
Abstract
Introduction
Prenatal education courses for pregnant women appear to be an effective strategy to facilitate maternal adaptation, especially during labor. Consequently, maintaining high adherence rates to these courses is crucial for improving health outcomes in pregnant women and enhancing their experience during the transition through this stage. However, in Latin America, low adherence to in-person prenatal education courses has consistently been reported. On the other hand, adherence to online courses and the factors associated with permanence have been poorly studied in this context.
Objective
This study aimed to identify factors that predict pregnant women's adherence to an online prenatal education course.
Methods
This retrospective cohort study included pregnant women who voluntarily enrolled in an open-access online prenatal education course between 2020 and 2025. The main outcome was adherence to the course. Sociodemographic variables and pregnancy-related characteristics were considered potential predictors. Population characteristics were summarized using descriptive statistics. A logistic regression model was constructed to identify independent predictors of adherence.
Results
A total of 1,624 pregnant women were included, 43.59% completed the course. Enrolling in the course between 2023 and 2025 (OR = 1.95, 95% CI = 1.57 to 2.41), having a planned pregnancy (OR = 1.81, 95% CI = 1.34 to 2.47), having an educational level higher than primary school (OR = 1.58, 95% CI = 1.21 to 2.06) and attending more prenatal visits (OR = 1.05, 95% CI = 1.00 to 1.09) were independent predictors of course completion.
Conclusion
Fewer than half of the enrolled pregnant women completed the online prenatal education course. Strategies need to be implemented to improve adherence, especially among pregnant women who report unplanned pregnancies, lower educational levels, and fewer prenatal visits.
Introduction
Maternal health care has been a constant worldwide concern, as reflected in the Health and Well-being goals for the sustainable development of nations established by the United Nations Development Programme (United Nations, 2015). Consistently, indicators such as maternal mortality are key determinants of a country's development, as they reflect the quality and accessibility of health services (World Health Organization, 2025).
Prenatal education is a care strategy to improve the level of knowledge and support pregnant women and their families in the main changes and care required during pregnancy, childbirth, and newborn care. This education is usually provided through in-person or virtual courses structured and led by healthcare professionals. Several studies have shown that this strategy that can be highly beneficial for maternal and neonatal health, improving fear and anxiety about childbirth, self-efficacy, rates of vaginal births, adherence to recommended prenatal practices, and reduce the use of epidural anesthesia (Alizadeh-Dibazari et al., 2023; Athinaidou et al., 2024; Escobar et al., 2022; Hong et al., 2021; Mengesha et al., 2021; Tajvar et al., 2022; Zaman et al., 2025).
In this sense, adherence to prenatal education courses refers to the participation and regular attendance of the pregnant woman until the course content is fully completed (Seyoum et al., 2021). Maintaining high adherence rates to these courses is crucial for improving the previously described health outcomes and enhancing the experience of pregnant women during the transition through this stage.
In the context of Latin American countries, low attendance rates in prenatal education courses, mainly those delivered in-person, have been documented, ranging from 10.00% to 30.77% (Barrera-Sanchez & Osorio-Aristizabal, 2019; Gomez-Medina, 2016). Some aspects related to low adherence to these courses are associated with economic and geographical factors, such as living in rural or hard-to-reach areas (Harizopoulou et al., 2024).
Additionally, time limitations particularly among multiparous women who are simultaneously engaged in early childhood caregiving, the lack of a support companion, and shortcomings in the delivery of prenatal education courses (because although these courses are offered on a continuous basis, they are not adequately promoted, are generally offered in-person, and their content do not consider specific educations needs of pregnant women), have also been considered as aspects related to a low adherence (Barrera-Sanchez & Osorio-Aristizabal, 2019; Gomez-Medina, 2016; Harizopoulou et al., 2024; Mora et al., 2014).
