
Abstract
Introduction
Cervical cancer (CC) remains a leading cause of morbidity and mortality among women in Sub-Saharan Africa, particularly in Tanzania, despite being preventable through screening and human papillomavirus (HPV) vaccination. Although national strategies exist, uptake remains low. This study explored awareness of CC screening, care, and vaccination among men and women in both urban and rural areas of Kilimanjaro, Tanzania.
Method
A qualitative descriptive design was conducted from April to May 2024. Four Focus Group Discussions with a total of 31 participants (including men and women) were conducted in both urban and rural communities. Simple random sampling was used to select the participants. A semistructured guide covered CC awareness, vaccination, screening, and community engagement. Transcripts were translated, coded, and categorized. Inductive content analysis was used. The study report used Consolidated Criteria for Reporting Qualitative Research guidelines.
Results
Participants showed limited knowledge of CC, its causes, and the benefits of HPV vaccination and screening. Three main categories with eight subcategories emerged: (1) Low health literacy, (2) Challenges in accessing CC prevention, and (3) Community involvement. Myths (e.g., vaccination causing infertility), healthcare system barriers, financial constraints, and stigma contributed to poor uptake. Male and opinion leader involvement was identified as crucial, but both groups lacked accurate information and were not actively promoting CC prevention.
Conclusion
This study highlights limited knowledge and persistent misconceptions about CC and its prevention among men and women in both urban and rural areas of Tanzania. Structural and sociocultural barriers, including low health literacy, financial constraints, gender norms, and misinformation, hinder access to screening and HPV vaccination. Engaging male partners, opinion leaders, and communities through targeted education and improved health communication is essential. These findings provide foundational knowledge to inform policy and design context-sensitive interventions to reduce the CC burden in Tanzania and similar low-resource settings.
Keywords
Introduction
Prevalence
Cervical cancer (CC) is a major global public health issue and the fourth most common cancer among women of reproductive age (Binka et al., 2017; Bray et al., 2018). Over 570,000 new cases and 311,000 deaths occur annually, projected to reach 700,000 cases by 2030 without stronger prevention (Arbyn et al., 2020; Barrow et al., 2020; Runge et al., 2019; WHO, 2022). Sub-Saharan Africa (SSA) bears the highest burden, with 20% of global cases and 24% of deaths (Griesel et al., 2021), and mortality could rise by 50% by 2040 without expanded vaccination and screening (Barrow et al., 2020). In Tanzania, CC is the leading cancer among women, with an incidence rate of 59.1 per 100,000, well above the global average of 13.1 (Bruni et al., 2019, 2022; Gesink et al., 2020). Late-stage diagnosis (Stage III or IV) contributes to poor outcomes, with nearly 7,000 deaths annually (Moshi et al., 2018; Runge et al., 2019).
Prevention
Human papillomavirus (HPV) is the primary cause of CC and can be effectively prevented through screening and vaccination, potentially lowering incidence and mortality by up to 80% (Bénard et al., 2023). However, global vaccine coverage remains low, with only 27% of the target population receiving the first dose well below the 90% target set for 2030 (Simelela, 2021; WHO, 2022). A multicountry study across 78 low- and middle-income countries (LMICs) estimated that full implementation of the WHO 90-70-90 elimination strategy could reduce CC mortality by almost 99%, potentially saving more than 62 million women's lives (Canfell et al., 2020)
In LMICs, CC accounts for over 90% of related deaths (Arbyn et al., 2020; WHO, 2020), yet only 3% of eligible girls receive the HPV vaccine and 44% of women undergo screening (Duncan, 2022). The HPV vaccine uptake in Africa varies from 34% to 93.3%, and safe vaccines combined with screening could reduce incidence by 90% (Gavi, 2021); Gultekin et al., 2020). In East Africa, coverage is only 35%, underscoring the urgent need for improved implementation (Agimas et al., 2024). In Tanzania, CC prevention efforts include the National Cervical Cancer Prevention and Control Strategic Plan (United Republic of Tanzania, Ministry of Health and Social Welfare, 2015) and the introduction of the HPV vaccine program in 2018 (Mphuru et al., 2022). Nevertheless, uptake remains low (Nhumba & Sunguya, 2022), with national screening coverage at just 7.28% (Asgedom et al., 2024) and only 6% of women screened in the Kilimanjaro region (Cunningham et al., 2015). Low screening rates, especially among asymptomatic women, pose a major challenge to achieving the WHO 90-70-90 elimination targets by 2030 (Gultekin et al., 2020; Stefan et al., 2022;WHO, 2022).
Review of Literature
Prevention, early treatment, and raising awareness of CC are crucial to reducing the disease burden. Low levels of CC screening and HPV vaccination are linked to poorer awareness of available prevention services in rural compared to urban areas. Contributing factors include the absence of screening and HPV vaccination services in rural settings, low health literacy on CC and HPV infection/vaccination (Zhetpisbayeva et al., 2023), low coverage of CC screening and vaccination, financial constraints from out-of-pocket expenses, and geographical barriers (Appiah et al., 2025), all limiting access to healthcare services in rural areas. Social and cultural barriers (Asgedom et al., 2024) are also more prominent, while a shortage of qualified practitioners further reduces participation in prevention strategies in rural settings (Appiah et al., 2025; Banks et al., 2022).
