
Abstract
Background
Leadership is a multifaceted process that inspires individuals to take action while providing the necessary support and motivation to achieve collaboratively set goals. Ineffective leadership among nurse managers has contributed to low morale, increased staff turnover, shortages, and rising healthcare costs.
Purpose
This research aimed to assess nurses’ perceptions of leadership practices and the factors influencing these practices of their managers.
Methods
A cross-sectional study was carried out at a facility involving 422 nurses, who provided data through a structured self-administered questionnaire. Descriptive statistics, as well as bivariate and multivariable linear regression analyses, were used to determine the factors associated with nurses’ views on their managers’ leadership practice. Variables with p-values less than .05 were considered statistically significant.
Results
Out of 422 respondents targeted, 403 completed the survey, yielding a response rate of 95.5%. The results showed that 125 nurses (31%) had a low perception, 164 (40.7%) had a moderate perception, and 114 (28.3%) had a high perception of their managers’ leadership styles. Factors influencing nurses’ perceptions included the lack of leadership training (β = −5.47, 95% CI: −8.548, −2.395), organizational commitment (β = 0.52, 95% CI: 0.361, 0.684), innovative work behavior (β = 1.1, 95% CI: 0.918, 1.250), and job-related stress (β = −0.13, 95% CI: −0.222, −0.039).
Conclusion and Recommendation
Less than one-third of nurses view high perception toward their managers’ leadership practice. Key factors associated with these perceptions include a lack of leadership training, levels of organizational commitment, innovative work behavior, and job-related stress. It is suggested that future research employ mixed methods to better understand nurses’ perspectives on their managers’ leadership practice.
Keywords
Introduction
Leadership in a healthcare organization is considered as a key element for assuring quality healthcare service, staff satisfaction, and financial performance (Smith & Ricci, 2015). Leadership is the ability to influence the attitudes, beliefs, and abilities of employees to achieve their organizational goals (Shafiu et al., 2019). Nursing leadership is a complex concept which is motivating nurses to improve quality of clinical care (Alvinius, 2017). Leadership practice is the demonstration or application of leadership skills (Northouse, 2021). Effective leadership practice in health care revolves around the improvement of quality patient care and outcomes, employee satisfaction, and financial performance (Akdere & Egan, 2020). Moreover, in organizations, the perceptions held by leaders and employees significantly influence the workplace climate and overall effectiveness. It's essential to recognize that perception is often conveyed through communication within any organization, regardless of its size, making it a vital leadership tool (Moslehpour et al., 2018). In the workplace, when there are stark differences in perceptions between employees and employers regarding aspects such as quality, quantity, and schedules, achieving meaningful objectives becomes challenging (Sean A. Newman, Robert C. Ford, Greg W. Marshall, 2020, n.d.). Typically, leaders in many organizations possess three primary skills: vision, interpersonal abilities, and technical expertise. However, one critical skill that is often overlooked is perception (Nandasinghe, 2020). Having the right perception is essential for effective leadership. A leader may have the best intentions and genuine concern for their employees, but if they fail to communicate in a way that employees can understand, those intentions may be misinterpreted (Robert & Maher, 2015). A leader who is attuned to employees’ perceptions must utilize communication to either reinforce positive views or alter negative ones. Cultivating the right perception goes beyond being competent and productive; it also involves embracing diversity and fostering harmonious relationships with all employees (Brown et al., 2019).
The absence of effective leadership practices among nurse managers is a contributing factor to low morale, resulting in staff turnover, shortages, and rising healthcare costs (Dassanayake, 2014; M Alshahrani & Baig, 2016). Healthcare systems globally are encountering numerous intricate challenges in delivering high-quality, safe, and cost-effective care. These challenges arise from evolving systems, rising healthcare costs, technological advancements, and a growing severity of patient illnesses (Porter-OGrady & Malloch, 2011). Managers are challenged with resolving these problems using critical thinking, especially leadership skills in healthcare (Ledlow & Coppola, 2013). Despite its significance, there was a dearth of published studies in Ethiopia regarding perception toward managers’ leadership practice among nurses to the researchers’ extent of searching. Therefore, the purpose of this study aimed to assess nurses’ perceptions of leadership practices and the factors influencing these practices of their managers.
