
Abstract
Introduction
Parental stress related to their infants’ hospitalization is a significant concern that affects both parents and their infants. Fathers’ experiences tend to be understudied compared to mothers. Further research on fathers’ stress levels is necessary. While parental stress has been correlated with infant health severity, the specific causes and risk factors contributing to heightened stress levels in parents of neonatal intensive care unit (NICU) infants are not yet fully understood and require further investigation.
Objective
This study aimed to examine the stress levels experienced by parents of premature infants in the NICU and to explore the factors associated with parental stress in this specific context.
Methods
A cross-sectional observational design was used to accomplish this study, which was carried out on 743 parents from nine different NICUs located in governmental hospitals across various locations in Egypt. We used characteristics of parents and premature infants, and Parent Stress Scale was used for data collection.
Results
A majority of parents reported experiencing high stress in the following domains: sight and sound (80.3%), infants’ appearance (69%), and the parent-infant relationship (81.4%). Additionally, about three-quarters (73.6%) of parents experienced high stress overall, with a mean score of 167.56 (21.3).
Conclusion
About three-quarters of the parents experienced high overall stress levels. Also, factors that were found to affect parents’ stress levels included premature infants connected to mechanical ventilators, previous neonatal death, parents living far from hospitals, infants delivered through cesarean section, insufficient income, and prolonged hospitalization beyond 5 days.
Introduction
Premature birth is a global issue, with 15 million infants born prematurely each year. The World Health Organization (WHO, 2023) states that the rate of premature births exceeds 1 in 10 babies. Complications of preterm birth lead to approximately 1 million child deaths annually. In the Middle East, Egypt has reported a 12% incidence of premature births (UNICEF, 2023).
Premature birth refers to babies born before 37 weeks of pregnancy (Akkoyun & Tas Arslan, 2019). Premature infants are at a high risk of developmental disabilities and delays and rely heavily on their parents (Ansari et al., 2022; Hendy et al., 2022). They are also more susceptible to life-threatening illnesses affecting the gastrointestinal, respiratory, neurological, and cardiovascular systems. Additionally, premature infants often face challenges related to poor muscle tone, immature motor control, and difficulties with feeding coordination (Samane et al., 2022).
Neonatal units (NNUs) are dedicated to providing specialized care to sick and premature infants, offering integrated services (Malouf et al., 2022). The neonatal intensive care unit (NICU) environment is filled with stressful stimuli due to complex technology and numerous treatment procedures. When infants are admitted to the NICU, the process of parental attachment can be disrupted due to the unique conditions of the unit (Heidarzadeh et al., 2023). The sense of powerlessness among parents may perceive in this situation can alter parental roles that increase negative feelings (Samane et al., 2022).
Premature birth and NICU admission are associated with various negative emotions experienced by parents, including sadness, fear, hopelessness, anger, insecurity, depression, anxiety, and parental stress (Lean et al., 2018). Stress can be defined as a state of mental tension caused by difficult situations (WHO, 2023). Stress has far-reaching effects at the individual, interpersonal, and societal levels, necessitating a comprehensive understanding to develop interventions that mitigate its impact (Ansari et al., 2022).
Parental stress is linked to concerns about the infant's health, their outcomes, changes in the parenting role, unexpected situations involving the baby, noise from equipment in the NICU, disruptions to parent-infant bonding, and feelings of grief related to the loss of an anticipated healthy child (Hagen et al., 2019). Poor communication with and among staff, often resulting from staff discontinuity, can damage trust and further contribute to parental stress (Bry & Wigert, 2019). Other factors that affect parents’ negative feelings include preexisting family factors and prenatal and perinatal experiences (Herini et al., 2022).
