
Abstract
Introduction
While the psychological impact on healthcare workers has been widely acknowledged, accessible interventions tailored to address these mental health challenges in the post-pandemic context remain limited.
Objectives
This study aimed to assess the impact of a mHealth-based group coping skills training on the level of stress, anxiety, depression, and posttraumatic stress disorder (PTSD) symptoms of frontline nurses post-COVID 19.
Methods
A non-randomized pretest-posttest design was conducted. Ninety nurses who had direct contact with COVID-19 patients were selected through convenience sampling. The intervention group received access to a 2-week online multimedia psychoeducational program through a WhatsApp group, while the control group received standard educational content (text based). The Generalized Estimating Equation (GEE) analysis was applied to evaluate the intervention's effects on the scores for depression, anxiety, stress, and PTSD across the follow-up.
Results
The intervention group showed lower PTSD symptoms (−4.40; 95% CI: −7.07 to −1.66), depression (−1.60; 95% CI: −2.58 to −0.80), anxiety (−1.91; 95% CI: −3.06 to −0.77), and stress scores (−2.29; 95% CI: −3.61 to −0.97) compared to the control group, after adjusting for time points. GEE analysis confirmed that the intervention group had significantly lower PTSD symptoms (−5.54; 95% CI: −8.47 to −2.61), depression (−1.78; 95% CI: −2.73 to −0.83), anxiety (−2.52; 95% CI: −3.77 to −1.28), and stress scores (−2.96; 95% CI: −4.37 to −1.55) after adjusting for characteristic variables.
Conclusion
The mHealth-based group coping skills training intervention significantly reduced PTSD symptoms, depression, anxiety, and stress scores among frontline nurses, with persistent benefits over time. These results highlight the potential of scalable, app-based and smartphone-enabled interventions delivered within an online group format to support the mental resilience of healthcare workers, underscoring the need for healthcare organizations to prioritize the implementation of such mobile-delivered programs to promote the well-being and retention of critical nursing staff.
Background
In 2020, the COVID-19 pandemic began changing global healthcare dynamics in various ways. In healthcare settings, COVID-19 significantly increased nurses’ working hours and created a high-stress environment. Due to the high number of hospitalizations, nurses had to work rapidly, contributing to negative health outcomes like disease complications and death (Readeau et al., 2023; Su et al., 2023). This situation caused nurses to experience anxiety because they lacked time to debrief, process grief, heal from trauma, and recover (Andrade et al., 2024; Angus et al., 2023; Salameh et al., 2023). Such experiences can affect work performance and communication skills, and increase irritability, denial, anger, and sleep disturbances (Angus et al., 2023). Additionally, concerns have been raised that mental health disorders among nurses could reduce the quality of patient care.
Stress disrupts the relationship between individuals and their environment (Jackson & Serenko, 2023; Valipoor et al., 2023). High-stress work environments have negatively affected nurses’ mental health, contributing to anxiety, depression, posttraumatic stress syndrome (PTSS), and posttraumatic stress disorder (PTSD) (Becket-Davenport et al., 2023; Salameh et al., 2023; Wu, Dai, Jing et al., 2023). Factors such as trauma, crowded conditions, lack of support, frequent exposure to death, and disrupted circadian rhythms due to work overload increase the risk of PTSD among nurses. Researchers in China found that nurses, especially women, working in intensive care units (ICUs) and COVID-19 wards were at the highest risk of developing PTSD-like symptoms (Wu, Dai, Jing et al., 2023). Other studies indicate that PTSD prevalence among ICU nurses ranges from 10% to 20% or higher (Zhang et al., 2023). A meta-analysis reported that during the pandemic, the prevalence rates of anxiety, depression, and insomnia were 23%, 28%, and 39%, respectively, with female healthcare providers, particularly nurses, exhibiting higher rates of affective symptoms compared to males (Kwon & Lee, 2022; Salari et al., 2020). The pandemic has highlighted the crucial need to recognize and address psychological distress and mental health issues among nurses, as well as to support their development of effective coping strategies.
