
Abstract
Introduction
Health literacy is a critical factor influencing patient outcomes, yet research indicates a persistent gap in nurses’ knowledge of this domain. This deficiency affects nurses’ ability to identify and effectively address patients’ health literacy needs.
Objectives
This study aimed to assess nursing students’ knowledge (cognitive domain), application (psychomotor domain), and confidence (affective domain) related to health literacy strategies.
Methods
A descriptive study design was used with 344 nursing students who completed the Health Literacy Knowledge, Application, and Confidence Scale. The scale's validity and reliability were established through expert review and factor analysis.
Results
While participants demonstrated the ability to apply some health literacy strategies, they lacked fundamental knowledge about health literacy concepts, including identifying at-risk populations and appropriate reading levels for patient education materials. Confidence was positively correlated with the frequency of strategy use, although knowledge alone did not predict application. Deficiencies were particularly noted in recognizing screening tools and understanding the requirements for educational materials.
Conclusion
Findings reveal a significant gap in nursing students’ knowledge of health literacy, despite some capacity for application and a link between confidence and strategy use. These results underscore the need for enhanced integration of health literacy education in nursing curricula to better prepare students for clinical practice.
Introduction
While low health literacy has been recognized for many years, it has become increasingly prominent as a significant healthcare issue in the United States and worldwide over the past two decades. As a result of this trend, health literacy has been addressed in the Affordable Care Act and the National Action Plan for Improving Health Literacy, developed in 2010, and remains a focus within the healthcare community (Parnell, 2014). Health literacy became an even larger focus during the COVID-19 pandemic, as the need to educate the public on the prevention and treatment of the coronavirus was global. The need to increase health literacy among individuals and the way healthcare systems interact with individuals who have low health literacy has become paramount. For individual health literacy to improve, healthcare providers must increase their understanding of health literacy. The fundamental key to ensuring that health providers possess health literacy knowledge is to incorporate it into the curricula that prepare them for their role. By acquiring health literacy competencies, nurses can deliver more effective patient-centered care (Kim & Cha, 2021).
Review of Literature
Nearly nine out of 10 individuals struggle to understand healthcare information that is filled with unfamiliar medical terminology (Centers for Disease Control and Prevention (CDC), 2025). It is predicted that over 90 million American adults struggle with inadequate health literacy, rendering them unable to make informed decisions about their healthcare or follow the healthcare plan developed for them (CDC, 2025). Low health literacy is associated with poorer health outcomes and less effective use of healthcare services (Nutbeam & Lloyd, 2021).
Health literacy was redefined in Healthy People 2030 (U.S. Department of Health and Human Services, Office of Disease Prevention and Health Promotion, 2025). Health literacy is defined as having two parts, personal and organizational. Personal health literacy is “the degree to which individuals have the ability to find, understand, and use information and services to inform health-related decisions and actions for themselves and others” (U.S. Department of Health and Human Services, Office of Disease Prevention and Health Promotion, 2025). Organizational health literacy is “the ability of an organization to equitably enable individuals to have personal health literacy” (U.S. Department of Health and Human Services, Office of Disease Prevention and Health Promotion, 2025). Adequate health literacy is crucial for ensuring the success of interactions between patients and healthcare professionals. The ability of healthcare professionals to understand and address low health literacy is crucial for achieving optimal patient outcomes and improving patient health literacy. Evaluating health literacy knowledge, application, and confidence in nursing students helps enhance organizational health literacy by ensuring the attainment of necessary health literacy knowledge and skills.
Saunders et al. (2019) conducted a systematic review of the implementation of health literacy curricula in health profession programs, which concluded that greater clarity of core health literacy content and teaching strategies was needed. Bulfone et al. (2024) identified 30 articles related to nursing students’ knowledge of health literacy. Of these articles, the majority were outside the U.S., with only seven evaluating nursing students in North America. Six of these articles are prior to 2016. Seven studies focused on educational interventions improving students’ health literacy. Three studies focused on the health behaviors of students, with most being conducted outside the U.S. The remaining articles focused on the development of personal health literacy among nursing students. There is still limited information available about the health literacy skills and knowledge of nursing students (Bulfone et al., 2024). A review of the literature revealed a paucity of information regarding nursing students’ health literacy knowledge, application, and evaluation.
