
Abstract
Introduction
Frontline nurses, particularly those working in highly infectious environments, experienced unprecedented challenges during the COVID-19 pandemic and faced significant physical, emotional, and psychological demands with uncertainty and risk. Understanding their experiences, coping practices, and the broader impacts on their career trajectories from a Roy adaptation model perspective is critical to informing future workforce support and resilience strategies.
Objective
To identify stressors experienced by the interviewed nurses, working in highly infectious environments during the initial peak of the COVID-19 outbreak, explore their coping practices, and investigate the impacts of pandemic stress on their career paths.
Design
A qualitative analysis of an interview study. Sixteen nurses participated in online interviews using semistructured and open-ended questions. Conversations were recorded and transcribed. Analysis of transcripts from sixteen nurses was conducted using Graneheim & Lundman's content analysis method.
Results
The study drew three themes distilled from the coded narratives of the transcripts: (1) lived experiences of stress including eight stressors: fear of infection, emotional frustration, lack of personal protective equipment, information overload, workplace uncertainty, increased workload, organizational disarray, and professional stigma; (2) adaptive coping practices employed by the nurses in response to the stressors including doing exercises, meditating, watching movies, listening to music, sleeping longer hours, engaging in gardening, studying, reading, and connecting with friends through social media; and (3) impacts of pandemic-induced stress on career goals and pursuits. The interviewed nurses exhibited positive attitudes toward managing stress and expressed determination to continue pursuing their nursing career paths.
Conclusion
The study revealed that stressors experienced by interviewed nurses working in highly infectious environments did not merely have negative impacts on their career paths. Successful coping strategies were observed to involve an intricate interplay between innate and acquired coping dimensions, manifested by adaptive stress coping practices.
Introduction
Review of Literature
Amid the global COVID-19 pandemic, frontline nurses played a vital role in combating the coronavirus, working in highly infectious environments and risking their own safety to attend to patients’ needs (Shin & Yoo, 2022). Recognized as heroic figures in one of the most significant healthcare crises in recent history (Phillips et al., 2023), nurses faced both professional and psychological challenges (Khademi & Imani, 2022). Unparalleled stress and exhaustion resulted in high nursing workforce turnover (Martin et al., 2023). A study by Grinspun et al. (2022) indicated a high turnover of the Canadian nursing workforce during the COVID-19 pandemic. Their study found that 69% of Canadian nurses were intending to leave their position in the next few years, and among them, 42% were considering quitting the nursing profession (Grinspun et al., 2022). A similar situation occurred to hospital nurses in New Jersey, USA. According to de Cordova et al.'s study (2022), 64% of 3030 surveyed nurses reported their experiences of burnout and 36% of them expressed their desire to leave hospital within the next year. Their study showed a significant correlation between elevated levels of burnout and the intention to depart from hospital (de Cordova et al., 2022).
Purpose of Study
The overwhelming stress, burnout, and resulting high turnover nursing workforce during the COVID-19 pandemic dominated the mainstream discourse. However, the successful coping strategies of individual frontline nurses working in highly infectious environments were rarely discussed and analyzed, leaving gaps in understanding how some nurses’ navigated stress differently. Notably, there was a lack of research examining pandemic-specific stress coping among frontline nurses from a Roy adaptation model perspective. Within this framework, Roy’s (2009) concept of adaptation emphasizes “conscious awareness and choice to create human and environmental integration” (p.26). This study applies the model to explore how nurses coped with stress in a highly infectious environment and examines pandemic-induced stressors that shaped nursing experiences and influenced nurses’ attitudes toward their career paths. It aimed to address this gap by providing insights into not only the challenges frontline nurses faced but also their personal coping strategies, offering a broader perspective on crisis management (Shin & Yoo, 2022) and reinforcing the importance of strong institutional support for frontline nurses’ physical and emotional well-being (Huerta-González et al., 2021), particularly during public health crises.
Roy Adaptation Model
This study's findings were analyzed through the lens of the Roy adaptation model, a core guiding framework for nursing practice. Roy’s (2009) model explains the human adaptive system, which consists of four interrelated modes: physiological, self-concept, role function, and interdependence. These modes operate across three adaptation levels of behavior: integrated, compensatory, and compromised (Roy, 2009). The discussion of Roy's three adaptation levels and innate and acquired coping concepts provided a structured framework for understanding how interviewed frontline nurses navigated overwhelming stress through personal coping strategies. These analyses also established a conceptual and empirical foundation for the recommendations.