Review of Literature
Effective stress management for nurses involves adopting coping strategies suited to high-pressure environments. Folkman (2013) describes two main functions of coping, including instrumental coping, which is associated with problem-centered coping styles, and regulatory coping, which is associated with emotional-centered coping strategies (Folkman, 2013). Coping skills training has been shown to maintain mental health in the wake of the negative consequences of the COVID-19 pandemic (Mulianda et al., 2022). In particular, mindfulness and moral resilience, cognitive behavioral therapy (CBT), motor interference therapy, and reconsolidation of traumatic memories proved beneficial in preventing the development of mental health issues in nurses during the pandemic’s challenging time (O’Doherty et al., 2023; Smith et al., 2021). Nurses who were unable to actively cope with high levels of stress and burden experienced the worst health outcomes and engaged in more unhealthy behaviors compared to their better-coping counterparts (Muhamad Robat et al., 2021; Varghese et al., 2023). Promoting mental health awareness and supporting the development of effective coping skills among nurses, especially among those who experienced burnout during the COVID-19 pandemic, is crucial for preventing anxiety, depression, and PTSD, and contributing to their well-being and quality of life (Huda et al., 2024; Sesaria et al., 2020).
Mobile health (mHealth) applications were widely adopted during the COVID-19 pandemic for self-assessment, contact tracing, and online health appointments (Huhn et al., 2022; Kruse et al., 2023; Tan et al., 2023). These digital interventions can engage those in need of psychological support and provide flexible treatment options while maintaining physical distance to prevent disease transmission. However, there is limited research on the measured effects of this digital approach. A recent review found that only 27% of mHealth apps supporting individuals during the pandemic were designed for healthcare professionals, with the majority targeting patients and their families (Tan et al., 2023). In 2020, there were more than 160 million smartphone users in Indonesia (Statista Report, 2024), and 47% of these users accessed health apps (Kwee & Widjojo, 2022), indicating increasing engagement with digital health tools. This presents a significant opportunity to develop mHealth-based group coping skills training, especially for nurses, who are highly exposed to technology.
Research Objective
To address the need for coping skills training and to maintain the mental health of Indonesian nurses after the COVID-19 pandemic, we developed an mHealth group-based coping skills psychoeducational training program. The purpose of this research was to investigate the effectiveness of this digital-based intervention. Specifically, our research question was “Can a mHealth group-based coping skills psychoeducational training program reduce the depression, anxiety, and PTSD symptoms among frontline nurses?.”
Methods
Study Design
This study employed a quasi-experimental, two-group, pretest-posttest design to evaluate changes in mental health indicators before and after the intervention. This design was appropriate due to the urgent need to address mental health issues and the practical and ethical challenges of working with a specific group of frontline nurses, enabling effective evaluation of the program's impact despite the lack of randomization. The research involved two groups: an intervention group and a control group. The study was conducted at two time points: before the intervention (T1) and after the intervention (T2). The independent variable was the mHealth-based group coping skills training, while the dependent variables were stress, depression, anxiety, and PTSD symptoms scores, measured using relevant questionnaires.
Ethical Approval
Ethical approval was obtained from the Ethics Committee of Nursing and Health Research, Faculty of Nursing, University Riau, Indonesia (approval number 68/UN.19.5.1.8/KEPK.FKP/2023, 23th May 2023).
Research Question
What is the effect of an mHealth-based group coping skills training delivered through a WhatsApp group compared to standard educational content (text based) on the levels of depression, anxiety, stress, and PTSD symptoms among Indonesian nurses impacted by the COVID-19 pandemic?
Sample
Ninety out of 250 eligible individuals who work full time, including direct care nurses and managers, were selected from a list of nurses who had direct contact with COVID-19-infected patients using convenience sampling. The respondents who were selected had worked in the hospital for at least 2 years, though most of the respondents had worked in the hospital for longer. To detect significant differences between groups at a 5% significance level with 90% power, a minimum sample size of 36 participants per group was required. Considering a potential 30% attrition rate, a sample of 45 participants per group was determined to be sufficient to evaluate the effects of the intervention.
