
Abstract
Introduction
Caring for patients who have schizophrenia in tidal floods requires more effort than patients who have schizophrenia in non-tidal flood areas. Family caregivers are required to manage stress and burden through adaptation to roles and the environment.
Objective
The purpose of this study was to explore the meaning of family adaptation experiences of those who care for patients with schizophrenia in a tidal flood area.
Methods
This research is a qualitative research with a descriptive phenomenology. The sampling technique used purposive sampling, and the number of participants was 10. The data collection used in-depth interview techniques. The Colaizzi method was used to analyze data.
Results
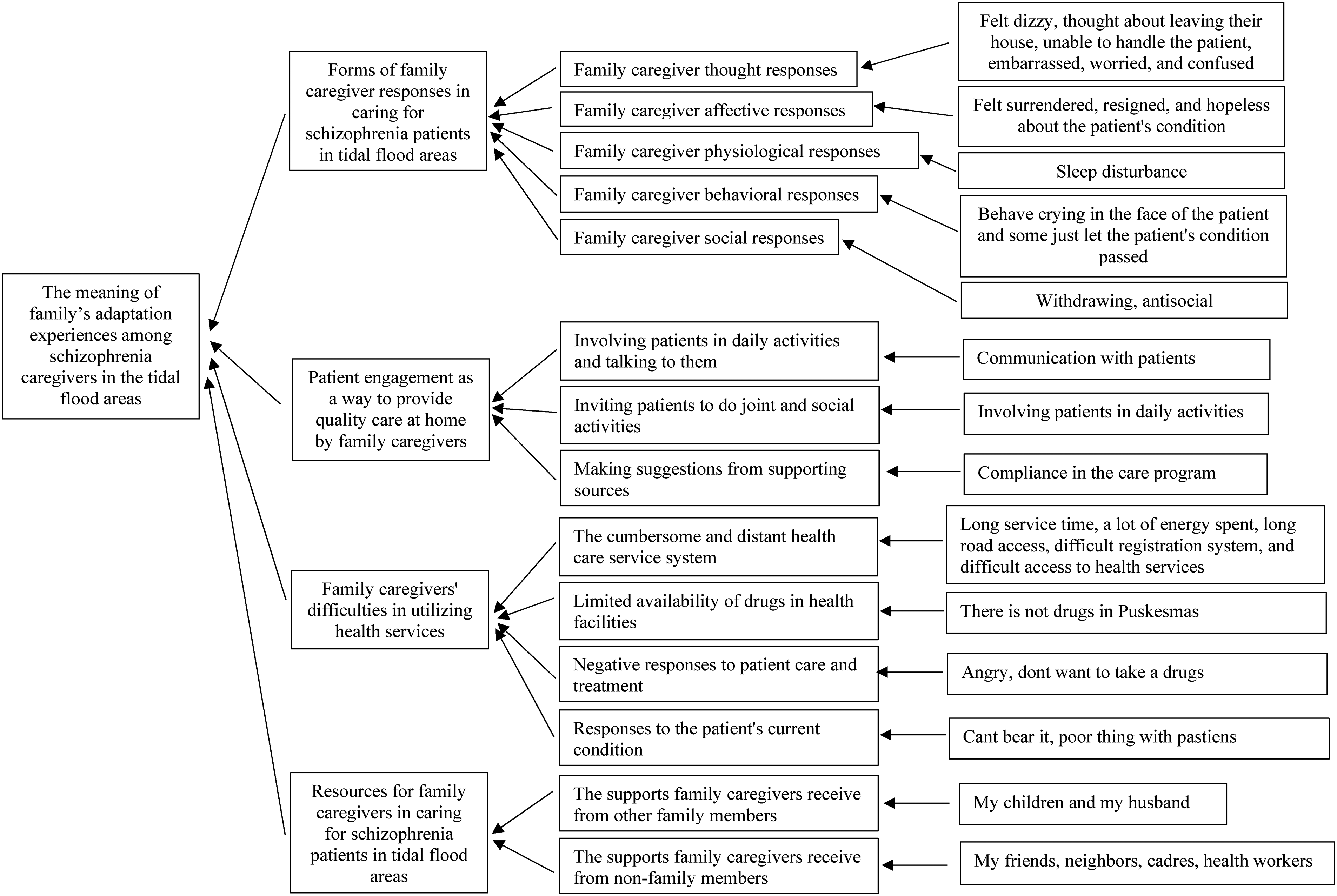
The adaptation experience meaning of family caregivers obtained four themes: (1) forms of family caregiver responses; (2) patient engagement as a way to provide quality care at home by family caregivers; (3) family caregivers’ difficulties in utilizing health services; and (4) resources for family caregivers.
