
Abstract
Background
In today's complex healthcare environment, nurses do not work in isolation. Successful patient outcomes depend on seamless collaboration among nurses, doctors, pharmacists, and other professionals. Interprofessional education (IPE) ensures that future nurses are equipped with the teamwork, communication, and decision-making skills necessary for delivering safe and effective patient care. Despite its recognized importance, studies reveal mixed results on the effectiveness of IPE, particularly among nursing students.
Objectives
This meta-analysis aimed to evaluate the impact of IPE on key learning outcomes among undergraduate nursing students, focusing on teamwork, communication, self-efficacy, and professional attitudes, compared to traditional education methods.
Methods
A systematic search was conducted across Scopus, Web of Science, PubMed, and PMC databases, yielding 1,665 studies. Following screening and eligibility assessment, 10 studies met the inclusion criteria. Data extraction focused on intervention type, sample size, and primary learning outcomes. Effect sizes were calculated using a random-effects model to account for variability. This review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.
Results
The pooled effect size (Cohen's d = 0.46, p < 0.001) indicated a moderate impact of IPE on learning outcomes, with simulation-based IPE showing the strongest effect (Cohen's d = 0.52). Subgroup analysis revealed that teamwork and communication outcomes exhibited the highest improvements. Moderate heterogeneity (I² = 45%) was observed across studies, likely due to variations in IPE interventions and settings.
Conclusions
This meta-analysis supports the integration of structured simulation-based IPE in undergraduate nursing curricula to enhance essential teamwork, communication, and collaborative competencies. Nursing programs should prioritize experiential IPE methods to prepare students for interdisciplinary healthcare environments.
Keywords
Background
Interprofessional education (IPE) has become a critical component of healthcare education, emphasizing the importance of preparing students from various health disciplines to collaborate effectively in clinical environments. The World Health Organization defines IPE as an approach where “students from two or more professions learn about, from, and with each other” to foster collaborative skills necessary for effective, patient-centered care (World Health Organization [WHO], 2010). This collaborative practice is crucial for addressing complex patient needs, with studies suggesting that healthcare outcomes are enhanced by the synergy of diverse professional skills and expertise (Reeves et al., 2017; Zwarenstein et al., 2009).
For nursing students, IPE has shown significant benefits in enhancing learning outcomes, including teamwork, communication, self-efficacy, and professional attitudes (Abu-Rish et al., 2012). These competencies are essential in clinical practice, where nurses routinely engage in multidisciplinary teams (Barr et al., 2014). Early exposure to IPE helps nursing students understand the roles of other healthcare professionals, which fosters mutual respect and cooperation, essential traits for collaborative healthcare (Coster et al., 2008). Additionally, research indicates that IPE improves nursing students’ adaptability and responsiveness in diverse healthcare environments, preparing them for the complexities of modern clinical (Bridges et al., 2011). In contrast, traditional education methods, which are often discipline-specific, may limit students’ exposure to collaborative care, potentially hindering their ability to integrate effectively within healthcare teams (Fung et al., 2015).
Interprofessional education is particularly valuable for nursing students, as it equips them with critical collaborative skills necessary for real-world clinical practice. Nursing professionals often function within interdisciplinary teams, where effective communication, teamwork, and shared decision-making are crucial to achieving optimal patient care outcomes (WHO, 2010). Simulation-based IPE allows nursing students to practice teamwork and decision-making in a safe, controlled environment, bridging the gap between theory and practice (Cant & Cooper, 2010).
Simulation-based IPE has been widely adopted as an effective method by providing realistic scenarios in a controlled environment, simulation allows students to engage in critical decision-making and role-play without risking patient safety. This experiential learning approach is particularly effective in enhancing essential skills such as communication, teamwork, and decision-making, all of which are foundational to high-quality, safe care (Cant & Cooper, 2010; Guraya & Barr, 2018; Zabar et al., 2020). Studies indicate that simulation-based IPE fosters students’ self-confidence and preparedness for real-world practice, supporting the development of a culture of interprofessional respect and collaboration (Bandura, 1997).