Inclusion Criteria
The inclusion criteria encompassed nurses who had direct contact with COVID-19 patients, expressed a willingness to participate, and had no previous history of mental health problems, such as ever being diagnosed with schizophrenia. The participants’ mental health status was reviewed in their healthcare worker record kept at the hospital. All participants signed an informed consent form, voluntarily took part in the study, and authorized the review of their healthcare worker record. They were assigned to one of the two study groups: the mHealth-based group coping skills training as the intervention group (n = 45) and standard educational content (text based) as the control group (n = 45).
Data Collection Procedure
Participant recruitment occurred from June 1 to October 10, 2023. A trained research assistant approached participants in person to invite them to voluntarily take part in the study. Written informed consent was obtained during a face-to-face interview. Participants were divided randomly and alternatively into the two groups: the first enrolled participant was allocated to the intervention group, then the next participant to the control group and so on. After consenting and completing the baseline measurement (T1) using questionnaires, participants were asked to provide their phone numbers and invited to join a WhatsApp group on their smartphones. The questionnaires were administered by an independent assessor, who was also a research assistant, and who had been trained to conduct measurements at specified time points. Engagement with the modules was actively monitored through follow-up by the research assistant via WhatsApp, ensuring all participants accessed and completed the modules.
Intervention
The mHealth-based group coping skills training was developed using the Transactional Model of Stress and Coping proposed by Lazarus and Folkman (1984) and Folkman (2013). The components of the psychoeducational program followed the protocol described by Shaygan et al. (2021). All participants in the intervention group received access to an online multimedia psychoeducational training for 2 weeks. The training included four modules that were scientifically based on relaxation training, breathing exercises, meditation, and principles of positive psychology (Figure 1). Participants were asked to complete all modules, each of which took approximately 40 min, and during the 2 weeks to engage in the module learning or follow-up tasks on a daily basis. Each module included videos, Microsoft PowerPoint™ files, educational texts, and an exercise related to the module’s content. All materials were designed by a team of psychologists, psychiatrists, public health experts, and a nurse manager and a clinical nurse with 7 years of experience based on the results of an extensive literature review. The intervention was culturally adapted to address language barriers, health beliefs, and myths related to COVID-19. After developing the intervention, the expert team evaluated the content, implementation strategy, usefulness, and applicability of the intervention through the use of an evaluative checklist (see Appendix 1 in the supplementary materials). The team also provided input on the ideal delivery strategy.

Components of an mHealth-group based coping skills training.
WhatsApp (Meta, US), a chat-based social media platform, was used to deliver the daily multimedia psychoeducational content to the nurses between 8 AM and 8 PM. Participants were asked to complete the modules and follow-up exercises outside of working hours. Participants could ask questions and discuss module content with the research team if they did not fully understand the training. Researchers sent emails and WhatsApp messages to remind and encourage participants to complete each module and their follow-up assessments after finishing the modules. All participants were fully engaged in all the modules. During the study process, the research team evaluated the completeness of each module and responded to all participants’ questions.
Control
The control group received standard care, such as routine health education flyers from the nursing department. Health education flyers consist of explanations related to managing mental health and finding support. However, they did not receive any face-to-face sessions or special training. At the end of the data collection period, control group participants received the same supplemental material booklet and training as the intervention group.
Measures
Subjects completed the Indonesian version of two questionnaires. The Depression, Anxiety, Stress Scale-21 (DASS-21) was used to measure the score of depression, anxiety, and stress (Lovibond & Lovibond, 1995). The Impact of Event Scale-Revised (IES-R) questionnaire was used to measure the score of PTSD symptoms (Weiss, 2007). Demographic data were also collected at the baseline (T1). The questionnaires took about 15–20 min to complete.
DASS-21 (Depression, Anxiety, and Stress Scale 21)
DASS, or Depression, Anxiety, and Stress Scale 21, is a shorter version of the DASS 42. The Indonesian version of DASS-21 is a 21-item self-administered questionnaire comprising three scales to assess the three aforementioned emotional states. It has good validity as an approved instrument for measuring adverse mental health status, including depression, anxiety, and stress in adults. It has been translated into various languages, including Indonesian (Ifdil et al., 2022).