Conclusion
The meaning of adaptation is whether the family caregivers feel the impact of their role and have difficulty utilizing health services in caring for patients. Despite this, family caregivers still try to continue to involve patients in daily activities and look for sources of support that are useful for them.
Recommendation
The physical and psychological well-being of family caregivers also need to be improved to support optimal care for patients who have schizophrenia by family caregivers at home.
Introduction
Family caregiver adaptation is the family caregiver's ability to improve coping in caring for patients who have schizophrenia and managing problems that arise as a result of caring for patients who have schizophrenia. Previous research states that family caregivers’ adaptation in caring for patients who have schizophrenia is influenced by stress, perceptions about schizophrenia, self-esteem, social support, coping mechanisms, and family caregivers’ perceptions about the condition they are experiencing (Suhita et al., 2017). The adaptation process in tidal flood situations is carried out at three different times, namely, before the tidal flood, during the tidal flood, and after the tidal flood occurs.
The research results show that before the tidal flood occurs, the adaptation process that must be had is adaptation to discomfort and anxiety to decide to stay in the tidal flood area. When a tidal flood occurs, the adaptation that must be had is adaptation to fear and panic when facing a flood situation. After the tidal flood, the adaptation that needs to be had is to face the impacts or changes that occur due to the tidal flood, both physical and psychosocial changes. However, the unpreparedness of adaptive attitudes and behavior toward the discomfort caused by tidal floods causes low psychosocial adaptation in communities in tidal flood areas, namely 72.02% (Putra et al., 2019). Physical adaptation of family caregivers to changes in the flood environment and the condition of patients who have schizophrenia has gone well, but psychosocial adaptation has not been achieved.
The tidal flood is a flood in coastal areas that occurs due to an increase in sea level, land subsidence, and changes in coastal space utilization (Kusumaning & Puriningsih, 2019). Tidal flood affected the mental health of 30% of the 51 participants more than the physical health impact of 14%. The other participants lost material by 31%, lost productivity by 6%, and only 19% did not feel any disturbing impact (Boyer-Villemaire et al., 2021).
Common mental health problems caused by tidal flooding include disturbed sleep patterns and stress (Boyer-Villemaire et al., 2021), adaptation problems, stress, and depression, fatigue, sadness, feelings of guilt, substance abuse, post-traumatic stress disorder, and suicide risk (Hayes et al., 2018). Previous research explains that mental health problems experienced by people in tidal flood areas occur for a long time, which can cause other problems if not addressed, namely, feelings of grief due to loss, maladaptive behavior in groups of children, domestic violence, and aggravate the condition of individuals with mental health problems that previously existed (Setiowati & Kuncoro, 2014). One of the previous mental health problems was schizophrenia.
There is no direct relationship between schizophrenia and tidal flood. Climate change is predicted to not only affect physical health, but is also likely to affect mental health. Rising environmental temperatures will likely increase rates of aggression and violent suicide, while prolonged drought due to climate change may cause more farmer suicides. Drought in turn can cause mental health problems and stress. The increasing frequency of disasters due to climate change can cause post-traumatic stress disorder, adjustment disorders, and depression (Walinski et al., 2023). However, the presence of tidal flood that triggers psychosocial problems, such as anxiety, stress, and post-traumatic stress disorder, may exacerbate previous schizophrenic conditions and living in tidal flood areas (Setiowati & Kuncoro, 2014). The patients with schizophrenia living in tidal flood areas are more vulnerable to psychosocial problems and relapse. The exposure to tidal flood exacerbates the symptoms of schizophrenia experienced. Previous research suggests that flooding is also associated with relapse in schizophrenia patients (Wei et al., 2019). The intensity of flooding that occurs continuously and the increasing severity of flooding further increase the mental burden of patients who have schizophrenia.
