
Abstract
Background
Tokophobia, or fear of childbirth, is a significant psychological concern for female oncology patients, particularly those considering fertility preservation therapies.
Aim
This study investigates the relationships between perceived barriers, knowledge of fertility preservation therapies, psychological capital, and tokophobia and explores the moderating role of psychological capital in these relationships.
Methods
Cross-sectional quantitative research was conducted among 312 female oncology patients. Data were collected using validated scales to measure barriers, knowledge, psychological capital, and tokophobia. Descriptive statistics, correlation analysis, and moderation analysis using the PROCESS macro for SPSS examined the role of psychological capital in moderating the relationship between knowledge and tokophobia.
Results
The study revealed that female oncology patients perceived multiple barriers to fertility preservation, with the total barriers score averaging 75.11 ± 18.1. Subscale means were personal (20.04 ± 4.3), medical (21.56 ± 5.8), relational (13.61 ± 4.1), and financial barriers (19.89 ± 5.5). These barriers were negatively associated with total psychological capital (PsyCap) (r = –.124, p < .05), particularly resilience (r = –.163, p < .01) and optimism (r = –.096, p < .05). Knowledge of fertility preservation (mean = 18.28 ± 4.2) was positively associated with PsyCap (r = .262, p < .01). Moderation analysis showed that PsyCap significantly moderated the relationship between knowledge and tokophobia (β = –0.034, p = .001).
Conclusion
This study highlights the complex interplay between knowledge, psychological capital, and tokophobia among female oncology patients. While knowledge of fertility preservation therapies can heighten tokophobia in patients with low psychological capital, it may reduce tokophobia in those with high psychological capital.
Keywords
Introduction
Fertility preservation (FP) therapies have emerged as a critical component of comprehensive cancer care (Hildingsson et al., 2024), offering female oncology patients the opportunity to safeguard their reproductive potential amidst the challenges of cancer treatment (Kapoor et al., 2024) Advances in medical science have significantly improved cancer survival rates (Tran et al., 2021), yet many treatments, including chemotherapy and radiotherapy, pose a substantial risk to fertility (Dudasova et al., 2021). Consequently, addressing fertility concerns is essential to improving female cancer survivors’ quality of life and holistic well-being (Örtegren et al., 2023).
Despite the growing recognition of FP therapies, barriers to their utilization persist. These barriers may include a lack of awareness, cultural and financial constraints, insufficient communication between patients and healthcare providers, and limited access to specialized services (Gilbert et al., 2021). Moreover, psychosocial factors, such as tokophobia (fear of pregnancy and childbirth; Kitamura et al., 2024) and psychological capital (PsyCap)—a positive psychological resource encompassing hope, resilience, optimism, and self-efficacy (Newman et al., 2014) may further influence patients’ attitudes and decision-making regarding FP options.
Tokophobia, though primarily studied in obstetric populations, may also affect female oncology patients’ perceptions of future childbearing (Ben-Rafael et al., 2023), particularly in the context of their cancer journey. On the other hand, psychological capital has been shown to enhance coping mechanisms and foster adaptive responses in the face of health adversities (Zoromba et al., 2024). Investigating the interplay between these psychosocial factors and knowledge and barriers toward FP therapies offers a nuanced understanding of patient needs and the support required to address them. Hence, this study aims to explore the levels of knowledge about FP therapies, identify barriers to their uptake, and examine their association with tokophobia and PsyCap among female oncology patients. By shedding light on these relationships, the findings had the potential to contribute to designing targeted interventions that enhance patient education, alleviate psychological distress, and promote equitable access to fertility preservation services, ultimately supporting the reproductive autonomy and psychological well-being of female cancer patients.
Review of Literature
FP therapies refer to medical interventions and techniques to safeguard an individual's reproductive potential, particularly in conditions or treatments that could impair fertility (Pathak et al., 2025). These therapies are especially relevant for individuals undergoing cancer treatments such as chemotherapy, radiation, or surgery, which often pose a high risk of infertility. FP options include cryopreservation of sperm, eggs, embryos, or ovarian tissue and gonadal shielding during radiation and ovarian transposition. Advances in reproductive medicine have expanded the availability and effectiveness of these therapies, allowing individuals to preserve their fertility and improve their quality of life (Li et al., 2024; Rodriguez-Wallberg et al., 2023).
Despite the potential benefits of FP therapies, there are significant barriers to their utilization, including limited knowledge among patients and healthcare providers, financial constraints, and inadequate access to specialized services (Chen et al., 2023; Ko et al., 2023). Many individuals remain unaware of their options for fertility preservation, particularly in time-sensitive scenarios like a recent cancer diagnosis (Jones et al., 2022). Additionally, healthcare providers may lack sufficient training or confidence in discussing FP with patients, further contributing to missed opportunities for intervention (Drost et al., 2023). Cultural beliefs, stigma, and logistical challenges, such as the availability of FP facilities, also limit uptake (Adamson et al., 2024). Understanding the knowledge gaps and barriers to FP therapies is essential for developing targeted educational programs, improving healthcare provider training, and implementing policies that enhance access to these critical services (Benedict et al., 2021).
