
Abstract
Introduction
The health status and survival of newborns depend on the quality of care provided by mothers. If mothers do not provide essential care due to a lack of knowledge or inappropriate traditional beliefs, it may adversely affect infant growth and development.
Objectives
This study evaluated the effectiveness of an infant health promotion education program on mothers’ knowledge regarding infant sleep, safety, dental care, hygiene, personal care, and vaccination.
Methods
The study used a quantitative, cross-sectional, pre-experimental, one-group, pre- and post-test design. The accessible population comprised 171 first-time pregnant women in their third trimester, attending maternity clinics of a university hospital in Amman, Jordan. A convenience sampling technique was adopted. Pre-test knowledge was assessed during the first visit of the third trimester. The nurse-led infant health promotion education program was implemented once per week. On completion after four weeks, the post-test was conducted. The participants completed a demographic data sheet and a knowledge questionnaire.
Results
After the intervention, participants’ knowledge about healthy infant sleeping, infant protection, dental care, vaccinations, and hygiene and personal care improved significantly (P < .001). Participants who scored highly in the health promotion program showed greater readiness to care for their infants at home.
Conclusions
Promoting infants’ health not only improves the health of the newborn; it also improves the quality of life of the infant, the new parents, and eventually the family. Thus, infant health promotion interventions should be included as part of routine hospital care, which would improve outcomes across the lifespan.
Introduction
The first few hours after birth are crucial for the survival of newborns (Abdu et al., 2019). A lack of knowledge and poor newborn care practices may contribute to higher mortality rates (Nampijja et al., 2024; Nasir et al., 2017). The neonatal period is the most vulnerable in a child's life. Globally, 2.4 million newborns died in 2020, with 47% of all deaths of children aged under 5 years occurring in the newborn period (World Health Organization, 2022). Many developed countries have shown noteworthy progress in neonatal and infant care, including Arabian Gulf countries, namely Oman, Saudi Arabia, the United Arab Emirates, Bahrain, and Kuwait (Salam & Al-Khraif, 2020). However, because child mortality is closely related to fertility and overall mortality levels, mortality rates are still affected by complicated pregnancies and deliveries, birth under improper conditions, and communicable and non-communicable diseases during pregnancy (Akseer et al., 2018). Therefore, newborn and infant care is crucial in promoting their health.
The health status and survival of newborns depend on the quality of care provided by parents (Nguyet et al., 2021). If parents do not provide essential care to their newborns due to knowledge deficits, or if they provide inappropriate or harmful care due to traditional beliefs, it may adversely affect growth and development (Sujatha, 2014). Evidence shows that first-time mothers have inadequate knowledge and skills to effectively care for their infants, have limited parent–infant interactions and lack the knowledge to provide holistic infant care (Chung et al., 2018). Knowledge gaps have been reported in essential newborn care, including eye care, cord care, and vaccination (Amolo et al., 2017). Furthermore, most postpartum mothers have inadequate knowledge regarding umbilical cord care, dangerous signs in newborns, neonatal jaundice, and vaccination (Nguyet et al., 2021). Mothers also lacked knowledge on breastfeeding, and breastfeeding rates in Vietnam decreased by 24% in 2014 and 17% in 2018 (Nguyet et al., 2021). A lack of knowledge can ultimately limit positive health behaviors and the transition to stable parenthood (Chung et al., 2018). Because a lack of newborn care knowledge adversely affects the health and development of infants, providing health promotion programs could fill the knowledge gap.
Literature Review
Becoming a first-time mother is a major transition in a woman's life. During this phase, the mother takes responsibility for caring for herself and the newborn. Mothers must prepare themselves physically and psychologically to care for their newborns. Therefore, motherhood preparation for first-time mothers is essential to enhance their knowledge, emotional status, and practice in newborn and infant care (Ahmed Thabet et al., 2024). Previous studies have shown the impact of infant health promotion educational programs on various maternal outcomes (Chung et al., 2018; Fu et al., 2014; Kolahi et al., 2021; Lee & Oh, 2016; Shrestha et al., 2016). These programs have improved confidence in the maternal role (Lee & Oh, 2016; Shrestha et al., 2016), enhanced the initiation and duration of exclusive breastfeeding (Fu et al., 2014), boosted infant and maternal health, increased maternal knowledge of newborn care, and reduced anxiety (Shrestha et al., 2016). Additionally, newborn care utilization during the first 2 months was improved after attending a newborn care–oriented education program (Kolahi et al., 2021). These educational programs also enhanced the quality of mother–infant interaction (Chung et al., 2018).
According to the World Health Organization, in 2022, around 2.3 million newborns worldwide died in the first 28 days of life. Of these neonatal deaths, 75% occurred during the first week of life, and the leading cause was premature birth (World Health Organization, 2022). Most neonatal deaths are preventable. Globally, the neonatal mortality rate was approximately 17/1,000 live births in 2022 (World Health Organization, 2022). In Jordan, the neonatal mortality rate in 2022 was reported at 8.2/1,000 live births (Statista, 2024). The neonatal mortality in Jordan has not decreased since 2012. Neonatal mortality rates have been reported as higher among homemakers compared to employed women. The odds of neonatal death in Ministry of Health hospitals were 21 times higher than in private hospitals. Most neonatal deaths are attributed to low birth weight, pre-term birth, and respiratory and cardiovascular disorders (Al-Sheyab et al., 2020). Maternal complications, including pregnancy-related complications, complications of the placenta and cord, and medical and surgical conditions, are also causes of neonatal death (Al-Sheyab et al., 2020).