Caring for patients who have schizophrenia in tidal floods requires more effort than patients who have schizophrenia in non-tidal flood areas. In addition to providing standard care for patients who have schizophrenia, family caregivers must also provide support to reduce the increased vulnerability of schizophrenia experienced (Cianconi et al., 2020). The role as a family caregiver that lasts for a long time can make the family caregiver bored and tired, giving rise to negative emotions. Negative emotions that are felt become stress and burden for the caregiver's family, including feelings of hopelessness, guilt, helplessness, anxiety, and depression (Leng et al., 2019).
Family caregivers who are unable to manage emotions and show high emotional expression will add to the burden and worsen the condition of patient care at home (Yusuf et al., 2019). Therefore, family caregivers are required to manage stress and burden through adaptation to roles and the environment. The unreadiness of adaptive attitudes and behaviors toward the discomfort caused by tidal floods has led to low psychosocial adaptation in communities in tidal flood areas, which is 72.02% (Putra et al., 2019).
Review of Literature
It was stated that the ability of family caregivers to manage stress and emotions has an important role in the care of patients who have schizophrenia. Apart from improving the psychological well-being of family caregivers themselves, they can also help care for patients who have schizophrenia. Previous research results indicate that self-esteem, community support, self-efficacy, family caregivers’ coping strategies, and assessment of the patient's own condition influence the adaptation process. The stress and burden of caring for patients who have schizophrenia complicate the adaptation process (Suhita et al., 2017). In tidal flood conditions, it adds to the stress and burden of caregiver families with changes in the environmental and emotional situation due to tidal floods. Tidal floods increase vulnerability to psychosocial problems experienced by both patients and caregiver families themselves (Boyer-Villemaire et al., 2021; Hayes et al., 2018; Padhy et al., 2015). The purpose of this study was to explore the meaning of family adaptation experiences for those who care for patients with schizophrenia in the tidal flood area. The adaptation experience of each schizophrenia caregiver is different. This is made worse by the persistent tidal flood situation. The need to explore the meaning felt by each schizophrenic caregiver regarding the care of schizophrenic patients in the tidal flood area is important to get a specific picture of the meaning of the adaptation process they are undergoing.
Method
Design
This research is a qualitative research with a descriptive phenomenology approach to describe and explore the experience of families as caregivers in adapting to the care of patients who have schizophrenia in the tidal flood area. The researcher explored the meaning of family's adaptation experience as a caregiver of patients with schizophrenia in the tidal flood area.
Research Question
The research question is: What is the meaning of family adaptation experiences for those who care for patients with schizophrenia in the tidal flood area?
Sample
The participants in this study were caregivers of patients with schizophrenia who lived in areas of tidal flooding in one of the regions in Central Java, which has four community health centers, some of which were affected by tidal flood. The location was chosen based on the increasing size of the affected areas with the number of patients who have schizophrenia living in the areas reaching 90 people. The sampling technique used purposive sampling. Sampling was carried out directly by meeting participants and explaining the research by the first researcher. Before the research was conducted, the researcher had never had contact with the research participants and did not know each other.
Inclusion/Exclusion Criteria
Samples were selected based on patient and family caregiver inclusion criteria. Patient inclusion criteria included patients who have schizophrenia who were registered at a health center in a flood area in one of the regions of Central Java, had relapsed at least once, lived at home and had a caregiver, and were cooperative and could communicate well. Family caregiver inclusion criteria include family members who take care of other family members with schizophrenia (informal caregiver), aged > 18 years who directly care for other family members with schizophrenia, live in one house with family members with schizophrenia, and are able to read and write and can communicate well. In the process of obtaining research consent, there were two potential participants who refused to be interviewed because they were busy, and the patient was healthy. The number of participants in this study was 10 family caregivers. All research participants were aware of the aims, benefits, and research procedures that had been previously explained by the researchers. The 10 participants were obtained using data saturation. The research data had reached saturation in the eight participant based on the results of discussions held with all researchers, but the researchers added two participants to ensure that no new data emerged. Hence, the final participant results obtained saturation data for 10 participants.
