
Abstract
Introduction
Insecure attachment styles among people with schizophrenia may exacerbate psychiatric symptoms and emotional distress, complicating recovery.
Objectives
This study aimed to assess attachment styles among individuals with schizophrenia and explore their relationship to symptomatology and emotional distress.
Methods
A cross-sectional descriptive correlational design was employed, involving 220 patients diagnosed with schizophrenia. Participants were assessed using the Psychosis Attachment Measure (PAM) to determine attachment styles, the Robertson Emotional Distress Scale (REDS) to evaluate emotional distress, and the Positive and Negative Syndrome Scale (PANSS) to assess psychiatric symptoms.
Results
The study found that 72.5% of participants exhibited high levels of avoidant attachment, while 61.7% displayed significant anxious attachment tendencies. Emotional distress was prevalent, with a mean REDS score of 43.48 ± 3.54, indicating high emotional distress levels. Positive correlations were identified between emotional distress and both avoidant (r = .378, p = .008) and anxious attachment (r = .644, p < .01). Additionally, psychiatric symptoms correlated positively with avoidant (r = .434, p = .018) and anxious attachment (r = .474, p < .01). Multiple regression analysis indicated that anxious attachment was a stronger predictor of psychiatric symptoms (B = 0.72, p < .001) and emotional distress (B = 0.82, p < .001) compared to avoidant attachment.
Conclusion
This study highlights the relationship between attachment styles, emotional distress, and psychiatric symptoms in schizophrenia. Participants exhibited avoidant and anxious attachment, linked to heightened emotional distress and severe symptoms. Avoidant attachment was characterized by emotional withdrawal and self-reliance, while anxious attachment involved dependency and relational anxiety. These insecure patterns predicted the severity of psychiatric symptoms, emotional distress, and anxious attachment. The findings emphasize the importance of addressing attachment dynamics in therapeutic nursing for schizophrenia, as these factors may worsen symptoms and emotional challenges. Using attachment-focused approaches can enable mental health nurses to better support symptom management and enhance well-being.
Introduction
Schizophrenia is a complex mental health disorder that significantly disrupts an individual's cognitive processes, emotional regulation, decision-making, and ability to form meaningful relationships. This chronic condition affects about 1% of the American population, usually developing during late adolescence to early adulthood in men and the late twenties to early thirties in women, with rare diagnoses before age 12 or after 40. The prevalence of schizophrenia in Egypt is estimated to be around 1.1% of the population, based on data from the Egyptian National Institute of Mental Health (Manea et al., 2020). Symptoms of schizophrenia are generally divided into three main categories: positive symptoms, negative symptoms, and cognitive symptoms.
The disorder presents with various symptoms grouped into positive, negative, and cognitive domains, which together impair functioning and quality of life (McCutcheon et al., 2020; Taha et al., 2025a, 2025b). Positive symptoms include hallucinations, delusions, disorganized speech, disorganized behavior, and catatonia. Conversely, negative symptoms involve a decrease in the brain's ability to process experiences and respond appropriately, resulting in flat affect, reduced motivation, difficulty reaching goals, slower responses, alogia, apathy, and anhedonia (El-Ashry et al., 2023; Hany et al., 2021). Cognitive symptoms can range in severity, appearing as attention deficits and impairments in reasoning, memory, and decision-making caused by dysfunction in brain regions responsible for these cognitive functions.
Review of Literature
Attachment styles are rooted in John Bowlby's attachment theory, which outlines how individuals engage in intimate relationships with key figures, such as parents, children, and romantic partners (Bretherton, 2013). These styles are classified as secure or insecure, with the latter providing a framework for understanding the development of schizophrenia-spectrum phenomena (Barbeito et al., 2024). Insecure attachment may serve as a target for preventive interventions, as it can elevate the risk of psychosis, especially in adverse developmental contexts (Lavin et al., 2020).
Research indicates that insecure attachment is frequently associated with schizophrenia; individuals who are less comfortable with intimacy may experience more severe symptoms. Insecure attachment styles have been linked to treatment outcomes and the severity of schizophrenia symptoms (Helyel & El-Sayed, 2025). Additionally, these styles may influence subjective recovery domains, such as self-esteem, independently of symptom severity. Clinical theories propose that attachment insecurity underpins difficulties in interpersonal functioning, and individuals with schizophrenia exhibit higher levels of insecure attachment (França et al., 2020; Helyel & El-Sayed, 2025).
The dimensions of attachment styles include avoidant and anxious attachment (Ferriby et al., 2015). Patients with avoidant attachment may resist seeking help, reinforcing negative perceptions of others, and struggling with trust and intimacy. These individuals often downplay their distress and are reluctant to seek assistance (Partridge et al., 2022). Conversely, anxious attachment has been associated with increased severity of positive and affective symptoms, with both attachment styles linked to hallucinations and feelings of persecution. However, avoidant attachment shows a weaker connection to negative symptom scores (Lavin et al., 2020). Emotional distress, characterized by symptoms such as anxiety, depression, irritability, and agitation, is prevalent among individuals with schizophrenia. It frequently manifests as depression (loss of interest, sadness) and anxiety (restlessness, tension; Riehle et al., 2024).