The rates of exclusive breastfeeding in children below 6 months of age and continued breastfeeding until 2 years of age were low. Additionally, complementary feeding diet standards were suboptimal. The burdens of low birth weight, anemia, and vitamin A and D deficiency were exacerbated, and fruit and vegetable consumption were inadequate (Al-Awwad et al., 2021). This evidence shows the necessity of education programs related to the care of newborns and infants for first-time mothers because they need appropriate knowledge and skills.
Given the evidence that a lack of knowledge and skills related to infant health is strongly linked to adverse maternal, neonatal, and infant outcomes, this study aimed to determine the effectiveness of a nurse-led infant health promotion program on knowledge among first-time pregnant women in Jordan. Conducting this research among first-time pregnant women has various benefits, including the possible enhancement of their knowledge of essential newborn care and improvement of their self-confidence in caring for their newborns. Additionally, the research findings will guide healthcare providers and policymakers to design a culturally tailored antenatal education program to meet the educational needs of mothers. This will be reflected in the improvement of maternal education and postnatal care services, eventually improving maternal and infant wellbeing (Ahmed Thabet et al., 2024). Moreover, in the study context, the neonatal mortality rate has remained high since 2012. Therefore, the study evaluated the effect of the infant health promotion program on maternal knowledge regarding infant health related to sleeping, safety, dental care, hygiene and personal care, and vaccination.
Being aware and knowledgeable about promoting infant health will empower first-time mothers to improve their health and develop self-efficacy, enabling them to develop a high level of wellness that will be reflected in raising the health status of their infants. Furthermore, providing first-time mothers with opportunities for skill-building, peer support, and positive reinforcement will strengthen maternal confidence in caring for their infants. Additionally, conducting an education program for first-time mothers will help in promoting infant health, developing targeted interventions that address maternal needs, enhancing maternal self-efficacy, and ultimately optimizing infant health outcomes.
Methods
Research Approach
The study used a quantitative research approach.
Research Design
A cross-sectional, pre-experimental, one-group, pre- and post-test study design was adopted. The study did not have a control group. The pre- and post-tests were conducted for the same group before and after the intervention. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines were used for reporting.
Research Question
Is a nurse-led infant health promotion education program effective in improving knowledge among first-time pregnant women?
Population
The target population comprised first-time pregnant women in their third trimester. The accessible population consisted of first-time pregnant women in their third trimester who attended the maternity clinics of a university hospital in Amman, Jordan.
Sample and Sample Size
Using power analysis parameters for the paired one-tailed dependent-groups t-test (one-tailed paired t-test), an estimated medium effect size of 0.2, an alpha level of 0.05, and a power of 0.8, the sample size for answering the research question was 156. The researcher approached 250 women who met the inclusion criteria to participate. The pre-test response rate was 68.4% (n = 171). Approximately 94.7% (n = 162) of those who agreed to participate in the study attended the educational sessions, and 157 (96.9%) completed the post-test questionnaire.
Sampling Technique
A convenience sampling technique was adopted.
Setting
Women were selected during their regular follow-up antenatal visits, in the waiting room of the maternity clinics at the Jordan University Hospital, an accredited teaching hospital. This is a tertiary hospital with a capacity of 599 beds in Amman, Jordan.
Inclusion and Exclusion Criteria
The study included Jordanian first-time pregnant women who attended the maternity clinic in their third trimester of first pregnancy (gravida 1, para 0), who had no history of miscarriage and were free from medical and surgical history, free from obstetrical and gynecological health history, willing to participate in the study, and prepared to give birth in the university hospital, and who agreed to participate in the follow-up antenatal visits. The study excluded women whose permanent residency was outside Jordan; who were multipara; who had a history of medical, surgical, obstetrical, or gynecological health problems, miscarriage, or stillbirth; who did not have frequent follow-up antenatal clinic visits; or who were in the first or second trimester of pregnancy.
Ethical Considerations
Ethical approval was obtained from the Research and Ethics Committee of University of Jordan (PF.17.8). After gaining ethical approval, the researcher identified eligible participants and explained the purpose of the study. Participants were given the right to withdraw from the study at any time. Written informed consent was obtained from the participants before data collection. The anonymity of the participants was ensured during and after the study. The data were secured and saved on the researchers’ computer. The questionnaire was coded by numbers to maintain the confidentiality of the data, and only the researchers had access to the data. The questionnaire and other hard-copy documents related to the study were secured in a locked cabinet and will be kept for 5 years.
Description and Interpretation of Study Instruments
Part 1: Participant Demographic Data
This questionnaire collected the demographic data of the participants. It included age, income, gestational age, level of education, marital status, cigarette smoking status, shisha smoking status, and husband's smoking status.