Methods
Design
This study used qualitative content analysis of interview data as the second phase of a two-phase project. The first phase, conducted from April to May 2020, was a cross-sectional quantitative survey involving a convenience sample of 267 respondents recruited through a university's nursing program (Zhang et al., 2021). This phase examined frontline nurses’ experiences during the initial peak of the COVID-19 outbreak in the United States. The second phase involved an in-depth content analysis of interview data, focusing on exploring interviewed nurses’ coping practices and assessing the impacts of the pandemic on their career paths.
Participants
Eighteen nurses from the initial respondent pool of the first phase, voluntarily participated in the interviews for the second phase of the project. The inclusion criteria required participants to be frontline nurses, and nonfrontline nurses were excluded. Upon review, two participants were identified as nonfrontline nurses caring for patients. The transcripts from 16 nurses were eventually included in this study. Of the 16 nurses, 14 (88%) were female and 2 (12%) were male. Regarding ethnicity and race, there were 12 White nurses (75%), 1 Black nurse, 2 Hispanic nurses, and 1 Indian Asian nurse. Among the participants, 9 nurses (56%) were married. In terms of nursing roles, there were 14 registered nurses (88%), 1 nurse preceptor, and 1 nurse assistant. Eight participants were part-time nursing students during the initial peak of the pandemic and at the time of the interviews. Among them, seven were pursuing graduate degrees and one was pursuing an undergraduate degree (Table 1).
Demographics of Participants.
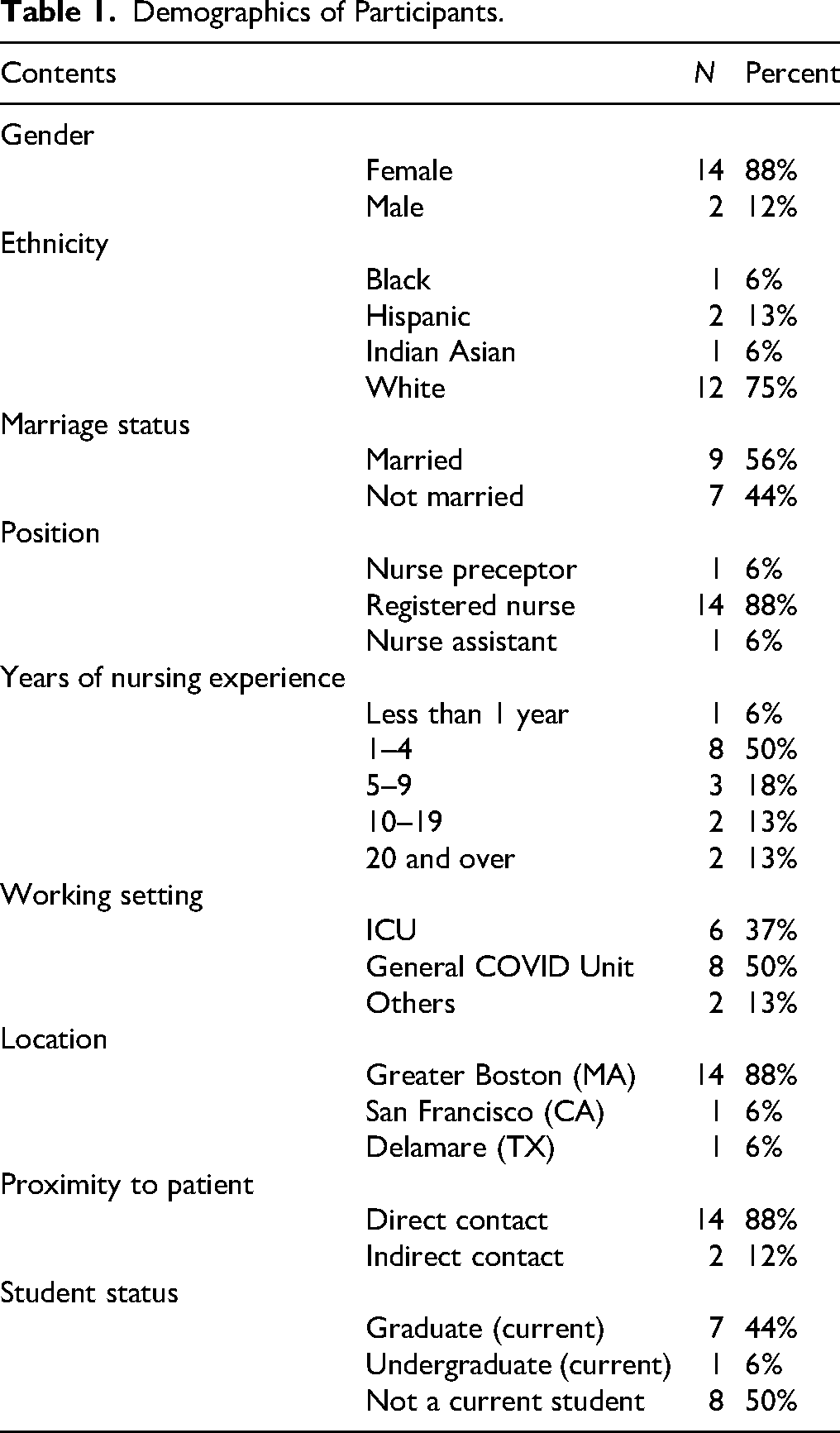
With an average nursing experience of 7.25 years and a standard deviation of 9.76 years, nine nurses (56%) had less than five years of nursing experience, including one nurse who worked for less than a year. Three nurses (18%) had nursing experience between five and nine years, while four nurses (26%) had more than 10 years