Patel et al. (2020) found that low awareness among women led to poor screening uptake. In SSA, awareness of CC is generally low, especially in rural areas where 60–80% of cases occur (Drokow et al., 2020; Moshi et al., 2018; Osei et al., 2021). A lack of knowledge about prevention increases CC risk (Binka et al., 2017). Many women are unaware of CC symptoms, causes, or screening options before diagnosis, with some patients reporting shock upon learning about HPV (Demissie et al., 2022; Jibat et al., 2024). Low public awareness exacerbates CC morbidity and mortality by hindering the uptake of preventive measures (Binka et al., 2017; Shrestha et al., 2020). Education campaigns have shown success in correcting misconceptions, increasing screening, and improving awareness about CC and HPV vaccination (Cooper et al., 2021; Osei et al., 2021). In Tanzania, myths about HPV affecting fertility, spread by community leaders, have further limited vaccine uptake (Cinya & Mubangizi, 2024). A study in Kilimanjaro found that although many women were aware of CC, only 6% had been screened, and knowledge of HPV vaccination was low (Cunningham et al., 2015). There are limited qualitative research on community-level factors influencing CC awareness, as most studies are facility-based in SSA. Therefore, this study aimed to explore awareness of CC screening, care, and vaccination in urban and rural areas among men and women in Tanzania.
Method
Study Design
This is a qualitative descriptive design, employing inductive content analysis to investigate awareness of CC screening, care, and vaccination among men and women in urban and rural areas of Tanzania. Data were collected through Focus Group Discussions (FGD; Krueger & Casey, 2015), a method suitable for capturing in-depth public insights. This approach was considered appropriate as qualitative methods are particularly effective for understanding participants’ experiences and perspectives of CC (Creswell & Poth, 2016). The study adheres to the Consolidated Criteria for Reporting Qualitative Research checklist, focusing on aspects such as research team reflexivity, study design, data analysis, and findings (Tong et al., 2007), see Appendix 1.
Research Questions
Are women and men in urban and rural areas of Kilimanjaro aware of CC screening, care, and vaccination? What are the contextual and sociocultural factors that influence awareness and uptake of CC prevention services in these communities?
Sample
A simple random sampling approach was used to select the study setting and participants. The study participants were men and women aged 18 and above in the Kilimanjaro region, which consists of seven districts. Two districts, Moshi Urban and Moshi Rural, were purposively chosen due to their high CC prevalence. The sample was drawn from communities with a high prevalence of CC, specifically the Moshi Urban and Moshi Rural districts of the Kilimanjaro Region, selected to capture populations most affected by the disease. According to data from the Kilimanjaro Population-Based Cancer Registry, the overall prevalence of CC in the region is 11.6%, with Moshi Rural exhibiting the highest prevalence at 57% (Kilimanjaro Christian Medical Centre, Cancer Care Centre, 2022).
Recruitment of Participants for FGD
From each district, two wards were randomly selected in Moshi Urban and Moshi Rural. In each ward, the respective Ward Executive Officer was contacted by telephone and appointments were arranged to present the study's purpose. Thereafter, one street in the urban area and one hamlet in the rural area were randomly chosen. The ward executive officer informed the local street chairpersons about the study and they, in turn, invited 10-cell leaders (local leaders) and introduced the principal investigator (PI). Using household lists provided by these leaders, eligible households were identified through systematic sampling. From each household, one adult (man or woman aged 18+) was randomly selected from a list of adults in the home. This process ensured a diverse and representative community sample. Selected participants were contacted by phone and invited to participate in FGDs the following day.
A total of 31 participants were recruited for the FGDs. Four face-to-face FGDs were conducted: two groups consisting of male participants and two groups consisting of female participants in urban and rural areas, respectively. Each group included members from different age brackets, ranging from 18 to 69 years, and comprised between 5 and 11 individuals. This diverse composition allowed for a broad representation of perspectives across genders and age groups (Krueger & Casey, 2015). All participants provided written informed consent and participation was voluntary. All participants were eligible to participate in the study regardless of their CC status. However, none of the participants had CC.
Inclusion Criteria
Men and women >18 years of age (without considering their CC status) and those who could speak Swahili.
Exclusion Criteria
Those who were not around during the data collection period were excluded from the study and those who did not provide informed consent.
Ethical Considerations
The study adhered to the guidelines on research on human subjects. The Declaration of Helsinki (WMA, 2013) ethical clearance certificates were obtained from the KCMC University Research Ethics Review Committee and the National Institute for Medical Research, Tanzania. The directors of the respective study sites granted permission. Written informed consent was obtained from participants, and participation in the study was voluntary. All information collected was handled at a high level of confidentiality. The participants had the freedom to withdraw anytime during the study without any negative consequences.