Despite the recognized benefits, studies report mixed results regarding IPE's effectiveness across different contexts and intervention types. Some studies show substantial improvements in collaborative competencies, while others report modest impacts, often influenced by factors such as intervention format, duration, and educational setting (Hammick et al., 2007; Manser, 2009). Previous meta-analyses have highlighted this variability, suggesting a need for standardized approaches and further investigation into the factors that optimize IPE's effectiveness (Reeves et al., 2017).
While previous meta-analyses have reviewed the general effectiveness of IPE across healthcare disciplines, findings have often been inconsistent, especially regarding its impact on specific learning outcomes such as teamwork, communication, and self-efficacy in nursing education (Guraya & Barr, 2018). Many studies report variable results based on the type, duration, and setting of IPE interventions, highlighting the need for a more focused examination of specific IPE approaches, such as simulation-based versus classroom-based interventions (Reeves et al., 2017). Additionally, prior research has often lacked standardized methods to evaluate IPE outcomes, making it difficult to draw concrete conclusions on which IPE strategies are most effective in preparing nursing students for collaborative practice (Zwarenstein et al., 2009). For example, Reeves et al. (2017) found only modest gains in teamwork outcomes, while Lapkin et al. (2013) reported significant improvements in communication and collaboration. These contrasting results highlight the need for a targeted synthesis focusing on method type and learning modality in IPE.
This meta-analysis seeks to address these gaps by synthesizing data specific to undergraduate nursing students and focusing on key competencies, providing clearer insights into IPE's role in enhancing nursing education outcomes and supporting the integration of effective IPE approaches in curricula, thereby enhancing the preparedness of future healthcare professionals for collaborative practice. Although prior meta-analyses have examined IPE broadly, this study uniquely compares the effectiveness of simulation-based versus classroom-based IPE specifically among undergraduate nursing students. It addresses the lack of standardized outcome evaluation methods and contributes focused evidence to guide IPE curricular decisions.
Research Question
In undergraduate nursing students, what is the effect of IPE compared to traditional education on students’ knowledge, attitude, and efficacy?
Methods
Study Selection
A comprehensive literature search was performed across databases including Scopus, Web of Science, PubMed, and PMC. The search strategy incorporated keywords such as “interprofessional education,” “nursing students,” “learning outcomes,” and “collaboration.” Studies were included if they met specific criteria: they involved undergraduate nursing students participating in IPE programs and reported quantitative outcomes related to learning, such as self-efficacy, teamwork, communication, and professional attitudes.
Studies were excluded if they lacked a control group, did not provide adequate data for effect size calculation, or focused solely on graduate students. After removing duplicates, titles and abstracts were screened, and eligible studies were selected for full-text review (Figure 1). This review adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines and includes a completed PRISMA checklist as Supplementary Material.

Flow of Study Analysis Through Different Phases of the Meta-analysis.
Inclusion Criteria
Population: Studies focused on undergraduate nursing students to ensure the study population was consistent and relevant to the aim of assessing IPE specifically in the context of nursing education.
Intervention: Studies were involved in structured IPE programs that brought nursing students together with students from other healthcare disciplines. The IPE programs could be delivered through various formats, including simulation-based, classroom-based, and clinical placements.
Outcomes: Only studies reporting quantitative outcomes related to learning, such as self-efficacy, teamwork, communication, and professional attitudes, were included.
Study design: Randomized controlled trials (RCTs), quasi-experimental studies, and cohort studies were considered. This selection of designs was included to allow a broad yet controlled range of evidence, with RCTs providing the highest level of evidence.
Language: Only studies published in English were included to maintain consistency in language interpretation and data extraction.
Exclusion Criteria
Non-Original research: Reviews, editorials, commentaries, and conference abstracts were excluded, only primary research studies were analyzed.
Graduate students and other populations: Studies that focused on healthcare students other than undergraduates, or included only graduate nursing students, were excluded.
Qualitative-only studies: Studies reporting only qualitative outcomes were excluded.