Hernes and Ott (2018) found that there is no core health literacy content within the nursing curriculum. A lack of consistent information about health literacy in the nursing curriculum is also present (McCleary-Jones, 2016). Although health literacy has been integrated into curricula, gaps still exist in important health literacy education (Mosley & Taylor, 2017). The findings revealed that educators perceived the content as present but not clearly visible. Limited research has been conducted on how the nursing profession interacts with or influences the phenomenon of health literacy through interventions and communication, as well as the nursing professional's understanding of health literacy (Yang, 2022).
A landmark document, “Health Literacy: A Prescription to End Confusion,” acknowledges that healthcare professionals need to be educated about health literacy from the beginning of their professional training (Kindig et al., 2004). Despite this key urgency, nursing education has not yet developed a clear and concise curriculum for health literacy that encompasses core competencies that include knowledge, skills, and affective domains. Although there is still no core curriculum, work on health literacy competencies has been initiated (Yang, 2022). Health literacy competencies encompass knowledge, skills, and attitudes related to health literacy, as well as methods for effectively using them with individuals who have low literacy (Kim & Cha, 2021). Core domains of health literacy practice include adequate ability to address health literacy, recognition and awareness of health literacy, confidence, and skills in caring for patients with low health literacy (Chang et al., 2017).
The nurse needs to understand what health literacy is and possess the skills necessary to work within the patient's level of health literacy. When nurses possess health literacy knowledge, they can apply their skills and feel more confident in addressing the health literacy needs of their patients. To better understand what students have learned and whether they are confident in using health literacy, the three domains of professional learning (affective, cognitive, and psychomotor) need to be explored. The Health Literacy Knowledge, Application, and Confidence Scale (HLKACS) incorporates these three domains. The emphasis placed on health literacy in nursing education can vary significantly, directly influencing the effectiveness of health literacy strategies and overall confidence. The three domains, cognitive (addressing knowledge), psychomotor (the application of strategies), and the affective domain (addressing confidence), in the HLKACS instrument ensure that all domains of professional learning are covered.
Conceptual Framework
The HLKACS was developed on the idea that nursing agency is needed to improve a patient's health literacy. Freire (2005, 2010) argues that human relationships exist in the plural. The nurse (nurse agency) and the patient (self-care agency) collaborate to address health disparities. This reflective action enables the empowerment of both the nurse and the patient in the health education process. Health literacy is a process of communication that enables informed decision-making and informed choices. Nursing acts as the agent to ensure that clear and understandable information is presented.
Improving health literacy leads to improved outcomes. Nursing agency is needed to develop an individual's health literacy, enabling them to meet their self-care demands. Orem (1991, 2001) stated that self-care is a learned behavior and a deliberate action. The response of the individual is not instinctive or reflexive but is performed with a rationale based on a known need. If the patient is unable to address needs due to health literacy deficits, self-care ability is compromised.
Orem's nurse agency focuses on developing a broadened awareness of the role of the nurse and creating a more comprehensive perspective (Orem, 2001). Curriculum needs are increasing at an alarming rate. As healthcare becomes increasingly complex and nursing knowledge expands, the risk of stagnation in thinking and diminished learner development increases. Orem (2001) claimed that nursing education needs to advance understanding and merge research into practice. Nursing education lacks a consistent curriculum on health literacy knowledge and strategies. Health literacy knowledge and strategies encompass basic facts on health literacy, the consequences associated with low health literacy, health literacy screening methods, guidelines for written healthcare materials, and the evaluation of health literacy interventions.