of nursing experience. During the initial peak of the pandemic outbreak, 6 nurses (37%) worked in the ICU, 8 (50%) in the general COVID unit, and 2 (13%) in other departments. Fourteen nurses (88%) were working at hospitals in the Greater Boston area, Massachusetts. One nurse was working in San Francisco, California, and one nurse was working in Delaware, Texas. Among the 16 nurses, 14 (88%) worked in highly infectious environment and had direct contact with COVID-19 patients during the initial peak of the outbreak (Table 1).
Data Collection
Interviews were conducted between September and October 2020, approximately four months after the initial peak of COVID-19 outbreak and carried out remotely via Zoom and were recorded and transcribed. Interviews lasted between 40 and 60 min. Participants were asked open-ended questions using a semistructured interview guide. Transcripts from 16 interviewed nurses were utilized in the content analysis after being reviewed and verified by these interviewed nurses.
Data Analysis
Graneheim and Lundman’s (2004) qualitative content analysis method was used to conduct a thorough analysis of 16 interview transcripts. The process included four steps: (1) extracting meaning units from the transcripts, which are defined as words, sentences, or paragraphs that reflect specific issues narrated by the nurses; (2) condensing each meaning unit into a single sentence, known as the underlying meaning; (3) summarizing these underlying meanings into 2–3 word codes to identify specific stressors; and (4) creating themes representing threads of interpretation (Graneheim & Lundman, 2004). This process is illustrated in Figure 1, showing the steps from original transcript narratives to the identification and coding of stressors, and the creation of themes. The same content analysis method was used for narratives regarding interviewed nurses’ coping practices and the impact of pandemic-induced stress on the nurses’ career paths. The analysis and outcomes were reviewed, cross-checked, and verified by coauthors.