Part 2: Knowledge Questionnaire
Knowledge was assessed using this questionnaire, developed by the researcher by reviewing the literature related to infant health promotion. It consists of 10 questions about infants’ sleep, four questions about safety, eight questions about dental care, eight questions on hygiene and personal care, and five questions about vaccination, totaling 35 questions. The questionnaire uses a 5-point Likert scale (strongly agree: 5 points, agree: 4 points, neutral: 3 points, disagree: 2 points, and strongly disagree: 1 point). The minimum is less than 11, and the maximum is more than 22.
Reliability and Validity of Study Instruments
To assess face validity, the questionnaire was translated into Arabic and reviewed by two faculty experts who are involved in research and teaching child health nursing courses. The Arabic version was back translated into English by the researcher and translator. After back translation, the draft was compared with the original tool, and modifications were implemented accordingly. The Cronbach's alpha for various health promotion components was assessed. (Table 1).
Reliability of knowledge questionnaire.
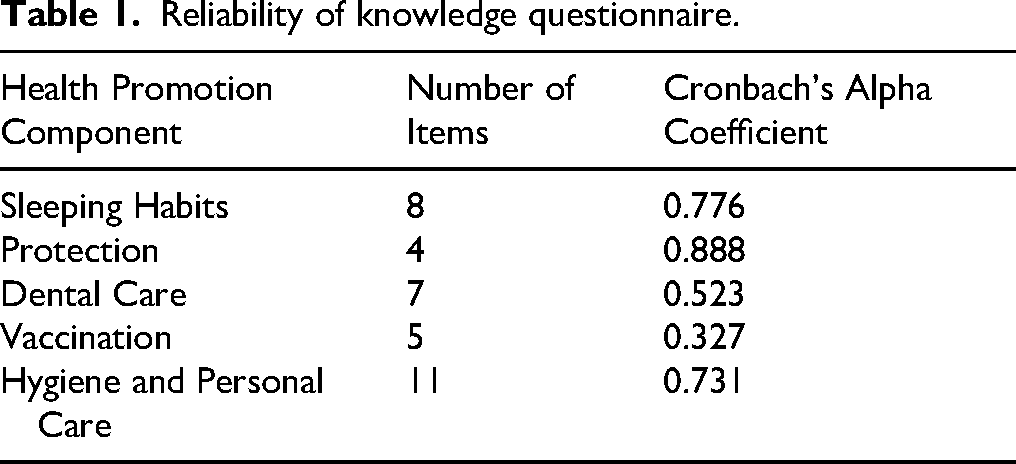
The internal consistency coefficient for the health promotion items ranged from 0.89 for the protection and safety items to 0.52 for the dental care items, indicating acceptable internal consistency reliability and content validity. The alpha coefficient for the vaccination item alone was 0.33.
Pilot Study
Before collecting the data, a pilot study was conducted among 15 first-time pregnant women to examine the feasibility of the study instrument and recruitment process and ensure that the data collection method was workable and acceptable for participants. No changes were made to the questionnaire on completion of the pilot study. The participants of the pilot study were not included in the main study.
Data Collection Procedure
The data were collected from December 2021 to August 2022 through two phases: Phase I (pre-assessment) and Phase II (intervention and post-assessment).
Phase I: Pre-Assessment
The pre-assessment was conducted in a private room at the antenatal clinic, where the participants were interviewed. Their knowledge was assessed using the pre-test questionnaire, which consisted of 14 questions related to demographic and health data and 35 questions related to knowledge of infant health. The pre-test interviews lasted 45–50 min. The data were collected by four trained research assistants and were directly collected and saved via a tablet. On completion of the pre-test data collection, the researcher critically analyzed the participants’ knowledge and categorized it into various levels.
Phase II: Intervention (Infant Health Promotion Education Program) and Post-Assessment
The infant health promotion education program was designed based on the studies of Jang and Ju (2020) and Abd Allah et al. (2023). The instructors included obstetricians, obstetric nurses, and midwives. The investigators were also trained to provide infant health promotion education programs. The researchers prepared the materials and handouts to share with the participants. The intervention was validated by experts in the field. The intervention was conducted by the researchers once a week in a private room at the antenatal clinics, using a variety of interactive approaches. These included discussion, illustrations, demonstrations, posters, and printed materials to ensure that the content was delivered accurately. The education was imparted over three weeks for 30–45 min per session. The sessions were conducted one-on-one, and any questions from the participants were answered. These sessions were conducted for four weeks. On completion of the fourth week, the post-test was conducted with the same knowledge questionnaire. The researchers shared their personal contact information with the participants for any follow-up or further questions related to the educational program.
Data Cleaning and Analysis
The data were analyzed using SPSS version 23. Descriptive statistics were used to describe the sample characteristics, and the item analysis used mean and standard deviation scores. Paired-sample t-tests (two-tailed) were used to assess mean differences between pre-intervention and post-intervention assessment scores, with the significance level set at P ≤ .05.
Results
Sample Characteristics
The mean age of the participants (n = 171) was 26.18 (SD = 4.33) years. Their mean monthly income was 543.95 (SD = 331.56) Jordanian dinars, and the mean gestational age was 32.84 (SD = 4.09) weeks. Of all participants, 64% (n = 110) had a university baccalaureate degree or higher, and 98.8% were married. Only 7.6% smoked shisha, whereas 52.6% of their husbands smoked (Table 2).
