseases. Initially, 400 participants were involved; however, since two provided incomplete data, there were complete responses from 398 participants. The majority of respondents were female (82.2%), engaged in gardening (80.7%), and had a high school education (1.5%). Most served as CHVs (98.5%) and had training in elderly care (71.4%).
Part 1: Analysis of Knowledge of Continuous Care for Elderly Individuals With Significant Diseases Among Caregivers and CHVs
The levels of knowledge of caregivers and CHVs in Surat Thani Province regarding continuous care for older adults with significant diseases were as follows. Knowledge about myocardial infarction had the highest mean score (mean = 11.26, SD = 1.26), followed by stroke (mean = 8.07, SD = 1.28), diabetes (mean = 7.43, SD = 1.47), falls (mean = 7.33, SD = 1.69), and dementia (mean = 5.26, SD = 1.21). Knowledge about osteoarthritis and hypertension had equal mean scores (mean = 6.64, SD = 1.52 and 1.31, respectively), as shown in Table 1.
Basic Statistics Regarding Knowledge of Continuous Care for Elderly Individuals With Significant Diseases Among Caregivers and CHVs (N = 398).

The CFA for common factors of significant diseases among caregivers and CHVs included myocardial infarction, stroke, falls, osteoarthritis, dementia, diabetes, and hypertension. The researchers input all observed variables from the knowledge scores into the measurement model to evaluate the harmony between the knowledge measurement model for continuous care of older adults with significant diseases and the empirical data, as shown in Figure 1 and Table 2.

Results of Confirmatory Factor Analysis for the Knowledge Measurement Model for the Continuous Care of Elderly Individuals with Significant Diseases.
Evaluation of the Observed Variables Used to Measure Knowledge for the Continuous Care of Elderly Individuals With Significant Diseases.

Note: The factor loading of MI is a fixed parameter (not estimated). ***p < .001.
The results shown in Figure 1 indicate that the knowledge measurement model for the continuous care of elderly individuals with significant diseases is consistent with the empirical data. The model fit indices are as follows: Chi-square/degrees of freedom (χ2/df.) = 1.250, Comparative Fit Index (CFI) = 0.994, Tucker–Lewis Index (TLI) = 0.986, Root Mean Square Error of Approximation (RMSEA) = 0.025, and Root Mean Square Residual (RMR) = 0.047.
Table 2 presents the details of each observed variable.
From Table 2, six out of seven observed variables significantly measured the knowledge variable for the continuous care of elderly individuals with significant diseases at the .001 level. These variables included knowledge about myocardial infarction, stroke, falls, osteoarthritis, dementia, and diabetes, but not hypertension, which did not significantly measure the knowledge variable. When considering construct validity, the criteria suggested by Hair et al. (2010) were used. According to these criteria, (1) standardized factor loadings (λ) should be at least 0.70 or statistically significant, (2) the reliability coefficients of the observed variables (R²) should be at least 0.50, (3) the composite reliability (CR) of the measurement model should be at least 0.70, and (4) the average variance extracted (AVE) should be at least 0.50.
Therefore, it was concluded that the knowledge measurement model (Know) for the continuous care of elderly individuals with significant diseases lacked construct validity and should be improved for future use.
Part 2: Analysis of Attitudes Regarding the Continuous Care of Elderly Individuals With Significant Diseases Among Caregivers and CHVs
Attitudes toward Self-Efficacy
The researchers used a set of 15 questions to measure attitudes toward self-efficacy among the sample group. Based on EFA, the results indicated that 12 questions had cross-loadings that did not exceed 0.40. These questions had a chi-square of Bartlett's test of sphericity of 3,523.582, a degree of freedom of 66, a p-value of 0.000, and a KMO of 0.853, indicating that the data from these questions had suitable interrelationships.
The grouping of the 12 questions resulted in two factors consistent with the criteria suggested by Hair et al. (2010). The first factor, attitudes toward self-efficacy in skills and knowledge (SK_SEF_C), comprises six questions—SEF_C1, SEF_C2, SEF_C4, SEF_C5, SEF_C6, and SEF_C15—with a percentage of variance of 27.222 and factor loadings ranging from 0.588 to 0.821. The second factor, attitudes toward self-efficacy in support (SP_SEF_C), comprises six questions—SEF_C7, SEF_C8, SEF_C9, SEF_C10, SEF_C11, and SEF_C13—with a percentage of variance of 37.910 and factor loadings ranging from 0.712 to 0.888.