Health literacy, a relatively new concept in healthcare, is often misunderstood and not adequately addressed within the nursing curriculum. Nutbeam & Lloyd (2021) state that health literacy enables individuals to take action on their health and address the social determinants of health. Nutbeam's model of health suggests three concepts: functional, interactive, and critical health literacy. First, functional health literacy encompasses the basic knowledge of health literacy and the methods to enhance it. Second, interactive health literacy is the application of the skills and strategies learned. Lastly, critical health literacy is having the ability to feel confident in using one's knowledge and skills to improve a patient's health literacy.
Sørensen et al. (2012) further developed an integrative concept model after identifying twelve concept models during a systematic review. Sorenson had four competencies: access, understand, appraise, and apply. Sorenson's model could be applied to the education of healthcare providers who require access to and understanding of health literacy knowledge, the need to appraise patients’ health literacy, and then apply strategies to assist individuals with low literacy. If the healthcare provider has these, they can then develop confidence when working with individuals who have low health literacy. Health literacy is a valuable asset to patients that healthcare providers must help build. Additionally, healthcare providers or the organization must prioritize building this asset alongside the patient.
Sørensen et al. (2012) also included a model of health literacy by Paasche-Orlow and Wolf in the integrated model. The Paasche-Orlow and Wolf model of health literacy views health literacy issues as both patient- and system-related (Paasche-Orlow & Wolf, 2007). There are three key points along the continuum where health literacy affects healthcare, including access to and utilization of healthcare, patient–provider interaction, and self-care according to the Paasche-Orlow and Wolf model (Paasche-Orlow & Wolf, 2007). The items in the HLKACS scale reflect each of the three components identified in the model. Items addressed the assessment and understanding of patient factors, including perceived barriers, self-efficacy, and navigation skills within the access continuum. System factors, such as complexity or tiers of service, and provider factors, including teaching ability and communication skills, were also examined.
HLKACS is grounded in a theoretical foundation of social justice, nursing agency, and health literacy. The HLKACS scale reflects current conceptual models of health literacy. It is a valuable tool to help nurse educators assess the current knowledge of health literacy within their student populations.
Purpose
The purpose of this study was to determine the level of knowledge (cognitive domain), application (psychomotor domain), and confidence (affective domain) in health literacy among nursing students, with a focus on their understanding of health literacy knowledge and strategies. Research on understanding the level of health literacy competency among nursing students is lacking. This study addresses this gap by collecting data on all three domains of health literacy to measure nursing students’ health literacy knowledge, skills, and confidence.
Method
Study Design and Population
A cross-sectional design was used to collect quantitative data to examine the following research questions:
What is the level of knowledge about health literacy and health literacy strategies, experience with health literacy strategies, and confidence among nursing students? Are there relationships between health literacy knowledge, application, and level of confidence in nursing students? Is there a difference in health literacy knowledge of nursing students based on academic standing? Is there a difference in health literacy knowledge of nursing students based on the program they attend?
Study Procedure
Nursing students who were attending accredited Bachelor of Science in Nursing (BSN) and Associate Degree of Nursing (ADN) programs in a midwestern state were recruited. The inclusion criteria were individuals aged 18 or older who were currently enrolled in either an associate degree or a bachelor's degree nursing program. Subjects were excluded if information related to their standing in the program was absent or if there was missing data on their online submission. The Institutional Human Participants Review Committee reviewed and approved the protocol for conducting this study. After obtaining permission from the organization and compiling the email lists, surveys were emailed to 350 faculty and deans at 60 schools of nursing (ADN, n = 36, BSN, n = 24) in a midwestern state using SurveyMonkey to help identify potential study participants. Schools were both private and public higher learning facilities. Deans and faculty at the schools were asked to disseminate the request for participation to their students.
Recruitment was conducted via email, where potential participants were informed about the study's purpose, as well as the voluntary and confidential nature of their participation. If individuals agreed to participate, they would receive a subsequent email including a link that would allow them to take the survey anonymously. Consent was implied based on the return of the completed survey. As a result, 406 consent forms were signed, whereas 344 completed the online surveys (yielding an 86% return rate), with 62 participants not completing the survey (with greater than 50% of all three subscales left blank) or inclusion criteria not met. Those who did not complete or had missing data were excluded. Additionally, the participants were asked to complete the electronic survey a second time, 2 weeks later, for reliability testing. Forty students completed the survey a second time, 2 weeks later, to establish test–retest reliability. The participant flow diagram is shown in Figure 1.