In the context of Egypt, unique sociocultural factors may further influence attachment styles and emotional distress. Cultural norms regarding family dynamics, stigma surrounding mental health, and varying levels of social support can significantly impact how individuals with schizophrenia experience and express their emotional and psychological challenges (Khedr et al., 2024; Merhej, 2019; Taha et al., 2025a, 2025b). Establishing a therapeutic rapport with individuals diagnosed with schizophrenia is a persistent challenge for psychiatric nurses, who must work collaboratively with families and communities throughout the varying stages of the disorder (El-Ashry et al., 2024). Psychiatric nurses play a crucial role in delivering effective treatment and care (El-Sayed et al., 2023; Kumar et al., 2020). By assessing attachment styles and emotional distress levels in patients, nurses can gain insights into behaviors, particularly those exhibiting avoidant traits like hostility and low self-disclosure. Helping patients develop techniques for emotional regulation is vital, especially since increased anxiety can lead to more threatening interpretations of their experiences (Maalouf et al., 2022).
Educating patients and their families about effective coping strategies can help manage factors that exacerbate schizophrenia symptoms, such as insecure attachment, family dynamics, and emotional distress (Saroca & Sargent, 2022). Establishing programs to enhance social problem-solving skills can improve understanding of daily challenges (Lee et al., 2018). Support from family and friends can act as a buffer against stress, enhancing social functioning and overall quality of life. Cognitive-behavioral therapy (CBT) has proven effective in addressing early signs of relapse and can alleviate emotional distress while promoting well-being (Nakao et al., 2021).
This study is significant as it explores the intricate relationship between attachment styles and psychiatric symptoms in individuals with schizophrenia. By focusing on this specific population, the research aims to uncover how different attachment patterns may influence the severity and experience of psychotic symptoms. Understanding these dynamics can provide valuable insights into the psychosocial factors that contribute to the disorder, potentially informing more personalized therapeutic approaches (Volkan, 2020).
Moreover, there is a notable gap in the literature regarding the specific impact of attachment styles on emotional distress and psychiatric symptoms among Egyptian patients with schizophrenia. The association between attachment insecurity and the severity of psychotic and affective symptoms, along with related emotional distress, indicates that these factors may predict the severity of psychotic features in the disorder. This descriptive correlational study aims to assess attachment styles among individuals with schizophrenia and explore their relationship to symptomatology and emotional distress, ultimately evaluating how these attachment styles relate to the overall experience of schizophrenia. By identifying the relationships between attachment styles, emotional distress, and psychiatric symptoms, nurses can better assess the psychological needs of their patients. This knowledge is crucial for developing tailored interventions that address emotional and relational dynamics, often overlooked in traditional treatment approaches. Furthermore, by recognizing the impact of insecure attachment on symptom severity and treatment response, psychiatric nurses can foster therapeutic relationships that promote trust and engagement, essential components of adequate care. Implementing strategies that enhance emotional regulation and coping mechanisms can empower patients to manage their symptoms more effectively.
Research Objectives
Determine the attachment styles among patients with schizophrenia.
Assess psychiatric symptoms among patients with schizophrenia.
Determine emotional distress levels among patients with schizophrenia.
Investigate the relationship between attachment styles, psychiatric symptoms, and emotional distress among patients with schizophrenia.
Methods
Research Design and Setting
A cross-sectional, descriptive, correlational design, following the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist guidelines, was employed in this study. The study was conducted in the inpatient psychiatric units of the Port-Said Psychiatric Health Hospital, which is operated under Egypt's Ministry of Health, General Secretariat of Mental Health and Addiction Treatment (GSMHAT). The hospital offers both inpatient and outpatient services, including diagnosis, medication management, psychotherapy, supervision, and follow-up care. The facility has a total capacity of 110 beds and consists of two male and two female psychiatric units, where patients with severe mental disorders, including schizophrenia, receive treatment. Data collection was conducted specifically within these inpatient units during patients’ admission and treatment periods.
Research Questions
RQ1. What are the dominant attachment styles among patients with schizophrenia?
RQ2. What are the common psychiatric symptoms among patients with schizophrenia?
RQ3. What are the levels of emotional distress among patients with schizophrenia?
RQ4. What is the relationship between attachment styles, psychiatric symptoms, and emotional distress among patients with schizophrenia?
Study Population
Sample Size Estimation
The estimate was calculated using the following equation. The formula used for the calculation was =
Sampling and Recruitment
Participants were recruited using a non-probability convenience sampling method from inpatient psychiatric units. All admitted patients during the study who met the eligibility criteria were approached consecutively to improve representativeness and minimize selection bias. The eligibility criteria included a confirmed diagnosis of schizophrenia for at least 6 months, as per the DSM-5 (APA, 2013), verified through medical records, an age of 18 or older, and stable cognitive ability to understand and consent to the study procedures.
Specific exclusion criteria were applied to maintain internal validity and minimize confounding factors. Patients were excluded if they had comorbid physical disorders, substance use disorders, stupor, agitation, or organic brain conditions that could impair their ability to participate reliably or provide informed consent. Continuous clinical evaluations ensured that participants were in a stable mental state suitable for inclusion.