To confirm construct validity, the researchers employed second-order CFA to verify whether the measurement model for attitudes toward self-efficacy (SEF_C), comprising two subdimensions and 12 indicators, aligned with the empirical data. The results of the CFA for SEF_C indicated consistency with the empirical data. (See figure in Supplemental Material 1).
The results indicate that the measurement model for SEF_C fits well with the empirical data (χ2/df. = 4.647, CFI = 0.960, TLI = 0.931, RMSEA = 0.096, and RMR = 0.039). (The details of each observed variable are presented in Supplemental Material 2.)
The measurement model for SEF_C has suitable construct validity because (1) all observed variables (12 in total) were statistically significant at the 0.001 level, despite SEF_C4 and SEF_C6 having values less than 0.70; (2) the reliability coefficients (R²) of the observed variables were not less than 0.50, except SEF_C4 and SEF_C6; (3) the CR was not less than 0.70 (CR = 0.882); and (4) the AVE was not less than 0.50 (AVE = 0.790).
Attitudes Toward Patient and Family Care
The measurement of attitudes toward patient and family care was conducted using nine questions. The EFA results indicated that all nine questions had appropriate interrelationships (chi-square of Bartlett's test of sphericity = 3,953.819, df. = 36, p = 0.000), and the sample size was adequate for EFA (KMO = 0.901). Since the nine questions could not be separated into distinct components, the variable attitudes toward patient and family care for caregivers and CHVs was considered unidimensional, comprising CARE1–CARE9 (% of variance = 74.991), with factor loadings ranging from 0.773 to 0.950.
To confirm the construct validity, the researchers used first-order CFA to verify whether the nine-indicator measurement model for attitudes toward patient and family care aligned with the empirical data. The CFA results for attitudes toward patient and family care indicated consistency with the empirical data. (See figure in Supplemental Material 3)
The results indicated that the measurement model for attitudes toward patient and family care (CARE) fits well with the empirical data (χ2/df. = 4.647, CFI = 0.960, TLI = 0.931, RMSEA = 0.096, and RMR = 0.039). (The details of each observed variable are presented in Supplemental Material 4.)
The measurement model for CARE has suitable construct validity because (1) all observed variables (nine in total) had factor loadings not less than 0.70 and were statistically significant at the .001 level, (2) the reliability coefficients (R²) of the observed variables were not less than 0.50, (3) the CR was not less than 0.70 (CR = 0.965), and (4) the AVE was not less than 0.50 (AVE = 0.711).
Attitudes Toward Social Support
The seven questions measuring attitudes toward social support employed EFA to validate the instrument. The EFA results indicated that all seven questions had appropriate interrelationships (chi-square of Bartlett's test of sphericity = 3,250.397, df. = 21, p = 0.000), and the sample size was adequate for EFA (KMO = 0.917). Since the seven questions could not be separated into distinct components, the variable attitudes toward social support for caregivers and CHVs was considered unidimensional, comprising SOCS1–SOCS7 (% of variance = 82.241), with factor loadings ranging between 0.834 and 0.933.
To confirm construct validity, the researchers utilized first-order CFA to verify whether the measurement model for attitudes toward social support, consisting of seven indicators, aligned with the empirical data. The CFA results for attitudes toward social support indicated consistency with the empirical data. (See figure in Supplemental Material 5)
The measurement model for attitudes toward social support (SOCS) fits well with the empirical data (χ2/df. = 4.182, CFI = 0.988, TLI = 0.979, RMSEA = 0.090, and RMR = 0.013). (The details of each observed variable are presented in Supplemental Material 6.)
The measurement model for SOCS has suitable construct validity because (1) all observed variables (seven in total) had factor loadings not less than 0.70 and were statistically significant at the 0.001 level, (2) the reliability coefficients (R²) of the observed variables were not less than 0.50, (3) the CR was not less than 0.70 (CR = 0.962), and (4) the AVE was not less than 0.50 (AVE = 0.783).
After confirming the construct validity of the observed variables in each of the attitude components (attitudes toward self-efficacy, patient and family care, and social support), the researchers performed second-order CFA to ensure the overall model fit for the combined attitudes toward continuous care for elderly individuals with significant diseases, as shown in Figure 2.