Literature Review
Healthcare organizations today face the dual challenge of providing excellent patient care and fostering a highly engaged and satisfied workforce. Effective nurse leadership is crucial for cultivating satisfied and committed staff nurses who directly deliver patient care (Khan et al., 2018). A cross-sectional study conducted in New York on staff nurses’ perceptions of their nurse managers’ leadership behaviors showed that leadership practice of nurse managers was moderate as perceived by staff nurses (Khan et al., 2018). A similar study conducted in New York on clinical nurses’ perceptions of their managers’ leadership indicated that nurses perceive their managers’ leadership practice at an average or moderate level (Raso et al., 2020).
A cross-sectional study conducted in China on the relationship between nurse managers’ leadership practice and job satisfaction among registered nurses stated that leadership practice of nurse managers as perceived by clinical registered nurses was moderate (Mirzaei et al., 2024). A study conducted in Rwanda military hospital showed that 22%, 43.8%, and 34.4% of nurses have low, moderate, and high perception toward their managers’ leadership practice, respectively (Nyirazigama, 2017).
In African nations, the shortage of nurses, driven by various factors, poses significant challenges for nurse managers in exercising effective leadership (Crisp & Chen, 2014). The failures within healthcare systems in sub-Saharan Africa can be attributed to weak or ineffective leadership capabilities (Crisp & Chen, 2014; Mutale et al., 2017). The absence of strong leadership has been recognized as a significant barrier to expanding and providing affordable services in low-income countries (Mutale et al., 2017). Research conducted in East Africa highlighted that the involvement of nurse leaders in health policy is crucial for influencing decisions, fostering relationships, communicating effectively, feeling empowered, and demonstrating professional credibility. Nevertheless, a considerable number of these leaders remain excluded from participating in the policymaking processes that impact nursing leadership practices (Shariff, 2014).
Ineffective nursing leadership contributes to a 21% increase in staff turnover, along with lower satisfaction among nursing staff, decreased productivity, and reduced effectiveness, which are affected by 17%, 17.1%, and 17.7%, respectively (Cummings et al., 2010; Nyirazigama, 2017). Research indicates that nursing leaders are frequently selected for their clinical expertise rather than their leadership abilities. This reliance on clinical skills can lead to difficulties for healthcare systems in empowering staff nurses and fostering a positive work environment that promotes effective nursing practice (Asiri et al., 2016). To the best of searching different studies revealed a lack of published studies in Ethiopia concerning nurses’ perceptions of managers’ leadership practices. Therefore, this study aimed to assess nurses’ perceptions of leadership practices and the factors influencing these practices of their managers.
Research Questions:
What is the perceived quality of leadership practices among managers, as reported by nurses working in public health facilities? What factors influence nurses’ perceptions of managers’ leadership practices within the public health facilities?
Research objectives:
To assess nurses’ perceptions of leadership practices of their managers To identify factors affecting nurses’ perceptions of managers’ leadership practices
Conceptual Framework
The conceptual framework used in this study was adapted from different literatures (Ahmed et al., 2019; Fardellone et al., 2014; Muksoud et al., 2021; Nanyonga et al., 2020; Rindu et al., 2020) (Figure 1).

Conceptual Frame Work on Perception Toward Managers’ Leadership Practice and Associated Factors Among Nurses Working at Jimma Town Public Health Facilities, 2021.
Methods
Source of Population: All nurses who were working at Jimma Town public health facilities Study Population: Sampled nurses who were working at Jimma Town public health facilities during the data collection period.
Study Design
This study employed cross-sectional design (Jimma, 2025). Researchers would like to clarify that this manuscript is part of a study previously published (Gashaye et al., 2023), where certain methods and information may overlap, despite its significance. The study was conducted in public health facilities in Jimma Town, which is situated in the Jimma Zone of the Oromia Regional State, about 352 km southwest of Addis Ababa. Jimma Town includes four public health centers, one general hospital, one medical center, and three private primary hospitals. According to information from the Jimma Town Health Office, there are 39 nurses across the four health centers, 641 at Jimma Medical Center (JMC), and 57 at Shenen Gibe Hospital, resulting in a total of 737 nurses in the public health facilities of Jimma Town. The research was carried out from August 16, 2021, to September 16, 2021.