Institutional Review Board Approval
Participants who met the inclusion criteria were given information about the research process and then given the freedom to decide on their participation in this research. Participants were not forced to participate in this research. Participants who agreed to be involved in the research were given a consent form before the research was carried out. Researchers maintain the confidentiality of their identity by being anonymous and the confidentiality of research data by not providing the data to anyone. This study has passed the ethics of the research from research ethics commission at one of the state universities in Indonesia.
Statistical Analysis
The data collection in this study used in-depth interview techniques and observation during the in-depth interview process. This research used a researcher as instrument in this research. The researcher created an interview guide that was asked directly to research participants with open questions. The interview guide was developed by the researcher based on the research objective, namely, to explore the meaning of the adaptation experiences of schizophrenia caregivers who live in tidal flood areas. The interview guide consists of demographic data, the patient's illness history, the caregiver's family history of caring for the patient, the caregiver's family's perception of the patient's condition and the tidal flood, the experience of living in the tidal flood area, and the efforts made to live with schizophrenic patients in the tidal flood area. Before the researcher conducted direct interviews with participants, the researcher conducted a trial interview first with the assistance of a supervisor to ensure that the researcher was competent in conducting interviews. An interview guide was created, and interviews were conducted in Indonesian. The results of the interviews that have been transcribed are then translated into English and back translated into Indonesian by different and certified people.
The researcher used open-ended questions in order to explore the participants’ experiences. The researcher who has been tasked with conducting interviews is the first researcher. The first researcher has experience in interviews and has the appropriate field of expertise, namely, in mental health nursing. The interview process was carried out at the participant's home. Interviews have been conducted varying between 45 and 60 min. Interviews were conducted alone between the researcher and the participant. The interviews were completed with field notes to identify situations and non-verbal responses during the interview process. The researcher wrote down the participants’ non-verbal responses on the interview transcripts to simplify the researcher in analyzing the data. In addition, the researcher used a good quality audio recorder to record conversations during the interview. The researcher confined all initial perceptions and knowledge related to the family's adaptation experiences as a caregiver in caring for schizophrenia in the tidal flood area. Bracketing was carried out by not directing participants to questions that were assumed by the researcher and not giving closed questions to participants during the interview process. After the interview was completed, the researcher delivered a closing sentence containing a schedule to validate the data or further explain the data that had been obtained. Researchers met with participants twice for interviews and to confirm the results of the interviews. Confirmation of the interview results was carried out by the researcher by giving the interview transcript to the participant for the participant to read and check for suitability. Participants stated that the data from the interview was in accordance with what was conveyed during the interview, and that there was no additional data that they wanted to add. The research was conducted in the period August–September 2023.
The researcher analyzed the data using the Colaizzi method. Data analysis was carried out manually by researchers. The researchers listened to the results of the interviews repeatedly to make data transcripts. Data transcripts were made in the form of verbatim transcripts. The researchers read the data transcripts repeatedly existing so that researchers can find the meaning of the data which is significant and provides a bottom line on participants’ important statements. All researchers identified keywords and grouping the similar keywords to category. The researchers grouped the categories into sub-themes, so that the sub-themes that emerge are again grouped into themes potential. The final stage is for the researcher to agree on the themes that are formed and describe the themes.
The researcher maintained the trustworthiness and validity of research data by writing down the entire process of analysis and data systematically to be checked repeatedly so as to avoid loss of data interpretation. The researcher described in detail the findings obtained in the form of a matrix or data analysis table, then in the form of an explanation of the interview results in the form of a scheme and a narrative that tells the interview and field notes, and then in the form of a discussion of the research results using articles and literature that are in accordance with the research topic. The researcher developed an audit trail by presenting excerpts from the interviews with the participants to explain the data from the participants through the original sentences of the participants.