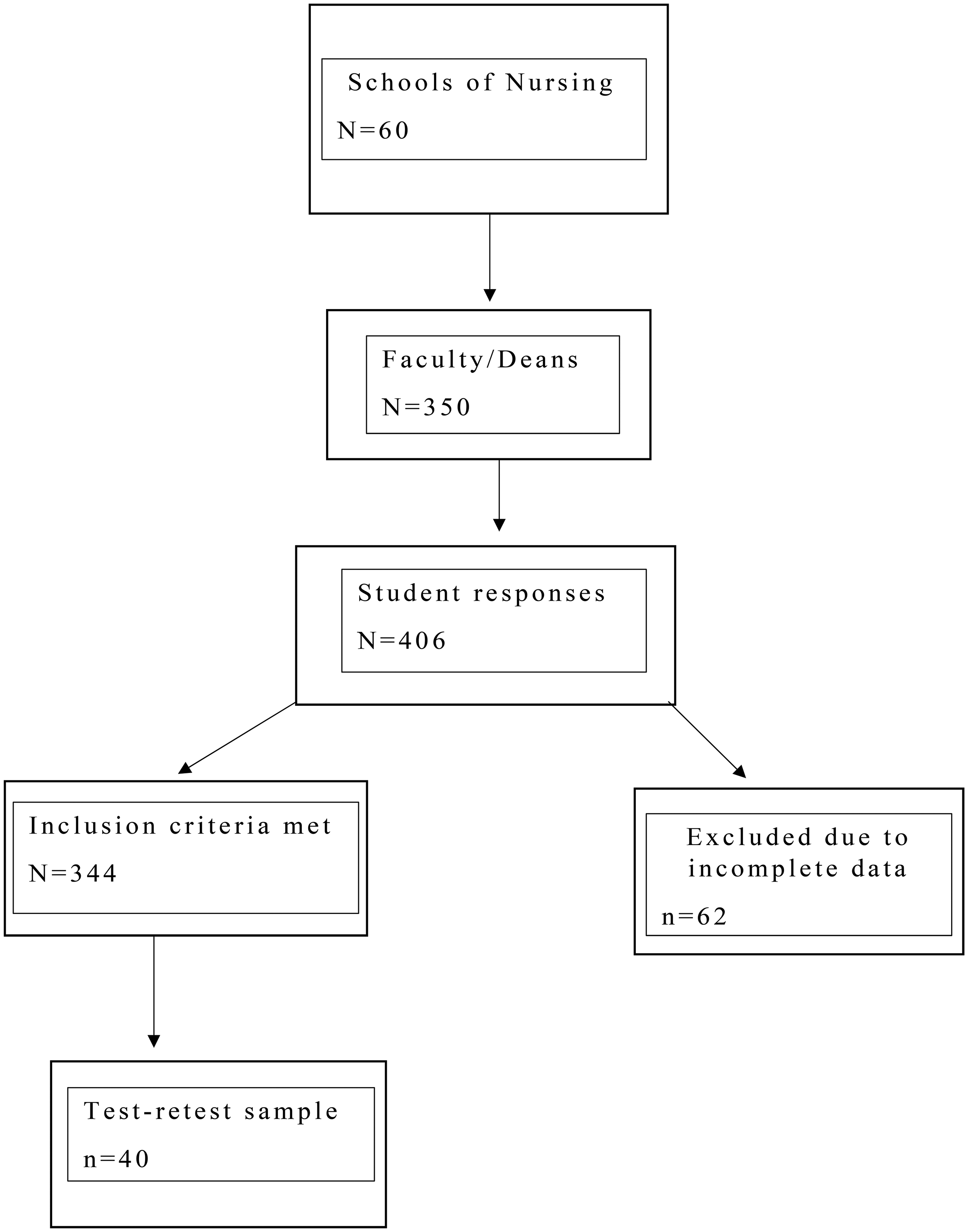
Strobe Participant Flow Diagram.