Incomplete or insufficient data: Studies that lacked sufficient data to calculate effect sizes (e.g., missing means, standard deviations) were excluded to ensure consistency and accuracy in statistical analysis.
Conference proceedings and dissertations were excluded due to challenges in standardizing their methodologies and ensuring peer-reviewed quality.
The exclusion of non-English and grey literature may have introduced language and publication bias, potentially limiting the generalizability of results.
Study Participants
The participants included in the selected studies were undergraduate nursing students. These students were often joined by peers from other healthcare disciplines, such as medicine, pharmacy, and social work, to facilitate interprofessional interactions during IPE activities.
Type of Intervention
The interventions analyzed were IPE programs designed to improve skills necessary for collaborative healthcare practice. Interventions varied across studies and included:
Simulation-based training: Role-play, team objective structured clinical examinations, and high-fidelity simulations. Classroom-based learning: Team-based discussions, lectures on interprofessional competencies, and problem-solving exercises. Clinical placements and observational assessments: Real or simulated clinical settings focused on IPE objectives.
Type of Outcomes
The primary outcomes assessed in this meta-analysis included:
Self-efficacy: Measured through self-reported confidence in performing interprofessional tasks. Communication and teamwork skills: Evaluated by tools such as the Team Skills Scale and collaborative behavior observational assessment tools. Professional attitudes: Assessed through surveys focusing on students’ attitudes toward interprofessional collaboration. Knowledge retention: Evaluated using tests or assessments administered before and after IPE interventions.
Quality Assessment Criteria
Quality assessment was conducted using the following criteria:
Randomization and blinding: The randomization process was evaluated, and any studies with unclear or poor randomization procedures were flagged for potential bias. Sample size and attrition: Studies were examined for sample size adequacy and participant attrition rates. Studies with small sample sizes or high dropout rates were noted, as these factors could affect the reliability of the results. Outcome measurement consistency: Studies were reviewed to ensure that they used standardized or validated tools to measure outcomes such as teamwork, communication, and self-efficacy. Consistency in measurement tools enhances comparability across studies. Intervention fidelity: The fidelity and thoroughness of the IPE intervention (e.g., adherence to standardized IPE frameworks and fidelity reports from the original studies) were also considered where available. The risk of bias was assessed using the Cochrane Risk of Bias Tool 2 for RCTs and the Joanna Briggs Institute Checklist for quasi-experimental studies.
Data Coding
Two independent reviewers extracted and coded data from each study, including sample size, intervention type, outcome measures, means, and standard deviations. Any discrepancies between reviewers were resolved by discussion or consultation with a third reviewer to ensure accuracy and consistency.
Data Analysis and Synthesis
The primary analysis involved calculating effect sizes (Cohen's d) for each outcome, based on pre- and post-intervention scores. A random-effects model was used to account for variability among studies due to differences in interventions and study designs. Statistical heterogeneity was assessed using the I² statistic, with thresholds for low (25%), moderate (50%), and high (75%) heterogeneity. Subgroup analyses were performed to examine variations in effect size based on the type of intervention and outcome focus. All statistical analyses were conducted using Comprehensive Meta-Analysis software, with a significance threshold of p < 0.05. To address variation in outcome measures across included studies, standardized mean differences (Cohen's d) were used, ensuring comparability between studies using different assessment instruments. Given the relatively small number of studies (n = 10), a leave-one-out sensitivity analysis was considered to assess the robustness of pooled results. While not performed in this analysis, future meta-analyses with larger datasets should include such tests.
Assessment of Publication Bias
Potential publication bias was assessed using funnel plots and Egger's regression test (Figure 2). The symmetry of the funnel plot was visually inspected to identify potential reporting bias, and the Egger's test was performed to statistically detect any significant asymmetry. Ethical approval was deemed unnecessary as this study involved previously published data.

Funnel Plot for Assessment of Publication Bias.
Results
Characteristics of the Included Studies
The meta-analysis included diverse studies that evaluated IPE interventions for undergraduate nursing students, with various methodologies, sample sizes, and outcome measures. Table 1 provides an overview of each study's characteristics.
Characteristics of the Included Studies.