A valid and economical alternative for countries in this region is virtual or online prenatal education, as features such as flexibility and accessibility make it possible to overcome economic, work-related, time availability, and geographical barriers that usually occur in these contexts and limit access to prenatal education, perpetuating inequality in health care for this population (Harizopoulou et al., 2024). In addition, parents from newer generations are generally comfortable with technology and the accessibility of online information, a trend that was reinforced by the need to communicate through these technologies to maintain physical distancing during the COVID-19 pandemic. Although online education courses may also present some barriers for prenatal education (e.g., less social interaction or the need for internet connection), the advantages appear to be superior and could be facilitators to ensure quality prenatal education that can impact pregnancy outcomes for this population (Harizopoulou et al., 2024; Shen et al., 2024).
Considering the described advantages of virtual prenatal education and the low attendance rates reported for in-person educational strategies in Latin American contexts, it is essential to first determine whether virtual courses could improve pregnant women's adherence to prenatal education and, secondly, which factors are associated with this adherence. Understanding these elements will enable nursing professionals to implement more effective educational strategies to improve health outcomes for pregnant women and their newborns.
Review of Literature
The factors associated with adherence to maternal healthcare services (e.g., prenatal visits) have been widely studied (Addisu et al., 2022; Idris & Sari, 2023; Zhou et al., 2020). In contrast, there is limited evidence on factors that specifically predict adherence to prenatal education courses.
A study conducted among 504 pregnant women attending a hospital in China, identified that women with higher educational level, and those in their second or third trimester of pregnancy, were more likely to participate in online prenatal education. In contrast, women with more than one child had a lower probability of participation (Shen et al., 2024).
In another study also conducted in China aiming to understand the use of online antenatal education classes accessed via “the Mother and Child Health Handbook app” during the COVID-19 pandemic, a higher participation rate in online education was identified in 2020 (period with physical distancing) compared to 2019 (period before physical distancing). The researchers considered that this finding could be related to a greater awareness of health self-management among pregnant women and a greater demand for online education due to the limitations of in-person education during the pandemic period (Chen et al., 2022).
To our knowledge, there are no studies carried out in Latin America to identify the factors associated with adherence to prenatal education. Given this scenario, it is important for nursing professionals to identify the factors that determine pregnant women's adherence to online prenatal education courses, to implement effective interventions that ensure accessibility for a larger proportion of this population and improve their knowledge, attitudes, and practices before, during, and after pregnancy. Therefore, the aim of this study was to identify the factors that predict adherence of pregnant women to an online prenatal education course.
Methods
Study Design and Setting
A retrospective cohort study was carried out among pregnant women who registered between November 2020 and February 2025 in an online prenatal education course developed by a healthcare provider institution that provides fourth-level quaternary care (highly specialized treatments and procedures) and also offers primary care services in a Latin America Country. This study is nested within a larger project titled “Meanings, knowledge, and experiences of pregnant women participating in the online prenatal education course for safe motherhood and fatherhood.” The main objective of the large project, which has not yet been published was to describe the meaning for pregnant women of preparation for motherhood and maternal and perinatal services that are part of the comprehensive maternal and perinatal care pathway.
Research Question
What factors predict pregnant women's adherence to an online prenatal education course?
Participants
This study was conducted within the context of the course called “Online prenatal education course for safe motherhood and fatherhood.” This is an online course designed and offered by a healthcare institution located in Bucaramanga (Department of Santander, Colombia). The course is part of the educational strategies of the institution's promotion and prevention area for prenatal preparation of pregnant women and their families.
As part of routine care, all pregnant women receiving services at the institution are encouraged by nursing staff to enroll and take the course during their pregnancy. Since 2020, this course has been offered to the public on a permanent basis. It offers open access to all pregnant women and their families (whether or not they receive healthcare services at the institution offering the course) through the institutional platform. Once a username is created to register for the course, participants are required to complete a form collecting sociodemographic data and information related to the characteristics of pregnancy.