While their neonate is in the NICU, parents often have to dedicate significant time either at the hospital or commuting between the hospital and their home. This separation from their family further contributes to their stress levels (Dadkhahtehrani et al., 2018). In addition to personal attributes such as age, gender, and physical health, factors like geographical location, socioeconomic status, race, and ethnicity have an impact on the level of stress experienced by parents and can potentially jeopardize their physical and mental well-being (Ganguly et al., 2020). Also, young age mothers suffered from high stress than old (Ionio et al., 2019). The mean score on the parental role alterations subscale was higher among mothers than fathers (Çekin & Turan, 2018).
Literature Review
The birth of a premature infant requiring intensive care is recognized as an extremely stressful event for parents (Hagen et al., 2019). The NICU environment contains multiple stressors including the infant's appearance and behaviors, staff interactions, sights and sounds of the unit, and altered parental role (Bry & Wigert, 2019). High levels of acute stress can negatively impact the mental health, coping, and parenting capacities of mothers and fathers (Ansari et al., 2022).
High levels of stress in parents can have adverse effects on their mental and emotional well-being. It can also impact their ability to bond with their infants and actively participate in their care, which can have long-term consequences for the infant's development (Hagen et al., 2019). Understanding the factors contributing to parental stress in the NICU can help healthcare providers identify areas where interventions may be needed to improve both parental and infant outcomes (Herini et al., 2022). Parental stress is linked with both anxiety and depression and can have a significant negative impact on parents, child health and family relationships (Johansson et al., 2020). This review synthesizes current evidence regarding parental stress levels in the NICU and factors that may influence the parental experience.
Prevalence of Stress in the NICU
A significant proportion of parents report severe to extreme stress related to their infant's NICU stay across studies worldwide. The study conducted by Ganguly et al. (2020) in the NICU of a tertiary care hospital in Eastern India on 100 mothers using the Parent Stress Scale (PSS) found that 60.8% of parents reported experiencing severe and extreme levels of overall stress. This study had a reasonably large sample size of 100 mothers. However, it was conducted at a single hospital so the findings may not be generalizable to the larger population. The use of a validated scale (PSS) to measure parental stress is a strength. Similarly, a study conducted by Shiab El-Din et al. (2020) in Egypt on 90 mothers using the validated Parental Stress Scale (Berry, 1995) at one hospital so the findings may not be generalizable to the larger population and revealed that two-fifths of mothers were at risk of experiencing high levels of stress due to their infant's admission to the NICU.
Sources of Parental Stress
Both situational and personal factors contribute to NICU parental distress. The study by Ionio et al., 2019 in Italy on 43 mothers and 38 fathers of preterm infants focused on identifying potential risk factors that may influence parents’ reactions and emotions after the premature birth of their infant. The use of two comparison groups and a focus on predictive factors were strengths, but the small sample size from one center and lack of details on measures used limit the reliability and generalizability of this study's findings. In addition, Turner et al. (2015) conducted study on 73 Parents of babies in an Australian NICU and stated that older parental age, very premature birth, and twin birth were significantly associated with a higher PSS.
Specifically, certain demographic and clinical factors related to the parents and the infant have been suggested to impact parental stress levels and negative feelings in the NICU (DeMier et al., 2000; Muller-Nix & Ansermet, 2009). An infant's degree of prematurity and severity of illness have been found to predict parental stress, as external infant characteristics signaling immaturity and poorer medical status may heighten parent stress, disrupting their parental role (DeMier et al., 2000; Muller-Nix & Ansermet, 2009).
In accordance with the Lazarus and Folkman Transactional Model of Stress and Coping, the experiences of parents of premature infants in the NICU can be elucidated through the lens of cognitive appraisals and coping mechanisms (Chang et al., 2006). As posited by the model, the primary appraisal phase involves the evaluation of the significance of the stressor, where parents facing the challenges of their infants’ critical health condition may engage in both problem-focused and emotion-focused coping strategies (Lazarus & Folkman, 1984). Moreover, the secondary appraisal stage highlights how the resources and coping mechanisms available to parents, such as social support, financial stability, and coping skills, play a crucial role in moderating the impact of stress on parental well-being (Miles et al., 2007).