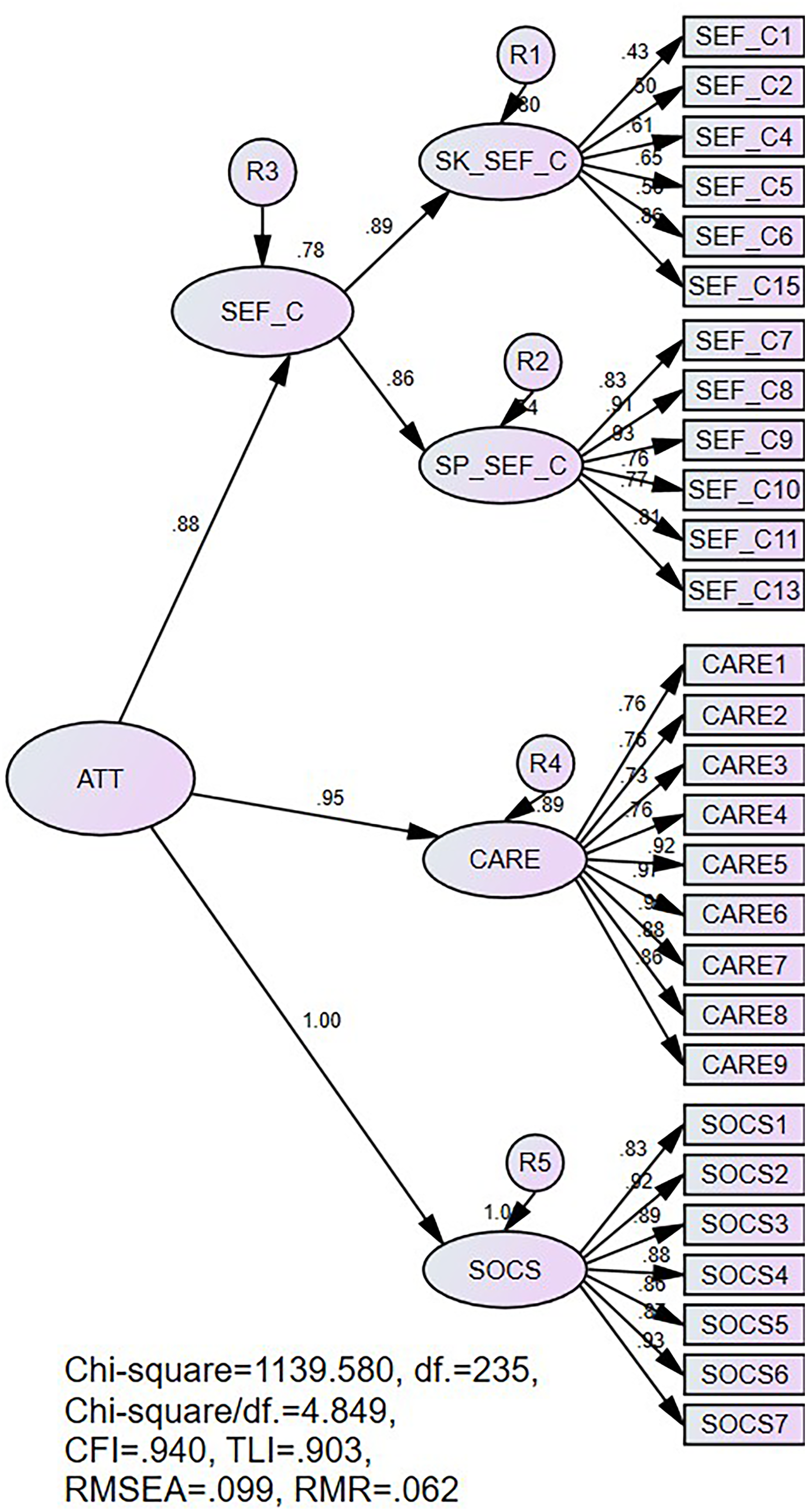
Results of Second-Order Confirmatory Factor Analysis for Combined Attitudes Toward Continuous Care for Elderly Individuals with Significant Diseases (ATT).
An evaluation of the indices used to measure the model fit for the combined attitudes toward continuous care for elderly individuals with major diseases (ATT) and the empirical data yielded the following results: χ2/df = 4.849, CFI = 0.940, TLI = 0.903, RMSEA = 0.099, and RMR = 0.062. These values indicate that the model fits well with the empirical data. Therefore, the researchers evaluated the subcomponents explaining the variance in ATT in Table 3.