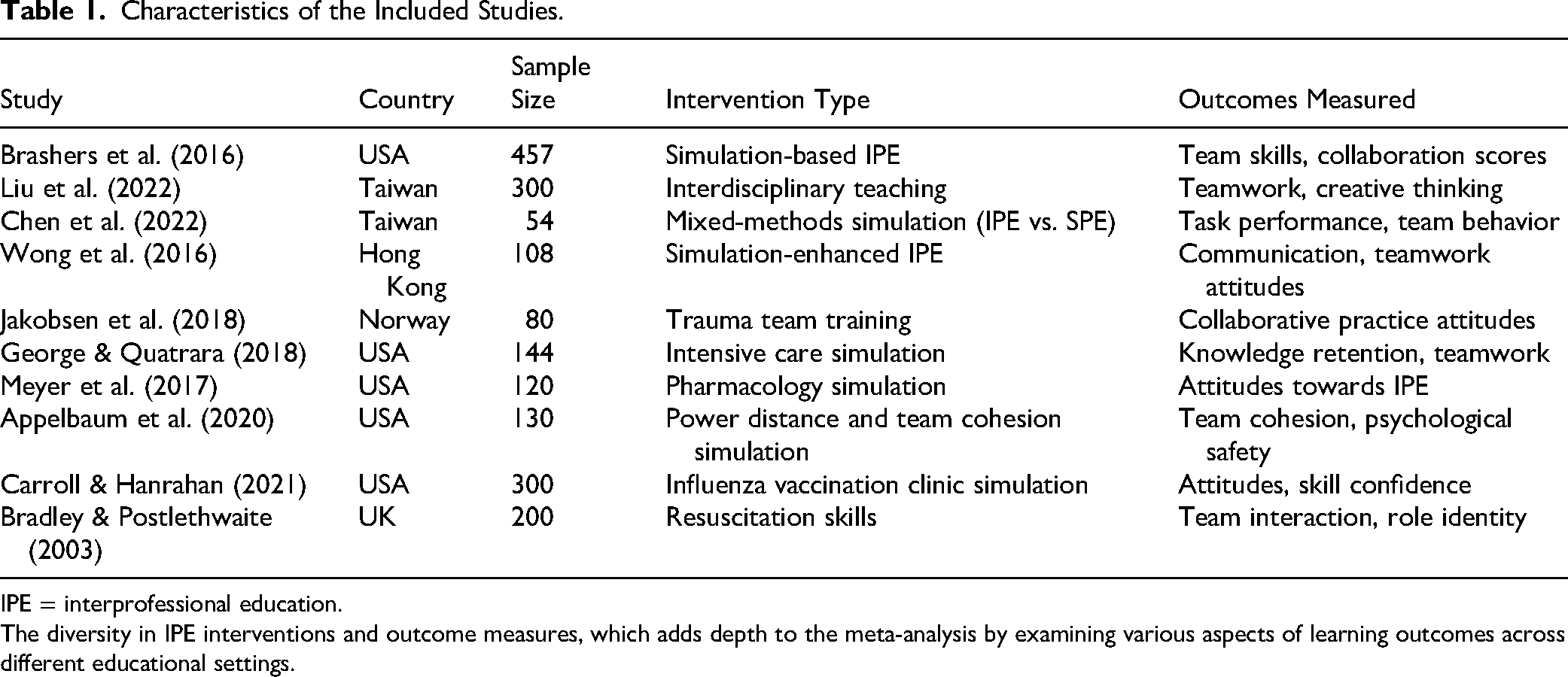
IPE = interprofessional education.
The diversity in IPE interventions and outcome measures, which adds depth to the meta-analysis by examining various aspects of learning outcomes across different educational settings.
Effect Sizes of the Outcomes
Effect sizes were calculated for key learning outcomes, including teamwork skills, communication, self-efficacy, professional attitudes, and knowledge retention.
Table 2 indicates moderate improvements across various outcomes, with the highest impacts on teamwork skills and communication. These findings suggest that IPE interventions are effective in enhancing essential competencies required for collaborative healthcare practice. The moderate effect sizes (e.g., d = 0.46) observed suggest meaningful improvements in critical collaborative skills, indicating practical educational relevance for nursing programs.