The utilization of this framework within the context of our study reveals the intricate interplay between cognitive appraisal processes, coping strategies, and the multifaceted stressors faced by parents in the NICU setting, ultimately contributing to a comprehensive understanding of the parental stress experience.
Moreover, in most of the past studies, researchers have focussed on experiences’ of mothers but limited studies especially at Egypt that assess fathers’ experience, so we assessed that. Also, while parental stress has been correlated with infant health severity, the specific causes and risk factors contributing to heightened stress levels in parents of NICU infants are not yet fully understood and require further investigation. So, our study aimed to examine the stress levels experienced by parents of premature infants in the NICU and to explore the factors associated with parental stress in this specific context.
Methods
Research Questions
Q1: What are the stress levels reported by parents of premature infants in the NICU?
Q2: What are the factors contributing to parental stress in the NICU?
Research Design
A cross-sectional observational design was employed for this study. Data were collected from nine different NICUs located in governmental hospitals across various locations in Egypt. The study included parents of premature infants who were hospitalized in the NICUs between February 2023 and May 2023. The sample of parents included in the study consisted of individuals, both parents of the same infant, whose infants were either born prematurely or near-term and were admitted to the NICU. A total of 985 parents were invited to participate in the study, and 743 of them agreed, resulting in a response rate of 75.4%.
Sample Size
To estimate the required sample size for estimating a population proportion with a confidence level of 95% and a margin of error of 3.59%, while assuming a population proportion of 53%

Using the Lazarus and Folkman Transactional Model of Stress and Coping as a framework for a study on the stress levels of parents of premature infants in the NICU provides a comprehensive approach to understanding and addressing the complexities of this experience.
Key elements of the Lazarus and Folkman transactional theory of stress as primary appraisal, secondary appraisal, and situational factors (Chang et al., 2006; Sharifabad et al., 2020).
Identification of Stressors
Primary Appraisal
Identify stressors perceived by parents of premature infants in the NICU. This could include medical concerns, uncertainty about the infant's health, separation from the baby, financial strains, and emotional distress.
Secondary Appraisal
Evaluate parents’ perceptions of their ability to cope with stressors. Assess available resources, support systems, and coping mechanisms. Consider factors such as parental knowledge about prematurity, the NICU environment, and the perceived level of control over the situation.
Tools of Data Collection
Potential factors influencing stress levels (Independent Variables) included two parts:
Part I: The first section of the questionnaire collected information on the parents’ characteristics, including age, occupation, distance from home to the hospital (whether they live near or far from the hospital), live with a partner, the presence of other living children, prior experiences of having an infant admitted to the NICU, previous neonatal deaths, family structure (extended or nuclear), and income Part II: Characteristics of premature infant: Gestational age, gender, breastfeeding, the use of mechanical ventilation, the number of days hospitalized, mode of delivery, and the age at which they were admitted to the NICU. Part III: The PSS, originally developed by Miles et al. (1993), was adopted by the researcher and subsequently translated into the Arabic language by the authors to make it suitable for our sample. This widely used tool in neonatal literature has demonstrated high validity and reliability. Measure parental stress levels as the dependent variable. The PSS: NICU comprises 45 items, which are categorized into four subscales and a general stress item. These subscales include Sights and Sounds (5 items), Infant Appearance (19 items), Parent-infant Relationship (10 items), and Staff (11 items).
In the Parental NICU stress model (Wereszczak et al., 1997) NICU environment stressors directly influence parents’ stress response. Four major NICU environment stressors were identified and described in detail by Miles et al. (1993). This scale has been widely used in the neonatal literature and has been shown to have high validity and reliability.
Participants were instructed to assess each item by indicating how stressful the described situation was for them, utilizing a scale that ranged from 1 (representing “not at all stressful”) to 5 (indicating “extremely stressful”), following the format established by Miles et al. in 1993. The final score was computed by summing the scores of their responses. Stress, in this context, was defined as the experience of feelings such as anxiety, upset, or tension. In instances where participants had not encountered a specific situation, they were directed to mark it as “not applicable.” For participants with multiple infants in the unit, they were asked to respond to the questions on the scale in relation to the most relevant infant.