Study Population and Sampling
The study involved 422 nurses. The sample size was calculated using a single population proportion formula, considering a 95% confidence interval (1.96), a 5% margin of error (0.05), and a population proportion of 50% (0.5) due to the lack of existing research on this subject in Ethiopia. The initial sample size calculated was 384; after adding a 10% nonresponse rate, the final sample size was adjusted to 422. To select the study respondents, the sampling frame was prepared by having lists of nurses from nursing service director for JMC, matron for Shenen Gibe Hospital, and human resource management for health centers. Finally, study respondents were selected by using a simple random sampling technique using lottery methods after proportional allocation to each unit. The sample size was distributed to each public health facility by proportional to size allocation, using the formula:

where ni = sample size of nurses from each public health facility, n = final sample size of nurses, N = total nurses, and Ni = total nurses at each public health facility (Figure 2).
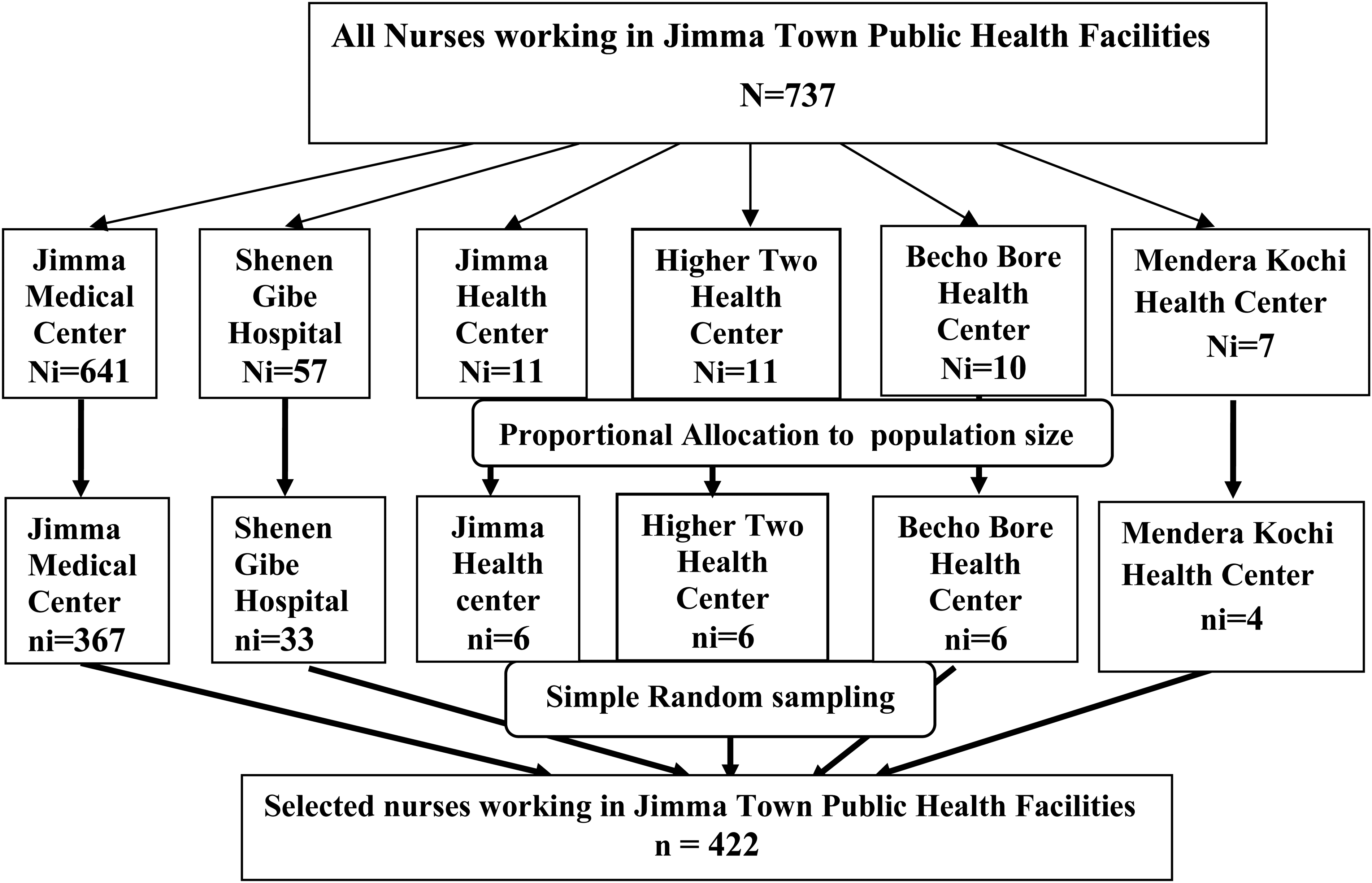
Schematic Representation of Sampling Procedure for Selecting Study Respondents Working at Jimma Town Public Health Facilities, 2021.