The sample size was determined based on a potential population of approximately 10,000 nursing students in Michigan (Michigan Center for Nursing, 2013). Using the approximate number of nursing students, a sample between 322 and 370 was suggested for a 95% confidence level for exploratory factor analysis (EFA) based on a chart in Mitchell and Jolley (2001). Rounding up to 400 allows for errors in absent data and incomplete surveys.
Statistical Analysis
The independent variables for this study were the academic level of nursing students and program type, with dependent variables of Health literacy knowledge, application, and confidence. Descriptive statistics were used to analyze demographic data. For the data related to three subscales (i.e., health literacy knowledge, application, and confidence), means and standard deviations (SD) were calculated. To test for bivariate relationships between the HLKACS scales in this sample, Pearson's correlations were performed with subscale scores. A one-way analysis of variance (ANOVA) was conducted to assess differences in mean scores on the knowledge, application, and confidence subscales between five levels of educational standing (i.e., associate degree-first year, associate degree-second year, BSN-sophomore, BSN-junior, and BSN-senior). ANCOVA testing was performed to control for covariance. Statistical significance for all testing was set at 0.05.
Health Literacy Knowledge, Application, and Confidence Scale Pilot Studies
Based on early findings from both qualitative and quantitative pilot studies conducted with RN to BSN students, traditional BSN nursing students, and a comprehensive literature review, the HLKACS was developed (DeBello, 2016). A pilot study was conducted to establish and evaluate a measurement that encompasses three domains of health literacy: knowledge, application, and confidence.
The initial HLKACS consisted of 40 items and included three subscales: Knowledge (15 items), Application (17 items), and Confidence (9 items). Reliability and validity were evaluated. Internal consistency, as measured by Cronbach's alphas, was used to evaluate reliability. In contrast, two of the three subscales demonstrated excellent internal consistency with Cronbach's alphas of 0.93 for the application subscale and 0.91 for the confidence subscale, respectively. The knowledge subscale had a Cronbach's alpha of 0.41. The items were knowledge-based and consistent with the format of a test item. Due to the format of test items, the knowledge subscale did not demonstrate good reliability because of the lack of variance within the items. The knowledge subscale scored poorly because it was at an ordinal level of measurement. Therefore, item analysis and item discrimination analysis were more effective evaluation strategies for determining the reliability of the knowledge subscale; these strategies were later employed in the complete psychometric testing of the revised HLKAC instrument.
Face validity was addressed by the ease of taking the survey online. Additionally, content experts validated the instrument's validity. Reliability was established using factor analysis. Principal component analysis was performed examining the associations among the knowledge, application, and confidence items, and the Varimax algorithm was used for factor rotation. This analysis generated nine factors with eigenvalues greater than one, with six factors (factors 1, 2, 3, 4, 5, and 6) representing the knowledge domain, two factors (factors 7 and 8) representing application, and one factor (factor 9) representing the confidence domain. Categorical PCA was used for the Knowledge subscale in this study.
Current Instrument
This study utilized the revised 36-item HLKACS, which comprises four sections. Section 1 included demographics (seven items). Section 2 was health literacy knowledge consisting of nine multiple-choice questions to assess nurses’ knowledge of health literacy in the following four content areas defined as: 1) Reading levels (3 items), 2) Risk and strategies (3 items), 3) Risk factors (1 item), and 4) Basic Facts (2 items). Section 3 was health literacy application, a 13-item scale measuring the use of health literacy strategies and evaluation of health education practices that uses a 5-point Likert scale that ranges from 1 to 5 scoring as follows: Never, 25% of the time, 50% of the time, 75% of the time, and 100% of the time. Finally, Section 4 was health literacy confidence consisting of 7 items that evaluate the confidence level in using health literacy strategies and assessing patients for health literacy issues, using a 10-point Likert scale, where 1 = “can never perform,” 5 = “can perform part of the time,” and 10 = “can perform all the time.”