Tokophobia, the intense fear or anxiety of pregnancy and childbirth, is a psychological condition that can profoundly impact women's reproductive health decisions (Striebich et al., 2018). For female oncology patients, this fear may be exacerbated by the physical and emotional challenges associated with their cancer diagnosis and treatment (Watson et al., 2021). The potential impact of cancer therapies on fertility, combined with concerns about the risks of pregnancy after cancer treatment, can amplify tokophobic tendencies (Farhat et al., 2023). Female oncology patients may experience heightened anxiety about their ability to conceive, carry a pregnancy, or endure childbirth safely (Klijn et al., 2023), which may lead to avoidance of FP discussions or decisions. Tokophobia in this population represents a complex interplay of psychological, physical, and medical factors that must be addressed holistically (Ibrahim Ali et al., 2024).
In this context, PsyCap plays a critical role in shaping the attitudes and behaviors of female oncology patients toward FP therapies (Guardini et al., 2023). PsyCap, defined by self-efficacy, optimism, hope, and resilience, equips individuals with the psychological resources to navigate complex and emotionally charged decisions, such as fertility preservation (Newman et al., 2014). High levels of PsyCap can help patients manage fears by fostering a sense of control and positivity about their reproductive future (Yıldırım et al., 2021). Moreover, PsyCap can empower patients to use problem-focused coping strategies (Cui et al., 2021). Integrating interventions to enhance PsyCap in female oncology patients may mitigate the impact of psychological barriers and improve the overall quality of life (Guo et al., 2022).
Method
Study Design and Setting
A cross-sectional quantitative research design was utilized for this study, adhering to the STROBE checklist for cross-sectional studies to ensure methodological rigor. The study was conducted at the outpatient clinics of the El-Minia Cancer Center, located in El-Minia City, Egypt. This center is a vital healthcare hub for cancer diagnosis, treatment, and follow-up care, catering to a diverse patient population from El-Minia and surrounding governorates. It provides a wide range of specialized oncology services, including chemotherapy, radiotherapy, surgical oncology, and palliative care, making it a comprehensive center for cancer management in the region.
Research Questions
What is the level of knowledge about fertility preservation therapies among female oncology patients?
What is the relationship between perceived barriers, fertility preservation knowledge, psychological capital, and tokophobia among female oncology patients?
Does psychological capital moderate the relationship between knowledge of fertility preservation therapies and tokophobia in female oncology patients?
Sample
The study targeted female oncology patients who were either receiving or planning to receive treatments that could potentially impact fertility, such as chemotherapy, radiation therapy, or surgical interventions.
Inclusion and Exclusion Criteria
Eligible participants were female oncology patients who were either receiving or planning to receive treatments that could potentially impact fertility, such as chemotherapy, radiation therapy, or surgical interventions. To ensure relevance to fertility preservation, participants were required to be of childbearing age, not currently pregnant, and willing to participate in the study.
Participants were excluded if they had previously undergone fertility preservation procedures, as this could influence their knowledge and perceptions regarding fertility preservation therapies. Additionally, individuals with severe cognitive impairments that could interfere with their ability to understand and complete study assessments were excluded. Those with severe psychiatric conditions that could confound the results related to tokophobia or psychological capital were also not included. Furthermore, women with severe comorbid medical conditions that could hinder study participation, those who were currently pregnant, or those who had reached postmenopausal status were excluded from the study.
Sample Size Calculation
The sample size was established using the G*Power 3.1.9.7 software (Geller et al., 2025). The calculation parameters were set at a power of .95, an alpha level of .001, and a moderate effect size of 0.15. These parameters indicated that a minimum of 304 participants was necessary. To accommodate potential dropouts, the sample size was increased to 330 participants. Finally, 312 valid questionnaires were collected and used for the final analysis.
Instruments
Questionnaire for Sociodemographic and Clinical Characterization
It includes sociodemographic data such as age, education level, marital status, residence, family structure, employment status, and income. Additionally, it explores medical history, including chronic diseases and cancer history. Lifestyle factors are also evaluated, covering exercise habits, dietary regimen, sleep patterns, smoking behavior, and exposure to passive smoking (Amin et al., 2024a).
Psychological Capital Scale
A revised, shorter version of the Compound Psychological Capital Scale-12 (CPC-12) was used to assess psychological capital (Duffin et al., 2024; Linkeviciute et al., 2014). This scale measures four key dimensions: self-efficacy, hope, resilience, and optimism, with each dimension represented by three items. Responses are rated on a 6-point Likert scale ranging from 1 (strongly disagree) to 6 (strongly agree), with higher scores indicating a greater degree of psychological capital. Example items include: “I am confident that I could deal efficiently with unexpected events” (self-efficacy), “The future holds a lot of good in store for me” (optimism), “I tend to bounce back quickly after serious life difficulties” (resilience), and “I can think of many ways to reach my current goals” (hope).
In the current study, the Cronbach's alpha was .99, indicating excellent reliability. An exploratory factor analysis (EFA) was conducted to assess the scale's validity. The factor loadings ranged from .512 to .715 before rotation and improved to between .552 and .878 after varimax rotation, exceeding the recommended threshold of .35. Bartlett's Sphericity Test was significant (p < .001), confirming that the data were appropriate for factor analysis. Additionally, the Kaiser–Meyer–Olkin (KMO) measure of sampling adequacy was .885, supporting the suitability of the factor model. Together, the identified factors accounted for 67.547% of the total variance.