Evaluation of the Second-Order Components of the Measurement Model for Combined Attitudes Toward Continuous Care for Elderly Individuals With Significant Diseases (ATT).

Note: The factor loading of SEF_C is a fixed parameter (not estimated). ***p < .001.
Table 3 shows that three subcomponents can significantly explain the variance in ATT at 0.001. The overall measurement model has suitable composite reliability (CR = 0.962) and can explain 89.4% of the variance in ATT (AVE = 0.894), indicating that it has suitable construct validity for measuring attitudes toward continuous care for elderly individuals with significant diseases among caregivers and CHVs in Surat Thani province.
From the above research results, the attitude measurement model for the continuous care of elderly individuals with significant diseases among caregivers and CHVs in Surat Thani province consists of three components. First, SEF_C includes two sub-components: SK_SEF_C, measured by six observed variables, and SP_SEF_C, also measured by six observed variables. Second, CARE is measured by nine observed variables. Third, SOCS is measured by seven observed variables.
The researchers averaged the data from each component's observed variables into a single observed variable. (The mean and standard deviation for each variable are presented in Supplemental Material 7.)
The caregivers and CHVs in Surat Thani province had an overall high attitude toward ATT. The subcomponents of attitudes had high mean scores for SOCS and CARE, while SEF_C had a medium mean score.
Part 3: Analysis of Behavior and Practice Variables in the Continuous Care of Elderly Individuals With Significant Diseases Among Caregivers and CHVs
The measurement of behavior and practice variables in the continuous care of elderly individuals with significant diseases among caregivers and CHVs consists of seven dimensions: (1) assessment and data collection (ASS), (2) care planning (PLAN), (3) care implementation (PLAC), (4) communication (COM), (5) consultation (CONS), (6) technology use in care (TECH), and (7) continuous care evaluation (EVAL).
The construct validity of the measurement model for the behavior and practice variables in the continuous care of elderly individuals with significant diseases among caregivers and community health workers (CHWs) was assessed using CFA. The results are shown in Figure 3 and Table 4.
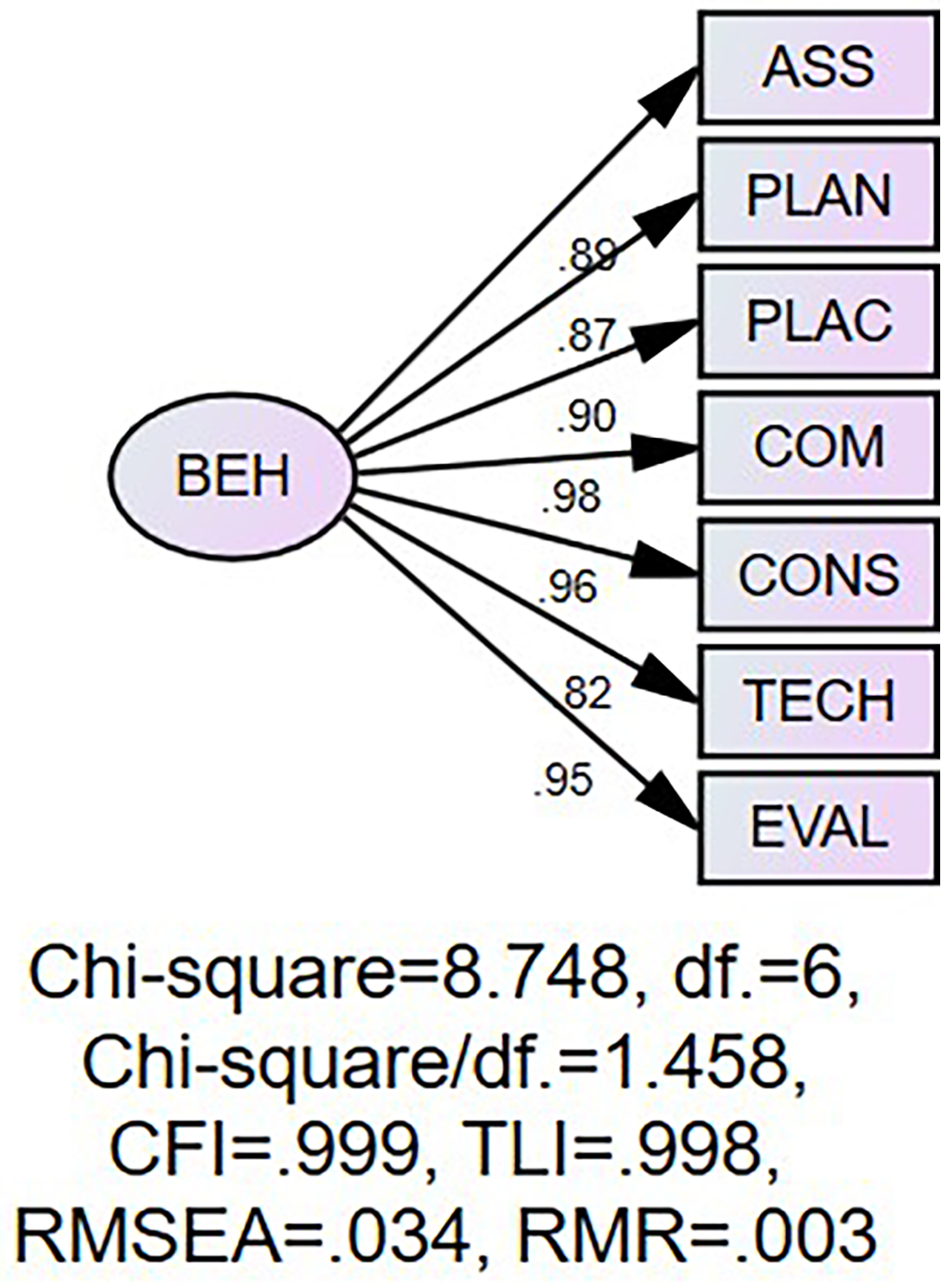
Results of the Confirmatory Factor Analysis for the Measurement Model of Behavior and Practice Variables in the Continuous Care of Elderly Individuals with Significant Diseases Among Caregivers and CHVs (BEH).