Course Contents
The course consists of six learning units structured as follows: Unit 1: Introduction to general concepts of motherhood and fatherhood, Unit 2: First trimester (Content: physiological and psychological changes during pregnancy 0–14.7 weeks; nutrition and diet in the first trimester; emotional bonding, and oral hygiene), Unit 3: Second trimester (Content: physiological and psychological changes during pregnancy 15–28.7 weeks, nutrition and diet in the second trimester, and emotional bonding), Unit 4: Third trimester (Content: physiological and psychological changes during pregnancy 29–42 weeks, nutrition and diet in the third trimester, and signs of postpartum depression), Unit 5: Labor and postpartum (Content: labor and delivery, breastfeeding, postpartum care and newborn care), Unit 6: Parenting guidelines and family planning. Each unit includes audiovisual content and is designed to be completed in approximately 40 h.
Once the enrolled individuals complete all the contents of each unit, they receive a certificate issued by the promotion and prevention area, which records the date and time of course completion.
Inclusion Criteria
All pregnant women who voluntarily registered for the online prenatal education course between November 2020 and February 2025 were considered eligible for this study.
Exclusion Criteria
Participants who registered outside the study period of interest were excluded. Also, duplicate entries were removed by the institutional office, retaining only the most recent registration per participant. Subsequently, the verified registrations were provided to the researchers without any identifying information of the participants.
Sample
The sample size for this study was 1,254 pregnant women. This was calculated using G-Power software, considering the following parameters: power level of 0.95, probability of alpha error of 0.05, and probability of an event under the null hypothesis of 0.1 (assuming that, according to studies reported in the literature in the Latin American context, the lowest percentage of pregnant women who complete prenatal education courses is approximately 10%) and an effect size (Odds ratio OR) of 1.4 for the multiple logistic regression analysis. Anticipating the possibility of information bias due to missing data related with self-reported information from participants, it was estimated that 1,500 pregnant women registered in the course would be included.
Procedures
To identify eligible pregnant participants, the promotion and prevention office provided the research team with a database containing anonymized records of all individuals enrolled in the course. As previously mentioned, this registration is routinely self-completed by all participants who voluntarily sign up for it. The registration form includes the registration date, type of participant (e.g., pregnant woman, or relatives), sociodemographic characterization variables and pregnancy-related variables.
The sample for this study was selected consecutively, starting with the oldest records (from 2020) through the most recent (2025), verifying the fulfillment of the eligibility criteria for each record in the database. Additionally, the institution office provided the research team with information regarding course completion status for each enrolled individual, including the date of course completion and certification for those who completed the training. The research team was responsible for reviewing each anonymized record in the database to ensure data consistency and to identify missing information across variables.
Ethical Considerations
The institution's scientific technical committee and the institutional ethics committee approved the conduct of this study (IRB number: 07931/2023). Additionally, its development followed the principles of the Declaration of Helsinki, as well as current national regulations.
Informed consent was not requested from the participants due to the retrospective nature of the study. This decision was based on two arguments: 1) the difficulty of contacting all participants registered during the 5-year observation period, and 2) the exclusive use of pre-existing information protected by the Institution's Internal Data Processing Regulations, which include authorization for research purposes. Additionally, at the time of registration for the course, each participant provides authorization to take part in the course and to allow the use of the information entered in the sociodemographic and pregnancy characterization form. The self-reporting of this data is considered part of the routine course process.
The promotion and prevention office anonymized all identifying data of pregnant women and provided researchers only with the variables of interest for the study.
Variables of Interest
The primary outcome of this study was adherence to the online prenatal education course, defined as the full completion of all course modules and receipt of certification. Therefore, adherence was considered as a dichotomous variable: adherent or non-adherent to the course. Possible predictors of adherence included sociodemographic characteristics of the pregnant women, such as follows:
age, municipality of residence (coded as: Bucaramanga, Metropolitan area and other municipalities), health insurance provider (coded as: main contributory, secondary contributory, other contributory, and subsidized regime providers), educational level (coded as: primary, high school, technical or technological, university, and postgraduate), and the type of household composition (coded as: partner, parents, only with children, and other relatives).