Data Collection
A semistructured FGD guide, (Appendix 2), was developed by researchers based on the study's objectives (Krueger & Casey, 2015). It included sections on sociodemographic characteristics, general awareness of cancer and CC prevention, risk factors, signs, and symptoms. The interview guide was initially created in English and translated into Kiswahili by bilingual researchers, followed by back-translation to ensure linguistic suitability for the community (Behr, 2017). The tool was piloted among male and female community groups of seven participants to assess the understanding of the guide. Only minor adjustments, such as typographical corrections and resequencing of questions, were made.
Data collection took place between April and May 2024. The same interview guide was used for all participants in every session. All FGDs were conducted face-to-face in the respective ward office conference room, with participants seated in a semicircle arrangement. All participants signed informed consent forms before the discussions started, following Marshall and Rossman (2016).
To maintain confidentiality, each participant was assigned a number displayed on paper for identification purposes. With participant consent, the FGDs were recorded using two digital recorders to ensure audio backup. The FGDs were moderated by two facilitators: for female groups, the first author (PhD student with an MSc in public health) and a female moderator; for male groups, a male social scientist with a master's degree in public health and extensive experience in qualitative research.
In the female FGDs, the social scientist acted as the note-taker, while the first author took notes during the male FGDs. All facilitators were assistant lecturers at the time of data collection. Each discussion lasted between 60 and 90 min. Data were collected only once, and transcripts were not returned to participants for review, though member checks were employed to enhance data accuracy. After each FGD, transcription and translation were completed, and data analysis began immediately, including data familiarization. Data saturation was reached after the third FGD in rural areas; however, the researchers agreed to conduct an additional (fourth) FGD in urban areas to confirm whether any new information would emerge.
Data Analysis
Data was analyzed using content analysis with an inductive approach inspired by Graneheim and Lundman (2004). The inductive content analysis was chosen, as the field was unexplored. This approach was chosen to explore the phenomenon directly from the participants, rather than being predetermined (Polit & Beck, 2017). The FGD audios were transcribed verbatim in Kiswahili. The transcripts were validated, meaning checked for quality, rigor, and relevance as per the audios, and later translated from Kiswahili into English by a bilingual Tanzanian for easy joint analysis for the whole research team and those who do not understand Kiswahili. The researchers read the transcripts several times to understand and be conversant with the transcripts to ensure the data quality. Checking the Kiswahili and English have the same meaning was also done before going to the next step of coding and analysis. The next step started with marking meaningful units in the transcripts. These were then condensed and given codes. Data was coded by three independent researchers. The codes containing similar meanings were developed into eight subcategories. Through this inductive analysis, developed by Graneheim and Lundman (2004), the subcategories were merged into three main categories. The researchers reached a consensus in the last step, see Table 1.
Composed Main Categories, Subcategories, and Codes.

CC: cervical cancer.
Rigor
To establish trustworthiness and rigor of the findings and research free from researcher bias, study's adherence to the trustworthiness criteria: credibility, dependability, transferability, and confirmability (Stenfors et al., 2020). Credibility was achieved by letting the data guide the analysis, supported by diverse samples from rural and urban areas, enhancing representativeness. Dependability, or data stability over time and conditions (Elo et al., 2014), was ensured through rigorous methods, including independent analyses, transcript validation, and bilingual translations. Inductive content analysis, participant quotations, and consensus on themes ensured confirmability. Transferability was strengthened by involving participants from varied settings, making the findings applicable to similar groups and contexts (Lincoln & Guba, 1985).