Recruitment began in August 2024 and extended through February 2025. Of the 235 patients initially invited, six were excluded because they did not meet the inclusion criteria. Five patients declined participation, and four withdrew before completing assessments. Ultimately, 220 patients completed the study, and their data were included in the analysis.
Measurements of Interest
Demographic Characteristics Data Sheet
Data on patients’ personal and clinical characteristics were gathered, encompassing variables such as gender, age, place of residence, educational attainment, marital status, occupation, living conditions, family history of psychiatric disorders, duration of illness, number of prior psychiatric hospitalizations, and age at onset of schizophrenia.
Psychosis Attachment Measure (PAM)
The PAM evaluates adult attachment styles by examining conscious feelings, thoughts, and behaviors in intimate relationships. It offers insightful indicators of attachment dynamics in adulthood. PAM was developed by Crowell et al., and it was translated into Arabic and validated by Abd El-Hamed (2014). The PAM evaluates attachment in psychotic patients by focusing on two dimensions: “anxious” and “avoidance.” It consists of 16 items, with eight items dedicated to assessing avoidance (e.g., “I prefer not to let other people know my true thoughts and feelings”) and eight items aimed at measuring anxiety (e.g., “I tend to get upset, anxious, or angry if other people are not there when I need them”). Participants assess the degree to which each item applies to them using a 4-point scale that ranges from not at all to very much. Total scores for each dimension are derived by averaging the individual item scores, with higher scores signifying increased levels of anxiety and avoidance. Each dimension's score ranges from 8 to 32, with scores categorized as low (8 to ≤16), intermediate (16 to ≤24), or high (24 to 32). A high overall total score denotes a generally insecure attachment style, while a lower score indicates a secure attachment. The Arabic version of the scale was validated among patients with schizophrenia, yielding Cronbach's alpha values of .83 for the anxiety dimension and .81 for the avoidance dimension (Abd El Hamed, 2014). These results indicate that the PAM is a reliable instrument, and this Arabic version was utilized in the current study.
Robertson Emotional Distress Scale (REDS)
The REDS is a self-assessment questionnaire designed to evaluate emotional distress by asking respondents to rate the applicability of 10 statements regarding their experiences over the past 4 weeks. Participants respond using a 6-point Likert scale, ranging from strongly disagree (0) to strongly agree (5). The scores for each statement are summed to produce an overall emotional distress score, with higher scores indicating greater levels of distress. The total score can range from 0 to 50 and is categorized as follows: normal (0–20), mild (21–30), moderate (31–40), and severe (41–50; Robertson, 2013). The scale has demonstrated robust psychometric properties, exhibiting a validity coefficient of .74 and a reliability coefficient of .89. The scale was translated into Arabic by two independent bilingual experts fluent in both English and Arabic to ensure linguistic and conceptual equivalence. Afterwards, a different pair of bilingual experts performed a back-translation from Arabic to English. Any discrepancies between the original and back-translated versions were reviewed and resolved by a panel of five subject matter experts, who confirmed the semantic accuracy and cultural relevance of the Arabic version. Then, the content validity of the 10 REDS items was evaluated by these five experts, with item-level content validity indices ranging from 0.67 to 0.82, resulting in an overall content validity index of 0.8, indicating satisfactory content validity. The internal consistency reliability of the Arabic version was assessed using Cronbach's alpha, yielding an acceptable coefficient of α = .85, demonstrating good reliability for the scale in this context.
Positive and Negative Syndrome Scale (PANSS)
The PANSS is utilized to evaluate a broad spectrum of psychiatric symptoms, specifically in patients with schizophrenia. It is structured into three subscales: the Positive Symptoms Scale, which consists of seven items that assess symptoms such as delusions, hallucinations, and hostility; the Negative Symptoms Scale, also comprising seven items that evaluate aspects like blunted affect, emotional withdrawal, and stereotyped thinking; and the General Psychopathology Scale, which includes 16 items addressing symptoms such as somatic concerns, poor attention, and lack of judgment (Kay et al., 1987). The PANSS encompasses 30 items, each with precise definitions and detailed anchoring criteria for all seven rating points. Each item is rated on a Likert scale from 1 (absent) to 7 (extreme), allowing for a nuanced assessment of symptom severity. The overall PANSS score is categorized into three levels: mild (scores less than 138), moderate (scores between 138 and 165), and severe (scores exceeding 165; Yehya et al., 2016). The Arabic version of the PANSS was validated in a study involving patients with schizophrenia, achieving a Cronbach's alpha value of .91 (Yehya et al., 2016). These findings indicate that the PANSS is a reliable measurement tool, and this Arabic version was employed in the present study.