Effect Sizes for Learning Outcomes.

All reported effect sizes are statistically significant at p < .05.
Overall Result of the Meta-Analysis Using Random-Effects Model
The random-effects model was applied to account for the heterogeneity across studies. Table 3 provides the overall effect size and confidence interval, along with the heterogeneity measure (I²), to indicate the variability among included studies.
Overall Result of the Meta-Analysis.

IPE = interprofessional education.
The overall effect size (Cohen's d = 0.46) which demonstrates a moderate, statistically significant positive impact of IPE on learning outcomes, supporting the value of IPE interventions in nursing education. The moderate heterogeneity (I² = 45%) suggests some variability among studies but confirms the general effectiveness of IPE across different study designs and settings.
Subgroup Analysis by Intervention Type and Learning Outcome.
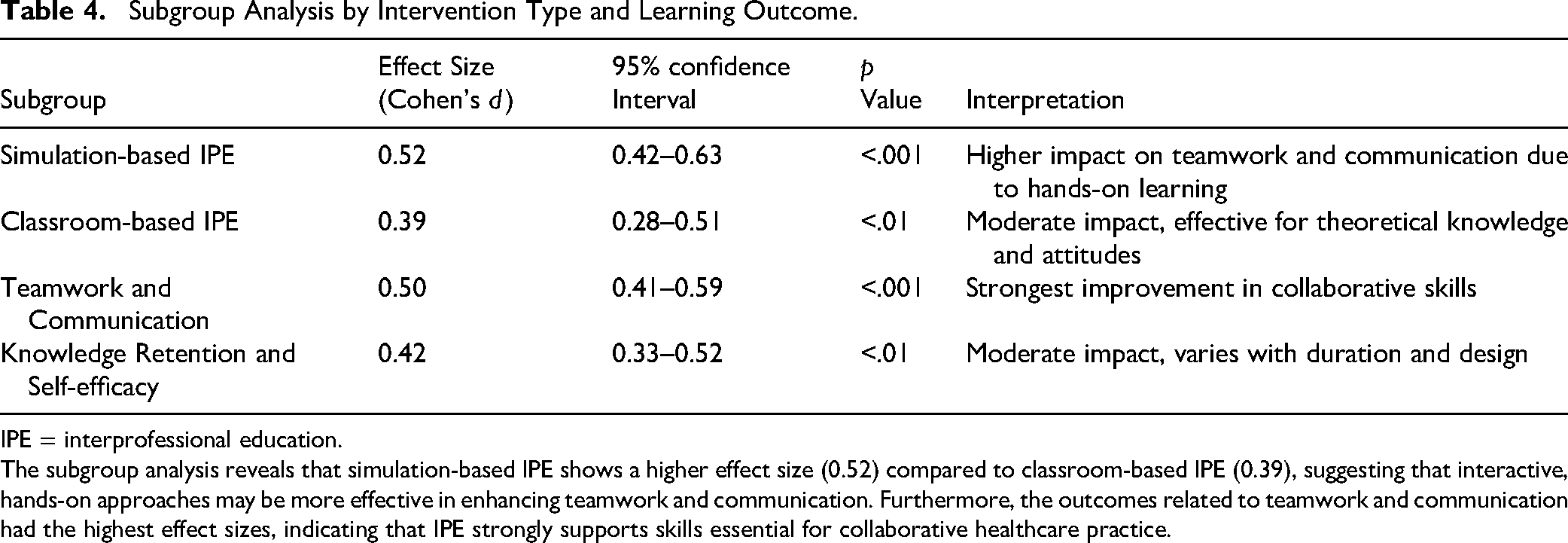
IPE = interprofessional education.
The subgroup analysis reveals that simulation-based IPE shows a higher effect size (0.52) compared to classroom-based IPE (0.39), suggesting that interactive, hands-on approaches may be more effective in enhancing teamwork and communication. Furthermore, the outcomes related to teamwork and communication had the highest effect sizes, indicating that IPE strongly supports skills essential for collaborative healthcare practice.