The results indicate that the DASS-21 is a valid and reliable instrument, with an item reliability value of 0.99, sufficient person reliability of 0.89, and a Cronbach alpha value KR-20 of 0.91. The seven elements on the scales are graded on a Likert scale from 0 to 3 (0: “Did not apply to me at all,” 1: “Applied to me to some degree or some of the time,” 2: “Applied to me to a considerable degree or a good part of the time,” and 3: “Applied to me very much or most of the time”). Depression, anxiety, and stress scores are multiplied by 2 to get the final scores for comparison with the cut-offs. According to the original properties, the resulting ratings are then classified as “normal, mild, moderate, severe, or extremely severe” (Lovibond & Lovibond, 1995).
The Impact of Event Scale-Revised (IES-R)
The Impact of Event Scale-Revised (IES-R) Questionnaire was used to measure stress levels and symptomatology due to the impact of the traumatic events (post-traumatic stress disorder) of the pandemic. The scale assesses the subjective distress caused by stressful and traumatic situations experienced by participants. Participants were asked to rate each item on a scale from 0 to 4 (0: “Not at all,” to 4: “Extremely all”) based on their experiences of traumatic events in the previous seven days. The overall score is between 0 and 88 (Warsini et al., 2015).
According to Horowitz et al. (1979), a score of >24 suggests some PTSD symptoms, >33 is the optimal cut-off threshold, and >37 indicates immune system suppression and severe PTSD. The Indonesian version has been translated and revealed a Cronbach’s alpha value of 0.90 for the test and 0.92 for the retest for the total score which shows it has good validity (Warsini et al., 2015).
Data Analysis
All statistical analyses were conducted using SPSS, version 23 (IBM, Inc., Armonk, NY, USA). The significance level was set as p value <.05. Descriptive statistics were used to summarize the characteristics and the scores for depression, anxiety, stress, and PTSD. Group differences in sample characteristics were assessed using an independent-sample t-test for continuous variables and chi square tests for categorical variables. The Generalized Estimating Equation (GEE) analysis was used to evaluate the intervention's effects on the scores for depression, anxiety, stress, and PTSD across the follow-up. Each GEE model