Pregnancy-related characteristics were also considered, including pregnancy planning, gestational age, number of pregnancies, number of prenatal visits at the time of course registration, and year of registration for the course.
Statistical Analysis
Sociodemographic characteristics of the pregnant women and pregnancy-related variables were summarized as absolute and relative frequencies for discrete variables, while continuous variables were presented as medians and interquartile range (IQR), given that the data showed a nonparametric distribution (Kolmogorov–Smirnov test). To explore the relationship between sociodemographic and pregnancy-related characteristics, these variables were described according to the outcome status: adherent or non-adherent to the course. The null hypothesis of no difference in variable distributions between these two groups was tested using the chi-square test or Fisher's exact test (for variables with fewer than 10 observations) and the Student's t-test or Mann–Whitney U test, according to the nature of the discrete or continuous variables and their distribution, respectively.
For interpretative clarity, the educational level variable was regrouped in three categories: primary education, secondary education, or higher education. In addition, the year of registration was dichotomized into two groups: registration between 2020–2022 and between 2023–2025, to account for potential variations associated with the COVID-19 pandemic. The effect size for each variable was estimated using unadjusted OR with their corresponding 95% confidence interval (95% CI). The description of the primary outcome included the absolute and relative frequency of pregnant women who adhered to the prenatal education course, as well as the median duration of course completion and its IQRs.
To determine the independent predictors of adherence to the prenatal education course, variables with a p-value <0.20 in the bivariate analysis were selected as candidate variables for inclusion in the multivariate logistic regression model (Zhang, 2016). The model was developed using a backward stepwise selection method, starting with a full model that included all main effects. At each step, the variable with the lowest contribution to the model was removed, and the fit of the resulting reduced model was reassessed. This process continued until the final model was obtained. For each variable in the final model, adjusted ORs with 95% CI were reported. Model goodness of fit was assessed using the likelihood ratio test, the Hosmer–Lemeshow test and the Bayesian information criterion index. A statistical significance level of 5% (two-tailed) was considered in all analyses. Statistical analyses were conducted using Stata version 12.0.
Results
Sample Characteristics
In total 2,615 individuals registered for the online prenatal education course between 2020 and 2025. Of these, 1,624 were eligible for inclusion in this study as they corresponded to pregnant women (See Figure 1).

Selection Process of Study Participants.
The median age of the pregnant women included in the study was 28 years (IQR = 24 to 32 years). The largest proportion of participants (55.17%) resided in municipalities within the metropolitan area of Bucaramanga, while 16.44% lived in other municipalities both within and outside the department of Santander. Less than one-quarter of the pregnant women had an educational level equal to or lower than high school (0.62% primary school and 16.69% high school), and majority lived with their partner (78.14%). A total of 37.62% of the pregnant women received prenatal care services from the main health insurance provider of the contributory regime affiliated with the institution offering the online prenatal education course (See Table 1).
Sociodemographic Characteristics of the Participants.

Data available for 1,602 pregnant women. bFisher's exact test.
IQR=interquartile range.
A total of 85.28% reported that their pregnancy was planned. The median gestational age was 23 weeks (IQR = 14 to 30 weeks), and the median number of prenatal visits received at the time of course registration was four checkups (IQR = 2 to 5). The majority of pregnant women (60.16%) enrolled in the online course during the post-COVID-19 pandemic period (See Table 2).
Pregnancy Characteristics of the Participants.

Data available for 1,612 participants. bData available for 1,619 participants. cData available for 1,618 participants. dStudent's t-test.
IQR=interquartile range.
Research Question Results
Of the total number of pregnant women registered for the course, 43.59% (n = 708) were adherent and successfully completed it. The median time to complete the course, from registration on the platform to obtaining the completion certificate, was 28 days (IQR = 6 to 80 days). The median age was significantly higher in the group of adherent participants compared to the non-adherent group (29 years versus 28 years, respectively; p < 0.001). Statistically significant differences were also observed in the distribution of municipality of residence, educational level, and healthcare provider. 20.62% of adherent participants reported residing in municipalities outside Bucaramanga and its metropolitan area, compared to 13.21% in the non-adherent group (p < 0.001).