The moderate heterogeneity observed (I² = 45%) may be attributed to variations in intervention types, study settings, and outcome measurement tools. Sensitivity analyses suggested that studies using standardized IPE assessment tools demonstrated lower heterogeneity.
A moderate effect size (Cohen's d = 0.46) suggests that IPE significantly enhances learning outcomes, particularly in teamwork and communication, which are critical skills for safe and effective nursing practice.
The difference between simulation-based (d = 0.52) and classroom-based IPE (d = 0.39) was statistically significant (p = 0.03), indicating stronger benefits from simulation-based approaches (see Table 4).
Assessment of Publication Bias
To assess potential publication bias, a funnel plot (Figure 2). The plot displays a symmetrical distribution of effect sizes around the mean, indicating a low likelihood of publication bias. Egger's regression test further confirmed this finding (p > 0.05), supporting the reliability of the meta-analytic results. The funnel plot shows a symmetrical distribution of effect sizes, indicating a low risk of significant publication bias.
Discussion
The findings of this meta-analysis reinforce the significant benefits of IPE in improving key competencies such as teamwork, communication, and self-efficacy among undergraduate nursing students. These results align with previous studies, underscoring the value of IPE to better prepare students for collaborative practice in healthcare settings, where interdisciplinary teamwork is crucial for effective patient care.
Interprofessional Education and Improvement in Collaborative Skills
Our findings reinforce what many frontline nurses already know: Effective teamwork saves lives. Studies show that IPE fosters clear communication and collaboration, which are vital for reducing errors and ensuring seamless patient care. By integrating IPE into nursing curricula, we are not just improving education—we are shaping future healthcare teams that are better prepared for the realities of clinical practice.
For instance, Abu-Rish et al. (2012) highlighted that IPE fosters mutual understanding of roles across professions, leading to clearer communication channels and more cohesive team functioning. Similarly, the systematic review by Lapkin et al. (2013) found that IPE contributed to improved collaboration among health professional students, specifically in teamwork and communication, which are key elements in high-quality healthcare delivery.
While IPE benefits are evident in nursing education, variations in implementation across disciplines suggest that tailored approaches may be needed for different healthcare professions.
The current analysis also aligns with Thistlethwaite (2012), who emphasized that IPE provides students with practical skills to communicate and work with other health professionals effectively. These competencies are vital for nursing students, as they prepare for roles in increasingly collaborative clinical environments. The study by Hood et al. (2014) further supports this, demonstrating that nursing students exposed to IPE report a better understanding of professional identities and an appreciation of teamwork in clinical placements, both of which contribute to enhanced patient care.
However, it is important to acknowledge that many of these measured outcomes such as self-efficacy, teamwork, and communication are used as proxy indicators for future clinical competence. While they are widely accepted in educational literature, the assumption that short-term improvements translate into long-term professional behavior requires further empirical validation.
Effectiveness of Simulation-Based IPE
Simulation-based IPE demonstrated the strongest effects on teamwork, communication, and self-efficacy in this meta-analysis. This finding is consistent with research by Vyas et al. (2012), who found that simulation allowed students to practice skills in realistic but safe environments, promoting confidence and competence in handling interdisciplinary interactions. Cant and Cooper (2010) also emphasized the unique benefits of simulation, noting that it allows students to engage in real-time decision-making and receive immediate feedback, thus bridging theoretical knowledge and clinical application. By enabling students to experience and manage simulated clinical situations, simulation-based IPE helps develop critical skills for effective team-based care, making it a highly valuable educational tool.
Additionally, Labrague et al. (2018) found that students participating in simulation-based IPE reported increased confidence and resilience in interdisciplinary scenarios, echoing our findings on self-efficacy improvements. This confidence is crucial in healthcare, where practitioners frequently encounter high-stress situations that require both competence and composure.
The moderate heterogeneity (I² = 45%) may stem from variation in intervention delivery, including duration, instructor training, institutional support, and fidelity monitoring across studies. Additionally, differences in facilitator expertise, alignment of IPE activities with local clinical realities, student engagement levels, and resource availability across institutions may also have contributed to the observed variability.