Results
Sociodemographic Results
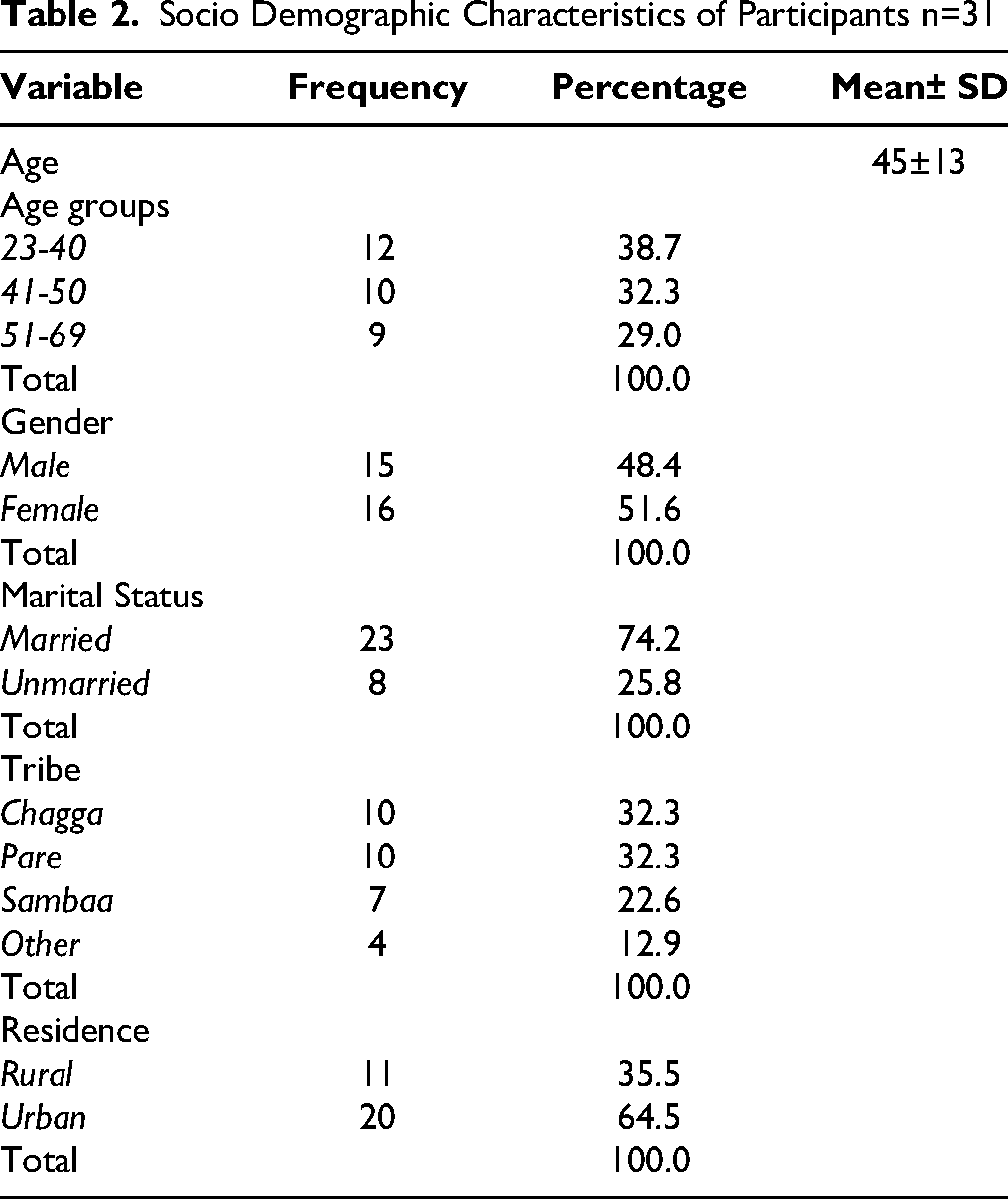
A total of 31 participants (16 females and 15 males) took part in four FGDs. Of these, 20 participants were from urban settings and 11 from rural areas, ensuring a diverse representation of perspectives across gender and geographical contexts. Further details of the participants’ characteristics are provided in Table 2.
Socio Demographic Characteristics of Participants n=31
Research Questions Results
Regarding the research questions, the content analysis generated 20 codes from the raw data, eight (8) subcategories, and three (3) main categories: Low health literacy, Challenges in accessing CC prevention, and Community involvement. The three (3) main categories with eight (8) subcategories, as well as the codes, are presented in Table 1.
Low Health Literacy
This category highlights the generally low level of awareness regarding CC among participants across all groups. Many individuals were unaware of the causes of the disease and had never heard of HPV, HPV vaccination, or associated risk factors. The subcategories within this category are: The silent disease and Myths and traditional beliefs about CC.