The Tokophobia Severity Scale
The Tokophobia Severity Scale (TSS) was developed by Wootton et al. (2020) to assess the severity of tokophobia, an intense fear of pregnancy and childbirth. The scale consists of 13 items rated on a 4-point Likert scale ranging from 0 (not at all) to 3 (always), with higher total scores indicating higher anxiety levels about pregnancy and childbirth. The TSS demonstrated excellent internal consistency (α = .93). Convergent validity was established through a significant medium correlation with the Wijma Delivery Expectancy/Experience Questionnaire (W-DEQ) (rs = .44, p < .001). Divergent validity was indicated by a significant medium correlation with the Patient Health Questionnaire-9 (PHQ-9) (rs = .35, p < .001). This study confirmed internal consistency with a Cronbach's alpha of .887, indicating strong reliability.
After translating the scale from English to Arabic, an EFA was conducted to assess its content validity. Factor loadings ranged from .523 to .988 before rotation and improved to .513 to .915 after varimax rotation, exceeding the recommended threshold of .35. These factors collectively accounted for 78.151% of the total variance, demonstrating strong construct validity.
The KMO measure of sampling adequacy was .903, indicating excellent suitability for factor analysis. Additionally, Bartlett's Test of Sphericity was statistically significant (p < .001), confirming that the correlation matrix was appropriate for factor analysis. As a result, all items on the scale were retained.
Fertility Preservation Knowledge Scale
The Fertility Preservation Knowledge Scale, adapted from Faul et al. (2007), assesses participants’ understanding of fertility preservation (FP) therapies. The scale consists of two sections that evaluate different dimensions of FP knowledge. The first section comprises nine items that measure participants’ general knowledge of fertility preservation, including awareness of FP options for males and females, potential side effects, and the availability of FP service centers in Egypt. Responses are recorded as Yes/No, with a “Yes” response assigned 1 point and a “No” response assigned 0 points. The total score for this section ranges from 0 to 9 points, with higher scores indicating greater familiarity with FP concepts. The second section consists of five items that explore factors influencing the use of FP services. These items are rated on a 4-point Likert scale: 1 (Never), 2 (Rarely), 3 (Usually), and 4 (Greatly). The total score for this section ranges from 5 to 20 points, with higher scores reflecting a greater perceived influence of various factors on FP decision-making. The total knowledge score is calculated by summing the scores from both sections, resulting in a possible range of 5 to 29 points. A higher total score indicates a greater overall understanding and awareness of fertility preservation therapies, highlighting participants’ level of knowledge in this domain.
Survivorship Oncofertility Barriers Scale
The Survivorship Oncofertility Barriers Scale (SOBS), developed by Hussein et al. (2020), assesses the barriers female cancer survivors face in achieving motherhood post-treatment. The scale comprises 22 items distributed across four subscales: personal barriers (6 items), medical barriers (6 items), relational barriers (4 items), and financial barriers (6 items). Each item is rated on a five-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree), with higher total scores indicating a greater perception of barriers to achieving motherhood after cancer treatment.
In terms of reliability and validity, prototype testing demonstrated acceptable internal consistency (Cronbach's alpha = .71) and test–retest reliability (intraclass correlation coefficient = .70). Known-group validity was supported by the scale's ability to discriminate between age groups (p = .02) and years since diagnosis (p = .01). Additionally, the financial subscale showed a significant correlation with the Economic Strain and Resilience in Cancer measure of financial toxicity (ρ = 0.39, p < .001). In this study, internal consistency was further confirmed with a Cronbach's alpha of .885, indicating strong reliability.
Following the translation of the scale from English to Arabic, an EFA was conducted to assess content validity. Factor loadings ranged from .450 to .970 before rotation and improved to .500 to .890 after varimax rotation, all exceeding the threshold of .35. The extracted factors collectively accounted for 76.25% of the total variance. The KMO measure of sampling adequacy was .895, confirming excellent suitability for factor analysis. Additionally, Bartlett's Test of Sphericity was statistically significant (p < .001), supporting the factorability of the correlation matrix. As a result, all items on the scale were retained.
Study Procedures
Tool Preparation and Pilot Study
The translation process of the research instruments, which included the Psychological Capital Scale, the TSS, the SOBS, and the Fertility Preservation Knowledge Scale, into Arabic was conducted with meticulous care. Bilingual experts proficient in both English and Arabic played a crucial role in ensuring accurate and culturally appropriate translations. To validate the translations, the translated versions were back-translated into English to confirm linguistic equivalence and address any discrepancies. Following the translation and back-translation stages, face validity assessments were performed for each instrument. Expert panels in the respective fields reviewed the translated tools to ensure they effectively captured the intended constructs within the Arabic context. To further validate the instruments, feedback from potential participants was sought to confirm the clarity, relevance, and cultural appropriateness of the translated items.
Reliability measures were subsequently implemented, with internal consistency reliability assessed using statistical methods such as Cronbach's alpha to ensure the consistency of items within each scale. Before conducting the main study, a pilot study was carried out to assess the feasibility, reliability, and validity of the survey instruments and procedures. This preliminary phase aimed to identify potential issues in the study design and refine the data collection tools. The pilot study involved a sample of 30 female oncology patients who were excluded from the main study. The results showed that all questions were clear and comprehensible, with no reported confusion. Participants found the length and sequence of the questionnaire to be manageable and logical. Based on these findings, it was determined that the study tools were well-suited for the main study and did not require any modifications. This pilot study was essential in confirming the adequacy and reliability of the instruments, thereby enhancing the overall validity of the research.