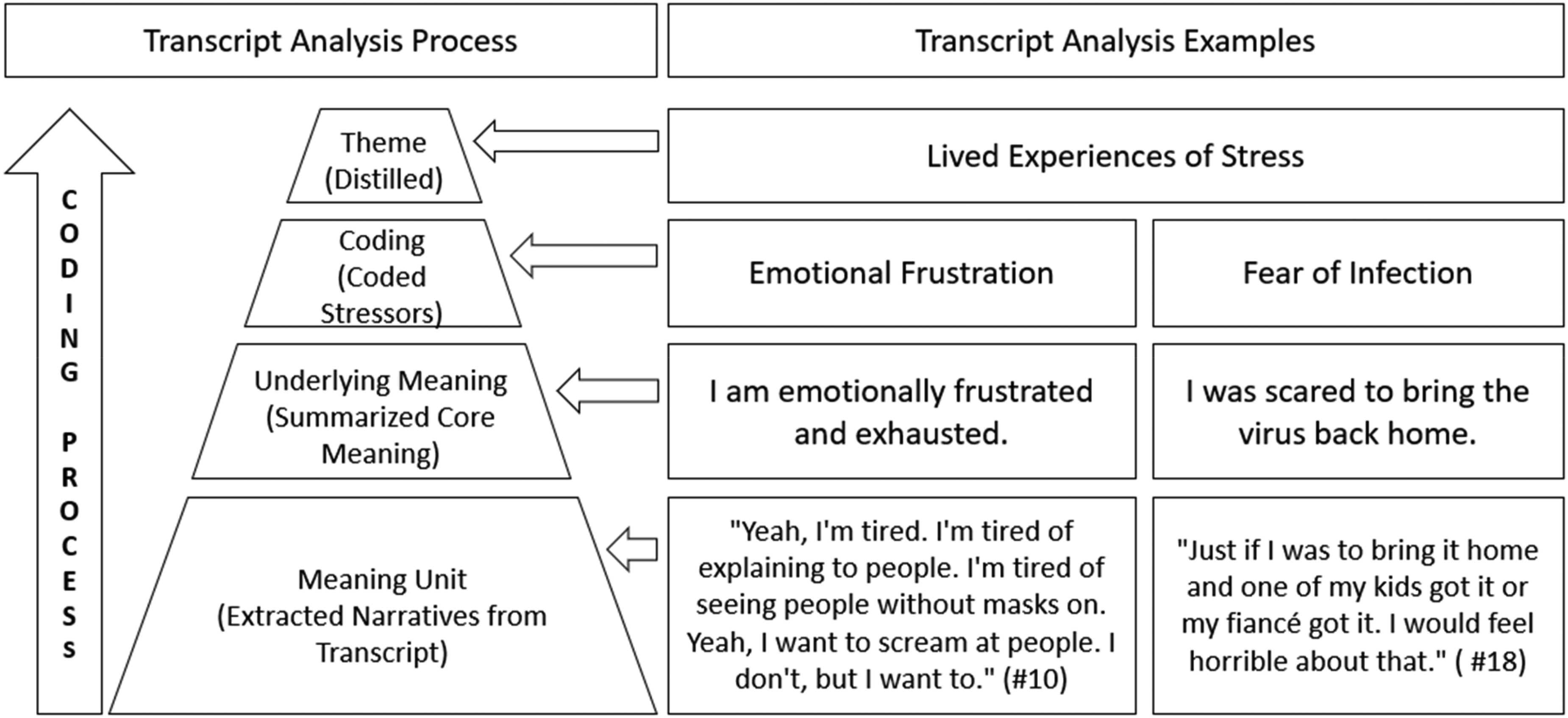
Transcript Analysis Process and Examples.
Ethical Consideration
The cross-sectional survey project, including this interview study as the second phase, was reviewed and deemed exempt by the Institutional Review Board at the University of Massachusetts (study number #2020084). Oral consent for audio recording was obtained from each participant prior to the start of the interview. An ID number was assigned to each participant to ensure anonymity during content analysis.
Results
Using Graneheim and Lundman's content analysis method, three themes were distilled from the coded narratives of the transcripts, each with its own subtitle. These subtitles are: (1) “Eight Identified Stressors” for experiences of stress, including eight stressors narrated by the interviewed nurses from their clinical encounters, listed in an order from most to least frequently reported; (2) “Adaptive Coping Practices” for the theme of adaptive coping practices employed by the nurses in response to the stressors; and (3) “Impacts on Career Path” for the impacts of the pandemic-induced stress on the nurses’ career paths related to their career goals and pursuits.
Eight Identified Stressors
Fear of infection: Out of the 16 participants, 12 (75%) expressed their fear of infection in highly infectious environments. One interviewed nurse expressed the fear, “Just if I was to bring it home and one of my kids got it or my fiancé got it. I would feel horrible about that” (Participant #18).
Emotional frustration: Eight nurses (50%) were emotionally frustrated to various degrees ranging from being unable to visit families and friends, to yelling at those who did not wear masks. One of the interviewed nurses emotionally expressed her frustration, “Yeah, I'm tired. I'm tired. I'm tired of explaining to people. I'm tired of seeing people without masks on. Yeah, I want to scream at people. I don't, but I want to” (Participant #10).