The Silent Disease
Most participants reported that discussions about CC are virtually absent within the community. Although there is a general sense of concern regarding the threat posed by CC, the community lacks detailed knowledge about the disease. As a result, individuals are unsure of what to discuss and remain silent, lacking the confidence to address the topic due to insufficient awareness. Male participants, in particular, noted that conversations about CC are rare because people generally do not know what information to share with friends or neighbors during social interactions. This silence was, however, observed among both women and men, in both rural and urban areas, rendering CC a “silent disease” within the community and underscoring the low level of awareness, as illustrated in the excerpt below. Women are not aware of CC, because when you sit with the majority of the community surrounding us, especially the middle aged, you cannot hear them talking about CC that is caused in this way and that way. The government is silent, the community is silent, and the family is silent. The leaders in the community don't know, so they don't talk to the community, and everyone in the community is quiet! (FGD 2; Male rural
Myths and Traditional Beliefs About CC
All groups revealed a lack of coherent understanding of HPV vaccination, largely due to the spreading of incorrect information about CC prevention within the community. Participants expressed concerns and uncertainty regarding the government's recommended strategies for CC prevention, including vaccination and screening, as a result of ambiguous narratives and rumors circulating within the community. One widespread rumor suggested that the vaccines had been imported from abroad with the intent of causing infertility, allegedly targeting young girls to prevent them from having children. This misinformation led many parents and guardians to reject the vaccination of their daughters, often keeping them at home on vaccination days to avoid participation in the program. But for sure, many parents from our street said - don't vaccinate your children. They will not be able to bear children at all if vaccinated. We agreed in the community that we should stop children from going to school on that day because they will not bear children. After all, HPV vaccination kills all the eggs. (FGD4; Female urban)
Furthermore, participants in the male groups expressed the belief that CC is hereditary and cannot affect an individual unless there is a family history of the disease. They explained further that if they trace their family history and find no evidence of CC among relatives, they feel unconcerned about the risk. Consequently, this perception leads participants to believe that vaccination and screening are unnecessary for preventing the disease. Others believe it is something that is inherited from the family, so it is not for them. They think they can't get the disease because of no history of the disease in their family. So, they take it easy; they don't take it seriously. (FGD1; Rural male)
Participants also shared several myths about the CC screening procedure, influenced by rumors circulating within the community. One widely held belief was that during screening, the uterus is temporarily removed to obtain a sample and then returned to the body. Additionally, women's groups in both rural and urban areas perceived the screening process as dangerous, based on the belief that taking a biopsy leaves a scar on the cervix, potentially causing harm. I heard that when you go for screening, the uterus is pulled out and then will be pushed in after screening. Yes! I heard women gossiping at the veranda lots of stories one saying, yes, when you go for screening the uterus pulled out and put hanging there and picked and picked! You see my mother died! You see like that, if am very fine, will I go? (FGD 1; Female rural)
Concerning prevention and treatment for CC, participants expressed the belief that the disease cannot be prevented or cured. They stated that available medical interventions are solely for palliative care, aimed at alleviating symptoms rather than providing a cure. Furthermore, the community widely held the view that prayer is the only means of preventing CC. Altogether, there is no treatment for CC, you will go and be given medication to help you add some days to life. Yes, I repeat, no medication. The only medicine there is to help you …. is life-prolonging, but for cancer, in general, there are no treatments. We need ONLY to pray to our God to help us! (FGD2; Male rural)
Challenges in Accessing CC Prevention
Several barriers were identified as hindering the utilization of CC prevention services and efforts within the community. Personal, family, healthcare-related, and community-level barriers were highlighted as important challenges in accessing CC prevention. For instance, many women reported a lack of time due to busy schedules spent earning a livelihood and fulfilling household responsibilities. Additionally, cultural barriers were noted, as some women required their husbands’ approval to access prevention services. However, many husbands were unaware of the importance of CC prevention, further complicating efforts to address the issue. These challenges are evident in the three subcategories: Inadequate healthcare facilities, Family and community barriers, and Women's health versus financial priorities.
Healthcare Facilities Barriers
In the women's FGDs, participants narrated that when they visit healthcare facilities and hospitals, healthcare providers often attribute health concerns solely to urinary tract infections (UTIs) or intestinal worms, which are perceived as the most common health issues in the community. This limited diagnostic approach means that further investigation into other potential conditions, such as CC, is rarely pursued. Moreover, CC screening services are unavailable at local healthcare centers, with UTI and deworming treatments being the primary services readily accessible to the community. Participants also highlighted that accessing CC screening services requires traveling to distant healthcare facilities, which involves additional costs, such as travel expenses, creating a significant barrier. Furthermore, the time needed to walk long distances to these facilities contributes to delays in seeking CC-related healthcare services, as women often feel that the effort and time investment are burdensome leading to a feeling of wasted time. UTI, or worms is what most healthcare providers think is the problem and is what they treat before doing a thorough assessment! Yes, no further diagnosis because the provider will be treating UTI but you might have been affected with CC already you don't know it grows. You find the next day you go with the same complaint, and you are given the same diagnosis and medication, and the problem becomes big! (FGD 1; Female rural)
Family and Community Barriers
The current situation, characterized by a lack of parental involvement in school-based vaccinations for CC, results in parents preventing their children from receiving the HPV vaccine. This issue was particularly noted during the FGDs with women in rural areas. … You know this thing about vaccination comes from school through our children, but we don't know anything as parents, as we are not informed and not involved as parents. This causes some parents to prevent their daughters from going to school during the day of vaccination. You find the vaccination might be very important, but a parent prevents a child from getting vaccination because we don't know the alpha or omega. (FGD1; Female rural)