Data Collection
Data collection for this study was conducted over 3 months, from July to September 2024. Before initiating the process, the researchers also secured the necessary administrative permissions from the participating healthcare facilities where the cancer survivors received treatment or follow-up care. Eligible participants were identified through patient records, and potential participants were approached during their routine visits to oncology clinics or through direct communication facilitated by healthcare providers. To foster transparency and trust, the researchers provided each participant with a clear explanation of the study's objectives.
To ensure a comfortable environment for participants, data collection was carried out in private, quiet settings, such as dedicated consultation rooms within oncology clinics. Participants were given the option to complete the questionnaire in either a self-administered format or with the assistance of a trained researcher. The process took approximately 20 to 30 minutes per participant. To enhance data quality, the researchers conducted routine checks for incomplete responses and addressed any ambiguities in real time.
Ethical Approval and Informed Consent to Participate
Approval for this study was obtained from the Research Ethics Committee of the Faculty of Nursing at El-Minia University, Egypt, under code number (REC202482). The well-being and rights of all participants were rigorously safeguarded in adherence to local laws, regulations, and the ethical principles outlined in the Declaration of Helsinki. Clear and comprehensive information about the study objectives was provided to all participants. They were explicitly informed that participation was voluntary and anonymous. Participants were assured that all data collected would be kept strictly confidential and accessible only to authorized members of the research team. Before data collection began, participants provided written consent. It was emphasized that participants had the right to withdraw from the study at any time without any obligation.
Statistical Analysis
All statistical analyses were conducted using IBM SPSS Statistics version 28. Descriptive statistics, including frequencies, percentages, means, and standard deviations, were used to summarize the sociodemographic and clinical characteristics of the participants and the key study variables. The normality of the data was confirmed. Pearson's correlation coefficients were calculated to identify significant associations among barriers, knowledge, psychological capital, and tokophobia. To examine the moderating role of psychological capital in the relationship between knowledge and tokophobia, a moderation analysis was conducted using the