To assess stress levels, the total scores of the items were categorized into two groups: high stress (scores ranging from 135 to 225) and low stress (scores ranging from 45 to 134). The internal consistency reliability of the scale was evaluated using Cronbach's α coefficient, which showed a high level of reliability with α = 0.875.
Fieldwork
Researchers interacted with NICU staff to gain permission to approach parents for study participation. Parents were approached at their infant's bedside during assigned visitation hours by the researcher who introduced themselves and provided a brief verbal overview of the study. A printed information sheet was given to parents outlining the study purpose, risks/benefits, voluntary participation, confidentiality practices, and researcher contact information. Parents were given time to read the information sheet and ask any questions about the study before being asked to provide written informed consent by signing a form. Consenting parents completed printed questionnaires in a private consultation room adjacent to the NICU. Data collection involved face-to-face interviews and the completion of questionnaire forms. Subsequently, parents were requested to complete the questionnaire forms, a process that typically took approximately 20 min. Upon finishing, parents were thanked for their time and reminded they could request their data be withdrawn even after participation by contacting the researcher.
Ethical Considerations
The study received ethical approval from the institutional review board of the Faculty of Nursing under the ID NUR1.June.2023. Participation in the study was entirely voluntary, and parents were assured that their responses would not affect the care provided to their infants. Parents were given the freedom to withdraw from the study at any point. Written informed consent was obtained from parents after explaining the study's objectives and the tools involved. The researchers refrained from applying any pressure or incentives to encourage questionnaire completion. Respondents filled out the questionnaire anonymously, and the collected data were treated with strict confidentiality and exclusively utilized for research purposes.
Statistical Analysis
The data was analyzed using the Statistical Package for the Social Sciences (SPSS Inc., version 27; IBM Corp., Armonk, NY, USA) on a personal computer. Descriptive statistics were employed to outline participants’ demographic details. Categorical variables were presented as frequencies and percentages, while continuous variables were expressed as means and standard deviations. Binary logistic regression was used to assess the odds ratio. This statistical method is commonly used for binary outcome variables, such as “High” and “Low” stress. The odds ratio measures the association between independent variables (predictors) and the likelihood of the outcome occurring. Multiple linear regression was employed to model the relationship between two or more independent variables and a continuous dependent variable. A statistical significance level of p < .05 was established.
Results
The study population is described in Table 1. More than half of the parents (57.7%) fell within the 30 to 40-year-old age group, with an average age of 32.81 (5.72) years. Moreover, the majority of parents (97.3%) cohabited with their partners, and approximately three-quarters (76.3%) resided a significant distance from the hospital, encompassing both urban and rural areas. In terms of employment, more than two-thirds (68.1%) of the parents were employed. Furthermore, about two-thirds (66.8%) of the parents had living children, while only a minority (14.1%) had a previous infant who required admission to the NICU. A large proportion of parents (88.4%) visited the NICU daily. Additionally, the majority of parents (74.6%) lived in nuclear families, and more than two-thirds (69.2%) reported having sufficient income.
Characteristics of Studied Parents (n = 743).

Table 2 provides an overview of the characteristics of the studied infants. The majority of infants (86.5%) were premature, and of those, 60.6% were female. In terms of hospitalization duration, more than half of the infants (56.1%) stayed in the hospital for 1–5 days. Furthermore, 39.1% of the infants were delivered via cesarean section, and 60.3% of them were admitted to the NICU within the first week of life.
Characteristics of Studied Infants (n = 743).

Based on the infants’ diagnoses, Figure 1 shows that 40.1% of them were diagnosed with respiratory distress syndrome (RDS), 24.4% with jaundice, 12.1% with sepsis, and 9.1% with birth asphyxia.

Diagnosis of studied infants.