Results
Sample Characteristics
Ten participants involved in this study were primary caregivers of patients who have schizophrenia derived from family members of the patients. The characteristics of the participants in this study are shown in Table 1 (participant characteristics). Range of schizophrenia caregivers’ age is 18–65 years. Most of schizophrenia caregivers are female and married. The relationship with the patient is as a mother and a sister. However, more than half of them continue to work, even as caregivers. Specifically, it is explained in Table 2 (participant codes and profiles) that the youngest schizophrenia caregiver was 41 years old. The education level of those who become schizophrenia caregivers is still low. Most of them treat patients who have schizophrenia who are at risk of violent behavior.
Participant Characteristics.

Interpretation in main text.
Participant Codes and Profiles.

Interpretation in main text.
Research Question Results
The adaptation experience meaning of family caregivers is shown in Figure 1. Result of data analysis obtained four themes as follows:
Forms of family caregiver responses in caring for patients who have schizophrenia in tidal flood areas. Family caregivers had responses to the conditions of patients who have schizophrenia in the tidal flood areas, which were supported by five subthemes, namely, family caregiver thought responses, family caregiver affective responses, family caregiver physiological responses, family caregiver behavioral responses, and family caregiver social responses. The unpredictable and uncontrollable condition of patients who have schizophrenia at the onset of the disease caused a response in the family caregiver's thoughts at the onset of the disease. Family caregivers thought about the patient's condition at that time and felt dizzy, thought about leaving their house, unable to handle the patient, embarrassed, worried, and confused.…I can't afford it (glazed eyes) (Participants 1, 4, and 6).…worried about going … or doing harm (Participants 2, 8, and 9).…I'm confused about what else to do… (Participants 3, 5, 7, 8, and 10).
Thematic analysis. The family caregivers’ thought response subtheme shows that family caregivers have suffered from psychosocial problems that are manifested in cognitive responses in the type of disturbing thoughts that do not necessarily occur and other thoughts that are triggered by the patient's schizophrenia. The feelings felt by family caregivers are the affective responses of family caregivers in dealing with patients at the beginning of their illness. The affective responses subtheme are supported by the category of family caregiver attitudes toward the patient. Family caregivers felt surrendered, resigned, and hopeless about the patient's condition. Family caregivers also felt upset and angry with the patient's condition.…I feel like giving up…and despairing…because sometimes it seems to get worse and does not heal (Participants 1, 6, and 7).…angry…pissed off… (elevated tone of voice) … (Participants 1, 4, and 8) Family caregivers also experience physical symptoms, which are physiological responses. Family caregivers’ statements about their physical symptoms are as follows.…Yes, the impact is that I can't sleep all night …(Participants 2, 6, 7, and 10). Sleep disturbance is a physical symptom experienced by family caregivers. The condition occurs in association with the patient's condition and behaviors that are harmful. Family caregivers’ behavioral responses are supported by the category of caregiver behavior towards the patient's condition. Some family caregivers behave crying in the face of the patient and some just let the patient's condition passed. The following are participants’ statements related to their behavior in dealing with patients at the beginning of their illness:Yes, just crying… My son… My daughter is like that, when I talk to people… I cry… (Participants 1, 5, and 8).…I asked hot hot hot, but I didn't respond (Participants 2, 5, 9, and 10). Family caregivers faced with stressors of schizophrenic patients also socially respond, which is supported by the category of antisocial behavior of family caregivers toward the patient's condition. This condition illustrated that family caregivers who care for schizophrenic patients have responses from those that are not visible from the outside to those that can be assessed from the outside, such as withdrawing or antisocial. Family caregivers preferred to stay at home.…So I just stay at home and confide in my children about my own neighbors getting angry (Participants 1, 3, and 5). Patient engagement as a way to provide quality care at home by family caregivers. The theme of patient engagement at home is supported by three subthemes, namely, involving patients in daily activities and talking to them, inviting patients to do joint and social activities, and making suggestions from supporting sources. Subtheme 1 involving patients in daily activities and talking to them is supported by the category of communication with patients.…If he's staring, I'll call him, come and sit here… (Participants 1, 6, 9, and 10). Subtheme 2 inviting patients to do joint and social activities is supported by the category of involving patients in daily activities.