PROCESS macro (version 4.2) Model 1 in SPSS, with knowledge as the independent variable, psychological capital as the moderator, and tokophobia as the dependent variable. The interaction term (knowledge × psychological capital) was included in the model, and conditional effects were calculated at three levels of psychological capital: low (16th percentile), moderate (50th percentile), and high (84th percentile). Bootstrapping with 5,000 resamples was used to generate bias-corrected confidence intervals (CI) for the moderation effects, with significance determined at 95% CI. All statistical tests were two-tailed, and statistical significance was defined as p < .05.
Results
Table 1 presents the sociodemographic and clinical characteristics of the 312 female oncology patients. The majority were aged over 30, with 30.8% in the 30–40 age group. Regarding educational attainment, 31.7% had a university education, followed by 27.6% with secondary education, and 26.9% with basic education. In terms of marital status, 50.6% were married, 36.9% were widowed or divorced, and 12.5% were single. More than half (52.9%) resided in rural areas. Most participants (73.7%) were from nuclear families, with 26.3% reporting an extended family structure.
Sociodemographic and Clinical Characteristics of Participants (N = 312).
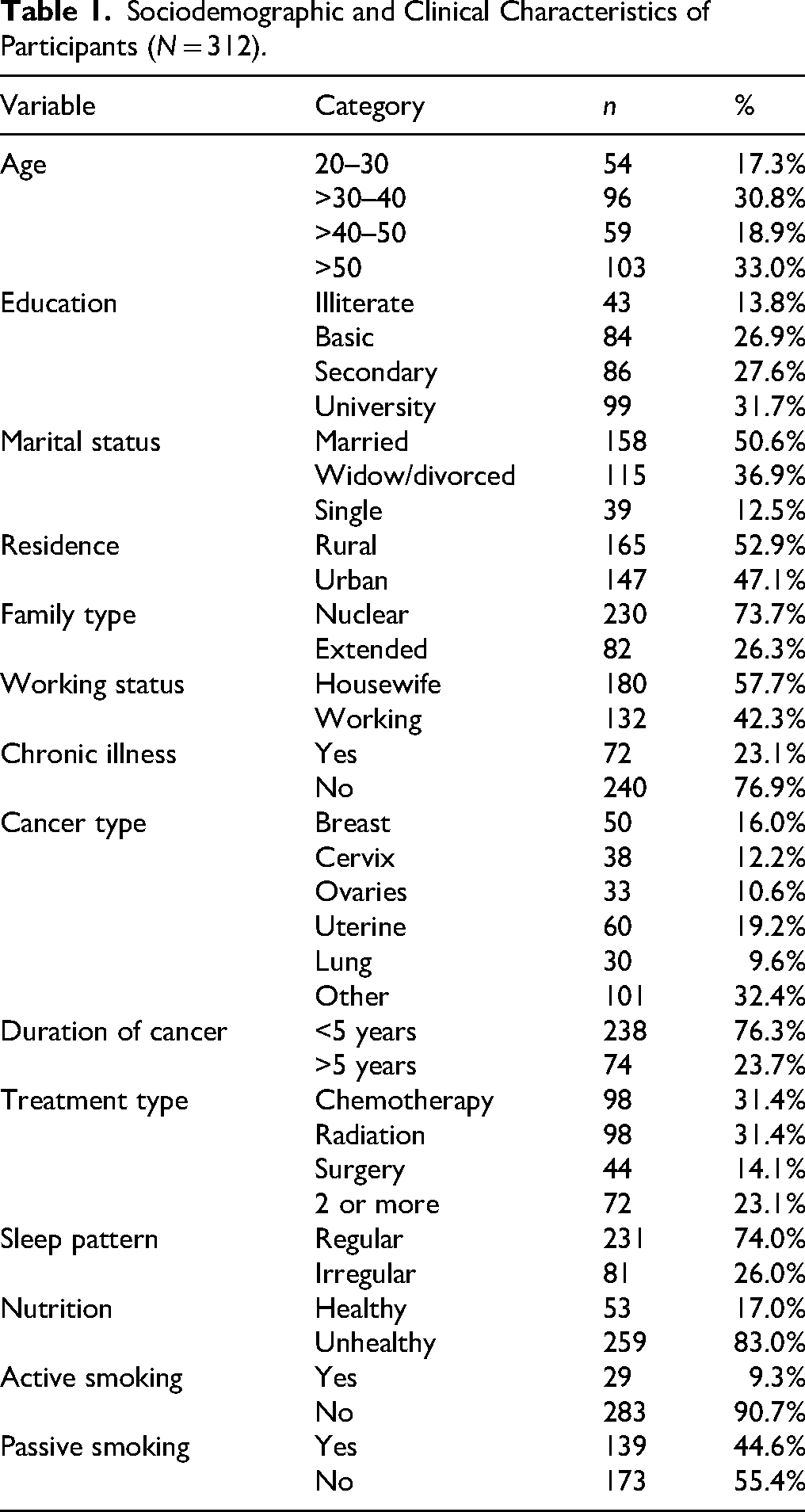
Cancer types varied, with “other cancers” (32.4%), uterine cancer (19.2%), and breast cancer (16.0%) being most common, followed by cervical (12.2%), ovarian (10.6%), and lung cancer (9.6%). Most participants (76.3%) had lived with cancer for less than 5 years, while 23.7% had had cancer for more than 5 years. Treatment types were evenly distributed among chemotherapy (31.4%), radiation therapy (31.4%), a combination of two or more modalities (23.1%), and surgery alone (14.1%).
The correlation matrix (Table 2) provides descriptive statistics for key variables: total barriers (75.11 ± 18.1), with subscale scores for personal (20.04 ± 4.3), medical (21.56 ± 5.8), relational (13.61 ± 4.1), and financial barriers (19.89 ± 5.5); knowledge (18.28 ± 4.2), with subscale scores for general knowledge (5.82 ± 1.9) and factors influencing fertility preservation use (12.46 ± 2.8); tokophobia (18.45 ± 10.3); and total psychological capital (34.37 ± 12.5). Total barriers showed strong positive correlations with its subdimensions (all r > .85, p < .01) but were negatively associated with total psychological capital (r = −.124, p < .05), particularly its resilience and optimism dimensions (see Table 2).
Correlation Matrix Between Studied Variables (N = 312).
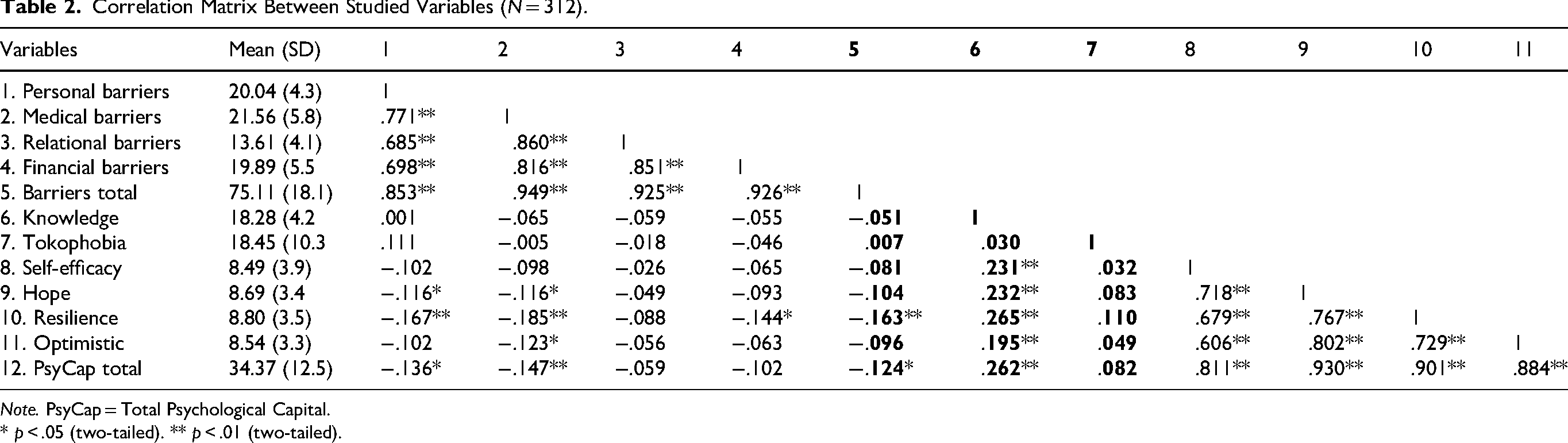
Note. PsyCap = Total Psychological Capital.
* p < .05 (two-tailed). ** p < .01 (two-tailed).