The lack of effective health education on CC within communities was identified by participants as a barrier to CC prevention initiatives. Participants explained that without adequate information about screening and HPV-vaccination, community acceptance and uptake of these preventive measures are likely to remain very low. Lack of information/awareness on HPV vaccination is a barrier … but if people get proper information and awareness … no one will hinder acceptance of the vaccine, … if they get an education they will go for screening … if not, they won't go, and even currently, they are not going because they are not aware. (FGD1; Female rural)
Women's Health Versus Financial Priority
The participants narrated that they are busy earning some money for their daily living and do not have time for health checkups. For women, not yet sick, health is not an immediate priority as financial priorities come first, to get money for daily food. … I don't have time - instead of going for screening, … I'd better go to the farm and look after my rice paddy and my tomatoes, … I want to go to “Manyema” (a local market in Moshi), and earn a living. The time I go for screening, what will my children and I eat? That is what causes women from Kilimanjaro not to go for testing/screening. (FGD4; Female urban)
Furthermore, it is not common practice in the community to go for health checkups without being sick. The custom is that people wait until they feel sick; to go to the hospital for treatment remedy is the normal practice among the participants. Furthermore, it happens that if somebody plans to go for screening or to vaccinate the daughter, the community discourages it because going to the hospital is common only for those showing sickness but not for those appearing healthy. The problem for us people in the lower class, we wait until a person gets sick and is told having this disease. But you cannot see a person going only for check-ups, for screening without being sick (laughing)! Screening is money and she doesn't have money, most in the community wait until they get sick is the time they go for treatment. (FGD2; Male rural)
Fear of Abandonment
The female participants stated fear of abandonment as a reason which hinders the utilization of CC preventive services. If they would receive a positive result after screening, they fear that they will be abandoned by their husbands. To be diagnosed with CC is seen as a stigma in the community, which leads to abandonment. Also, women are afraid of testing/screening. I saw one woman who went for screening, and she told her husband that I went for screening and was found to have CC symptoms. They continued to live, and the husband had to run away from that woman. “As she has that disease, she is of no use to me,” he runs away. So, a woman can go for screening and still fear to disclose in the community. They are afraid because many marriages have been broken because of CC (FGD4; Female urban).
The Role of Community Involvement
Community involvement plays a major role in any program intervention. Participants narrated there was a low level of involvement, and most of the stakeholders were not involved and informed about CC screening and vaccination. Within this category, this is further developed in the subcategories of male involvement and involvement of community leaders.
Male Involvement
The participants narrated that male involvement in CC prevention could significantly enhance support for CC screening and vaccination. Culturally, men are regarded as heads of the family and primary decision-makers, giving them substantial influence over their wives’ and daughters’ acceptance of CC prevention measures. Male participants explained that women cannot independently decide to undergo screening or take their daughters for vaccination without their husbands’ approval.
Men expressed that women could not decide to go for screening or even take their young girls for vaccination without their husbands’ approval, and educating men on CC prevention will enhance women’s habit of going for screening and vaccination. They further emphasized that educating men about CC prevention could encourage women to adopt regular screening habits and ensure their daughters receive the HPV vaccination without their husbands’ approval. Involving both males and females in awareness about the prevention of cervical cancer will influence women/wives to go for screening and vaccination to prevent CC because men have power in decision-making. He is the head of the family, and women cannot just decide to go for screening for CC. They will only go if their husbands sensitize them to go. (FGD2; Male rural)
The quote above shows that women are vulnerable and dependent on their husbands’ understanding of the severity of CC and their approval to seek healthcare
Involvement of Opinion Leaders
Participants emphasized the importance of involving local government and religious leaders in promoting acceptance of HPV vaccination and screening within the community, as these leaders are often more trusted to deliver culturally sensitive information than healthcare providers. However, it was noted that local leaders rarely address the topic of CC due to a lack of adequate information. Engaging these leaders in disseminating accurate information about CC could considerably enhance community acceptance of prevention strategies, as they are highly trusted as representatives of the government. If the government leader passes over the announcement to insist on CC screening and HPV vaccination, this will reassure the community, because the leader could not accept something that destroys the community. You will go and tell your child to go for that vaccination! Yeah, because you have proper information from your leader in that community! (FGD2; Male-rural) They can inform us through the village leaders, and we will understand vaccination. (FGD 1; Female rural)
Discussion
This study investigated awareness of CC screening and vaccination among men and women in urban and rural areas of the Kilimanjaro region, Tanzania. Findings revealed three main categories: Low health literacy, Challenges in accessing CC prevention, and Community involvement. There is a critical need to address health literacy to dispel prevalent myths about screening and vaccination. Barriers such as healthcare infrastructure limitations, family dynamics, and community factors significantly impede service utilization. Engaging men and community opinion leaders could promote greater acceptance of vaccination and screening programs.
Low Health Literacy
The study found low health literacy on cervical CC, with limited knowledge and confidence to discuss the disease. Poor public awareness underscores the need for better information dissemination, such as brochures and social media, which have proven effective for CC prevention (Baharum et al., 2020; Petersen et al., 2022). Unlike prior studies, participants were largely unaware of risk factors, including HPV and its vaccine (Chelva et al., 2024; Demissie et al., 2022; Drokow et al., 2020; Jibat et al., 2024; Lin et al., 2020; Rick et al., 2019), though women in both urban and rural areas identified multiple childbirths as a risk factor, an understanding absent among men. In contrast, Swai et al. (2023) found high awareness of CC risk factors, HPV, testing eligibility, and screening benefits, likely due to their hospital-based setting. Okyere et al. highlight the need for community sensitization and behavioral change to improve vaccination and screening uptake. Extensive campaigns have enhanced public confidence in discussing health issues, and similar efforts could boost CC awareness, increase preventive service use, and reduce CC-related morbidity and mortality, contributing to economic growth.