According to the stress levels among parents, the majority of parents reported high stress in the following domains: sight and sound (80.3%), infants’ appearance (69%), and parent-infant relationship (81.4%). Additionally, about three-quarters (73.6%) of parents experienced high stress overall, with a mean score of 167.56 (21.3). For more detailed information, please refer to Table 3.
Stress Levels Experienced by Parents of Infants (n = 743).

Regarding the Odds Ratio for parents’ stress, Table 4 reveals that parents of infants delivered through C/S were 1.4 times more likely to be stressed in comparison to normal delivery (p = .0051). Parents of premature infants were 5.5 times more likely to be stressed in comparison to near-term infants (p < .0001). Infants connected to mechanical ventilation (MV) increased parents’ stress by 3 times (p = .0016). Breastfeeding for infants decreased parental stress by 4.1 times (p = .00001). Increasing days of hospitalization beyond 5 days made parents 1.7 times more likely to be stressed (p = .009). Mothers were 1.5 times more likely to be stressed than fathers. Parents living far from hospitals were 3.1 times more likely to be stressed (p < .0001). Additionally, previous neonatal death and insufficient income increased the risk of parental stress by 3.2 and 1.4 times, respectively. Despite being statistically insignificant, male infants (p = .731), working parents (p = .6344), living away from a partner (p = .5139), and nuclear family setup (p = .7372) were found to be more likely to exhibit stress (Figure 2).

Odds ratio for parents’ stress.
Odds Ratio for Parents’ Stress.
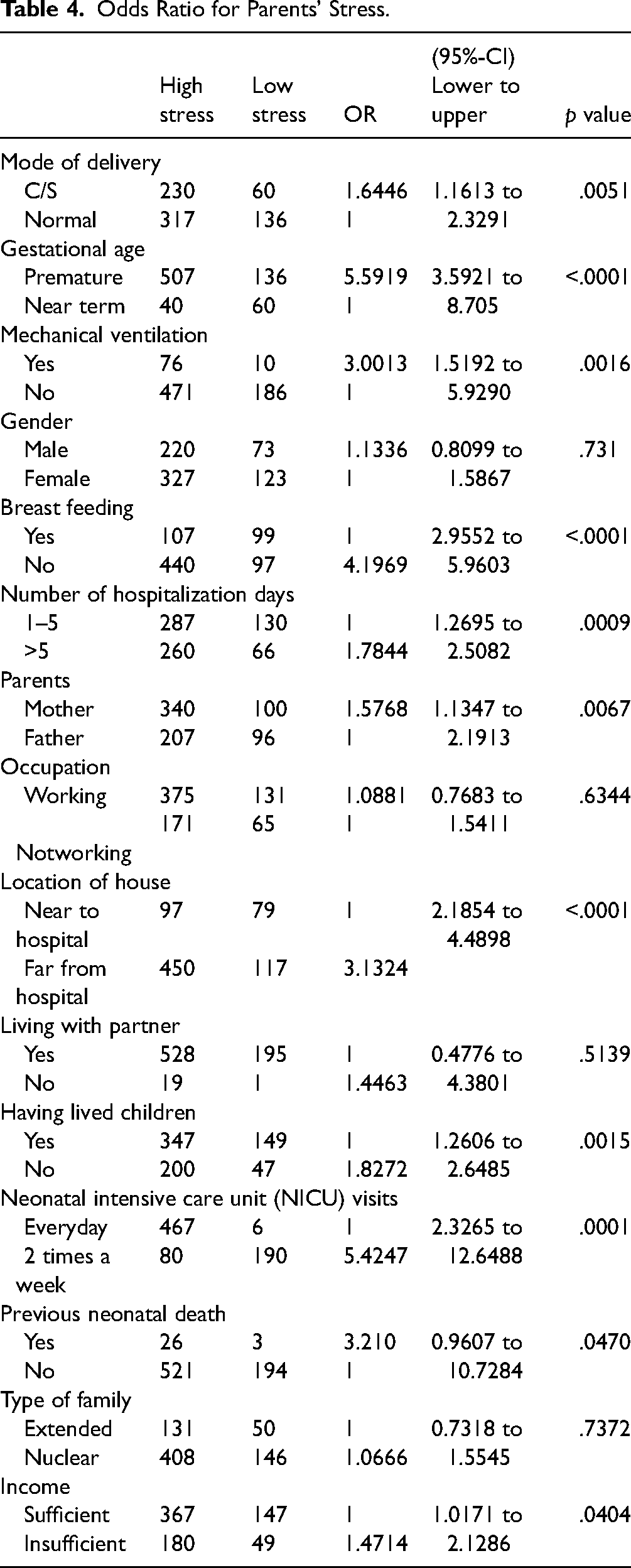
Table 5 reveals the presence of a highly significant model, as indicated by the F-test result of 119.65 with a p-value of .000. This model explains 90% of the variation in parental stress, with an R-squared value of 0.896. Furthermore, it demonstrates that the domain of infant appearance has a strong predictor of stress with B 0.503 and Beta 0.320, followed by the domain of parent-infant relations at B 0.466 and Beta 0.352, staff domain B 0.315 and Beta 0.219. While sight and sounds are weak predictors at B 0.280 and Beta 0.136.
Multiple Linear Regression for Total Stress.

Table 6 demonstrates strong, statistically significant positive correlations between total stress scores and all four domain subscale scores from the Parental Stressor Scale. The highest correlation is seen between total stress scores and the Infant Appearance subscale (r = .917, p < .001), followed by the Parent-Infant Relationship subscale (r = .876, p < .001).
Correlation between Domains and Total Stress.

Discussion
Our study aimed to examine the stress levels experienced by parents of premature infants in the NICU and explore the factors associated with parental stress in this specific context. The study revealed that a majority of parents reported high levels of stress in specific domains, including the sensory environment, the appearance of their infants, and the parent-infant relationship. Furthermore, an overwhelming three-quarters of the parents experienced high overall stress levels.