Demographic Characteristics of Study Participants (n = 171).

Research Question Results
Knowledge of Infant Health Promotion Components
Knowledge of Infants’ Healthy Sleeping
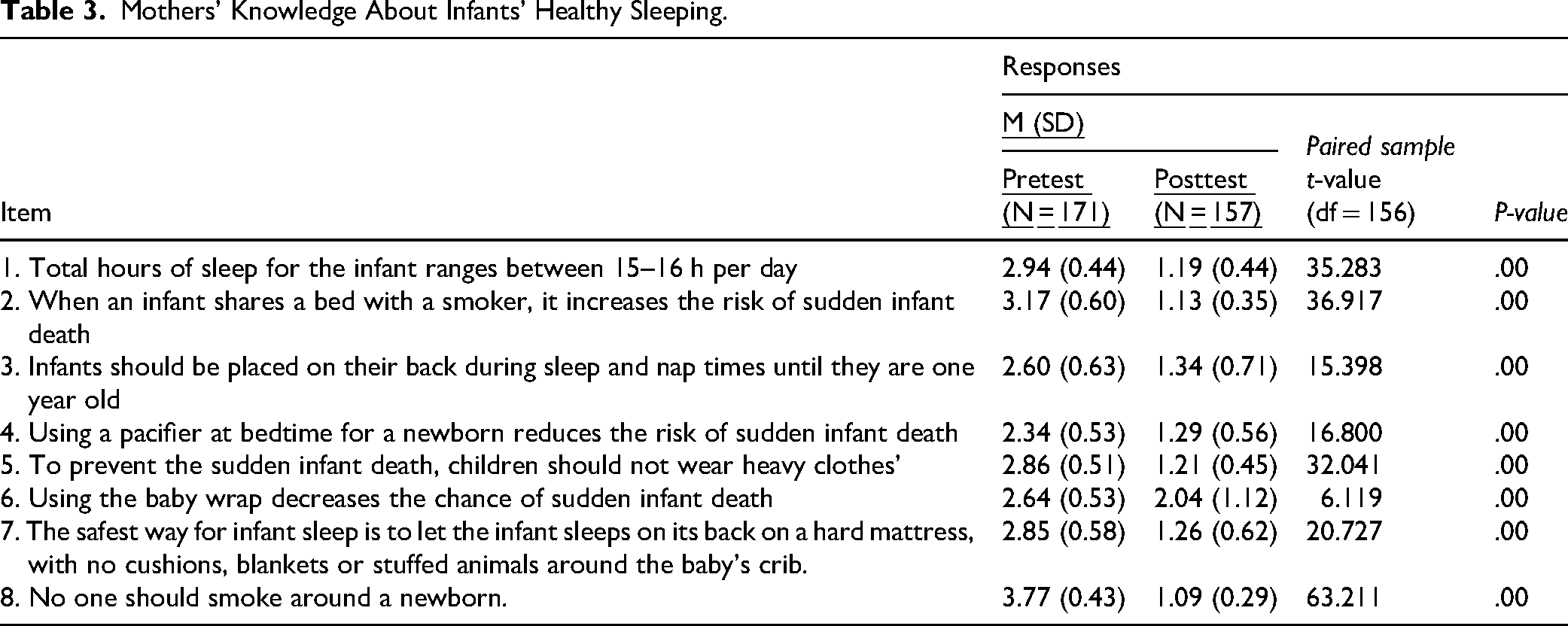
Table 3 shows the pre- and post-intervention item analysis and comparisons regarding participants’ knowledge about infant health promotion components. Item analysis showed that most participants had adequate knowledge regarding smoking hazards and the range of total hours of infant sleep. Overall, their knowledge of infants’ healthy sleep improved significantly after the intervention (mean difference: 12.63; t = 41.764; P < .001).
Mothers’ Knowledge About Infants’ Healthy Sleeping.
Knowledge of Infant Safety
The item analysis of participants’ knowledge of infant safety and protection (Table 4) showed that most demonstrated adequate knowledge regarding all items, including the most essential danger signs and household hazards. Overall, participants’ knowledge of infant protection improved significantly after the intervention (mean difference: 8.96; t = 52.204; P < .001).
Mothers’ Knowledge About Infants’ Safety.