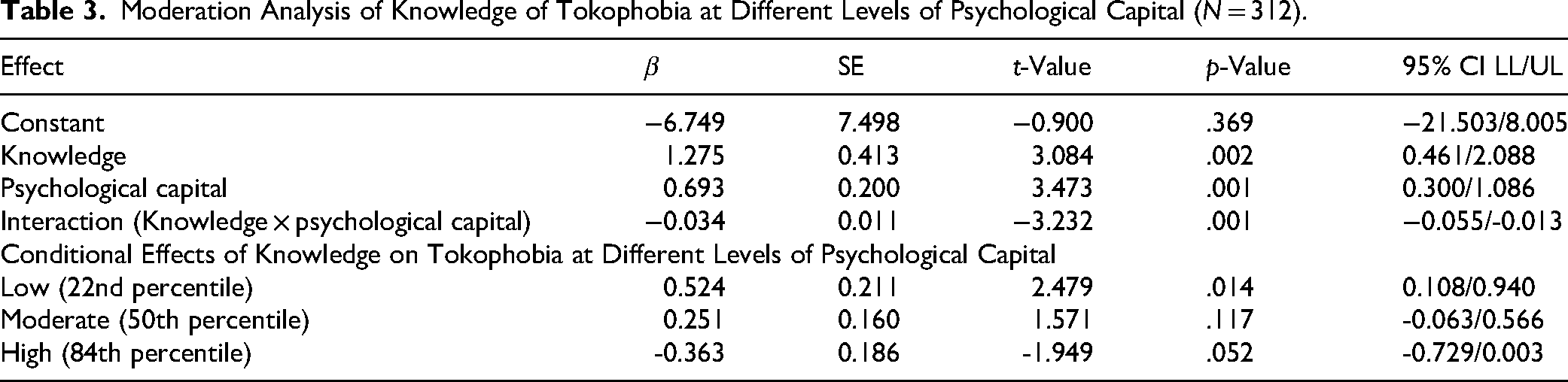
Table 3 presents the moderation analysis examining the role of psychological capital in moderating the relationship between knowledge of fertility preservation therapies and tokophobia. The overall model was statistically significant (F = 4.234, p = .006) and accounted for approximately 4% of the variance in tokophobia. The interaction term (knowledge × psychological capital) was significant (β = -0.034, p = .001). At low psychological capital (22nd percentile), knowledge was positively associated with tokophobia (β = 0.524, p = .014). At moderate psychological capital (50th percentile), the effect was weaker and not significant (β = 0.251, p = .117).
Moderation Analysis of Knowledge of Tokophobia at Different Levels of Psychological Capital (N = 312).
Discussion
The findings from this study highlight significant knowledge gaps and barriers related to fertility preservation (FP) therapies among female oncology patients, aligning with previous research. Villarreal-Garza et al. (2021) revealed that while 83% of young breast cancer patients considered it a high responsibility to inform patients about treatment-related infertility risks, only 58% of healthcare providers consistently addressed these risks. Similarly, only 38% always discussed FP options, and just 52% referred patients to fertility specialists. Misconceptions, such as the belief that pregnancy or GnRH analogs are detrimental, were held by 24% of providers, further complicating FP discussions. Key barriers identified included costs, lack of specialists, and prognostic concerns.
Additionally, this study found that 50% of the participants were single, divorced, or widowed, raising important questions about their interest in fertility preservation and the options available to them. While fertility preservation is often associated with patients in stable relationships, many single women, including those without immediate reproductive plans, may still wish to preserve their fertility for future use. Discussions surrounding alternative reproductive options, such as the use of sperm donors, are essential in ensuring that all patients receive comprehensive FP counseling. However, research suggests that these discussions are often overlooked, highlighting the need for healthcare providers to proactively address reproductive concerns for all patients, regardless of marital status.
Baek et al. (2023) observed that physicians in South Korea, other Asian countries, and Latin America exhibited substantial knowledge and favorable attitudes toward FP, positively influencing patient discussions and referrals to reproductive endocrinologists. However, similar to these findings, limitations in human resources and materials posed significant challenges, emphasizing the necessity for a systematic approach to enhance FP practices for young cancer patients.
Moreover, Lorenz et al. (2016) emphasized the critical importance of FP for young cancer survivors, as 70–75% express a strong desire for parenthood despite the significant reduction in fertility post-treatment. However, healthcare professionals often lack sufficient knowledge or harbor biases that hinder practical FP discussions. They advocate for patient-centered fertility counseling, decision support, and personalized care tailored to individuals’ values and goals. These findings underscore the need for improved education and resources for healthcare providers, alongside system-level interventions, to address FP comprehensively and empathetically for female oncology patients.
The findings indicate that perceived barriers to fertility preservation (FP) are significantly and negatively associated with psychological resources such as resilience, optimism, and total psychological capital. These results can be attributed to the interplay between psychological stress, decision-making challenges, and the complex emotions experienced by female oncology patients navigating FP options. Di Mattei et al. (2020) noted that female cancer patients undergoing FP tend to exhibit lower levels of psychological vulnerabilities, such as immature defense mechanisms, depression, and trait anxiety, while displaying higher levels of mature defense mechanisms. This suggests that patients may develop adaptive coping strategies to navigate the stressors of FP. However, the emotional burden of treatment decisions, along with underlying barriers, may still erode their psychological resilience and optimism.
Lawson et al. (2015) highlighted additional factors contributing to psychological distress among FP patients, including pre-existing mental health issues, uncertainty about future relationships, and ethical dilemmas related to treatment. The complexity of these challenges can overwhelm patients, making them feel less capable of managing their situations effectively. Furthermore, barriers such as financial costs, ethical concerns, and treatment expectations (e.g., pregnancy outcomes or risk of miscarriage) may amplify feelings of helplessness and reduce their capacity to maintain positive outlooks.