Lack of personal protective equipment: Seven participants (44%) encountered a shortage in the supply of personal protective equipment (PPE). An interviewed nurse told the interviewer, “The PPE still is in shortage, but I've been buying my own surgical masks” (Participant #17).
Overload of information and misinformation: Six participants (38%) felt that they were overwhelmed by a combination of information overload and misinformation that was hard to absorb and led to confusion. One of the nurses described the overwhelmed information influx, “We'd get like five emails a day about different policies and different procedures, like the PPE procedures have changed. I don't know if you want to know the specifics of that” (Participant #7).
Uncertainty at the workplace: Five nurses (31%) expressed worries about workplace uncertainty, not knowing what was going on and what would happen next. One of the interviewed nurses expressed the uncertainty, “In the beginning it was super frustrating and it kind of felt like nobody knew what was going on. That like we didn't, we didn't have leadership” (Participant #14).
Increased workload: Five nurses (31%) indicated an increased workload that ranged from occasional additional hours to some substantial amount of overtime. Three (19%) experienced a substantial increase in workload, one had a moderate increase, and one reported a slight increase. The remaining 11 (69%) nurses did not report working overtime. One interviewed nurse explained, “I did occasionally pick up an extra shift because we did have a need for more nurses at the time” (Participant #16).
Organizational disarray: Four nurses (25%) felt organizational chaos at the workplace and believed that managers were ill-prepared to manage the crisis. One nurse mentioned, “I don't think managers have been trained to deal with crises and to deal with how to help employees face all this. The managers, directors, even educators on the floor, I don't think they know how to handle, just personally, how to help people who are going through a tough time and need extra support” (Participant #9).
Professional stigma: One nurse pointed out instances of professional stigma in the workplace, where nurses’ knowledge and input were disregarded, and they were excluded from meetings that were meant to involve nurses. The nurse reflected, “The employer did not respect our knowledge and our input and held meetings without us” (Participant #1).
Adaptive Coping Practice
Several proactive coping approaches were reported by 12 nurses (75%), with many of them utilizing multiple methods. Some reported exercise, meditation, watching movies, and listening to music. Others used more personalized ways such as sleeping longer hours, engaging in gardening, studying, reading, and connecting with friends through social media. They were mindful about taking breaks and spending more quality time with families. Only one participant transferred to a different hospital for the purpose of reducing stress. When the interviewer asked, “On a more personal level, what have you been doing in response to stress?”, one of the nurses responded, “Just meditating and trying to be really regular about [it]. Even if I can't see friends and family, like talking to them over the phone and just kind of decompressing that way. I also like to run, that's something that is a de-stressor for me” (Participant #8). Another nurse echoed, “I've made exercise a demand on a daily basis. Um, and that has been very helpful, whether it be on my bike or yoga or meditation or something, but something every single day” (Participant #14).
Impacts on Career Path
The majority of the interviewed nurses (94%) in this study expressed a commitment to staying in their current position and continuing their nursing careers. Three of them (19%) took pride in their ability to save the lives of COVID-19 patients. They believed that their experience during the pandemic had strengthened their nursing career paths. When the interviewer asked, “How did these stressful experiences lead you to make changes in your career plans?” One nurse responded, “If anything, it's solidified them. I felt very privileged to be caring for such critically ill patients” (Participant #16). Twelve nurses (75%) reported that their COVID-19 experience had minimal negative impacts on their nursing careers. One nurse commented, “We're always going to deal with challenges that are un[fore]seen; and I think anyone who's considering the current nursing [career], should be aware of that, but it's also one of the most rewarding careers” (Participant #8). One nurse (6%) was considering transferring to an outpatient department, which she believed was less risky.
Discussion
Common and Unique Stressors
The discussion of the stressors shared by the participants ranged from high to low frequency. To provide the context, commonly identified stressors from the reviewed literature were compared with unique experiences narrated by the interviewed nurses in this study.