…I told him to sit there with me so that we can talk together with a friend. If he's alone, he'll be lost in thought… (Participants 1, 3, and 5).…I send you to the stall, for example, to shop…to the prayer room to pray (Participants 2, 4, and 7).Subtheme 3 of taking advice from supportive sources is supported by the category of compliance in the care program. The family caregivers followed what the health worker suggested and said there was no other choice but for them to take care of the patient.…diverted if you want to stare, diverted like that sir… (Participants 1, 4, 5, and 9).…If it's not me who takes care of it then who else… no other choice (Participants 3, 6, and 10). Family caregivers’ difficulties in utilizing health services. The theme of problems in utilizing health services was structured by four subthemes, namely, the cumbersome and distant health care service system, limited availability of drugs in health facilities, negative responses to patient care and treatment, and responses to the patient's current condition. The cumbersome and distant health care service system was supported by the categories of long service time, a lot of energy spent, long road access, difficult registration system, and difficult access to health services. Participant statements that support these categories include:…have to go back and forth in flood conditions… have to wait a long time… (Participants 1, 3, 5, and 8).…I had to wait until night just waiting for the drugs… (Participants 2, 4, and 9).…It usually takes me up to three days… (Participants 1, 7, and 10).…registering using the app (JKN) is difficult for me… (Participants 3 and 6). Resources for family caregivers in caring for patients who have schizophrenia in tidal flood areas. This theme is organized by two subthemes, namely, the support family caregivers receive from other family members, and the support family caregivers receive from non-family members.…I am strong because of my children and my husband… for the sake of my family…. (Participants 1, 7, 9 and 10).…My friends…neighbors…cadres…all helping me and my family… (Participants 1, 2, 3, 4, 5, 6, and 8).…Health workers (nurses) at the health center are very helpful… (Participants 1, 3, 4, 7, and 10).…The village apparatus and neighbors… (Participants 1 and 9).
Discussion
Caregivers of patients who have schizophrenia are informal caregivers who are still related to patients who have schizophrenia and provide assistance and care to patients, such as husbands, wives, children, and parents (Bumagin, 2009). Informal caregivers who are related to the individual being assisted are commonly referred to as family caregivers.
Forms of family caregiver responses in caring for patients who have schizophrenia in tidal flood areas.
Family caregivers in caring for patients who have schizophrenia have a variety of responses. Especially in the first experience of dealing with a sick schizophrenic patient in the early period, family caregivers show the same response (Niman, 2019). These responses include cognitive, affective, physiological, behavioral, and social responses. Previous research has shown that family caregivers who first cared for a family member with mental illness felt shocked, unexpected, sad, and hurt (Niman, 2019). The same thing happened in this study that participants felt dizzy, unable, embarrassed, worried, confused, desperate, irritated, crying, and unable to sleep, even at home.
The response that emerged among family caregivers was due to the increased responsibility for caring for patients who have schizophrenia and facing problems related to the signs and symptoms of schizophrenia itself, such as violent behavior and tantrums (Putri et al., 2022). Family caregivers who have dual roles also add negative responses as a burden in caring for patients who have schizophrenia. Previous research explains that family caregivers who have a dual role, namely, caring for patients who have schizophrenia and doing housework, cause the burden felt to increase (Tamizi et al., 2020). In the end, the burden felt by the caregiver family affects the physical, mental, social, and economic health of the caregiver family.
The strongest family caregiver response is shown by family caregivers who have a relationship as the patient's mother. A mother has a strong emotional bond with the child so that the grieving process that occurs in a mother is more profound than a family caregiver who has a family relationship as the patient's mother. Negative responses to caring for patients who have schizophrenia are influenced by the character of the family caregiver, tasks, the patient's condition, and the support received by the family caregiver themselves (Meheli, 2023).
Negative responses to patients who have schizophrenia are felt by family caregivers as a heavy burden. Therefore, family caregivers must have the knowledge and ability to create adaptive coping strategies. Adaptive coping strategies possessed by family caregivers of patients who have schizophrenia can improve their ability to care for patients who have schizophrenia and increase success in achieving treatment goals. Apart from that, with optimal knowledge and abilities, family caregivers can also overcome negative responses caused by caring for patients who have schizophrenia, such as stress, anxiety and depression (Zhou et al., 2021).