These findings collectively highlight how the psychological toll of navigating FP decisions, compounded by external barriers, can diminish psychological capital. Addressing these challenges requires targeted interventions, such as providing personalized psychological counseling, fostering emotional support, and minimizing perceived barriers through patient education and healthcare system improvements.
The positive association between tokophobia (fear of childbirth, FOC) and knowledge of fertility preservation (FP) therapies can be understood in the context of heightened anxiety and proactive coping mechanisms among affected individuals. Women with tokophobia may be more motivated to explore and understand FP options as part of their broader effort to manage reproductive health concerns and alleviate fears about future childbirth and related complications. Tokophobia's association with FP knowledge reflects a coping response where women channel their fear into acquiring information about fertility options, seeking control over future reproductive possibilities amidst their concerns. Addressing tokophobia and providing clear, empathetic counseling on FP could help alleviate fear while fostering informed decision-making (Amin et al., 2024b).
Rublein and Muschalla (2022) provide insight into childbirth fear and mindsets. While most women in their study exhibited low fear and a natural or medical mindset, a minority reported higher fear levels regardless of mindset. Despite these differences in fear, knowledge about childbirth and non-medical pain relief approaches was inconsistent across groups. This suggests that fear does not directly equate to comprehensive knowledge, but it may drive some women, particularly those with elevated fear, to seek information actively, aligning with these findings.
Furthermore, Duraes et al. (2022) underscore the importance of FP for young women facing breast cancer treatment. Their study reveals that although the FP rate increased steadily, gamete reuse and live birth rates post-treatment remained low, with most births resulting from spontaneous pregnancies. This highlights the uncertainty and emotional complexity surrounding FP, which may intensify feelings of fear and drive individuals with tokophobia to acquire detailed knowledge about FP as a potential strategy for maintaining reproductive options.
The observed relationship between low psychological capital and increased tokophobia with more excellent knowledge is novel and unique in this research. Hoffman et al. (2023) point out that women with a FOC are particularly vulnerable to anxiety and depression during the perinatal period. Enhanced awareness of fertility preservation challenges might exacerbate this vulnerability by magnifying perceived threats and stressors, potentially overwhelming psychological resources such as self-efficacy and resilience. This suggests that more excellent knowledge, while essential, could inadvertently trigger anxiety when not accompanied by adequate psychological support. Furthermore, Abdolalipour et al. (2023) emphasized that mindfulness-based interventions could mitigate FOC and enhance self-efficacy, highlighting the importance of tailored strategies to address the emotional needs of pregnant women. The findings underscore the need for more targeted and personalized approaches in healthcare settings, as the “one-size-fits-all” strategy may not sufficiently support women experiencing a heightened FOC.
The finding that psychological capital (PsyCap) acts as a buffering moderator in the relationship between knowledge and tokophobia can be explained by its role in enhancing individuals’ ability to manage fear and anxiety. PsyCap, which includes resilience, optimism, hope, and self-efficacy, provides the psychological resources to process potentially distressing information, such as the risks and uncertainties associated with childbirth or fertility preservation (FP). Previous studies support this dynamic. Rublein and Muschalla (2022) found that women with higher childbirth fears often seek information proactively, but without adequate psychological resources, such knowledge may intensify anxiety. PsyCap helps by enabling individuals to view knowledge as empowering rather than fear-inducing.
Resilience and optimism, key components of PsyCap, mitigate the impact of fear by fostering a positive outlook and adaptive coping, as seen in Duraes et al. (2022), where FP offered hope for future fertility despite low reuse and live birth rates. Similarly, hope motivates constructive actions, turning fears into goals, aligning with findings by Di Mattei et al. (2020) on mature defense mechanisms in oncology patients. Furthermore, PsyCap enhances self-efficacy, helping individuals navigate complex FP decisions, such as ethical dilemmas or future uncertainties, as identified by Lawson et al. (2015). By buffering against negative emotions, PsyCap transforms knowledge about FP from a potential trigger of tokophobia into a tool for empowerment, emphasizing the importance of fostering psychological resources alongside informational support.
Limitations of the Study
This study has several limitations that should be considered when interpreting the findings. Firstly, we did not assess the levels of anxiety, stress, or coping mechanisms among the participants. These psychological factors could significantly influence the relationship between knowledge, barriers, psychological capital, and tokophobia. Anxiety and stress, in particular, are known to exacerbate fears related to fertility and childbirth, and their exclusion limits the depth of psychological insights that could have been derived from the study.
Secondly, the study population included a general sample of female oncology patients without distinguishing between specific cancer types. Fertility preservation concerns may vary significantly among patients with different diagnoses, such as breast cancer, cervical cancer, or ovarian cancer, due to variations in treatment regimens, prognoses, and fertility risks. Future research should focus on more specific subgroups of oncology patients to provide tailored insights and recommendations. Although the moderation model revealed statistically significant relationships, the explanatory power of the model was relatively low (R² ≈ 4%). This suggests that the model explains only a small portion of the variance in tokophobia, which limits the practical predictive power of the findings. Further studies are needed to identify additional variables that may contribute to a more comprehensive understanding of the factors influencing tokophobia among female oncology patients.
Additionally, we did not assess patients’ social, emotional, family, or financial support, including insurance coverage. These factors could play a crucial role in their ability to access fertility preservation options and cope with related psychological distress. Their exclusion limits the study's ability to fully capture the broader contextual factors influencing patients’ decisions and well-being.