Procedure
Ethical Considerations
This study was conducted in strict accordance with the ethical principles of the Declaration of Helsinki (DoH, October 2008). Ethical approval was obtained from the Research Ethics Committee (REC) at Port Said University's College of Nursing
Validity of the Measurement
The study utilized validated Arabic versions of PAM and PANSS. Bilingual researchers translated the REDS through forward and backward translation to ensure accuracy. Content validity was evaluated using the Content Validity Index to verify the structural integrity and alignment of the translated scale with the original. A panel of five expert academic professionals in psychiatric and mental health nursing assessed the instruments for face validity, focusing on the appropriateness, relevance, and clarity of the items for the target population. The experts confirmed that the items were culturally suitable, accurate, and easily understandable. Additionally, the scales’ reliability was tested using Cronbach's alpha, which indicated satisfactory internal consistency.
Pilot Study
A pilot study was conducted with 10% of the study participants (20 patients) to evaluate the research instruments before initiating data collection. The pilot study's objectives included assessing the clarity, applicability, and feasibility of the tools, as well as estimating the time required for participants to complete them. It also aimed to identify potential obstacles or issues hindering data collection. Based on the findings from the pilot study, several modifications were made to the instruments; consequently, the patients involved in the pilot were excluded from the primary study sample.
Data Collection
This study collected demographic and clinical data from patients with schizophrenia using a specialized data sheet. Participants were approached in the hospital setting, where trained researchers provided them with information about the study. They received a detailed explanation of the study's goals, procedures, and the significance of their participation. Each patient was assured that their responses would remain confidential and anonymous. Information was collected through an in-depth review of their medical histories. The data collection involved one-on-one interviews lasting approximately 25–30 min, conducted in a quiet, comfortable, and private room within the hospital unit. To ensure comprehensive coverage of all measures, participants completed two to three interviews on scheduled follow-up days. Informed consent was obtained from all participants, emphasizing that their involvement was entirely voluntary, with no coercion from the interviewer and no incentives offered.
Statistical Analysis
The data were input into the computer and analyzed using the IBM SPSS software package Version 25.0. The normality of distribution was verified using the Kolmogorov–Smirnov test. Descriptive statistics, including means, standard deviations, and frequencies, were calculated to summarize demographic and clinical characteristics. Pearson correlation coefficients were employed to examine the strength and direction of relationships between attachment styles, emotional distress, and psychiatric symptoms. Multiple regression analysis was utilized to determine the predictive power of attachment styles on psychiatric symptoms and emotional distress, with R2 values indicating the proportion of variance explained by the model. Additionally, ANOVA was conducted to assess the differences in psychiatric symptoms and emotional distress across various demographic groups. Significance levels were set at p < .05 and p < .01 to assess the statistical significance of the findings. All analyses were performed using appropriate statistical software, ensuring a robust examination of the data.
Results
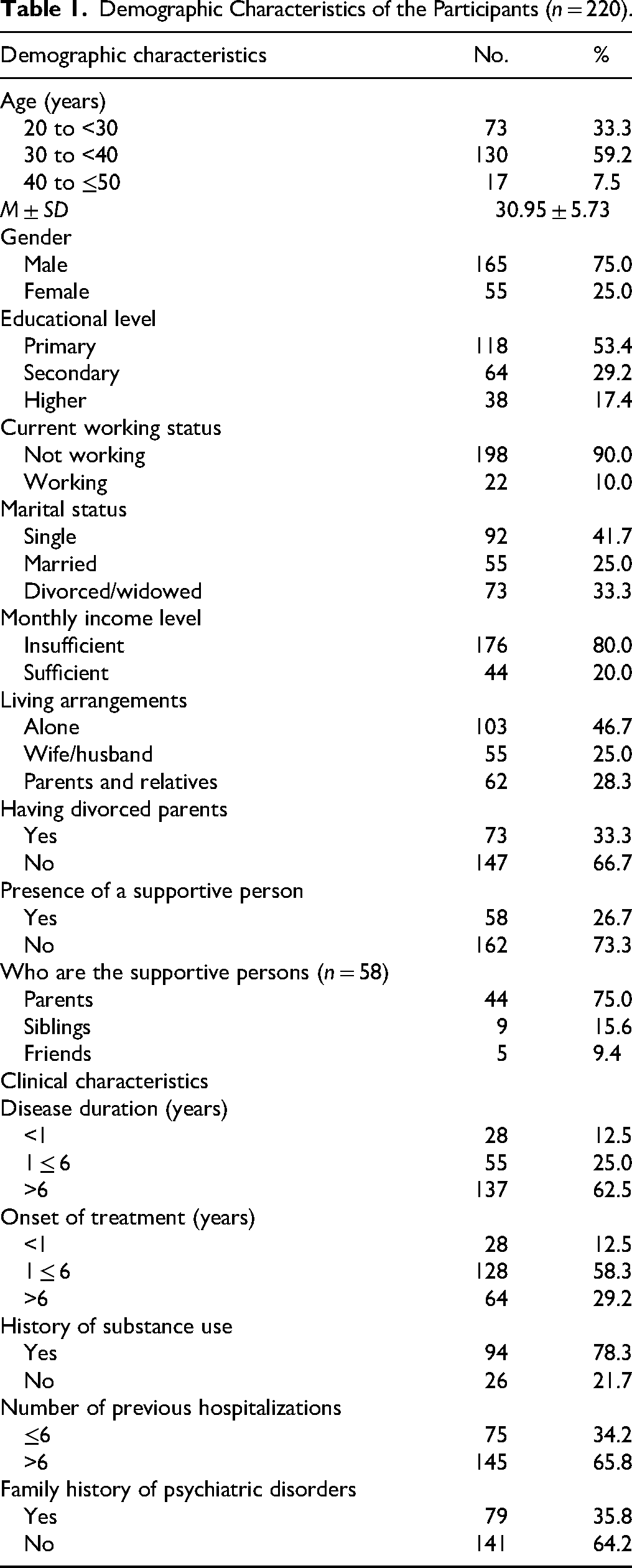
Most participants (59.2%) and 75% were males. Over half (53.4%) had primary education, and only 17.5% had higher education. Most (90%) were not working, and 80% reported insufficient monthly income. Regarding marital status, 41.7% were single, 25% married, and 33.3% were divorced or widowed. Regarding family dynamics, 33.3% had divorced parents, as opposed to 66.7% who did not. Among those with support (n = 58), 75% relied on parents, 15.6% on siblings, and 9.4% on friends. Clinical characteristics revealed that 62.5% of patients were diagnosed more than 6 years ago, and 58.3% started treatment within 1–6 years. Substance use history was reported by 78.3%, while 21.7% did not. Regarding hospitalizations, 65.8% had over six hospitalizations. Lastly, 35.8% reported a family history of psychiatric disorders, while 64.2% did not, as shown in Table 1.