included the main effects of time (baseline as the reference category) and intervention effect (control group as the reference category), the two-way interaction effects of time × intervention, and the main effects of control variables (patient characteristics). Patient characteristics as shown in Table 1 were treated as the control variables in the GEE model. The differences between the two groups in terms of the change from baseline (T1) to the later follow-up (T2) were warranted when the interaction effects were significant, suggesting the intervention effect was supported.
Participants’ Characteristics.
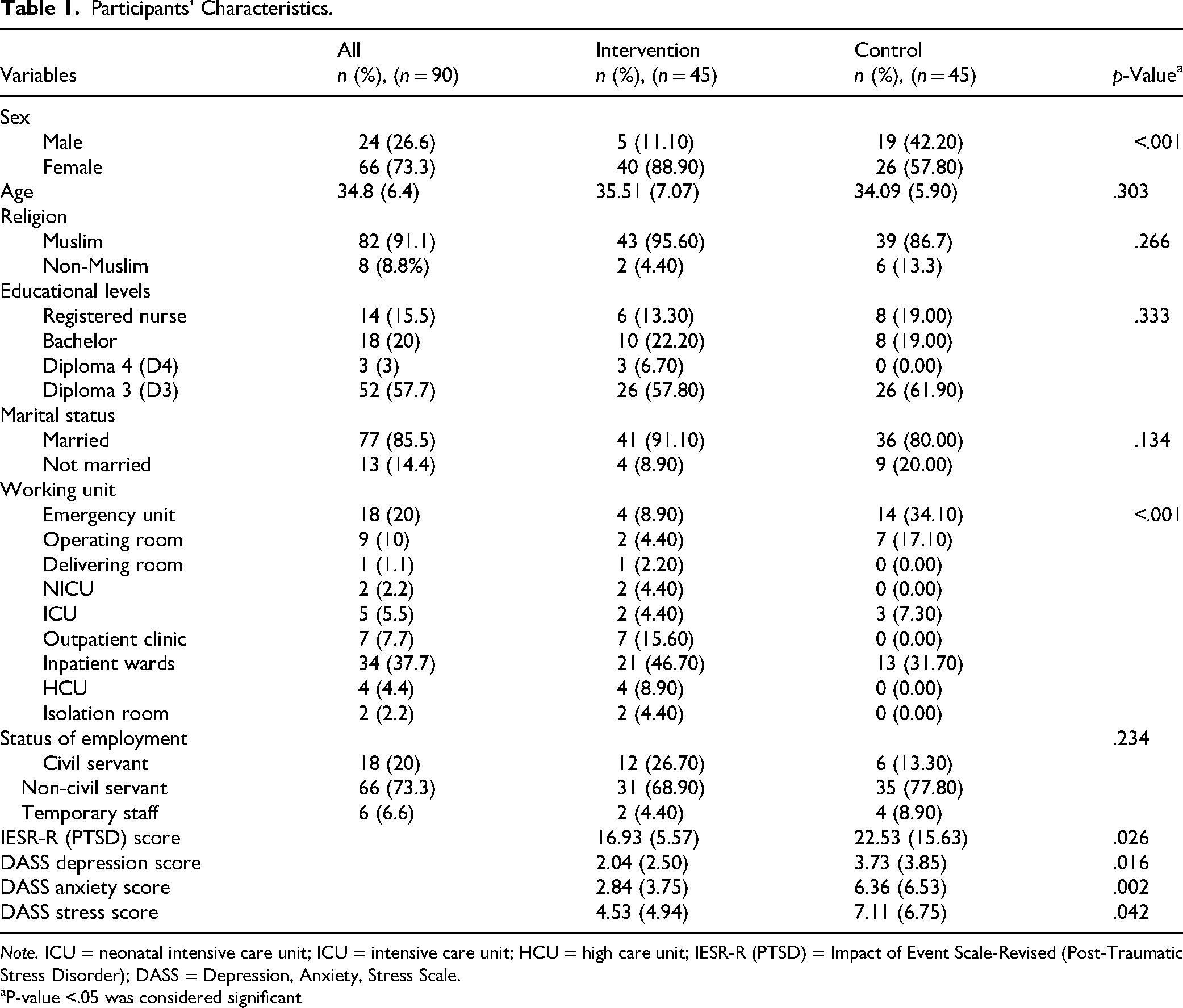
Note. ICU = neonatal intensive care unit; ICU = intensive care unit; HCU = high care unit; IESR-R (PTSD) = Impact of Event Scale-Revised (Post-Traumatic Stress Disorder); DASS = Depression, Anxiety, Stress Scale.
P-value <.05 was considered significant
Results
A total of 90 participants were included, with a mean age of 34.8 years (SD: 6.4) for both groups. Female participants represented 73.3% of the total. Most were Muslim (91.1%) and married (85.5%). Additionally, 73.3% were noncivil servants and most worked in inpatient wards (37.7%). Up to 35.5% had a bachelor's degree in nursing while most of the participants had graduated with a diploma in nursing (indicated 3 years of nursing education, compared to 5 years for those with a bachelor's in nursing). No significant differences were found between the intervention and control groups regarding age, religion, educational level, marital status, and employment status. However, significant differences were noted in sex and working unit variables. The intervention group had more female participants while the control group had more participants in the emergency unit and wards. Significant differences were also found in baseline outcome variables (depression, anxiety, stress, and PTSD scores) where the control group showed higher depression, anxiety, stress. and PTSD. This differentiation could be caused by their workplace, as most of the control group respondents worked in the emergency unit and ward. Previous research found that nurses working in emergency wards were more vulnerable to distress, anxiety, depression, and posttraumatic syndromes (Aditya et al., 2022; Carmassi et al., 2022: Kottler et al., 2025). Table 1 shows the participants’ characteristics by group.