Health Literacy Knowledge, Application, and Confidence Scale Reliability & Validity
The HLKACS instrument showed satisfactory internal consistency with a Cronbach's alpha of 0.79 in overall HLKACS and excellent internal consistency for the Application and Confidence subscales with Cronbach's alphas of 0.91 and 0.92, respectively. The Knowledge subscale had a low alpha value (0.34) due to its correct-not correct format. A low Cronbach's alpha for reliability indicates that the items do not measure the same construct. This was expected, as the knowledge subscale measures knowledge across four content areas, and low reliability of the knowledge subscale was anticipated. Item discrimination and difficulty were performed. Item analysis reported biserial r values ranging from 0.03 to 0.54 for the knowledge domain. The standard range for difficulty is 0.25 to 0.75, with discrimination over 0.20. The overall scores for the knowledge subscale items fell within acceptable levels of item discrimination and difficulty. The Cronbach's Alpha for knowledge is likely to be low due to variability in students’ knowledge and the lack of correct answers being selected.
Test–retest reliability was conducted on responses from 40 participants who completed the survey twice within 1 month, and Pearson's (r) coefficients from correlations of pre- and post-subscale scores ranged from 0.51 to 0.59, which demonstrated satisfactory test–retest reliability. Test–retests were also performed using t-tests; the results showed that there were no significant differences between the pre- and post-test results for the knowledge, application, and confidence subscales, indicating good test–retest reliability among the three subscales.
The content validity of HLKACS was established by three content experts with expertise in health literacy, who provided comprehensive reviews of the items during the instrument development process. The reviewers were doctoral-prepared nurses with research experience and publications related to health literacy. Each rated survey questions using a three-point Likert scale, with 1 = not important, 2 = somewhat important, and 3 = Important, and rated if the question is clear and concise (based on a Yes or No response). Based on feedback from content experts, the wording of items was modified, and those deemed repetitive were removed. The final HLKACS consisted of three subscales: the knowledge subscale, which consisted of nine questions; the application subscale, which consisted of 13 questions; and the application subscale, which consisted of seven questions. Construct validity was established by exploring the factor structure of the HLKACS using EFA with the principal component analysis method of factor extraction and the Varimax rotation method. The EFA was first performed on Health Literacy Application and Confidence subscale items and results generated four factors: Factor 1 (eight items)—Health literacy application strategy: Assessment of reading level (with an eigenvalue of 8.5); Factor 2 (seven item) Health literacy confidence (with an eigenvalue of 2.41); Factor 3 (two items)—Health literacy application strategies: Language (with an eigenvalue of 1.32) and Factor 4 (3 items)–Health literacy application strategies: Health literacy (with an eigenvalue of 1.03), Together, the four factors explained 66.36% of the variance of the HLKACS Application and Confidence subscales.
Due to the knowledge subscale being at the nominal level, EFA could not be used. Categorical principal component analysis (CPCA) was used on the health literacy knowledge subscale. CPCA is performed on data at the nominal level. CPCA was performed on the Knowledge subscale, as this analysis was conducted separately due to the correct-not correct response format of the Knowledge subscale. The analysis identified four factors in the Health Literacy Knowledge subscale: Factor 1 (three items)—Reading levels (with an eigenvalue of 1.69); Factor 2 (three items)—Risks and strategies (with an eigenvalue of 1.40); Factor 3 (one question)—Risk Factors (with an eigenvalue of 1.17), and Factor 4 (two items)—Basic facts (with an eigenvalue of 1.05). The four factors accounted for 58.98% of the total variance within the HLKACS knowledge subscale.