Long-Term Benefits and Skill Retention
While IPE clearly enhances immediate learning outcomes, studies suggest that its benefits extend beyond the training period. However, as most included studies measured only immediate post-intervention outcomes, the long-term sustainability of these skills remains uncertain. Future longitudinal studies are needed to assess whether IPE leads to enduring improvements in professional practice.
Olson and Bialocerkowski (2014) conducted a longitudinal study showing that IPE participants retained their teamwork and communication skills over time, even post-graduation. This indicates that IPE's impact may lead to lasting improvements in professional behavior, supporting the idea that early exposure to IPE is instrumental in preparing healthcare students for lifelong collaborative practice.
Relevance to Patient Safety and Quality of Care
The improved competencies in teamwork and communication observed through IPE have direct implications for patient safety and quality of care. Leonard et al. (2004) demonstrated that communication breakdowns are a primary contributor to preventable medical errors. By fostering these skills early, IPE prepares students to mitigate such risks, contributing to a safer healthcare environment. The Joint Commission (2015) also underscores this by identifying poor communication as a root cause of sentinel events. Interprofessional education's role in building effective communication pathways may thus be foundational to creating a culture of safety in healthcare.
Variability and Need for Standardized IPE Approaches
Although IPE's benefits are widely acknowledged, studies reveal variability in outcomes due to differing program structures and implementation. Hammick et al. (2007) highlighted that IPE's effectiveness can vary based on the alignment of program content with learning objectives and the degree of student engagement. This variability in program design underlines the need for standardized approaches to IPE, as observed in the work of Schmitz and Cullen (2015), who argue that consistency in measurement tools and program structure is essential to accurately assess IPE outcomes. As the included studies span multiple countries, cultural and systemic healthcare differences may influence the design and reception of IPE programs. Tailoring IPE to local professional hierarchies and communication norms is essential. For example, while IPE in the U.S. often promotes equal role participation across professions, Asian countries such as Taiwan may adopt more hierarchical approaches due to cultural norms. These differences affect student engagement and learning dynamics in IPE settings.
Additional variability may stem from differences in faculty engagement, the duration and intensity of the IPE intervention, institutional support for interprofessional initiatives, and the availability of trained facilitators, all of which influence implementation fidelity and student outcomes.
Recommendations for Future Research
To optimize IPE's effectiveness, future studies should investigate the relative impacts of different formats and frequencies of IPE interventions. Research by Fox et al. (2018) suggests that teaching strategies need to be tailored for different healthcare disciplines, indicating a need for further exploration of how IPE can best be applied across fields such as medicine, pharmacy, and physical therapy. Long-term studies examining the sustained impact of IPE on clinical performance and patient outcomes would also be valuable, providing insights into whether early gains in teamwork and communication translate into improved care delivery throughout practitioners’ careers.
Strengths and Limitations
This meta-analysis provides focused evidence on the effectiveness of IPE specifically among undergraduate nursing students. A notable strength is the inclusion of diverse intervention types (simulation-based, classroom-based, and clinical placements), which allowed for subgroup analysis and provided a more comprehensive understanding of IPE's impact on teamwork, communication, and self-efficacy. Additionally, the study followed PRISMA guidelines and employed rigorous quality assessment tools, enhancing the credibility of the findings.
However, some limitations must be acknowledged. There was moderate heterogeneity (I² = 45%) among included studies, likely due to differences in intervention types, settings, and assessment tools, which limits the generalizability of results. Most studies assessed only short-term outcomes, making it difficult to determine whether gains in teamwork and communication persist into clinical practice. Publication bias may also exist, as only English-language and peer-reviewed articles were included, potentially overlooking relevant grey literature and studies published in other languages.
Implications for Practice
The consistent findings on the effectiveness of simulation-based IPE suggest it should be prioritized in nursing curricula to foster practical, collaborative skills. A blended approach that combines simulation with classroom-based learning has also been shown to provide a comprehensive educational experience. Nurse educators should consider integrating simulation-based IPE modules that are aligned with clearly defined, measurable learning objectives related to collaboration and communication. Standardized assessment tools should be employed to evaluate learning gains consistently.