Evaluation of the Observed Variables Used to Measure the Behavior and Practice Variables in the Continuous Care of Elderly Individuals With Significant Diseases Among Caregivers and CHVs (BEH).

Note: The factor loading of ASS is a fixed parameter (not estimated). ***p < .001.
The results in Figure 3 show that the measurement model for BEH in the continuous care of elderly individuals with significant diseases fits well with the empirical data (χ2/df. = 1.458, CFI = 0.999, TLI = 0.998, RMSEA = 0.034, and RMR = 0.003). Table 4 presents the details of each observed variable.
Table 4 indicates that the measurement model for BEH in the continuous care of elderly individuals with significant diseases has suitable construct validity because (1) all observed variables (seven in total) had factor loadings not less than 0.70 and were statistically significant at the .001 level, (2) the reliability coefficients (R²) of the observed variables were not less than 0.50, (3) the CR was not less than 0.70 (CR = 0.971), and (4) the AVE was not less than 0.50 (AVE = 0.829).
The BEH measurement model for the continuous care of elderly individuals with significant diseases among caregivers and CHVs in Surat Thani province includes seven dimensions: ASS, PLAN, PLAC, COM, CONS, TECH, and EVAL. The mean and standard deviations for each dimension are presented in Table 5.
Basic Statistics for the Behavior and Practice Variables in the Continuous Care of Elderly Individuals With Significant Diseases Among Caregivers and CHVs (BEH) in Surat Thani Province (N = 398).

Note: 1.00–1.80 = very low, 1.81–2.60 = low, 2.41–3.40 = medium, 3.41–4.20 = high, 4.21–5.00 = very high.
Table 5 shows that the caregivers and CHVs in Surat Thani province had a medium level of BEH in the continuous care of elderly individuals with significant diseases. The subcomponents of BEH had high mean scores for PLAC, ASS, and PLAN, while the other dimensions had medium mean scores.
Discussion
This study aimed to develop a valid and reliable assessment tool for caregivers’ knowledge, attitudes, and practices (KAP) in providing continuity care for older adults with significant diseases. The key findings indicate that this objective was revealed, as the newly developed instrument demonstrated strong psychometric properties across all three domains, as follows:
Together, these results suggest that the instrument is psychometrically sound and aligns well with the research objectives of assessing KAP in continuity of care.