Fear of infection was consistently acknowledged as a top stressor among nurses both within the United States and globally during the initial peak of COVID-19 (Jo et al., 2021). However, this study revealed that the fear expressed by interviewed nurses was not only about getting infected themselves or cross-infecting internally within the hospital but more so about bringing the virus home and transmitting it to their immediate family members. In circumstances where the risk of infection was high and PPE was in short supply, one interviewed nurse specifically mentioned that she purchased surgical masks at her own cost for the safety of her immediately family and herself. Emotional frustration reported in this study was resonant with the reviewed literature. Emotions were widely recognized (Brown et al., 2023) and often manifested through feelings of anger, helplessness, or sadness (Lapum et al., 2021). These emotions could be negative and seen as part of the stress symptoms (Paterlini et al., 2022).
Lack of resources, especially the shortage of personal protective equipment, was prevalent during the initial peak of the COVID-19 outbreak. Based on the study by Rich-Edwards et al. (2021), approximately 22% of 22,232 frontline healthcare professionals in the United States reported facing occasional or consistent shortages of personal protective equipment. Overload of information and misinformation, including both accurate and misleading content spread through social media, created confusion during the initial peak of the pandemic (Russell, 2021). Our study suggests that the internal handling of information within healthcare organizations may also contribute to information overload and misinformation.
The study by Martin et al. (2023) indicated that about 62% of 53,533 nurses across 45 states in the US reported increased workload during the COVID-19 pandemic. However, the majority of the interviewed nurses did not report working overtime. Despite Massachusetts being among the worst hit states during the initial peak of the pandemic outbreak, the number of the interviewed nurses facing increased workload appeared to be fewer than that of the national average. Workplace uncertainty nurses faced from the onset of the pandemic (Temsah et al., 2022) was echoed by some of the interviewed nurses in this study. Not knowing what might unexpectedly happen next in the workplace could lead to physical and mental fatigue, therefore hindering professional effectiveness (Stavropoulou et al., 2022).
Organizational disarray appeared to be a new stressor that emerged from this study. Few studies have reported on this phenomenon (Mackay et al., 2022). Was the reported organizational disarray an issue of institutional leadership, systematic and strategic preparedness, or a tactic/technical problem? Were these shared narratives subjective perceptions from personal experiences of these nurses or could the perceived mismanagement and/or disorganization be objectively measured? The study on professional stigma by Labrague et al. (2021) showed evidence of a growing number of healthcare professionals reporting instances of being socially discriminated against and stigmatized. Among these professionals, nurses faced the greatest likelihood of encountering discriminatory actions or behaviors directed at them from the public (Labrague et al., 2021). However, one of the interviewed nurses in this study shared the experience of feeling neglected and excluded by the management within the organization. It raised the question of whether this experience was an isolated case perceived subjectively by the interviewed nurse or indicative of an issue within some healthcare institutions. Understanding the stressor of professional stigma may require further investigation at individual, leadership, and organizational levels.
Innate and Acquired Coping Dimensions
Stressors, acting as stimuli, trigger interactions between human body system and the external environment (Roy, 2009). They activate the body's integrated adaptation system to manage stress and compensate for challenges to functional capacity (Roy, 2009) posed by stressors. Roy’s (2009) adaptation model defines two coping dimensions: innate and acquired. The innate coping dimension, determined by an individual's genetic makeup (Roy, 2009), operates unconsciously in responses to stressors, as observed in the experiences of interviewed nurses. These responses may exemplify the innate coping mechanisms, constituting the first dimension of innate coping in the face of stressors.
The second dimension of coping, as outlined by Roy (2009), is developed through learning and can be acquired through real life experiences and deliberate training. According to interview findings, many nurses may consciously apply proactive practices, such as engaging in physical exercises, watching movies, listening to music, and meditation, which reflected the acquired coping dimension when facing identified stressors. The manifestation of this acquired coping dimension demonstrated that the interviewed nurses were able to minimize the negative impacts of stressors on their well-being and their nursing careers.
Impacts on Nursing Career Path
The initial peak of the COVID-19 outbreak put nurses under severe and enduring psychological stress (Galanis et al., 2021), which led to intense emotional fatigue (Kurtzman et al., 2022) and the high nursing workforce turnover, either through seeking employment elsewhere or leaving the nursing profession entirely (Grinspun et al., 2022). This study appeared to present a different and counterintuitive perspective. Among the 16 interviewed nurses, only one nurse expressed the consideration of changing her role from the inpatient unit to the outpatient unit to reduce potential exposure to the coronavirus. The remaining 15 interviewed nurses believed that their experience during the most stressful initial peak of the outbreak either minimally influenced their pursuit of a nursing career or strengthened their determination to continue their nursing trajectory.