Table 2 shows the impact of the intervention on all outcome variables, stratified by time points. At T2, significant impacts were observed on all outcome variables, except anxiety scores. Participants in the intervention group had lower depression and anxiety scores compared to the control group at T2. The table also shows the impact of time points on all outcome variables for both the intervention and control groups. In the intervention group, significant effects of time were observed on outcome variables, except for anxiety scores. In the control group, significant effects of time were found for all outcome variables, including anxiety scores. Among intervention participants, a significant decrease in depression, stress, and PTSD scores was noted. The control group also showed lower depression, anxiety, stress, and PTSD scores at T2 compared to T1. An improvement trend in DASS scores was observed in both groups.
The Impacts of the Intervention on the Outcome Variables Stratified by Time Points.

Note. IESR-R (PTSD) = Impact of Event Scale-Revised (Post-Traumatic Stress Disorder); DASS = Depression, Anxiety, Stress Scale.
P-value <.05 was considered significant.
Table 3 displays the results of a simple GEE model assessing the intervention's impact on PTSD and DASS-related scores at various time points. The intervention significantly affected PTSD, depression, anxiety, and stress scores. A notable effect of time points was observed for all outcome variables. After controlling for time, participants in the intervention group had lower PTSD scores (−4.40; 95% CI: −7.07 to −1.66), depression scores (−1.60; 95% CI: −2.58 to −0.80), anxiety scores (−1.91; 95% CI: −3.06 to −0.77), and stress scores (−2.29; 95% CI: −3.61 to −0.97)) compared to the control group.
Results of the GEE Model on the Outcome Variables.

Note. PTSD = post-traumatic stress disorder; CI = confidence interval.
Table 4 shows the results of an adjusted GEE model examining the intervention's impact and time points on various outcome variables. The analysis revealed significant intervention effects on PTSD, depression, anxiety, and stress scores after controlling for characteristic variables. Specifically, participants in the intervention group had significantly lower PTSD scores (−5.54; 95% CI: −8.47 to −2.61)), depression scores (−1.78; 95% CI: −2.73 to −0.83), anxiety scores (−2.52; 95% CI: −3.77 to −1.28)), and stress scores (−2.96; 95% CI: −4.37 to −1.55)) compared to the control group, even after adjusting for characteristic variables and time.
Results of an Adjusted GEE Model for the Intervention and Time on all Outcomes.

Note. PTSD = post-traumatic stress disorder; CI = confidence interval.
Adjusted with baseline outcome variable (PTSD, Depression, anxiety, and stress), age, sex, religion, educational level, marital status, working place, and working status.
Discussion
This study explored the impact of mHealth-based group coping skills training on the mental health of front-line nurses following the COVID-19 pandemic. The results demonstrated significant improvements in PTSD symptoms, depression, anxiety, and stress scores among the intervention group. These findings suggest that the mHealth-based group coping skills training effectively supports mental health, aligning with prior research showing the benefits of digital mindfulness-based self-help applications in reducing stress among healthcare professionals (Arshed et al., 2023; Baumann et al., 2023). The mechanism underlying this effectiveness relates to the cognitive appraisal and coping processes emphasized by the Transactional Model of Stress and Coping (Folkman, 2013). The intervention provided psychoeducation and practical exercises—such as relaxation, breathing, and meditation—that helped participants reframe stressors and develop adaptive coping strategies. Additionally, the accessibility and instantaneousness of WhatsApp facilitated active engagement and peer support, which are known to enhance motivation and reinforce learning. This study demonstrates that this mHealth-based intervention could be implemented as a part of a coping skill strategy to support healthcare professionals’ mental health (Arian et al., 2021; Jaafari et al., 2023).
During the pandemic, healthcare professionals, including nurses, were at the frontline, facing chaotic situations and the risk of virus transmission. The stress experienced by many nurses eroded their resilience. Resilience is the ability to cope with stress through healthy strategies, enabling individuals to achieve their goals with minimal physical and psychological cost (Pranata et al., 2022). Resilience is essential for reducing the impact of traumatic situations, including lowering anxiety, depression, and PTSD symptoms, and enhancing the quality of care provided (Bennett et al., 2023; Ye et al., 2022). While most individuals typically demonstrate resilience after trauma, several factors can affect this adaptation process. These factors include a history of mental health disorders, being female, limited access to social support, recent childbirth or nursing, and the intensity of emotions experienced, such as anger and stress (King et al., 2021; Park, 2005). Nurses often exhibit one or more of these factors, which can hinder their adaptation process. Given the decline in nurses’ resilience during the COVID-19 pandemic, it is crucial to develop alternative coping strategies to help rebuild their resilience. The coping skills training approach taken in our intervention aimed to assist in resolving their mental health issues rather than merely suppressing them.