Inclusion Criteria
The source population involved all nurses working at these facilities, while the study population consisted of nurses who had at least six months of work experience.
Exclusion Criteria
Nurses who were absent during the data collection period due to annual or maternity leave were not included in the study.
Study Instruments
Data were collected using a structured self-administered questionnaire (Bowling & Ebrahim, 2005). Study tool was adapted from a valid and reliable tool called Leadership Practice Inventory (LPI) tool (Kouzes & Posner, 2003) with 25 items which were 5-point Likert scale: 1 denotes almost never, 2 denotes once, 3 denotes sometimes, 4 denotes often, and 5 denotes frequently. The perception toward managers’ leadership practice was assessed by using LPI, organizational commitment tool (Allen & Meyer, 1990) with 18 items which was 5-point Likert scale: 1 denotes very dissatisfied, 2 denotes dissatisfied, 3 denotes neutral, 4 denotes satisfied, and 5 denotes very satisfied, job-related stress tool (Dagget et al., 2016) with 24 items which was 4-point Likert scale; 1 denotes never stressful, 2 denotes sometimes stressful, 3 denotes frequently stressful, and 4 denotes always stressful; and innovative work behavior tool (Jong, 2007; Kleysen & Street, 2001) with 11 items which was 5-point Likert scale; 1 indicates never, 2 indicates almost never, 3 indicates sometimes, 4 indicates fairly often, and 5 indicates very often.
Data Collection Procedures
Data collection was conducted by three trained Bachelor of Science midwives under the supervision of a health officer. The data collectors clearly communicated the study's objectives to each respondent. Each respondent was informed about the study's objectives and made aware of their right to withdraw from the study at any time without any repercussions. Informed consent was obtained, and respondents were provided with a copy of their signed consent forms. Data collectors were responsible for data collection and submitting data to supervisor daily by complying research ethics. They did not participate in study design, proposal writing, funding, analysis, and manuscript write-up other than data collection to avoid research bias.
The supervisor provided guidance throughout the data collection process, and continuous monitoring was implemented to ensure data integrity. Data collection occurred at mutually agreed-upon times, taking into account the respondents’ existing nursing care responsibilities. Both the supervisor and the researcher facilitated the process, ensuring the completeness and accuracy of the collected data through daily checks. Confidentiality and data privacy were prioritized at all stages of the study, safeguarding respondents’ information throughout the research process.
Data Quality Management
Data collectors were selected from health facilities located outside Jimma Town and did not take part in the study itself. They, along with their supervisors, received a one-day training session from the principal investigator covering the study's objectives, content, and data collection methods before the actual data collection commenced. A pretest of the questionnaire was administered to 21 nurses at Agaro Hospital and Health Center one week before the main data collection to assess its clarity, flow, completeness, and internal consistency. The reliability of the LPI tool was evaluated using Cronbach's alpha, resulting in a score of 0.87. Modifications were made to improve clarity and flow. Supervisors verified the completeness and appropriateness of the collected data. Both the principal investigator and supervisors closely monitored the data collection process.