Knowledge of Infant Dental Care
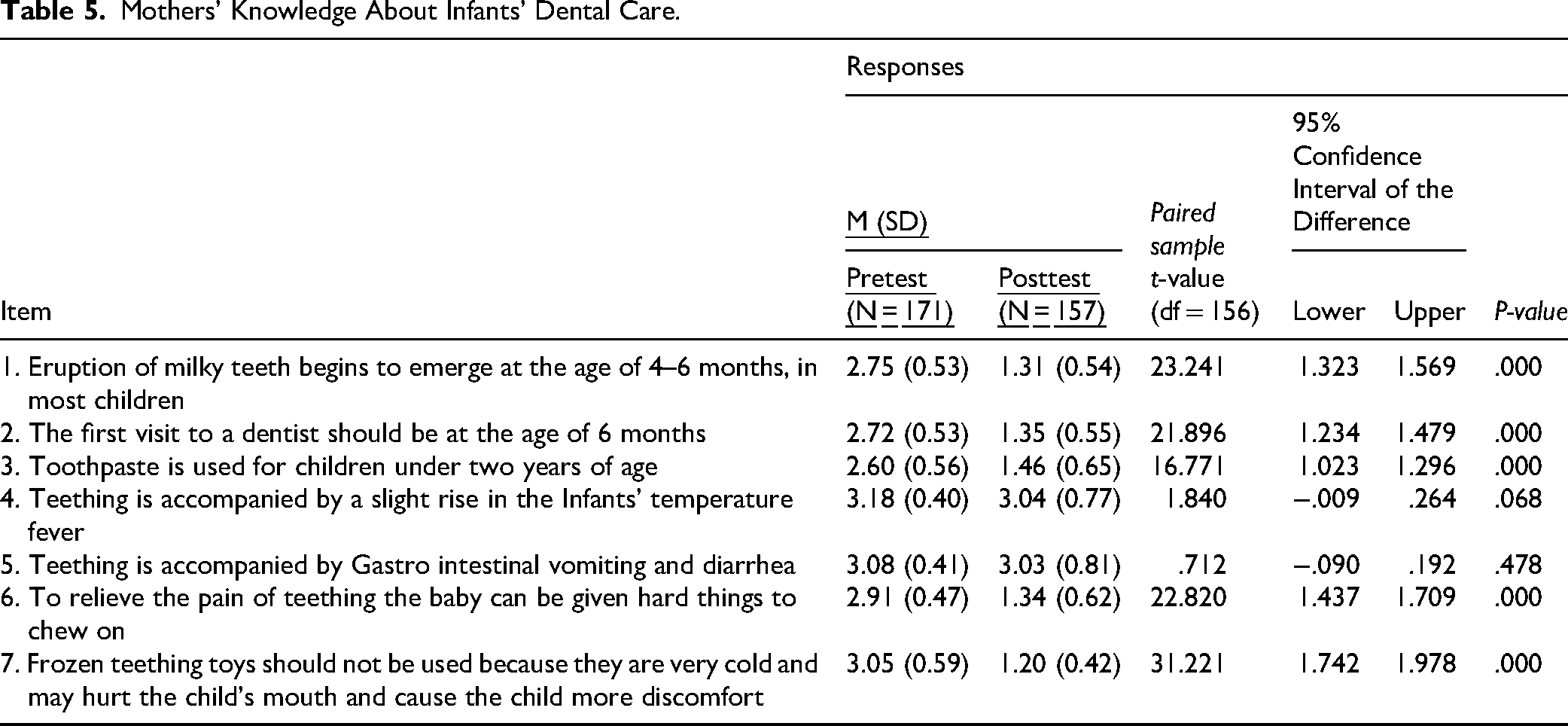
The item analysis of participants’ knowledge of infant dental care (Table 5) showed that most demonstrated adequate knowledge regarding all but two items, regarding the time for the first visit to a dentist during infancy and the use of toothpaste for children aged under 2 years. Knowledge of infant dental care improved significantly after the intervention (mean difference: 7.57; t = 33.625; P < .001), except for two items regarding the signs accompanying teething, fever, and infection.
Mothers’ Knowledge About Infants’ Dental Care.
Knowledge of Infant Vaccinations
Table 6 shows the pre- and post-intervention item analysis and item comparisons regarding participants’ knowledge of infant vaccinations. Most showed little knowledge regarding the effect of multiple vaccines on infants’ immune systems, the need to vaccinate a breastfed child, and the chance of an infant contracting a disease they have been vaccinated against. However, their knowledge improved significantly after the intervention for all items (mean difference: 2.20; t = 13.192; P < .001).
Mothers’ Knowledge About Infants’ Vaccination.