The outcomes of this psychometric evaluation largely align with previous research on caregiver competency instruments and KAP studies in geriatric care. Similar to this study, earlier instrument development efforts reported high internal consistency and validity across knowledge, attitude, and practice scales. For instance, Sari et al. (2022) demonstrated that their KAP questionnaire for Indonesian family caregivers was reliable and valid, with strong Cronbach's alpha values in each domain. The instrument of this study reflects a similar level of reliability in measuring KAP for continuous elder care. Furthermore, the pattern in which most knowledge items exhibited significant factor loadings is consistent with other knowledge assessments. Existing quizzes and surveys often find that the most well-designed knowledge items significantly contribute to the total score (Mitike et al., 2023). Dikken et al. (2018) observed this in a Dutch study in which all items of the knowledge questionnaires on older patient care had good item characteristics and achieved very high reliability. The findings regarding six out of seven significant knowledge items were comparable, primarily indicating the robust coverage of the knowledge construct. This study's findings imply that caregivers of elderly individuals should know about managing chronic diseases and preventing falls to provide proper care and reduce complications (Arai et al., 2015; Kraiwong et al., 2014). This result is consistent with Hailu et al. (2024), who emphasized that caregivers need proper knowledge and training to improve the quality of life of elderly individuals. Nevertheless, the variable concerning knowledge of hypertension fails to satisfy the quality assessment criteria. The complexity of knowledge regarding hypertension and the variations in caregiver training may contribute to this issue. Therefore, it might be required to make improvements in this area or carry out additional assessments in subsequent studies.
While several studies have been conducted on the psychometric properties of measuring the knowledge, attitude, and practice of family caregivers, this study highlights the differences in focus for seven significant diseases in older adults that are specific to rural community contexts.
Additionally, attitudes toward the continuous care of elderly individuals with significant diseases among caregivers and CHWs encompass self-efficacy. The model fit indices for attitudes toward self-efficacy with empirical data showed a good fit of 79.0%. These findings suggest that positive attitudes and perceptions among caregivers directly influence caregivers’ confidence and readiness to care for elderly individuals.(DiZazzo-Miller et al., 2020). This result is consistent with Teichmann et al. (2022), who found positive caregiver attitudes increase confidence and readiness to care for elderly individuals. The attitudes toward patient and family care among caregivers and CHVs aligned well with the empirical data. Similarly, the attitude toward social support among caregivers and CHVs showed a good fit of measurement. The current findings highlight that the developed instrument can be used to measure the continuity of care in caregivers and also require an appropriate intervention related to attitude for enhancing the social support to achieve quality care for older adults in the community. (del-Pino-Casado et al., 2018)
From these research results, it can be concluded that elderly individuals with chronic diseases often depend on their families, communities, and society for care. Caregivers and community members are essential for enhancing the quality of life of older adults (Tuttle et al., 2022). The results of this study align with recent research suggesting that strengthening family and caregiver support in elderly care leads to holistic and effective care (Schulz et al., 2020; Tuttle et al., 2022). Therefore, the developed assessment tool for continuous care competency for elderly individuals with significant diseases, which includes knowledge and attitudes toward continuous care, can be effectively used to assess the competency of caregivers and CHVs. Health agencies should use this assessment tool to evaluate caregiver readiness and link it to caregiver training and preparedness for elderly care.
Similarly, the current study's unidimensional and valid attitude domain echoes results from other contexts; for example, instruments such as the Older People's Acute Care Survey (OPACS) capture nurses’ attitudes toward older adult care as a single factor, with excellent validity and reliability (Mitike et al., 2023). The notion that a caregiver's positive attitude or willingness to care is a distinct, measurable trait has been supported in various cultural settings (Sari et al., 2022). This study reinforces this notion within the rural Thai caregiver context. Additionally, measuring caregiver practices has been the focus of several studies, and this research's success in validating the practice domain resonates with these studies. For example, Kaspar and Hartig (2016) and others detailed key caregiving tasks and found that caregivers’ self-reported practices can be reliably quantified. This research confirms many patterns seen in prior KAP research—namely, the high reliability of well-constructed scales and the feasibility of assessing family caregiver competencies in elder care in a structured way.