Ethical Consideration
At the initial stage of data collection, informed written consent was taken from respondents and the respondents were assured that their participation was recoded anonymously. Respondents were informed the purpose, merit, and demerits of the study and their participation were voluntary and the choice to participate or not will have no any kind of effect on them. All the data obtained in due course was kept confidentially by a paper copy of the collected data which were kept in a locked and secured location and the electronic data was kept in password-protected computer.
Data Analysis
The gathered data were examined for completeness and consistency, coded by the principal investigator, and entered into Epi-Data Manager version 4.6 prior to being exported to Statistical Package for Social Sciences version 25.0. The assumption of normality for multiple linear regressions was evaluated, showing a maximum Variance Inflation Factor of 1.50. The adequacy of the model was assessed using the Kolmogorov–Smirnov test, which yielded a p-value of .074, indicating a good fit. Both descriptive and analytical analyses were performed, calculating means, frequencies, and percentages in the descriptive analysis. Simple linear regression analysis was conducted to identify potential variables for multiple linear regression, selecting those with a p-value <.25. Variables with p-values <.05 were considered significantly associated with nurses’ perceptions of their managers’ leadership practices. The strength of these associations was expressed through unstandardized β values along with a 95% confidence interval and p-values (Tizón-Couto & Lorenz, 2021).
Results
Sociodemographic Characteristics
Out of the 422 nurses initially targeted for inclusion in this study, 403 completed the survey, resulting in a response rate of 95.5%. Among the respondents, over half (57.1%) were female. In terms of marital status, 248 nurses (61.5%) reported being married. Nearly two-thirds (63.8%) identified as Oromo in ethnicity. The four most common working units for the nurses were surgical (17.4%), medical (15.9%), pediatric (13.9%), and emergency units (13.4%). A significant majority (89.1%) had not received any leadership training. The average age of respondents was 29.20 years (±5.49), ranging from 20 to 48 years old. On average, respondents had 5.36 years (±3.57) of service experience, with a minimum of 10 months and a maximum of 18 years. Monthly salaries ranged from a minimum of 3,000 ETB to a maximum of 10,095 ETB, with an average salary of 6,345.52 ETB (±1,400.55) (Table 1).
A Sociodemographic Characteristic of Nurses’ (n = 403).

*Adventist, Joba-witness. # Sidama, Dawro, Wolayta.
**Ophtha, ART, Dermatology.
Nurses’ Perception of Their Managers’ Leadership Practice
The overall mean score of nurses’ perception of their managers’ leadership practice in this study was (76.30 ± 16.00) with a minimum score of 37 and a maximum score of 113. The level of nurses’ perception toward their managers’ leadership practice was done by using data in tertiale classification by rank order lower tertiale represents the low level, middle tertiale represents to moderate level, and upper tertiale indicate a high level of perception toward nurse managers’ leadership practice. According to tertiale classification, 125 (31.0%), 164 (40.7%), and 114 (28.3%) of nurses have low, moderate, and high levels of perception toward their managers’ leadership practice, respectively (Figure 3).

Level of Perception Toward Managers’ Leadership Practice Among Nurses.
Factors Associated with Nurses’ Perception of Their Managers’ Leadership Practice
Both bivariate and multivariable linear regression analyses were conducted to determine the factors influencing nurses’ perceptions of their managers’ leadership practices. The bivariate analysis indicated that several variables: such as education level, marital status, type of healthcare facility, leadership training, monthly salary, overall organizational commitment, total job-related stress, and innovative leadership behavior were potential candidates for multivariable linear regression with a p-value < .25. These candidate variables were then included in a multivariable linear regression model using the enter method for variable selection. Variables with p-values < .05 were deemed significantly associated with nurses’ perceptions of their managers’ leadership practices (Tizón-Couto & Lorenz, 2021). The findings revealed that leadership training; organizational commitment, innovative work behavior, and job-related stress were significantly linked to nurses’ perceptions. Specifically, an increase in organizational commitment among nurses was associated with a 0.52 increase in their perception of managers’ leadership practices (95% CI = 0.36, 0.68; p < .001). Additionally, an increase in innovative work behavior correlated with a 1.1 rise in perception (95% CI = 0.92, 1.25; p < .001). Conversely, a negative relationship was found between the lack of leadership training and job-related stress, which negatively impacted nurses’ perceptions of their managers’ leadership practices. Specifically, an increase in job-related stress by one unit led to a decrease in perception by 0.13 (95% CI = −0.22, −0.04; p = .005). Furthermore, nurses without leadership training had perceptions of their managers’ leadership practices that were 5.5 times lower compared to those who had received such training (95% CI = −8.55, −2.40; p = .001) (Table 2).