Participants in the present study believed that HPV vaccination causes infertility among their daughters, discouraging its acceptance in both urban and rural communities. This misconception, prevalent among women's groups, reflects a lack of awareness regarding the vaccine's role in preventing CC, despite the WHO (2024) confirming its safety and efficacy. Similar myths associating the vaccine with infertility or family planning have been reported in other studies (Chona et al., 2023; Hasahya et al., 2016). Additional concerns about vaccine complications, as noted by Almehmadi et al. (2019) and Drokow et al. (2020), further contribute to rejection. Dispelling these myths and emphasizing the vaccine's benefits is essential for increasing uptake and reducing the CC burden.
Misinformation about CC screening was found in this study, which limits women's access to preventive services. False beliefs increase fear and reduce screening uptake in rural and urban areas (Chona et al., 2023; Cunningham et al., 2015; Petersen et al., 2022). Some participants incorrectly believed that the cervix pulled out during screening, which reflects a lack of accurate information, also confirmed in research (Hasahya et al., 2016). Furthermore, the perception of CC as solely hereditary lowers perceived risk, particularly among men in rural areas, who see no need for vaccination or screening. This aligns with findings by Adedimeji et al. (2021). Addressing these myths through community education could help meet WHO's (2020) goal of screening 70% of women aged 35–45, enabling early CC detection and treatment in LMICs.
Challenges in Accessing CC Prevention
This study identified key barriers to CC prevention, including inadequate healthcare infrastructure, limited parental involvement in HPV vaccination, financial constraints, cultural factors, and fear of abandonment. Rural women faced added challenges such as long travel distances, transport costs, and time spent accessing urban screening services, consistent with earlier studies (Asgedom et al., 2024; CDC, 2024; Gizaw et al., 2022; Hussein et al., 2024; Isaacson et al., 2023; Srinath et al., 2023). Long wait times and associated costs also deterred use, particularly in rural areas where facilities are less equipped (Adedimeji et al., 2021; Bensemmane et al., 2022; Chapola et al., 2021).
Parental involvement was a barrier, especially among rural women and urban men, with parents feeling excluded from HPV vaccination decisions for their daughters, leading to hesitancy (Ho et al., 2022; Mihretie et al., 2022; Osei et al., 2021; (Tobaiqy & MacLure, 2024) For rural women, cultural beliefs and low education may discourage provider engagement, while urban men's family health concerns drive their interest in inclusion. In contrast, higher parental acceptance has been reported when providers offer information (Anyaka et al., 2024; Davies et al., 2021). Strengthening parent–teacher partnerships and public awareness could improve uptake.
Financial difficulties significantly impacted healthcare prioritization, with urban men and women reporting that daily expenses took precedence over health, consistent with findings by the Osei et al. (2021), and Adler et al. (2023). Cultural norms favoring health-seeking only when symptomatic further lowered screening and vaccination rates (Adler et al., 2023; Tapera et al., 2019).
Fear of abandonment was another barrier, especially among urban women, who feared stigma and partner rejection if diagnosed with HPV or CC. This fear, often linked to low health literacy, reflects findings from other studies where women faced blame or abandonment after diagnosis (Chona et al., 2023; Dirar et al., 2022; Morse et al., 2023). Such concerns discourage screening and treatment, perpetuating low uptake (Bateman et al., 2019; Defo & Domgue, 2020; Ragan et al., 2018; Srinath et al., 2023).
Community Involvement
Engaging men in health promotion is crucial for effective CC prevention. This study found that rural and urban participants supported male involvement in HPV screening and vaccination to boost acceptance and uptake (Tobaiqy et al., 2023). Men were willing to support partners and vaccinate daughters if provided accurate information, consistent with findings from Uganda (de Fouw et al., 2023). Women's participation in CC screening is often shaped by male partners, who control resources and grant service permission, particularly in African contexts where men are key decision-makers (Adedimeji et al., 2021; Chapola et al., 2021; Chelva et al., 2024; de Fouw et al., 2023; Drokow et al., 2020; Jibat et al., 2024; Mantula & Toefy, 2023).
Opposition from male partners can hinder uptake, with married women sometimes less likely to be screened (Adewumi et al., 2019; Gizaw et al., 2022; Srinath et al., 2023), highlighting the need for effective male engagement. Involving trusted community leaders, such as religious and government figures, can also improve acceptance of CC prevention (Adewumi et al., 2019; Mantula & Toefy, 2023; Tapera et al., 2021). However, this study found these leaders were not actively promoting such services, likely due to low health literacy and misconceptions that can hinder HPV vaccine uptake (Cinya & Mubangizi, 2024). Training and sensitizing opinion leaders is therefore critical for improving outreach, acceptance, and early detection.