Patient engagement as a way to provide quality care at home by family caregivers.
Family caregivers take care of patients who have schizophrenia at home as an effort to adjust to the presence of patients who have schizophrenia at home. Care for patients who have schizophrenia at home in tidal flood areas is carried out by family caregivers by involving patients in daily activities, chatting, inviting patients to joint activities, involving in social activities, and implementing other advice and advice from health workers. Family caregivers try to adjust to the caregiver role of caring for patients who have schizophrenia in the tidal flood area. Family caregivers in the home care for patients who have schizophrenia to prevent and improve the condition of patients who have schizophrenia. Family caregivers who are able to adjust to providing schizophrenia care at home mean that family caregivers can accept the patient's condition and are committed to helping the patient get better. In addition, care efforts are carried out by maximizing the patient's potential, increasing the patient's self-esteem, and helping to increase the patient's enthusiasm and motivation in living life (Ayu et al., 2019).
Family caregivers need to receive intervention to increase their ability to improve the quality care at home for patients who have schizophrenia. Previous research explains that empowering families as caregivers can increase the family's capacity to care for schizophrenia patients and prevent relapse (Iswanti et al., 2024). This form of empowerment can increase involvement in daily activities of family caregivers with patients who have schizophrenia, receive social support, and improve care skills for schizophrenia patients.
The high burden of caring for patients who have schizophrenia requires family caregivers to remain adaptive and have an attachment to the patient in their care. Bonding with patients who have schizophrenia can minimize the emergence of emotional expressions in the family. Attachment and involvement of patients who have schizophrenia in daily activities are a form of supportive effort that can prevent relapse and improve the health status of families and patients who have schizophrenia (Chien et al., 2020).
Family caregivers’ difficulties in utilizing health services.
Efforts made by family caregivers to adjust to the caregiver's patient care duties during the tidal flood did not go as expected because family caregivers experienced obstacles in utilizing health services. Family caregivers felt that the health care system was cumbersome, that is, the location of health centers and hospitals was far away, and there are negative responses to patient treatment. In addition, family caregivers also felt that the availability of medicine at the health center was limited. The previous study mentioned that difficulties in accessing health care facilities were an obstacle for family caregivers in adjusting the role of caring for patients who have schizophrenia at home. The distant location of hospitals and health centers is a problem in reaching out related to the time, energy, and money spent to get to the hospitals and health centers (Chaudhari et al., 2017).
Other research states that care for patients who have schizophrenia in utilizing health services is supported by health insurance (BPJS) (Putri et al., 2022). However, challenges in health services for patients who have schizophrenia are still encountered, such as access to health services and awareness of family caregivers to utilize health services (Tamizi et al., 2020). One of the reasons for the limited use of health services by family caregivers is tidal flood. As a result, access to services and knowledge of family caregivers becomes limited. At the end, innovative efforts are needed in health services for family caregivers and patients who have schizophrenia in tidal flood areas, such as carrying out routine home visits and a strict evaluation monitoring process.
This form of health service can also be provided by providing telephone counseling services. Previous research states that telephone counseling and education services can overcome family caregivers’ problems in caring for patients who have schizophrenia, such as reducing stress and burden (Abdigaravand et al., 2023). It is hoped that family caregivers who have psychological well-being can optimally utilize health services for treating schizophrenia patients.
Resources for family caregivers in caring for patients who have schizophrenia in tidal flood areas.
Support in dealing with barriers to schizophrenia care in the tidal flood area by family caregivers is obtained from other family members, the community, and health workers. Other family members as a support system for family caregivers are children and husbands. Support systems from the community are the head of the RT, neighbors, and health cadres. Support systems from health workers are doctors who treat patients and nurses in charge of mental health programs. The other family members can provide support to family caregivers to improve their ability to care for and overcome the difficulties faced in caring for patients. Previous research explains that family support for schizophrenia caregivers can improve the coping process and adaptation in dealing with stress and prolonged crisis in caring for patients who have schizophrenia (Pesik et al., 2020). Support from other family members improves the communication process in the family and family confidence in caring for family members with schizophrenia.