Multivariable Linear Regression Analysis Final Model for Perception Toward Managers’ Leadership Practice among Nurses (n = 403).

*Significant value at p < .05.
**Highly significant value at p < .001 and (1): reference group.
Discussion
This study aimed to evaluate nurses’ perceptions of their managers’ leadership practices and the factors influencing these perceptions across various healthcare facilities. The findings revealed that 125 nurses (31%) had a low perception, 164 (40.7%) had a moderate perception, and 114 (28.3%) had a high perception of their managers’ leadership practice. This suggests that nurses’ engagement in health care services is low, resulting in poor quality of patient care and safety (Alsadaan et al., 2023). Additionally, this may contribute to higher nurses’ turnover due to dissatisfaction with their leaders’ practices. These results are lower than those from a study at Rwanda Military Hospital, where 34.2% of nurses reported a high perception, 43.8% a moderate perception, and 22% a low perception of transformational leadership by their managers. This discrepancy may be attributed to the leadership training available to nurses in the military setting, which likely enhances their perceptions (Nyirazigama, 2017).
More than one-third of the nurses in this study exhibited a moderate perception of their managers’ leadership practices, consistent with findings from studies in New York (Khan et al., 2018). However, this contrasts with higher perceptions reported in studies from Malta (Sammut & Scicluna, 2020). These variations could stem from differences in training, workload, job satisfaction, healthcare environments, and resource availability within the health system.
Concerning sociodemographic characteristics of study respondents, the finding showed that there was no association with age, gender, working unit, work experience, educational level, and income. In contrast, various studies conducted on perception toward managers’ leadership practice among nurses were found that there was association with age, year of experience as a nurse, educational level, and working unit (Ahmed et al., 2019; Fardellone et al., 2014; Olu-Abiodun & Abiodun, 2017). This difference may be related to sociocultural differences, workload, job satisfaction, healthcare setup, and availability of resources across the health system (Alrobai, n.d.). Additionally, the study identified significant factors associated with nurses’ perceptions of managerial leadership practices. Specifically, leadership training, organizational commitment, innovative work behavior, and job-related stress were all found to significantly influence these perceptions.
Notably, there was a significant negative correlation between the lack of leadership training and nurses’ perceptions of their managers’ leadership practices (β = −5.471; 95% CI = −8.548, −2.395; p = .001). Nurses who had not received leadership training were 5.5 times less likely to have a positive perception of their managers compared to those who had received such training. This finding aligns with research from Colorado (Wallis & Kennedy, 2013), which indicated that leadership training for nurses enhances performance and job satisfaction, leading to improved perceptions of managerial leadership. In-service leadership training likely provides nurses with a better understanding of leadership, thereby increasing their positive perceptions of their managers’ practices (Lunden et al., 2021).
This study also found a positive association between nurses’ organizational commitment and their perceptions of their managers’ leadership practices (β = 0.523; 95% CI = 0.361, 0.684; p < .001). Nurses with higher levels of organizational commitment tend to have a more favorable view of their managers’ leadership compared to their peers. This finding is consistent with other research conducted in the United States (Brewer et al., 2016), New York (Moneke & Umeh, 2013), and Pakistan (Iqbal et al., 2020). Committed nurses often exceed expectations in their roles, fostering better relationships with their managers through open communication, which enhances leadership skills and improves perceptions of managerial practices (Uslu Sahan & Terzioglu, 2022).