Demographic Characteristics of the Participants (n = 220).
The distribution of attachment styles revealed a high prevalence of insecurity. Anxious attachment was the most common style, present in 74.2% of participants, followed by high avoidant attachment in 53.3% (Figure 1). The mean scores on the PAM subscales were 24.20 (SD = 3.40) for avoidance and 25.60 (SD = 4.73) for anxiety, confirming high levels of both insecure attachment styles (Table 2).

Frequency of Attachment Styles Among the Participants (n = 220).
The Mean Scores of the Participants on PAM and REDS (n = 220).

Note. PAM = Psychosis Attachment Measure; REDS = Robertson Emotional Distress Scale.
Participants reported severe levels of emotional distress, with a mean score on the REDS was 43.48 (SD = 3.54), as shown in Table 2. This was further evidenced by the finding that 90.0% of the sample was categorized within the severe distress range (Figure 2).

Frequency of Emotional Distress Among the Participants (n = 220).
The overwhelming majority, 90.0%, experienced severe emotional distress, indicating a high prevalence of psychological strain within the sample. In contrast, only 7.5% of participants reported moderate emotional distress, and a minimal 2.5% experienced mild emotional distress, as illustrated in Figure 2.
The distribution of PANSS levels among the participants showed that most were in the moderate symptom range (62.5%), followed by the severe range (32.5%), as illustrated in Figure 3. Furthermore, Table 3 shows the distribution of participants across various severity levels on the PANSS. For positive symptoms, delusions were mild in 29.2%, moderate in 34.2%, and severe in 36.7%. Hallucinatory behavior was primarily severe in 54.2%. Excitement was mostly moderate (51.7%) and severe (36.7%). Grandiosity and suspiciousness/persecution symptoms were evenly distributed, with approximately 40% of cases at moderate and severe levels. Hostility levels mostly ranged from moderate to severe, with 46.7% classified as moderate and 48.3% as severe. Regarding negative symptoms, blunted affect and emotional withdrawal were mostly severe, seen in over 80% of cases. Poor rapport and passive or apathetic social withdrawal were also mostly in the moderate to severe range, with each having nearly or exceeding 80% combined scores. For general symptoms, anxiety was 100% classified as severe. Unusual thought content was distributed with 43.3% severe, 30% moderate, and 26.7% mild. Lack of judgment and insight, as well as disturbance of volition, were mostly severe, at 85.8% and 73.3%, respectively. Preoccupation was predominantly moderate (49.2%), and active social avoidance was primarily severe (83.3%).

Frequency of Emotional Distress Among the Participants (n = 220).
Distribution of Participants on the PANSS (n = 220).

Note. Severity classification: mild (scores less than 138), moderate (scores between 138 and 165), and severe (scores exceeding 165). PANSS = Positive and Negative Syndrome Scale.
Significant positive correlations were found between emotional distress and avoidance (r = .378, p = .008) and anxious attachment styles (r = .644, p < .01). In addition, substantial positive correlations were observed between psychiatric symptoms and avoidant attachment (r = .434, p = .018) and anxious attachment styles (r = .474, p < .01), highlighting that insecure attachment patterns are associated with more severe psychiatric symptoms. Furthermore, a significant correlation was found between emotional distress and psychiatric symptoms (r = .233, p = .008), suggesting that emotional distress may play a role in the severity of psychiatric symptoms, as shown in Table 4.
Correlation Coefficients Among the Attachment Styles, Emotional Distress, and Psychiatric Symptoms of Schizophrenia of the Participants (n = 220).

Note. PANSS = Positive and Negative Syndrome Scale; REDS = Robertson Emotional Distress Scale; r = Pearson correlation.