Support systems from other family members are important because they are the closest environment to family caregivers who will affect the well-being of family caregivers. Other family members can help with the care provided by family caregivers to patients who have schizophrenia at home. Thus, family caregivers will feel that they get attention and help from other family members (Amalia & Rahmatika, 2020). Support systems from the community, such as neighbors and friends, can promote positive social relationships. Family caregivers have a purpose in life and psychological well-being. The life goals of family caregivers consist of targets and hopes to be achieved in caring for patients who have schizophrenia at home in tidal flood areas. Hope will create motivation and make family caregivers make optimal efforts in caring for patients who have schizophrenia at home (Amalia & Rahmatika, 2020).
Strengths and Limitations
The results of this research provide a real and actual picture of the meaning of family caregiver adaptation. The use of qualitative research methods obtains sensitive and meaningful data that describe real conditions that require direct problem solutions. Therefore, the results of this study open up further research. The limitation of this research is that because it is qualitative research that obtains a lot of exploratory data, further research is needed that can design strategies to overcome the problem of meaning adaptation in family caregivers of schizophrenia. This research aims to describe the phenomenon of adaptation without addressing the problems that accompany the meaning of adaptation.
Implications for Practice
Health workers in providing health services apart from focusing on schizophrenic patients can also pay attention to their family caregivers. The physical and psychological well-being of family caregivers also need to be improved to support optimal care for patients who have schizophrenia by family caregivers at home. Health workers can provide informational, emotional, and instrumental support so that family caregivers can adapt well in the process of caring for patients who have schizophrenia in tidal flood areas. The results of this research provide important information for policy makers as intervention material in handling the impact of tidal floods on mental health through the family caregiver adaptation process.
Conclusion
The family caregiver adaptation means responses to the conditions of patients who have schizophrenia in the tidal flood areas, with family caregivers still involving the patient in daily activities as a part of home care efforts. In addition, family caregivers have difficulty utilizing health services. However, family caregivers have sources of support to strengthen and convince family caregivers to continue caring for patients who have schizophrenia in tidal flood areas.
Supplemental Material
sj-docx-1-son-10.1177_23779608241289099 - Supplemental material for The Meaning of Family's Adaptation Experiences Among Schizophrenia Caregivers in the Tidal Flood Areas in Indonesia: A Phenomenology Study
Supplemental material, sj-docx-1-son-10.1177_23779608241289099 for The Meaning of Family's Adaptation Experiences Among Schizophrenia Caregivers in the Tidal Flood Areas in Indonesia: A Phenomenology Study by Eka Budiarto and Mustikasari in SAGE Open Nursing
Supplemental Material
sj-docx-2-son-10.1177_23779608241289099 - Supplemental material for The Meaning of Family's Adaptation Experiences Among Schizophrenia Caregivers in the Tidal Flood Areas in Indonesia: A Phenomenology Study
Supplemental material, sj-docx-2-son-10.1177_23779608241289099 for The Meaning of Family's Adaptation Experiences Among Schizophrenia Caregivers in the Tidal Flood Areas in Indonesia: A Phenomenology Study by Eka Budiarto and Mustikasari in SAGE Open Nursing
Footnotes
Acknowledgments
The authors would like to thank the Indonesia Endowment Funds for Education (LPDP) and Center for Higher Education Funding (BPPT). They also thank the Doctoral in Nursing Program, Faculty of Nursing, University of Indonesia for supporting and facilitating this research.
Author Contributions
Conceptualization (EB; M), methodology (M), investigation (EB), formal analysis (EB; M), and writing, including review and editing (EB; M).
Declaration of Conflicting Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study has passed the ethics of the research from Faculty of Nursing Ethics Commission, University of Indonesia with the number KET-150/UN2.F12.D1.2.1/PPM.00.02/2023.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received funding from Indonesia Endowment Funds for Education (LPDP) and Center for Higher Education Funding (BPPT).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.