Additionally, the study indicated that nurses’ innovative work behavior was statistically linked to their perceptions of managerial leadership (β = 1.084; 95% CI = 0.918, 1.250; p < .001). Engaging in innovative behaviors boosts nurses’ perceptions of their managers’ leadership through intrinsic motivation and knowledge sharing. This aligns with findings from studies in Pakistan (Masood & Afsar, 2017) and Taiwan (Weng et al., 2015). Nurses involved in innovative processes freely share creative ideas, which can enhance performance, effectiveness, and efficiency, ultimately leading to increased motivation and satisfaction, thereby improving their perceptions of managerial leadership (Sorour et al., 2024).
Furthermore, the study revealed a negative correlation between job-related stress and nurses’ perceptions of their managers’ leadership practices (β = −0.131; 95% CI = −0.222, −0.039; p = .005). Stressors such as heavy workloads, conflicts, lack of support, and uncertainty about patient care negatively impact nurses’ perceptions of their managers’ leadership. This finding is supported by research from Indonesia Hospital (Rindu et al., 2020) and Finland (Pekurinen et al., 2019), suggesting that job-related stress leads to dissatisfaction and demotivation among nurses, resulting in lower perceptions of their managers’ leadership practices (Labrague et al., 2020).
Strengths and Limitations of the Study
This study provides insights into nurses’ views on leadership practices, serving as a valuable resource for future researchers for the first time. Due to the lack of literature on this topic in this country, the comparison of study results was done with other countries where the health institution setup, health policy, and other factors may differ.
This study is not without limitations; since it has typical limitations of a cross-sectional study; researchers focused solely on correlation rather than establishing cause and effect. Moreover, this study analysis was limited to the quantitative aspects of nurses, and researchers did not explore the qualitative perspectives of both nurses and leaders, which could have provided more comprehensive insights for the study.
Implications for Nursing Practice and Research
This study plays its roles to improve nursing services including patient care, evidence generation, and education by identifying areas for improvement regarding nursing leadership practice. This study’s finding helps to prepare strategies for in-service training regarding nursing leadership practice. For administrative, it contribute to give attention to reduce job-related stress among staff nurses. For nurses, it helps to encourage organizational commitment and innovative work behavior of staff. The findings serve as baseline data for future research and encouraged to expand this investigation to include nurses at a national level, and longitudinal studies are recommended to explore causal relationships.
Conclusion
Less than one-third of nurses hold a high perception of their managers’ leadership practices. Factors influencing these perceptions include a lack of leadership training, organizational commitment, innovative work behavior, and job-related stress. Both organizational commitment and innovative work behavior were positively associated with nurses’ views on their managers’ leadership. Conversely, lack of leadership training and job-related stress was negatively influence these perceptions.
Footnotes
Acknowledgments
The authors would like to thank Jimma University for sponsoring this study. The authors deepest thank also extended to instructors at the school of Nursing of Jimma University who supported us either directly or indirectly by giving a constructive comments and guidance. Last but not least, the authors would not wrap up without thanking our data collectors for their support and encouragement throughout this work and nurses who participated in this study for their willingness to share their experiences.
Ethics Approval and Consent to Participants
Ethical clearance was obtained from the Research and Ethics Committee of Jimma University's Ethical Institutional Review Board with Ref. No: with Ref. No. IHFPG/368/21. Written informed consent was taken from study participants. The respondents were got an introduction concerning the aim of the study and were asked their consent by guaranteeing their confidentiality and anonymity. The participants have full right to reject or accept to answer the questions. The name of the respondents was not recorded on the questionnaire and was assure the study may not have any risk. All collected data from the respondents were only served for research purposes. Data were stored in a lockable and secured cabinet to maintain their confidentiality. All methods were performed in accordance with the relevant guidelines and regulations.
Authors’ Contribution
Mihret Gashaye Yeneget made substantial contributions to the conception and design. Bayisa Bereka Negussie, Admasu Belay Gizaw, Desalew Tilahun Beyene, and Mihret Gashaye Yeneget acquired, analyzed, and interpreted the data and performed data acquisition, analysis, and interpretation of data. Mihret Gashaye Yeneget took part in drafting the article or revising it critically for important intellectual content; agreed to submit it to the current journal. All authors gave their final approval for the version to be published; and agreed to be accountable for all aspects of the work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Jimma University.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The datasets used in this study are available from the corresponding author upon request.