*p ≤ .05. **p < .01.
Multiple regression analysis revealed that both anxious and avoidant attachment styles significantly predicted psychiatric symptoms and emotional distress in individuals with schizophrenia. In predicting psychiatric symptoms, anxious attachment showed a stronger association (B = 0.72, β = .35, p < .001) compared to avoidant attachment (B = 0.51, β = .30, p = .006), with the model explaining 35% of the variance (R2 = .35, adjusted R2 = .33, F(2, 117) = 16.78, p < .001). Similarly, for emotional distress, anxious attachment had a more substantial predictive effect (B = 0.82, β = .42, p < .001) than avoidant attachment (B = 0.45, β = .29, p = .002), accounting for 41% of the variance (R2 = .41, adjusted R2 = .39, F(2, 117) = 20.45, p < .001), as displayed in Table 5.
Multiple Regression Analysis of Attachment Styles on Psychiatric Symptoms and Emotional Distress (n = 220).

Note. B = unstandardized coefficient; SE = standard error; β = standardized coefficient; PANSS = Positive and Negative Syndrome Scale; REDS = Robertson Emotional Distress Scale; F = ANOVA test, t-test of significance.
**p < .01.
Discussion
The relationship between attachment styles and mental health has garnered increasing attention in psychological research, particularly concerning its implications for individuals with schizophrenia. Attachment theory posits that early relationships with caregivers shape individuals’ emotional and interpersonal functioning (Mikulincer & Shaver, 2018). In the context of schizophrenia, insecure attachment styles may exacerbate psychiatric symptoms and emotional distress, complicating recovery and overall quality of life. This study aims to assess attachment styles among individuals with schizophrenia and explore their relationship to symptomatology and emotional distress, ultimately evaluating how these attachment styles relate to the overall experience of schizophrenia.
The current findings reveal significant trends in how individuals with schizophrenia relate to others and manage their emotional needs, which can profoundly impact their recovery and overall mental health. The avoidance style subscale indicates a strong tendency among participants to withdraw emotionally from others. A notable majority preferred not to share their true thoughts and feelings, which may be influenced not only by their attachment styles but also by the stigma associated with their diagnosis.
In Egypt, cultural norms surrounding family dynamics and the stigma attached to mental health issues can significantly shape these attachment styles (Shlapy, 2022). Families often prioritize collective harmony and may discourage open discussions about mental health, leading individuals to internalize their struggles and avoid seeking help. This cultural context can exacerbate feelings of isolation and hinder the development of supportive relationships, which are crucial for recovery (Merhej, 2019).
This reluctance to engage in vulnerability could stem from a fear of judgment or misunderstanding, aligning with existing literature that highlights how individuals with avoidant attachment styles often prioritize self-reliance and emotional distance as coping mechanisms in stressful situations. Such tendencies can hinder the development of supportive relationships, which are essential for recovery in mental health contexts. Understanding these dynamics is crucial for tailoring interventions that address both attachment patterns and the impact of stigma, ultimately enhancing recovery outcomes (Arriaga et al., 2018).
Moreover, the data show that many participants find it challenging to accept help from others, reinforcing the notion that avoidant individuals may struggle with dependency and support-seeking behaviors. This reluctance can lead to increased feelings of isolation and exacerbate mental health issues, as social support is a critical component of effective coping strategies (Hellström et al., 2019). The preference for solitude during stressful times further underscores the avoidance trend, indicating that these individuals may prioritize self-isolation over seeking comfort from others, which can be detrimental to their emotional well-being.
In contrast, the anxious style subscale reveals a high level of relational anxiety among participants. Many expressed significant distress when separated from others, indicating a strong emotional dependency. This dependency can lead to heightened anxiety and fear of abandonment, which are common characteristics of anxious attachment styles. The findings suggest that individuals with anxious attachment may experience increased emotional distress when they perceive a lack of support or approval from others, which can complicate their recovery process (Roesel et al., 2024).
The concern about being liked and the discomfort felt when others seek to know them better further illustrate the complexities of their interpersonal relationships. Such feelings can create barriers to forming healthy connections, as individuals may oscillate between seeking closeness and fearing rejection. This dynamic can lead to a cycle of anxiety and avoidance, making it challenging for these individuals to engage in meaningful relationships that are essential for their recovery.
Furthermore, the current findings demonstrate the high level of emotional distress among participants, emphasizing significant anxiety, depression, irritability, and other psychological issues. A substantial portion of participants reported feelings of anxiety and depression, with many also expressing irritability or anger. While existing literature emphasizes the prevalence of emotional distress among individuals facing various life challenges (Dasa et al., 2024). This study specifically sheds light on how these emotional struggles manifest uniquely in the lives of people with schizophrenia. By linking emotional distress to attachment styles and relational dynamics, our findings provide a deeper understanding of the psychological landscape of this population. This insight is crucial for developing targeted interventions that address not only the symptoms of emotional distress but also the underlying relational factors that contribute to it. Thus, this paper makes a significant contribution to the field by highlighting the complex interplay between attachment, emotional distress, and recovery in individuals with schizophrenia.