Study Strengths and Limitations
This study provides valuable insights into community experiences with CC prevention by incorporating perspectives from both men and women. Two skilled qualitative researchers (male and female) conducted focus groups, ensuring participant views were well represented (Creswell & Poth, 2016). Adherence to trustworthiness criteria, credibility, dependability, transferability, and confirmability (Stenfors et al., 2020) was achieved through diverse sampling, rigorous procedures such as transcript validation, bilingual translation, and independent coding (Elo et al., 2014), and consensus-based inductive analysis (Lincoln & Guba, 1985). While limited to specific geographic areas and subject to the inherent subjectivity of qualitative research (Polit & Beck, 2017), the study's methodological rigor and varied contexts strengthen the applicability of its findings.
Implications for Practice
The study found low awareness of CC in both urban and rural areas, underscoring the need for targeted interventions. These results provide baseline data to guide tailored health programs and inform policies that promote screening and vaccination among both adults and children. Such initiatives can increase preventive service use, helping Tanzania and other LMICs in SSA work toward the WHO elimination target and reduce CC-related morbidity and mortality (WHO, 2022).
Conclusions
The study revealed that both men and women in urban and rural Tanzania had limited knowledge and several misconceptions about CC, its causes, screening, care, and HPV vaccination. Awareness of HPV and its preventive role was low, and beliefs like the vaccine causing infertility or CC being hereditary and untreatable were common. Sociocultural factors as gender norms, fear of abandonment, and lack of parental involvement, strongly influenced awareness and attitudes. Structural barriers, including long distances to health facilities, financial constraints, and limited outreach, further hindered access. Male partners and community opinion leaders were identified as key influencers, yet they lacked adequate information. The findings highlight an issue of low health literacy and the urgent need for community-based education and improved health communication to support participation in CC prevention.
To address these gaps, integrating CC education into school curricula for both girls and boys would promote early awareness, support HPV vaccination uptake, and reduce future disease burden in line with WHO's 90-70-90 targets and Sustainable Development Goal (SDG) 3 (United Nations, 2015). Healthcare providers should counter prevailing myths with evidence-based information, while strengthening women's health literacy supports gender equality and informed decision-making (SDG 5). Training trusted community stakeholders, local leaders, religious figures, and community health workers in culturally sensitive CC prevention can improve community trust and uptake of screening and vaccination, contributing to national and global CC elimination goals. Overall, this study adds important evidence on community perspectives and barriers to CC prevention in both rural and urban contexts in Tanzania, underscoring the need for tailored interventions that can strengthen awareness, promote equitable access, and ultimately reduce the CC burden in the country and comparable settings.
Footnotes
Authors’ Note
The work was carried out at KCMC University, Tanzania, and the data was collected in Tanzania.
Acknowledgments
The authors gratefully acknowledge the study participants in Moshi rural and Municipal Kilimanjaro, Tanzania and staff at Kilimanjaro Christian Medical Centre engaged in the data collection.
Ethical Statement
This study adhered to the guidelines on research as per the Declaration of Helsinki regarding research on human subjects. Ethical clearance certificates were obtained from the KCMC University Research Ethics and Review Committee No. 2626 and the National Institute for Medical Research, Tanzania (NIMR) No. NIMR/HQ/R.a8/Vol.IX/4589. Permission was obtained from the Municipal Executive Directors for the Moshi-urban district and the District the Moshi-rural district. Written informed consent was obtained from the participants. For confidentiality purposes, participants were identified using numbers and not names, also they were reminded not to mention their names during the FGD.
Author Contribution Statements
CM, GB, DM, JM, JC, and PK conceptualized the study; CM, RM, and PK did the data collection, transcription, and translation. The data analysis was done by CM, GB, JM, JC, HM, DM, RM, and FS. The Manuscript was drafted by CM and all authors reviewed, edited, and approved the final version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Appendix 1. COnsolidated criteria for REporting Qualitative research (COREQ) Checklist
A checklist of items that should be included in reports of qualitative research. You must report the page number in your manuscript where you consider each of the items listed in this checklist. If you have not included this information, either revise your manuscript accordingly before submitting or note N/A.
Source. Developed from: Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. International Journal for Quality in Health Care. 2007. Volume 19, Number 6: pp. 349–357.
Once you have completed this checklist, please save a copy and upload it as part of your submission. DO NOT include this checklist as part of the main manuscript document. It must be uploaded as a separate file.
Appendix 2.
Interview Guide FGD
"Cervical Cancer—A Silent Disease in the Community”—A Qualitative Study on Awareness of Cervical Cancer in Tanzania
Introduction and warm-up:
Thank you for coming to the Focus Group today. First, we will collect sociodemographic details by filling in the piece of paper provided. You will identify with yourselves using the numbers provided to each of you, visible to everyone. You are encouraged to speak freely and share your personal opinions and experiences from your community. Remember, there is no right or wrong response.