Among the adherent participants, 37.71% reported having a university-level education, compared to 32.21% in the non-adherent group who reported the same level of education (p = 0.001). In addition, a higher proportion of adherent pregnant women received prenatal care from the main health insurance provider of the contributory regime affiliated with the institution offering the online course, compared to the proportion of non-adherent participants (41.53% versus 34.61%; p = 0.003) (See Table 1).
Regarding pregnancy-related characteristics, 89.83% of the adherent participants reported that their pregnancy was planned, compared to 81.77% in the non-adherent group (p < 0.001). Adherent participants also had a higher median gestational age compared to non-adherent participants (24 weeks versus 22 weeks, respectively; p = 0.012). Additionally, those who completed the course had attended more prenatal visits at the time of registration (median = 4 checkups) compared to those who did not complete the course (median = 3 checkups; p < 0.001). The proportion of pregnant women who registered for the course between 2023 and 2025 and were adherent was significantly higher than the proportion of non-adherent participants who registered during the same period (60.49% versus 52.95%, respectively; p < 0.001).
Table 3 shows the results of the multivariate analysis. Of the total variables evaluated, 7 were selected as candidates for the multiple regression model based on data from 1,591 pregnant women with complete information. Ultimately, four variables were identified as independent predictors of adherence to the course. Registering for the course between 2023 and 2025 (OR = 1.95, 95%CI = 1.57 to 2.41), having a planned pregnancy (OR = 1.81, 95%CI = 1.34 to 2.47), having an education level higher than primary education (OR = 1.58, 95%CI = 1.21 to 2.06), and attending more prenatal visits (OR = 1.05, 95% CI = 1.00 to 1.09) independently increased the likelihood of pregnant women completing the prenatal education course.
Predictors of Adherence to Online Prenatal Preparation Courses.
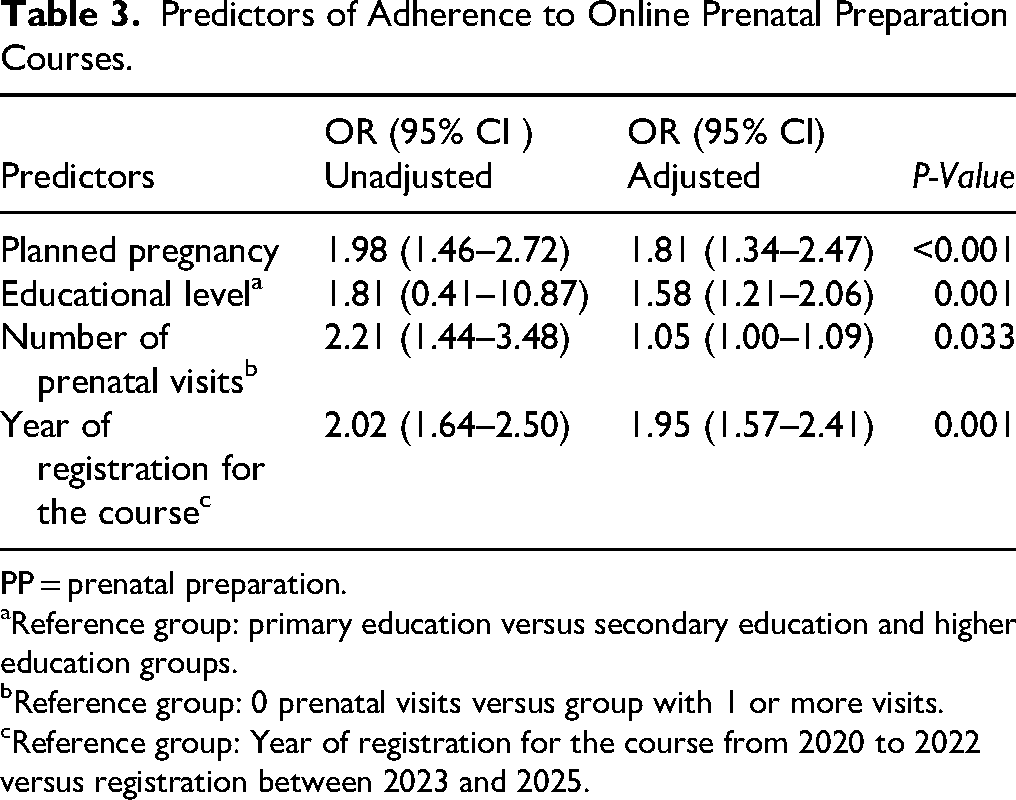
PP = prenatal preparation.