The intervention group that engaged with the various training modules in this psychoeducational training, experienced decreased stress, anxiety, depression, and PTSD scores compared to the control group, indicating that focusing on relaxation, breathing exercises, meditation, and psychological principles can improve nurses’ coping strategies and mental health. The modules in our intervention consisted of videos, presentations, and narratives. Previous research has shown that educational videos administered during the COVID-19 pandemic were particularly effective at increasing knowledge, reducing communication barriers, and decreasing anxiety symptoms (Delanerolle et al., 2022; Salameh et al., 2023; Wu, Dai, Xiao et al., 2023). Moreover, such videos proved to be more effective at increasing knowledge and encouraging behavior change towards using appropriate coping strategies, compared to paper-based education. Behavioral change programs delivered via video have also received high satisfaction levels (Nolan et al., 2021; Shek et al., 2023; Zhu et al., 2021).
Among participants in our study, 20% worked in emergency care units, where healthcare professionals faced higher distress levels compared to other departments. Additionally, more participants in our study were female than male, aligning with nursing staff demographics. The high percentage of nursing staff that are female may be related to females experiencing higher rates of PTSD during the pandemic (Andreou et al., 2011; D’Amico et al., 2023). Female nurses may have also experienced increased psychological burden due to their fear of spreading the virus to their family members at home. The increased stress experienced both at work and at home highlights the need for positive coping strategies. Studies indicate that using positive methods like relaxation and humor is linked to better outcomes, including reduced posttraumatic stress (Er & Sökmen, 2018; Liao, 2021; Liu et al., 2023). Although our study noted slight improvements in nurses’ mental health, it also found that the pandemic's effects were long-lasting. A well-implemented coping skills intervention might have significantly reduced PTSD over time. Thus, timely development and delivery of specific coping skills approaches are crucial to prevent the negative impacts of mental pressures on nurses (Bryant, 2021; Huda et al., 2024).
Strengths and Limitations
The novelty of this study is grounded in the Transactional Model of Stress and Coping used in the development of this mHealth-based group coping skills training, which emphasizes appraisal to evaluate harm, threat, and challenges in the process of coping with stressful events, including the COVID-19 pandemic. A group of public health, nurse manager, and psychology experts were involved in the development of the intervention and measures. Educational videos embedded in the mobile app were carefully designed based on the literature and COVID-19 guidelines released by the Ministry of Health, the Republic of Indonesia. Other programs, such as relaxation, breathing techniques, and meditation also supported the process of coping and recovery. This mHealth-based group coping skills intervention is also designed as a cultural adaptation to address language barriers, health beliefs, and myths related to COVID-19 prevention and control. The implementation of cultural adaptations has been suggested for health education, as it allows for the process of learning and adaptation, therefore increasing knowledge and skill transfer.
This study acknowledges a few limitations. First, the nonrandomized design led to significant differences in participant characteristics between the groups, particularly sex. This introduced potential bias and affected the internal validity of the findings. Second, the short follow-up period of only 3 weeks restricts the insights that can be gained regarding the long-term impact of the intervention. Third, the small and region-specific sample size limits the generalizability of the results to other populations. Fourth, although we used GEE analysis to account for confounders, we did not perform a formal Difference-in-Differences (DiD) analysis, which could better address baseline disparities. Finally, the baseline imbalances between the groups, as well as the reliance on self-reported measures, may have influenced the study's findings. These factors warrant a cautious interpretation of the study's findings.