Knowledge of Infant Hygiene and Personal Care
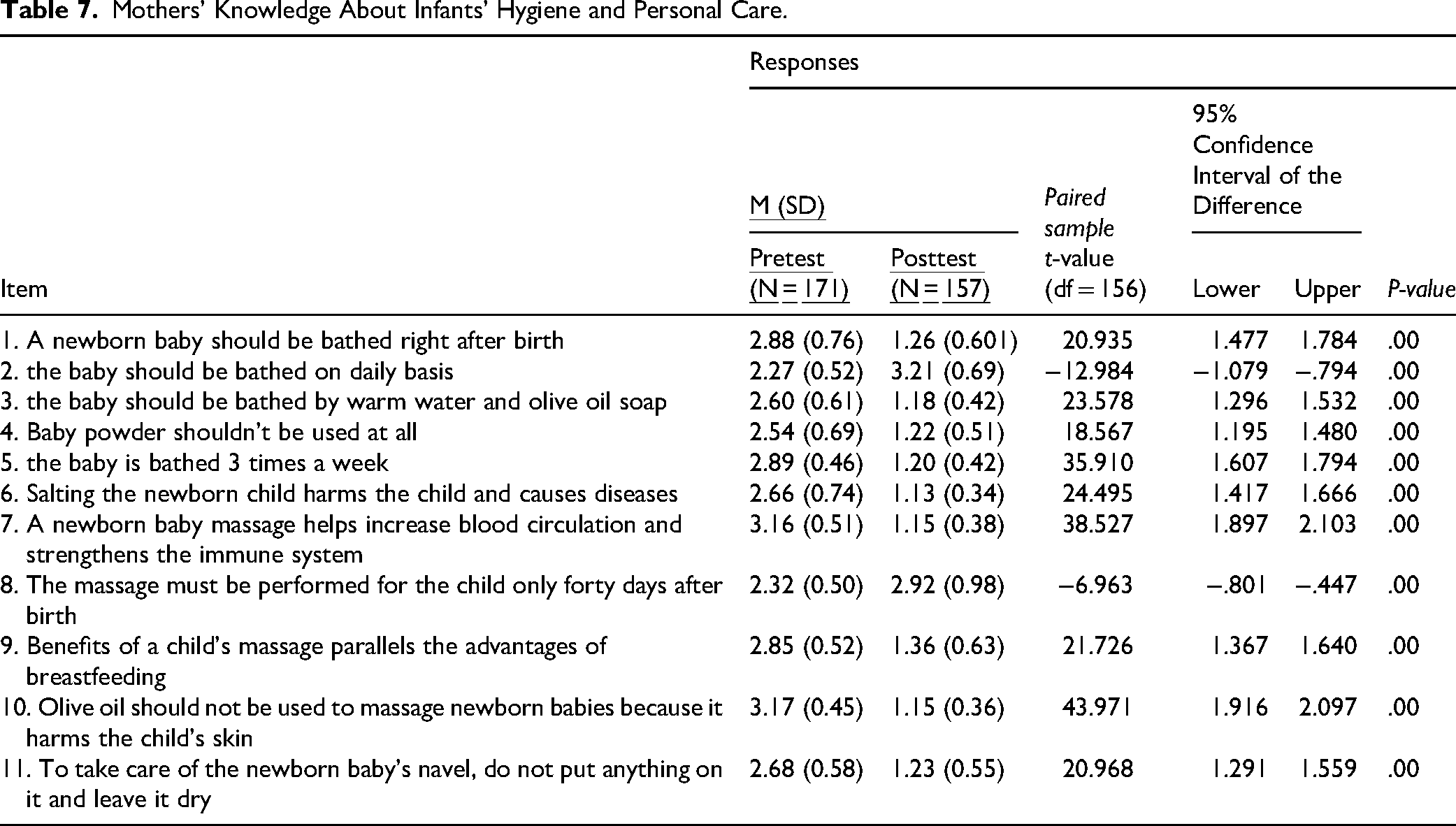
Most participants had limited knowledge regarding most of the hygiene items and had better information regarding the benefits of massage and the use of olive oil. Generally, their knowledge about infant hygiene and personal care improved significantly after the intervention for all items (mean difference: 12.94; t = 38.907; P < .001), as shown in Table 7.
Mothers’ Knowledge About Infants’ Hygiene and Personal Care.
Overall Program Effectiveness
The dependent t-test results showed statistically significant differences between pre- and post-test scores for sleeping habits (t = 41.764, P = 0.001), protection (t = 52.204, P = .001), dental care (t = 33.625, P = .001), vaccination (t = 13.192, P = .001), and hygiene and personal care (t = 38.907, P = .001). The differences in mean scores for sleeping habits (M = 12.63), safety (M = 8.96), dental care (M = 7.57), hygiene and personal care (M = 12.94), and vaccination (M = 2.20) were used to evaluate the effectiveness of the health promotion program. Participants who scored highly on the health promotion program components were perceived to be more ready to care for their infants at home (Table 8).
Effectiveness of Health Promotion Program on the Health Promotion Components.

Discussion
High-quality care during pregnancy improves women's health in general and keeps infants healthy (U.S. Department of Health and Human Services, n.d.). Interventions including increasing breastfeeding rates, promoting vaccinations, safe sleep practices, a healthy and safe home environment, good nutrition, and performing developmental screening tests are key to improving infant health (Centers for Disease Control and Prevention, 2022). Further, UNICEF advocates for infant and young child policies to ensure the provision of continuous, quality, lifesaving maternal, newborn, and childcare services. These services involve adequate nutrition, care for good health, safety and security, opportunities for learning, and responsive caregiving. They enhance the chances of child survival and provide equal chances for quality early stages of infant development and better life outcomes (UNICEF, 2023). Considering the recommendations of the Centers for Disease Control and Prevention and UNICEF, this study determined the effectiveness of a nurse-led infant health promotion education program on knowledge among first-time pregnant women in Jordan.
The participants’ knowledge about infants’ healthy sleeping, protection, dental care, vaccinations, and hygiene and personal care improved significantly after the program. Participants who scored highly in the components of the health promotion program were more ready to care for their infants at home.