It appeared that proactive and adaptive coping practices played a key role in fostering continued commitment to the nursing career among the nurses interviewed in this study. These nurses demonstrated the ability to proactively manage elevated stress levels through applications of adaptive coping practices. Although the causality was undetermined, the adaptive coping responses may have contributed to participants’ wellbeing and supported a sense of determination to continue in their nursing career.
Human Adaptation Levels
According to Roy's model, there are three levels of “life processes of the human adaptive system: integrated, compensatory, and compromised” (Roy, 2009, p. 36). The first level of adaptation is called integrated. It refers to the cohesive functioning of life processes to meet the body's needs (Roy, 2009), typically when nurses encounter stressful circumstances at a very early stage with body's automated function of eliminating stress. The second level of adaptation is called compensatory, activated when the stressful situation persists rather than attenuating (Roy, 2009). This level is also referred to as “the wisdom of the body” (p.150) which depicts the body's self-regulating process through extra and strengthened efforts to cope with continued stress (Roy, 2009). The third level of adaptation is called compromised when both integrated and compensatory levels are insufficient to cope with the increased or persistent stress (Roy, 2009), such as augmented stress from COVID-19 pandemic imposed on nurses, resulted in dysfunction of body's coping system and various health conditions. The effective intervention of acquired coping dimension, in conjunction with innate coping dimension, prevents body's adaptation system from escalating to the third coping level from the first and second levels (Roy, 2009).
According to the three-adaptation levels of Roy’s (2009) model, there is an intricate interplay between the innate and acquired coping dimensions. The innate coping dimension alone without acquired coping dimension is not sufficient to combat sustained stress (Roy, 2009). A deliberate development of practical coping skills through learning and training becomes essential. The proactive coping practice of interviewed nurses demonstrated that the acquired dimension helped reinforce the innate dimension, working together to mitigate stress before stressors surpass human adaptive capacity. Within the context of Roy's three adaptation levels, had interviewed nurses not actively engage in destressing themselves through various proactive adaptive coping activities, the integrated and compensatory adaptation levels might have escalated to the compromised adaptation level, leading to potential harm or damage to the physical and psychological well-being of these nurses. The damage from coping at the compromised adaptation level would ultimately result in severe burnout, physiological and psychological fatigue, and consequently force them to rethink their nursing professional path.
Implications for Nursing Practice
Nurses working in high-risk, infectious environments faced multiple stressors. Early recognition and preparedness could provide nurse managers with the tools to implement support mechanisms that protect both physical and psychological well-being. This study implies that structured stress-coping programs, jointly supported by healthcare organizations and nursing education, could strengthen nurses’ acquired coping skills. Regular training, whether annual or periodic, could reinforce resilience, promote well-being, and help reduce turnover. Despite high-stress and high-infectious environments, encouraging individually tailored self-care practices and adopting proactive coping mechanisms with ongoing support could empower nurses to remain committed to their carers during public health crises.
Recommendations
The human adaptive system is a nonlinear, multifaceted, and intricate phenomenon (Roy, 2009). Rather than a single stimulus triggering a specific response, this system operates through complex interaction (Roy, 2009), involving an interplay between innate and acquired dimensions. The acquired dimension, characterized by learned skills, requires nurturing and training. This feature underscores the need for ongoing support and development to optimize the functioning of the nurses’ adaptive system through health organization-initiated training programs. The stress-alleviation programs need to be specifically designed to enhance nurses’ coping capacity in both clinical and academic settings. These programs should be implemented through collaboration between healthcare organizations and nursing departments of education institutions. By doing so, they not only boost the frontline nurses’ self-confidence but also strengthen their trust in the institutions they serve. The programs focus on enhancing awareness of the acquired dimension, providing nurses with stress-coping strategies, and equipping them with practical coping skills. Implementing stress-coping training programs annually for frontline nurses could serve as a potential intervention strategy for reducing stress and sustaining workforce stability.