The finding that many participants no longer find pleasure in activities they once enjoyed is particularly concerning. This symptom, often referred to as anhedonia, is a hallmark of depressive disorders and can severely impact an individual's quality of life and motivation to engage in social or recreational activities (Kleinman et al., 2012). The high percentage of participants reporting low self-esteem and self-confidence further underscores the pervasive nature of emotional distress, which can contribute to a cycle of negative self-perception and increased psychological vulnerability (Dvořáková et al., 2024).
Physical symptoms of distress, such as tension, agitation, and fatigue, were also prevalent among participants. These physical manifestations are often intertwined with emotional distress, as chronic stress can lead to somatic symptoms that exacerbate feelings of anxiety and depression. The significant number of participants reporting difficulties with concentration and sleep disturbances highlights the cognitive and physiological toll of emotional distress, which can hinder daily functioning and overall well-being.
The prevalence of positive symptoms, particularly delusions and hallucinatory behavior, indicates a substantial burden of psychotic experiences among participants. Delusions, characterized by false beliefs, were reported at varying severity levels, with a notable proportion experiencing them as highly severe. This aligns with existing literature that emphasizes the central role of delusions in the clinical presentation of schizophrenia, often correlating with poorer outcomes and increased treatment resistance (Fountoulakis et al., 2019).
Conceptual disorganization emerged as a prominent symptom, with most participants reporting moderate to severe levels of this symptom. This symptom is critical as it can significantly impair cognitive functioning and daily living activities, highlighting the need for targeted interventions. The high prevalence of hallucinatory behavior further underscores the complexity of schizophrenia, as auditory and visual hallucinations can profoundly affect an individual's reality and functioning (Baandrup et al., 2022). Furthermore, negative symptoms, such as blunted affect and emotional withdrawal, were also prevalent, indicating that these aspects of schizophrenia are often underrecognized yet significantly impact patients’ quality of life. The severity of negative symptoms can lead to social withdrawal and difficulties in interpersonal relationships, which are crucial for recovery and rehabilitation (Baandrup et al., 2022; Hieronymus et al., 2023).
The current findings indicate that both avoidant and anxious attachment styles are positively correlated with emotional distress. This suggests that individuals with insecure attachment patterns may experience higher levels of emotional distress, which aligns with attachment theory, positing that insecure attachments can lead to difficulties in emotional regulation and increased vulnerability to distress (Partridge et al., 2022). Moreover, the substantial correlations between attachment styles and psychiatric symptoms underscore the impact of attachment on the severity of psychotic experiences. Specifically, individuals exhibiting avoidant and anxious attachment styles tend to report more severe psychiatric symptoms. This is consistent with previous research indicating that insecure attachment is associated with poorer mental health outcomes, including increased psychotic symptoms and difficulties in interpersonal relationships (van Bussel et al., 2023). The presence of these attachment styles may hinder effective coping mechanisms, leading to exacerbated symptoms in individuals with schizophrenia.
Incorporating educational programs aimed at preventing the exacerbation of insecure attachment represents a promising avenue for enhancing clinical practice in the treatment of schizophrenia. These programs can provide patients and their families with essential knowledge about attachment dynamics and emotional regulation. Research has shown that understanding attachment styles can significantly improve emotional responses and interpersonal relationships (Sagone et al., 2023). By fostering an understanding of how insecure attachment influences mental health, participants can learn effective coping strategies and communication skills.
Additionally, the correlation between emotional distress and psychiatric symptoms suggests that emotional distress is closely linked to the severity of psychiatric symptoms. This finding highlights the importance of addressing emotional distress in therapeutic settings, as it may contribute to the overall symptomatology of schizophrenia. Recent studies have emphasized the need for integrated treatment approaches that consider both attachment styles and emotional distress to improve recovery outcomes for individuals with psychotic disorders (Partridge et al., 2022; Van Bussel et al., 2021).
The regression analysis of the current study reveals that both anxious and avoidant attachment styles significantly contribute to the severity of psychiatric symptoms as measured by PANSS and emotional distress as assessed by REDS. In the context of psychiatric symptoms, anxious attachment was found to be more strongly associated with higher severity of symptoms compared to avoidant attachment. This indicates that individuals with elevated levels of anxious attachment may be more likely to experience more severe psychiatric symptoms. However, it is essential to note that this association does not imply causation, given the study's cross-sectional nature. This aligns with existing literature that highlights the detrimental effects of insecure attachment styles on mental health outcomes, particularly in populations with psychotic disorders (Sood et al., 2022). Anxious attachment is characterized by a heightened sensitivity to rejection and a preoccupation with relationships, which can exacerbate feelings of distress and lead to more pronounced psychiatric symptoms (Shen et al., 2021).
Similarly, the analysis indicates that both attachment styles significantly predict emotional distress, with anxious attachment again showing a more substantial effect. This reinforces the notion that emotional distress is closely linked to attachment patterns, as individuals with insecure attachments may struggle with emotional regulation and coping strategies (Eilert & Buchheim, 2023). The significant variance explained by the models (41% for emotional distress) underscores the importance of considering attachment styles in understanding the emotional experiences of individuals with schizophrenia.