Health promotion interventions published by the World Health Organization can be used to promote the health of mothers and newborns. These interventions are designed to improve home care practices and care-seeking across the care continuum (Smith et al., 2017). One core health promotion developmental intervention is maintaining the infant's sleeping position to prevent harm and promote overall health. Therefore, parents should create safe infant sleeping arrangements (Task Force on Sudden Infant Death Syndrome, 2005). Unsafe infant sleeping positions are associated with unexpected sleep-related problems and sudden infant death syndrome (Yetwale et al., 2023). In this study, mothers gained adequate knowledge about infants’ healthy sleeping practices after attending the nurse-led infant health promotion education intervention. Consistently, mothers receiving prenatal educational sessions on safe sleep practices have followed these during the postnatal period (McDonald et al., 2019; Ramos et al., 2023). This highlights the need to enrich the infant sleep–related knowledge of pregnant women and design national follow-up programs. Further, parents should be provided with personalized and understandable information related to sleep routines, sleeping arrangements, and behaviors that are suitable for their sociocultural traditions (Landsem & Cheetham, 2022).
Child safety is an essential component of health promotion programs (Ali et al., 2019). Unintentional injury to children at home is a significant cause of death and disability. Suffocation while sleeping in the crib, drowning in the swimming pool, fire-related injuries, and poisoning are some of the major safety threats to infants. Improved awareness of infant safety prevents unintentional injuries and the related negative consequences (Filemban et al., 2022). In this investigation, participants’ knowledge of infant protection improved significantly after the intervention. Similarly, a systematic review of 16 studies showed that educational interventions were effective in preventing unintentional injuries to infants (Scott et al., 2022). Another scoping review concluded that safety and accident prevention educational interventions, including creating a safe home environment and routine follow-up, were highly effective in preventing accidents in infants (Nguyet et al., 2021). Policymakers should thus organize educational sessions for first-time parents to promote infant safety.
Early childhood caries is a severe form of dental caries affecting children aged under 3 years (Dhull et al., 2018). Proper dental care prevents caries and allows for the early detection of any abnormalities (Salama et al., 2020). Mothers play a vital role in maintaining the oral hygiene and dental care of their infants (Thomas et al., 2015). Within this research, participants’ knowledge about infant dental care improved significantly after the intervention. Mothers’ knowledge of dental care improves with their educational status, occupation, and socioeconomic status (Salama et al., 2020). Another study found significant improvements in the level of knowledge four weeks after receiving an educational intervention compared to before (Lloclla-Sauñe et al., 2024). Culturally appropriate, personalized educational sessions are needed, especially during the prenatal period, to improve oral care and decrease early childhood dental caries (Rossato et al., 2021).
Protecting children from diseases is an essential part of healthcare systems and an effective mechanism to prevent mortality and morbidity in children. Vaccination significantly reduces the rates of diseases and improves the quality of life of children (Almutairi et al., 2021). Greater knowledge of vaccination is associated with a higher educational level of mothers (Almutairi et al., 2021; Giannakou et al., 2021; Nassar et al., 2023). In this study, most participants had limited knowledge regarding the effect of vaccines on infants’ immune systems and the need to vaccinate a breastfed child. However, their knowledge improved significantly after the intervention. Consistently, significant improvements in parental knowledge of vaccination have been observed after receiving educational interventions (Azmi et al., 2018). Further, knowledge of vaccination is associated with mothers’ educational levels (Giannakou et al., 2021). Thus, multiple education sessions are recommended to improve the vaccination knowledge of first-time parents. Further, improving the communication between pediatricians, pediatric nurses, and parents will enhance parental knowledge about vaccination (Giannakou et al., 2021).
Maintaining infant hygiene is challenging for first-time parents because newborn skin is fragile, and parents are generally anxious to hold and bathe their infants (Silva et al., 2023). In general, mothers have inadequate knowledge and practice regarding infant personal hygiene (Missiriya, 2016). Similarly, most mothers have inadequate knowledge regarding face, ear, nose, head, and mouth hygiene, the sequence of cleaning the face and scalp, and infant care (Bulut & Gulay, 2021; Silva et al., 2023). Mothers have been found to practice immediate bathing, apply traditional substances to the cord, delay the initiation of breastfeeding, discard the colostrum, and feed newborns with pre-lacteal feed due to a lack of knowledge of infant care (Asaro et al., 2023; Gul et al., 2014). However, mothers with increased parity, higher educational levels, and regular antenatal visits had increased knowledge of infant care (Leta, 2022; Missiriya, 2016). Corroborating these findings, in this study, participants’ knowledge of infant hygiene improved after attending the education program. Therefore, regular maternal and newborn health programs should be organized by healthcare providers to prevent harmful practices and promote healthy infant care practices (United States Agency for International Development, 2004).
Lastly, statistically significant differences were notable between the pre- and post-test scores on sleeping habits, protection, dental care, hygiene and personal care, and vaccination in this study. This shows that the program was highly effective in improving infant care practices. Thus, policymakers should provide regular health promotion education programs in hospital and community settings to improve the quality of life of infants (Bhusal, 2021).
Strengths and Limitations
This study highlights the importance of empowering first-time mothers with knowledge of infant care practices. The investigators faced a challenge in finding eligible participants. Thus, the data collection period was longer than expected. Digitalization of the data collection process could be beneficial to mitigate this issue. Implementing an online survey distributed across various platforms would allow for faster and more efficient data collection, enabling wider participant reach while reducing logistical challenges. Convenience sampling and the single data collection setting limit the generalizability of the study findings.