Strengths and Limitations
This study represents a significant contribution to nursing literature by applying the Roy adaptation model to examine stress coping among frontline nurses during a public crisis. It is, to our knowledge, the first paper to utilize the concepts of innate and acquired coping skills as well as three adaptation levels within this model to interpret how nurses successfully adapted to highly stressful and infectious environments. This novel application provides a new theoretical lens for understanding nurses working environment adaptation and contributes meaningfully to the body of knowledge on nurse coping mechanisms.
In the meantime, we also acknowledge some of the limitations of this study. All eight stressors were reported subjectively by interviewed nurses. Differentiated years of working experience and varied working environment might lead to distinct personal interpretations of the degrees or extents of these identified stressors. This raises the question of whether these differences could potentially hinder an unbiased understanding of the magnitude of impacts that each stressor had on nurses, both physically and psychologically. Similarly, we do not know how the unexpected duration of the pandemic may affect frontline health workers’ coping responses or career path decisions. The relatively small university-based sampling of 16 interviewed nurses also limits the generalizability and representativeness of this study's findings to a larger population of nurses.
Conclusion
This study unraveled unique characteristics experienced by the interviewed nurses working in highly infectious environment during the initial peak of COVID-19 outbreak. Particularly, they exhibited resilience and strong determination to continue their professional trajectory in nursing despite high risks of infection and overwhelming stress. Their stress coping practices revealed an intricate interplay between the innate and acquired coping dimensions. It posited that fostering awareness of the acquired coping dimension could yield conscious coping practices, subsequently reducing workplace stress. It was proposed that nurses’ capacity for coping with stress could be nurtured by harnessing the acquired dimension through stress alleviation programs. It aimed to purposefully attenuate the high turnover within the nursing workforce through implementing stress-coping training programs as a potential intervention strategy. This study offers important considerations and suggests possible strategies to strengthen the nursing workforce during times of major public health crises, particularly in environments with high infection risks. It serves as an empirical backdrop for future studies aimed at developing resilient responses to unforeseen challenges in the face of the likely emergence of public health crises in the future.
Supplemental Material
sj-pdf-1-son-10.1177_23779608251385729 - Supplemental material for Frontline Nurses’ Coping Practices and Career Impacts in Highly Infectious Environments: A Roy Adaptation Model Perspective
Supplemental material, sj-pdf-1-son-10.1177_23779608251385729 for Frontline Nurses’ Coping Practices and Career Impacts in Highly Infectious Environments: A Roy Adaptation Model Perspective by Hua Chen, PhD(c), Lingling Zhang, MPA, MS, ScD, FAMIA, Janice Foust, RN, PhD, Suzanne G. Leveille, RN, PhD, Grace Derboghossian, RN, Sarin M. Tapalyan, RN, PhD and Ellen Benjamin, RN, PhD in SAGE Open Nursing
Supplemental Material
sj-pdf-2-son-10.1177_23779608251385729 - Supplemental material for Frontline Nurses’ Coping Practices and Career Impacts in Highly Infectious Environments: A Roy Adaptation Model Perspective
Supplemental material, sj-pdf-2-son-10.1177_23779608251385729 for Frontline Nurses’ Coping Practices and Career Impacts in Highly Infectious Environments: A Roy Adaptation Model Perspective by Hua Chen, PhD(c), Lingling Zhang, MPA, MS, ScD, FAMIA, Janice Foust, RN, PhD, Suzanne G. Leveille, RN, PhD, Grace Derboghossian, RN, Sarin M. Tapalyan, RN, PhD and Ellen Benjamin, RN, PhD in SAGE Open Nursing
Footnotes
Acknowledgments
The study was supported by Dr. Lingling Zhang's startup funds from the Donna M. and Robert J. Manning College of Nursing and Health Sciences, University of Massachusetts Boston.
Ethical Consideration
The cross-sectional survey project, including this interview study as the second phase, was reviewed and deemed exempt by the Institutional Review Board at the University of Massachusetts (study number #2020084). Oral consent for audio recording was obtained from each participant prior to the start of the interview. An ID number was assigned to each participant to ensure anonymity during content analysis.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The Manning College of Nursing and Health Sciences, University of Massachusetts Boston, (grant number Dr. Lingling Zhang’s Startup Funds).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.