Reference group: primary education versus secondary education and higher education groups.
Reference group: 0 prenatal visits versus group with 1 or more visits.
Reference group: Year of registration for the course from 2020 to 2022 versus registration between 2023 and 2025.
Discussion
In this study, approximately two out of every five pregnant women enrolled in the online prenatal education course were adherent and completed all course content. Furthermore, pregnant women who registered in the course in the years following the COVID-19 pandemic, reported having a planned pregnancy, had an education level higher than primary school, and attended a greater number of prenatal visits were more likely to complete the online course.
Compared to other studies conducted in the Latin American context, which report adherence rates between 10% and 31% to prenatal education courses (Mora et al., 2014; Rubio-Rodriguez & Cardona-Montes, 2020), the present study reported an adherence rate greater than 40%. This increase in adherence may be favored by the online format of the course offered in this study, which represents an advantage for pregnant women with limited time, those who are employed, or those living in remote areas where in-person courses are less accessible.
Additionally, within the healthcare institution offering the online course, pregnant women who complete the course and obtain certification are routinely offered the incentive of allowing their partner to accompany them during labor or cesarean delivery, which could explain the higher adherence observed in this population. Although the healthcare provider entity was not identified as an independent predictor of adherence in the multivariate analysis, offering incentives such as partner accompaniment or personal and newborn items could serve as motivational strategies to encourage course completion among pregnant women.
The highest proportion of pregnant women in this study registered for the preparation education course in the period between 2023 and 2025, furthermore, registration during this period independently increase the likelihood of adherence to the course. The COVID-19 pandemic facilitated greater acceptance of online education among the general population (Chen et al., 2022; Davrieux et al., 2021; Harizopoulou et al., 2024; Kansal et al., 2021); the need to maintain confinement to prevent contagion while still acquiring knowledge, improvements in internet access and electronic devices, and increased familiarity with virtual platforms were factors that favored the process of adaptation and acceptance of this educational format during the pandemic and subsequent years. This familiarity with online education would explain why registration in the post-pandemic period was identified as the main predictor of adherence to the online prenatal education course.
On the other hand, age was not found to be an independent predictor of adherence to the prenatal education course in the present study. In contrast, having a higher educational level significantly increased the likelihood of pregnant women completing the course. In this sense, the effects of age could be mediated by the educational level of the pregnant women.
Consistently, the cross-sectional study conducted by Shen et al. (2024) among pregnant women attending services at a tertiary hospital in China identified educational level as a factor positively associated with participation in online prenatal education courses. Additionally, studies conducted in various settings have also identified the influence of this factor on the general utilization of maternal health services (Herwansyah et al., 2022; Midhet et al., 2023). A higher level of education usually provides better abilities for understanding information and self-directed learning, as well as greater skills for navigating online platforms. Those factors support continued participation in education offered through this modality and may explain the association between educational level and adherence to the online prenatal education course.
Moreover, in the study by Shen et al., a higher gestational age was identified as a positive factor associated with participation in online prenatal education courses, whereas having more than one child was negatively associated with this outcome (Shen et al., 2024). Although in the present study, pregnant women who adhered to the course had a significantly higher median gestational age compared to non-adherent women, this variable was not identified as an independent predictor of adherence in the multivariate analysis.