Implications for Clinical Practice
Empowering first-time mothers will support them in providing comprehensive care to their infants. This will be reflected in promoting mothers’ and infants’ health and wellbeing (Jang & Ju, 2020). Additionally, healthcare providers will be more aware of the knowledge deficit among first-time mothers. Therefore, the components of routine antenatal care could be reviewed and modified in collaboration with multidisciplinary healthcare team members, considering the current study findings, to meet the needs of new mothers and maximize the benefits of antenatal care education sessions, adopting a person-centered care approach (Nasir et al., 2017).
Artificial intelligence–embedded mobile applications can be developed to educate parents on infant health promotion strategies. The educational content can be personalized in the mobile application based on parents’ individual learning needs. Learning can be monitored in real time, with continuous support provided through interactive platforms or chatbots. This innovation could make health education more accessible, particularly in rural or hard-to-reach areas, thereby improving the quality of infant care (Nguyet et al., 2021).
Recommendations
Healthcare providers should regularly assess the health needs, knowledge, attitudes, and practices of women during pregnancy, and health education sessions or programs should be conducted accordingly. Since pregnancy is not the woman's responsibility alone, the involvement and participation of husbands and families should be encouraged. Additionally, studies should assess the knowledge, attitudes, and practices of expectant fathers. The use of infant health promotion knowledge could be evaluated in future studies. This study should be replicated in different settings with larger samples.
Conclusions
Pregnancy, childbirth, and the postpartum period represent a stressful transition for first-time parents. Assessing the needs of pregnant women and accordingly implementing health education programs during pregnancy are important to promote their infant care knowledge, skills, and attitudes. In this study, the nurse-led infant health promotion education program enhanced the knowledge of first-time pregnant women of various aspects of infant health. To make first-time mothers confident in caring for their infants, nurse-led educational interventions are a viable option to enhance their knowledge and practice. Empowering mothers by assessing their knowledge and practices regarding infant needs and care practices, and providing them with adequate knowledge and practices, will help them increase their self-confidence and efficacy in providing holistic care for their infants. Healthcare providers must be aware that educating pregnant women during the last trimester is an inexpensive, sustainable, and feasible strategy that could reduce neonatal mortality and morbidity rates.
Supplemental Material
sj-docx-1-son-10.1177_23779608251378558 - Supplemental material for Effectiveness of a Nurse-Led Infant Health Promotion Education Program on Knowledge Among First-Time Pregnant Women in a Middle Eastern Country
Supplemental material, sj-docx-1-son-10.1177_23779608251378558 for Effectiveness of a Nurse-Led Infant Health Promotion Education Program on Knowledge Among First-Time Pregnant Women in a Middle Eastern Country by Suhaila Halasa, Judie Arulappan, Nadin M Abdel Razeq, Mahmoud Ai-Hussami, Dua’ Al-Maharma, Ommayah Nassar, Manar Nabolsi, Shawqi Saleh and Ibrahim Al Faouri in SAGE Open Nursing
Supplemental Material
sj-docx-2-son-10.1177_23779608251378558 - Supplemental material for Effectiveness of a Nurse-Led Infant Health Promotion Education Program on Knowledge Among First-Time Pregnant Women in a Middle Eastern Country
Supplemental material, sj-docx-2-son-10.1177_23779608251378558 for Effectiveness of a Nurse-Led Infant Health Promotion Education Program on Knowledge Among First-Time Pregnant Women in a Middle Eastern Country by Suhaila Halasa, Judie Arulappan, Nadin M Abdel Razeq, Mahmoud Ai-Hussami, Dua’ Al-Maharma, Ommayah Nassar, Manar Nabolsi, Shawqi Saleh and Ibrahim Al Faouri in SAGE Open Nursing
Footnotes
Acknowledgements
The researchers extend their sincere thanks to the expectant mothers for their participation in this study.
ORCID iDs
Ethics Approval and Consent to Participate
Ethical approval was obtained from the Research Committee, University of Jordan (PF.17.8). Written informed consent was obtained from the participants before data collection.
Consent for Publication
All the authors have consented for publication of this manuscript.
Authors’ Contributions
SH: Ideas; formulation or evolution of overarching research goals and aims; Development or design of methodology; writing the initial draft. JA: Writing the initial draft; critical review of the manuscript. NAR: Conducting a research and investigation process; critical review of the manuscript. MAH: Conducting a research and investigation process; critical review of the manuscript. DAM: Conducting a research and investigation process; critical review of the manuscript. ON: Conducting a research and investigation process; critical review of the manuscript. MN: Conducting a research and investigation process; critical review of the manuscript. SS: Conducting a research and investigation process; critical review of the manuscript. IAF: Conducting a research and investigation process; critical review of the manuscript.
Funding
The study was funded by The Deanship of Scientific Research at The University of Jordan.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of Data and Materials
The data will be made available upon reasonable request.
Supplemental Material
All supplemental material mentioned in the text is available in the online version of the journal.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.