Implications for Practice and Further Research
A mobile-based coping skills training can be implemented for use by healthcare professionals, especially nurses, to help them cope with stressful conditions, such as infection outbreaks. Mobile-based applications are easy to access and reduce the burden of paper-based interventions which lack attractiveness and engagement. However, potential harms such as increased screen time, frustration with content, and privacy concerns should be carefully monitored. Barriers to implementation include limited internet access, cultural or language mismatches, and varying levels of digital literacy. Addressing these factors is crucial for effective and safe deployment.
In future research, we recommend conducting a randomized controlled trial, a Difference-in-Differences (DiD) analysis with longer follow-ups in larger populations, and extended follow-up in communities or multicenter hospitals to establish effectiveness, broader applicability, and sustainability. Qualitative research or a mixed-method study could also be considered as these methods would allow researchers to explore the perceptions, feelings, and emotions of nurses when facing an infectious disease outbreak and struggling with the negative consequences of their mental health.
Conclusions
mHealth-based group coping skills training effectively decreased the stress, anxiety, depression, and PTSD symptoms among nurses in the intervention group compared to the control group after 3 weeks of follow-up. This mobile-based group intervention was developed to overcome a lack of coping strategies and a supportive system during the traumatic events and heavy burdens that nurses experienced during COVID-19. This digital intervention can be implemented as an effective and efficient tool to deliver a coping skills approach and psychoeducational program during future disease outbreaks.
Supplemental Material
sj-docx-1-son-10.1177_23779608251379030 - Supplemental material for Enhancing Mental Resilience Among Frontline Nurses Post-COVID-19: A Non-Randomized Study of mHealth-Based Group Coping Skills Training
Supplemental material, sj-docx-1-son-10.1177_23779608251379030 for Enhancing Mental Resilience Among Frontline Nurses Post-COVID-19: A Non-Randomized Study of mHealth-Based Group Coping Skills Training by Nurul Huda, Malissa Kay Shaw, Made Satya Nugraha Gautama, Satriya Pranata, Bayu Satria Wiratama and Made Ary Sarasmita in SAGE Open Nursing
Supplemental Material
sj-docx-2-son-10.1177_23779608251379030 - Supplemental material for Enhancing Mental Resilience Among Frontline Nurses Post-COVID-19: A Non-Randomized Study of mHealth-Based Group Coping Skills Training
Supplemental material, sj-docx-2-son-10.1177_23779608251379030 for Enhancing Mental Resilience Among Frontline Nurses Post-COVID-19: A Non-Randomized Study of mHealth-Based Group Coping Skills Training by Nurul Huda, Malissa Kay Shaw, Made Satya Nugraha Gautama, Satriya Pranata, Bayu Satria Wiratama and Made Ary Sarasmita in SAGE Open Nursing
Footnotes
Acknowledgments
We extend our sincere gratitude to the frontline nurses who participated in this study, contributing their valuable experiences. We also acknowledge the Universitas Riau Indonesia and the University of Health Sciences and Pharmacy in St Louis for providing essential funding support that made this research possible.
Ethical Approval and Informed Consent Statements
Ethical approval was obtained from the Ethics Committee of the Nursing Faculty, Universitas Riau, Indonesia (No: 68/UN.19.5.1.8/KEPK.FKP/2023). All participants provided informed consent before taking part in the study. The research was conducted in accordance with the Declaration of Helsinki and adhered to all ethical guidelines for human subjects research.
Author Contributions
Conceptualization: Huda N., Shaw M.K., and Gautama M.S.N.; Data curation: Huda N., Sarasmita M.A. and Pranata S.; Formal analysis: Huda N. Funding acquisition: None.; Methodology: Huda N. and Shaw M.K.; Project administration: Huda N.; Visualization: Wiratama B.S. and Pranata S.; Writing–original draft: Huda N., Wiratama B.S., Sarasmita M.A., and Gautama M.S.N. ; Writing–review and editing: Huda N., Shaw M.K. and Gautama M.S.N.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Institute of Research and Community Service/Lembaga Penelitian dan Pengabdian Masyarakat (LPPM) Universitas Riau, Indonesia through Dana DIPA Universitas Riau PIU ADB AKSI International Collaborative scheme 2023 No: 8333/ UN19.5.1.3/PT.01.03/2023.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The dataset used in this study is available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.