Strengths and Limitations
While this study provides valuable insights into the relationships between attachment styles, emotional distress, and psychiatric symptoms in schizophrenia, several limitations must be acknowledged. First, the cross-sectional design restricts our ability to infer causality between the studied variables. Second, key potential confounding variables were not controlled for. The current medication regimens of participants (including type, dosage, and duration) were not recorded. Given that psychotropic medications can substantially influence both symptom severity and emotional states, this omission is a significant limitation that may confound the observed relationships. Similarly, while a history of substance use was reported by a high proportion of participants, a factor known to independently impact attachment security and psychiatric presentation, it was not statistically controlled for in our analyses. Third, the potential influence of psychotherapy was not assessed. The presence, type, frequency, and quality of ongoing or previous psychotherapy could significantly shape attachment patterns and levels of emotional distress. The absence of these data is a limitation, as therapeutic interventions are a core component of treatment and may modify the variables of interest. Finally, the reliance on self-reported measures for attachment and emotional distress, while using validated tools, may be subject to response biases. Future research would benefit from supplementing self-reports with clinician-administered assessments and behavioral observations. We recommend that future studies employ longitudinal designs to establish temporal precedence and causality. Furthermore, systematically controlling for medication variables, substance use history, and psychotherapy exposure would provide a more precise understanding of the unique contributions of attachment styles to symptomatology and distress.
Implications for Practice
The findings of this study hold important implications for clinical practice, particularly in the treatment of individuals with schizophrenia. The strong association between insecure attachment styles, especially anxious attachment, and heightened psychiatric symptoms underscores the need for targeted interventions that address relational and emotional vulnerabilities. Incorporating attachment-focused therapies, such as mentalization-based therapy (MBT) or attachment-informed CBT, can help patients develop healthier emotional regulation strategies and improve interpersonal functioning. For instance, MBT can be integrated into nursing care by encouraging reflective dialogue and fostering a deeper understanding of mental states, which may reduce distress and enhance reality testing. Building secure therapeutic relationships should be a priority for mental health professionals, as trust and emotional safety are foundational for effective treatment. Routine assessment of attachment styles in clinical settings can help identify patients at higher risk for emotional distress, allowing for early, personalized interventions. Additionally, psychoeducation programs for patients and families should emphasize coping strategies for managing insecure attachment dynamics, such as improving communication skills and reducing relational anxiety. Social problem-solving training and family support initiatives can further reinforce these efforts, creating a more stable and supportive environment for recovery and long-term success. By addressing attachment-related challenges alongside traditional symptom management, clinicians can promote more holistic and sustainable outcomes for individuals with schizophrenia.
Conclusion
The findings of this study emphasize the significant interplay between attachment styles, emotional distress, and psychiatric symptoms in individuals with schizophrenia. Participants exhibited marked tendencies toward avoidant and anxious attachment, which were strongly correlated with increased emotional distress and more severe psychiatric symptoms. Avoidant attachment was characterized by emotional withdrawal and self-reliance, while anxious attachment indicated emotional dependency and relational anxiety. These insecure attachment patterns were predictive of both psychiatric symptom severity and emotional distress, with anxious attachment demonstrating a strong association.
Supplemental Material
sj-docx-1-son-10.1177_23779608251383584 - Supplemental material for How Attachment Styles Influence Emotional Distress and Psychiatric Symptoms Among Individuals With Schizophrenia: A Cross-Sectional Nursing Survey
Supplemental material, sj-docx-1-son-10.1177_23779608251383584 for How Attachment Styles Influence Emotional Distress and Psychiatric Symptoms Among Individuals With Schizophrenia: A Cross-Sectional Nursing Survey by Huda Gaber Hamzaa, Mona Metwally El-Sayed, Mahmoud Abdelwahab Khedr, Amal Sobhy Mahmoud, Loujain Sharif, Alaa Mahsoon, Khalid Sharif and Samar Atiya Abo-Saleh Gabal in SAGE Open Nursing
Footnotes
Acknowledgments
The authors are grateful to the patients who took part in this study.
Ethical Approval
The study adhered to the principles and standards of the Declaration of Helsinki (DoH, October 2008). The Faculty of Nursing Research Ethics Committee (REC) at Port Said University (Reference Number: NUR:5/11/2023) approved data collection.
Informed Consent
Participants were required to fill out an informed consent form, which detailed the research and evaluated their understanding. They were told their participation was voluntary and they could withdraw their consent without any adverse effects. Robust measures were established to safeguard the privacy and confidentiality of the collected data.
Author Contributions
HGH, MME, and MAK: conceptualization, methodology, original draft preparation, and reviewing and editing. ASM and LS: visualization and supervision. AM and SAAG: investigation and analysis. KS and SAAG: validation, formal analysis, and reviewing and editing. All the authors reviewed the final draft of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The datasets utilized or analyzed in this study are available from the corresponding author upon request.
Use of AI Software
The authors declare not using AI in writing this manuscript.
Supplemental Material
Supplemental material for this paper is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.