These results emphasize the substantial emotional burden parents may experience during the neonatal period. The identified domains in the study shed light on the factors contributing to parental stress, including the sensory environment in the NNU, concerns about their infants’ physical appearance, and interactions with healthcare staff.
The highest correlation is seen between total stress scores and the Infant Appearance subscale (r = .917, p < .001), followed by the Parent-Infant Relationship subscale (r = .876, p < .001). This indicates that parents’ perceptions of their infant's appearance and their relationship with their infant are most closely associated with their overall stress levels.
Ionio et al. (2019) found that the mothers and fathers in their study experienced high stress related to infant behavior and appearance, as well as the sight and sound domains. Similarly, Abd Elrahman Mahmoud et al. (2022) reported that in their study, most mothers experienced high stress related to infant appearance, parent-infant relationship, and healthcare staff behaviors. Furthermore, Ansari et al. (2022) identified stress among mothers across four domains of the scale.
These results are in line with previous research. Çekin and Turan (2018) studied 101 parents of premature babies in a university hospital's NICU and found high-stress levels among parents with infants in the NICU. Ganguly et al. (2020) reported that 60.8% of parents experienced severe and extreme stress levels. Similarly, Syamsu et al. (2021) mentioned that almost all mothers found their experience with their premature baby in the hospital extremely stressful (97.1%). Meanwhile, Pathak et al. (2022) reported that the majority of parents experienced moderate stress (93.3%).
Our study identifies significant factors associated with parental stress during neonatal hospitalization. The findings emphasize that certain circumstances contribute to increased stress levels among parents. Specifically, parents of infants delivered through C-section and parents of premature infants are particularly vulnerable, facing higher risks of experiencing stress. These results attributed to Premature infants may require specialized medical care and an extended stay in the NICU, leading to feelings of uncertainty, helplessness, and anxiety among parents. According to Herini et al., 2022 mentioned that Parents with a preterm baby express feelings of sadness, fear, hopelessness, anger, insecurity, stress, and guilt that make them cry and have hindered interactions with their baby. Also, align with Akkoyun & Tas Arslan (2019), who reported that the most common causes of parental stress were middle–low income, C-section deliveries, newborns on ventilator support, and parenteral feeding.