Despite these similarities, notable differences exist between this study's findings and some earlier studies, highlighting the unique contribution of the current research. One difference is the breadth of context, with many prior tools focusing on a single disease or a specific aspect of care (Lv et al., 2024; Phetrnui et al., 2025). In contrast, this study addressed a wider range of “significant diseases” and the required continuity of care, making this instrument more comprehensive for general geriatric care in the community. This broader scope may explain why the practice domain is not split into as many subfactors. In addition, this study's focus on continuity of care is a distinguishing factor. Prior research has often looked at knowledge, attitudes, and practices in a static sense by centering on continuity of care to ensure consistent and uninterrupted care as patients move through different stages or settings (Idoudi et al., 2024; Zhou et al., 2024). This research's findings underscore the dynamic aspect of caregiving competency. This continuous care perspective is crucial for chronic disease management, but has been explored less in instrument design. We found that caregivers’ attitudes and behaviors regarding maintaining long-term care can be quantified reliably. This result opens the door to future research and interventions focused on improving continuity of care via caregiver training—a link that previous studies only tangentially addressed (Meyer et al., 2022; Premnazeer et al., 2025). Moreover, the findings of this study highlight the effective reduction of the original 280 items of measurement into a concise, valid, and reliable instrument of 265 items, which ensures the accuracy process for psychometric development in the healthcare context. In summary, the study's results corroborate many findings from the literature and expand the conversation by introducing a broader, continuity-centric tool tested in a new cultural setting. These differences enhance the understanding of caregiver competencies and highlight the need to tailor and expand instruments to diverse caregiving contexts (Rong et al., 2024).
Strengths and Limitations
This study indicates that the measurement has robust validity, ensuring the rigor that health care providers can employ in similar primary healthcare contexts of rural communities. In addition, the measurement encompasses the technological capability of caregivers, which is essential to evaluate the effectiveness of care in the era of new technologies that influence primary healthcare services. In contrast, the study's limitations include the random recruitment of research samples across the Ban Na Derm district, which is part of the city of Surat Thani. This research site selection could be a limitation that needs to be addressed to obtain more data from other similar contexts in gerontological care, thereby allowing for more generalizations. Moreover, the measurement of hypertension knowledge did not meet the significance benchmarks, requiring an in-depth analysis for the factors’ relevance to the validity and adjustments for appropriate further implementations, as well as test-retest reliability and external validity of measurement require further confirmation. Finally, the number of items and the length of the measurement for geriatric care may contribute to participant fatigue, which can result in response bias, affecting subsequent research outcomes. The various items were screened by researchers and carefully considered to select content relevant to the care of older adults within seven significant disease groups, while reducing redundancy in the questionnaire. However, given these limitations, future implications or modifications of this tool may involve developing a shorter version of the measurement.
Implications for Practice
To enhance effective work in continuity of care for older adults in rural communities, nurses play a crucial role in assessing caregivers’ competencies and considering practical strategies and interventions for caregivers, in particular, community training in consultation skills, technology use in care, continuous care evaluation, and self-efficacy to gain better continuity of care for older adults in rural communities.
Conclusion
This study effectively developed a psychometric instrument to assess CHVs’ competencies in providing continuous care for elderly individuals with chronic medical conditions in rural Thai communities. The findings confirm the tool's construct validity, with six out of seven observed variables significantly measuring knowledge and appropriately validating attitude and behavioral models. The results uncovered during the investigation accentuate the benefits of applying the standard measurement in community supportive care to confirm that caregivers are suitably equipped to handle elderly care. Moreover, the tool serves as a foundation for further consideration by building comprehensive assessment models for elder adult care in Thailand. Further studies could focus on improving caregivers’ capacity to provide consistent care through training programs and pilot studies to develop care capability levels in primary healthcare services. The instrument offers basic guidance; however, streamlining is expected to upgrade usage across towns. Additionally, long-term investigations following preparatory outcomes could measure care outcomes and identify areas for targeted improvement.