Similarly, this study did not directly measure the number of children the pregnant woman was caring for; however, data was collected on the number of pregnancies at the time of registration (which may be interpreted as a related variable). The distribution of this variable did not differ significantly between the adherent and non-adherent groups in the online course. The discrepancies observed between studies regarding these findings may be related to contextual differences between populations, as well as to methodological aspects influencing the conduct of each investigation.
Planned pregnancy is a factor that has been associated with greater utilization of maternal healthcare services (Addisu et al., 2022; Idris & Sari, 2023; Zhou et al., 2020). This supports the relationship between planned pregnancy and course adherence identified in the present study, a result that may be attributed to the higher level of commitment and involvement in health care commonly demonstrated by pregnant women who have intentionally planned their pregnancies, and who are more willing to engage in prenatal education.
Finally, in this study, more prenatal visits at the time of course registration were identified as a predictor of adherence to the online prenatal education course. Although this predictor has not been reported in previous studies and had the smallest effect size in the present analysis (with borderline confidence intervals), greater exposure to prenatal care services may have increased the likelihood that pregnant women were encouraged to participate in the online prenatal education course, as well as reinforced their perceived need to acquire more knowledge about the pregnancy, childbirth, and postpartum processes.
Strengths and Limitations
This study has several strengths and limitations. Among its strengths, it stands out as the first reported study in the Latin American literature to date that identifies predictors of adherence to online prenatal education courses within a country in this context. The study used data from an open-access course in which the majority of participants were pregnant women from the Santander region but also included participants who accessed from other regions of Colombia. The sample size allowed for the identification of a sufficient number of outcomes (course adherence) to develop robust regression models and identify independent predictors.
Since the information used in this study was not collected for research purposes and informed consent was not requested but rather as part of the routine care provided by the institution's promotion and prevention area to identify individuals registering for the online course, we recognize as a limitation of this study the potential for information bias related to the self-reporting of variables by pregnant participants.
Furthermore, the use of self-reported data limited the access to potential predictors of adherence to the online course, such as the pregnant women's time availability and occupation, as well as qualitative aspects like their perceptions and experiences during the course. Finally, since the pregnant women analyzed in this study primarily reside in the Santander region, the findings may not be generalizable to other contexts.
Implications for Practice
The findings of this study highlight that, although there has been greater acceptance of online health education courses among pregnant women in the post-COVID-19 pandemic period, additional activities are needed to improve adherence to these courses. These efforts should be especially focus on pregnant women who report unplanned pregnancies, have lower educational levels, and have attended few prenatal visits.
In this regard, this study provides essential information to guide future research aimed at evaluating the effectiveness of various strategies to improve adherence, for example offering incentives such as allowing a partner to be present during childbirth or providing resources for maternal and newborn self-care.
Additionally, in light of these findings, it is important to consider expanding the availability of prenatal education courses using a multimodal approach (virtual, institutional in-person, or home-based in-person), offered as open-access courses across different healthcare institutions in the country. This would help address the diverse needs and preferences of pregnant women, especially in Latin American contexts.
Conclusion
This study identified that approximately 43% of pregnant women adhered to the online prenatal education course. The factors that increased the likelihood of adherence to the course included enrollment in the years following the COVID-19 pandemic, reporting a planned pregnancy, having a higher educational level, and attending more prenatal visits. Consequently, it is essential to provide greater follow-up and implement strategies to improve adherence to prenatal education, especially among women who do not share these characteristics. Further research is needed to assess the impact of strategies aimed at enhancing adherence to prenatal education.
Footnotes
Acknowledgment
We would like to express our thanks to Nicolle Mariana Mendez Dallos who participated in the manuscript translation.
ORCID iDs
Author Contributions Statements
SMV, DMRB, MLJV, DMAM, and JKST participated in the study design. DMAM, JKST, and MLJV participated in data collection. SMV and DMRB participated in data analysis and drafting of the manuscript, and all authors participated in critical review of the contents.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declare no potential conflicts of interest related to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets analyzed during the current study are available from the corresponding author on reasonable request.