The presence of MV in infants and prolonged hospitalization beyond 5 days also contribute significantly to parental stress. On the other hand, breastfeeding is identified as a protective factor, reducing parental stress. Furthermore, mothers are more likely to experience higher levels of stress compared to fathers, and parents living far from hospitals are at an increased risk of stress. Risk factors such as previous neonatal death and insufficient income are associated with heightened parental stress, highlighting the importance of addressing these challenges and providing appropriate support. Although factors such as male infants, working parents, living away from a partner, and a nuclear family setup show a tendency toward increased stress, their statistical significance was not established.
Moreover, Varma et al. (2019) found that higher maternal stress was associated with mothers’ perception of the baby's discomfort, lower birth weight, and infants on ventilators. Ionio et al. (2019) mentioned that factors affecting mothers’ stress included young age and the baby's need for respiratory support. For fathers, their own young age and the baby's lower gestational age and worse condition at birth were significant predictors of stress and negative feelings. Robinson et al. (2020), in their systematic review, reported that low gestational age and very low birth weight were the most common causes of parental stress.
Our study indicated that the level of stress among mothers is higher than fathers and that the distance between home and the hospital causes increased stress. Also, allowing a higher number of visits helps reduce the rate of stress among parents. Also, we used the Odds ratios which provide a measure of association between an exposure and an outcome.
Additionally, Syamsu et al. (2021) mentioned that high-stress levels were found among parents whose babies had a young gestational age, low birth weight, and were on a respiratory device. Conversely, Ansari et al. (2022) reported no statistically significant difference in mean stress scores for maternal gravida, mode of delivery, and length of stay.
Implication for Practice
According to Lazarus and Folkman, there are two aspects to managing a stressful situation: Problem-based coping and Emotion-based coping
Providing parents with accurate information, reassurance, and guidance to alleviate stress associated with infant appearance concerns. Educating parents on effective bonding, communication, and attachment strategies can be beneficial in reducing stress levels among parents. Providing training and support to healthcare professionals in dealing with stressed parents can contribute to a more positive experience for both parents and staff. Strategies for managing environmental factors in healthcare settings, such as noise levels and visual stimuli as applying healing environment.
Conclusion
The majority of parents participating in the study reported experiencing high levels of stress in specific domains, including the sensory environment, the appearance of their infants, and the parent-infant relationship. Furthermore, an overwhelming three-quarters of the parents experienced high overall stress levels.
The infant’s appearance had the most frequent and pronounced impact on parent stress, followed by the domain of parent-infant relations. The interaction and communication with the staff also played a notable role, and the sensory aspects of the NICU.
Factors that were found to affect parents’ stress levels included having premature infants, infants connected to mechanical ventilators, previous neonatal death, parents living far from hospitals, infants delivered through C-section, insufficient income, and prolonged hospitalization beyond 5 days. These factors were identified as particularly vulnerable, increasing the risks of experiencing stress. Mothers were more likely to experience higher levels of stress compared to fathers. However, breastfeeding, visiting the baby every day, having living children, and living with a partner were identified as protective factors, reducing parental stress.
Recommendations
Provide education and counseling for parents regarding their baby's condition, NICU equipment, and how to best participate in their care. Train nurses in therapeutic communication skills to offer emotional support to families. Facilitate skin-to-skin kangaroo care as soon as the baby is stable to enhance bonding. Minimize separation between parents and their baby. Encourage self-care and peer support for parents to prevent burnout. Furthermore, further research in this area is warranted to explore additional factors and develop comprehensive approaches to support parents in managing and coping with stress effectively.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.