Supplemental Material
sj-docx-1-son-10.1177_23779608251393313 - Supplemental material for Psychometric Development of the Thai Version of Geriatric Care Competency in Significant Diseases Among Caregivers in a Rural Thai Community
Supplemental material, sj-docx-1-son-10.1177_23779608251393313 for Psychometric Development of the Thai Version of Geriatric Care Competency in Significant Diseases Among Caregivers in a Rural Thai Community by Praditporn Pongtriang, Pilaiporn Sukcharoen, Aranya Rakhab, Vasinee Somsiri and Apinya Ingard in SAGE Open Nursing
Supplemental Material
sj-docx-2-son-10.1177_23779608251393313 - Supplemental material for Psychometric Development of the Thai Version of Geriatric Care Competency in Significant Diseases Among Caregivers in a Rural Thai Community
Supplemental material, sj-docx-2-son-10.1177_23779608251393313 for Psychometric Development of the Thai Version of Geriatric Care Competency in Significant Diseases Among Caregivers in a Rural Thai Community by Praditporn Pongtriang, Pilaiporn Sukcharoen, Aranya Rakhab, Vasinee Somsiri and Apinya Ingard in SAGE Open Nursing
Supplemental Material
sj-docx-3-son-10.1177_23779608251393313 - Supplemental material for Psychometric Development of the Thai Version of Geriatric Care Competency in Significant Diseases Among Caregivers in a Rural Thai Community
Supplemental material, sj-docx-3-son-10.1177_23779608251393313 for Psychometric Development of the Thai Version of Geriatric Care Competency in Significant Diseases Among Caregivers in a Rural Thai Community by Praditporn Pongtriang, Pilaiporn Sukcharoen, Aranya Rakhab, Vasinee Somsiri and Apinya Ingard in SAGE Open Nursing
Supplemental Material
sj-docx-4-son-10.1177_23779608251393313 - Supplemental material for Psychometric Development of the Thai Version of Geriatric Care Competency in Significant Diseases Among Caregivers in a Rural Thai Community
Supplemental material, sj-docx-4-son-10.1177_23779608251393313 for Psychometric Development of the Thai Version of Geriatric Care Competency in Significant Diseases Among Caregivers in a Rural Thai Community by Praditporn Pongtriang, Pilaiporn Sukcharoen, Aranya Rakhab, Vasinee Somsiri and Apinya Ingard in SAGE Open Nursing
Supplemental Material
sj-docx-5-son-10.1177_23779608251393313 - Supplemental material for Psychometric Development of the Thai Version of Geriatric Care Competency in Significant Diseases Among Caregivers in a Rural Thai Community
Supplemental material, sj-docx-5-son-10.1177_23779608251393313 for Psychometric Development of the Thai Version of Geriatric Care Competency in Significant Diseases Among Caregivers in a Rural Thai Community by Praditporn Pongtriang, Pilaiporn Sukcharoen, Aranya Rakhab, Vasinee Somsiri and Apinya Ingard in SAGE Open Nursing
Supplemental Material
sj-docx-6-son-10.1177_23779608251393313 - Supplemental material for Psychometric Development of the Thai Version of Geriatric Care Competency in Significant Diseases Among Caregivers in a Rural Thai Community
Supplemental material, sj-docx-6-son-10.1177_23779608251393313 for Psychometric Development of the Thai Version of Geriatric Care Competency in Significant Diseases Among Caregivers in a Rural Thai Community by Praditporn Pongtriang, Pilaiporn Sukcharoen, Aranya Rakhab, Vasinee Somsiri and Apinya Ingard in SAGE Open Nursing
Supplemental Material
sj-docx-7-son-10.1177_23779608251393313 - Supplemental material for Psychometric Development of the Thai Version of Geriatric Care Competency in Significant Diseases Among Caregivers in a Rural Thai Community
Supplemental material, sj-docx-7-son-10.1177_23779608251393313 for Psychometric Development of the Thai Version of Geriatric Care Competency in Significant Diseases Among Caregivers in a Rural Thai Community by Praditporn Pongtriang, Pilaiporn Sukcharoen, Aranya Rakhab, Vasinee Somsiri and Apinya Ingard in SAGE Open Nursing
Footnotes
Acknowledgments
This research was successful because all participants dedicated themselves to the data collection process to encourage valuable data. Our gratitude goes to the healthcare personnel of the four primary care settings in the Ban Na Derm district for assisting in the completion of data collection; without their dedication, this project would not have been completed.
Ethical Approval
This research has been approved by the Human Research Ethics Committee of Surat Thani Provincial Public Health Office (No: STPHO2023-186). This phase of research strictly considers the sample's privacy and confidentiality rights. The sample received sufficient information before deciding to participate in the research and signed the informed consent to participate in the research project. However, the sample group can withdraw from the research at any time without affecting any contribution to the service in the local healthcare unit.
Author Contributions
PP, PS, AR, and VS designed the research method and developed the research instruments. PP and PS contributed to the instrument validity process. PP, PS, and AR conducted the data collection. AI performed the data analysis. PP and PS drafted the manuscripts in consultation with AR, VS, and AI. All authors reviewed the final version of the Manuscripts. PP is responsible for the Acquisition of funding.
Funding
The National Research Council of Thailand provided support for the research grant (Grant no. N34A660300).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The additional research data supporting the results are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.