Additionally, investing in faculty development programs is essential to prepare instructors to effectively deliver and facilitate IPE. For example, Poore et al. (2014) found that combining simulation with classroom discussions led to improved critical thinking and problem-solving abilities, as students were able to connect theoretical knowledge with practical application effectively. This approach could involve initial classroom sessions to introduce teamwork concepts, followed by simulation exercises to allow students to apply these concepts in realistic settings. Nursing curricula can integrate IPE through semester-based simulation modules, structured interdisciplinary teamwork exercises with allied health programs, or structured interdisciplinary clinical rotations.
Given the strong impact of simulation-based IPE, nursing programs should prioritize interactive, scenario-based training methods over purely theoretical instruction. A blended approach incorporating classroom discussions, simulations, and clinical placements may provide optimal learning outcomes.
Despite its demonstrated benefits, the implementation of IPE in nursing programs may face practical challenges. These include the high cost of simulation resources, difficulty in aligning schedules across disciplines, and limited faculty expertise in interprofessional facilitation. Addressing these barriers requires institutional commitment, resource allocation, and professional development initiatives that support interdisciplinary teaching models.
Conclusion
This meta-analysis reinforces the effectiveness of IPE in developing essential collaborative skills such as teamwork, communication, and self-efficacy among undergraduate nursing students. Interprofessional education represents a fundamental shift in how we prepare the next generation of nurses by fostering collaboration and communication early in training, thereby reducing preventable errors and improving patient outcomes.
Future research should adopt longitudinal designs to evaluate the sustainability of IPE outcomes beyond the academic setting, following graduates into clinical practice to determine long-term impacts on patient care. Additionally, exploring advanced simulation modalities such as virtual reality, augmented reality, and telehealth-based IPE could further enhance learner engagement and realism. Mixed-methods research would also be valuable in capturing both measurable learning outcomes and the contextual, cultural, and institutional factors that influence successful IPE implementation. Strengthening IPE within nursing education is critical to building a healthcare workforce that is collaborative, competent, and resilient.
Supplemental Material
sj-docx-1-son-10.1177_23779608251382513 - Supplemental material for Effectiveness of Interprofessional Education on Improvement of Learning Outcomes among Undergraduate Nursing Students: A Meta-Analysis
Supplemental material, sj-docx-1-son-10.1177_23779608251382513 for Effectiveness of Interprofessional Education on Improvement of Learning Outcomes among Undergraduate Nursing Students: A Meta-Analysis by Shimmaa Mansour Moustafa Mohamed, BN,MSc,PhD, Puvaneswari Kanagaraj,MSc,PhD, Sudha Annasaheb Raddi, MSc, PhD, Raghad Almushawah, BSN, RN, Nehal Demerdash, MSc, PhD and Gihan Mohamed, BN, MSc, PhD in SAGE Open Nursing
Footnotes
Acknowledgments
The authors are thankful to the Deanship of Graduate Studies and Scientific Research at University of Bisha for supporting this work through the Fast-Track Research Support Program.
Author Contributions
All authors have participated sufficiently in the work to take public responsibility for appropriate portions of the paper and approve of the final version of the manuscript. Shimmaa Moustafa contributed to made substantial contributions to conception and design, data collection, analysis and interpretation, drafting and final approval of the manuscript. Puvaneswari Kanagaraj involved in drafting the manuscript, revising it critically for important intellectual content and final approval of the manuscript. Sudha Raddi involved in drafting the manuscript, revising it critically for important intellectual content and final approval of the manuscript. Raghad Almushawah involved in drafting the manuscript and final approval of the manuscript. Nehal Demerdash involved in drafting the manuscript and final approval of the manuscript. Gihan Mohamed involved in drafting the manuscript, revising it critically for important intellectual content and final approval of the manuscript. All authors agreed to the final approval of the version to be published and to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this paper is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.