Another potential limitation of the study is related to data collection. Participants had the opportunity to either self-complete the questionnaire or receive assistance from a third person. This could introduce response bias, as answers may have been influenced by the presence or interpretation of the assisting individual. Future studies should consider standardized administration methods to minimize potential biases and ensure consistency in data collection.
Implications for Practice
The findings of this study highlight the need for integrated interventions that combine educational and psychological support tailored to the specific needs of female oncology patients facing fertility-related decisions. Psychological counseling should prioritize enhancing psychological capital (PsyCap), particularly dimensions such as resilience, optimism, hope, and self-efficacy, which can empower patients to effectively manage tokophobia (Damayanti et al., 2022; Atta et al., 2024a). To promote the development of PsyCap in clinical oncology settings, structured interventions such as strengths-based counseling, cognitive-behavioral therapy (CBT), and guided self-reflection techniques can be integrated into fertility preservation (FP) programs.
These interventions can be delivered through one-on-one sessions or group formats led by trained psycho-oncology specialists or clinical psychologists embedded in oncology care teams.
Structured FP counseling programs must be patient-centered, with a focus on addressing individual fears, personal values, and reproductive goals (Kamhawi et al., 2013). Emotional support and the development of a trusting therapeutic relationship are crucial in alleviating reproductive fears and enabling patients to make informed decisions that align with their long-term aspirations (Atta et al., 2024b). Additionally, the observed association between psychological capital and perceived barriers emphasizes the importance of addressing emotional and cognitive hurdles. Barriers such as high costs, limited availability of fertility specialists, and concerns about disease prognosis significantly hinder the adoption of FP services and should be systematically addressed in clinical practice through interdisciplinary coordination and resource referral systems.
Furthermore, the link between tokophobia and patients’ knowledge of FP therapies suggests that fear plays a central role in shaping awareness and attitudes. Empathy-based counseling and psychoeducational workshops may serve as effective strategies to reduce anxiety, correct misinformation, and support patients in making empowered, informed reproductive decisions (Amin et al., 2025; Elzohairy et al., 2024). Finally, future research should consider the implementation of longitudinal studies to examine how knowledge, perceived barriers, and psychological factors evolve. Such studies would be valuable for establishing causal relationships and understanding the long-term impact of psychological and educational interventions in this vulnerable population.
To improve the model's predictive value in future studies, additional psychological and contextual variables—such as anxiety, coping strategies, perceived social support, and prior childbirth experiences—should be incorporated. These factors may enhance the explanatory power and offer a more comprehensive understanding of the dynamics influencing tokophobia. Finally, longitudinal studies are warranted to examine how knowledge, perceived barriers, and psychological factors evolve, contributing to stronger causal inferences and more targeted interventions in this vulnerable population.
Conclusion
In conclusion, this study highlights the interplay between psychological and educational factors in addressing tokophobia among female oncology patients. By prioritizing psychological well-being and fostering PsyCap, healthcare providers can empower patients to navigate the complexities of FP therapies with confidence and hope. Fear and anxiety driven by tokophobia can drive individuals to actively seek information about fertility options, which reflects their desire to regain control over their reproductive health. Providing empathetic counseling and targeted education could help bridge knowledge gaps, reduce barriers, and foster more confident and informed decision-making in this sensitive area.
Supplemental Material
sj-docx-1-son-10.1177_23779608251376079 - Supplemental material for Fertility-Preservation Knowledge, Perceived Barriers, and Tokophobia Among Female Oncology Patients: The Moderating Role of Psychological Capital
Supplemental material, sj-docx-1-son-10.1177_23779608251376079 for Fertility-Preservation Knowledge, Perceived Barriers, and Tokophobia Among Female Oncology Patients: The Moderating Role of Psychological Capital by Sara Mamdouh Mohamed Hussien and Mohamed A. Zoromba, Heba Emad El-Gazar, Ola Mousa, Shaimaa Mohamed Amin, Mohamed Hussein Ramadan Atta in SAGE Open Nursing
Supplemental Material
sj-docx-2-son-10.1177_23779608251376079 - Supplemental material for Fertility-Preservation Knowledge, Perceived Barriers, and Tokophobia Among Female Oncology Patients: The Moderating Role of Psychological Capital
Supplemental material, sj-docx-2-son-10.1177_23779608251376079 for Fertility-Preservation Knowledge, Perceived Barriers, and Tokophobia Among Female Oncology Patients: The Moderating Role of Psychological Capital by Sara Mamdouh Mohamed Hussien and Mohamed A. Zoromba, Heba Emad El-Gazar, Ola Mousa, Shaimaa Mohamed Amin, Mohamed Hussein Ramadan Atta in SAGE Open Nursing
Footnotes
Acknowledgments
This study is supported by funding from Prince Sattam bin Abdulaziz University's project number: PSAU/2025/R/1446.
Ethical Considerations
Approval for this study was obtained from the Research Ethics Committee of the Faculty of Nursing at El-Minia University, Egypt, under code number (REC202482). The well-being and rights of all participants were rigorously safeguarded in adherence to local laws, regulations, and the ethical principles outlined in the Declaration of Helsinki. Clear and comprehensive information about the study objectives was provided to all participants. They were explicitly informed that participation was voluntary and anonymous.
Consent for Publication
All authors have consented to the publication of this manuscript.
Authors’ Contribution
All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Materials
Supplemental material for this paper is available online.