According to Yong and Pearce (2013), a loading factor above 0.32 is required for a sample of over 300 to be statistically significant. Loading scores for knowledge ranged from .50 to .84, which could be related to the diversity present among the questions. The range of loading values is most likely due to inconsistencies in students’ knowledge of health literacy. Factor analysis can be challenging when questions assess knowledge and may not accurately represent the dimensions within the knowledge subscale. Based on the suggested loading values, knowledge items within the knowledge subscale were statistically significant and measured health literacy knowledge. The results of EFA/CPCA demonstrated satisfactory factor structures for health literacy knowledge, application, and confidence domains.
Results
Sample Demographics (N = 344).

BSN = Bachelor of Science in Nursing.
Health Literacy Knowledge
Knowledge items were categorized into four content areas: reading levels, risk and strategies, risk factors, and basic facts. The mean scores for each content area of health literacy knowledge subscales are presented in Table 2. The percentage of correct answers for each item is shown in Table 3. In the content area of reading levels related to health literacy, it was surprising that almost all student participants (>99%) were unaware of the reading level of written health materials. They also (>89%) were unaware of the JCAHO-recommended reading level for patient educational materials. In the context of risks and strategies, two-thirds of students were unaware that the elderly are at the highest risk for low health literacy. In contrast, most students (83%) were able to identify the strategies needed to improve their comprehension of health information. Another deficit area of knowledge is that only about 40% of students were able to identify that individuals at all reading levels can have low health literacy. In the area of basic facts for health literacy, alarmingly, more than 99% of students could not identify that low literacy increases hospital readmissions, and fewer than half of the students could identify the components of health literacy skills.
Mean and Standard Deviations for Health Literacy Knowledge Subscale (N = 326).

SD = standard deviation.
Percentage of Correct Answers for Health Literacy Knowledge Subscale (N = 326).

Health Literacy Application
The participants’ responses on the 13-item Health Literacy Application Subscale yielded a mean total score of 47.23 ± 8.79, with a possible score range of 13–65. Application items were categorized into three content areas: assessment of reading levels, language, and health literacy strategies. Table 4 displays the means, SD, and percentages of various application strategies used by participants. Interestingly, assessment of reading level items showed the lowest levels of application. In this study sample, participants reported using plain language more frequently during their teaching, assessed their use of their native language, and employed open-ended questions. Nevertheless, participants reported that they less frequently assessed educational levels or evaluated the reading level of health care materials before using them for patient teaching. Another area that students applied less frequently was assessing patients’ ability to use health-related internet sources.
Responses to Health Literacy Application Subscale (N = 326).

SD = standard deviation.
Health Literacy Confidence
The participants’ responses on the 10-item Health Literacy Confidence Subscale yielded a mean total score of 47.83 (SD = 10.91), with a possible score range of 7–70. While participants reported having more confidence in adjusting methods of delivering instruction and finding additional resources to help the provider when dealing with low literacy, they reported less confidence in assessing low literacy, using best practices for addressing health literacy, and identifying educational resources for lower literacy (Table 5).
Responses to Health Literacy Confidence Subscale (N = 326).

SD = standard deviation.
Relationships Between Knowledge, Application, and Confidence
Pearson's correlation coefficients were analyzed to determine the relationships between knowledge, application, and confidence. The Bonferroni approach was used to control Type I errors. The results showed a statistically significant positive correlation between knowledge and application (r(315) = 0.164, p = 0.004) and between application and confidence (r(312) = 0.534, p < 0.001). There was no significant correlation between knowledge and confidence, r (314) = 0.026, p = 0.65.
Health Literacy Knowledge, Application, and Confidence Scale, Program Types and Academic Standing
Differences in health literacy knowledge, application, and confidence between ADN and BSN programs were examined to determine if program type or academic standing affected scores on the scale. This allowed us to examine the maturation of subjects as they progressed through the program, as well as to identify any significant differences between programs in terms of health literacy knowledge and skills. As seen in Table 6, ADN students demonstrated a higher level of health literacy knowledge (t (307) = 88.19, p < .001), application (t (307) = 42.23, p < .001), and confidence (t (307) = 78.81, p < .001) than BSN students. ANCOVA testing met the assumption of homogeneity of variances.
HLKACS and Academic Standing.
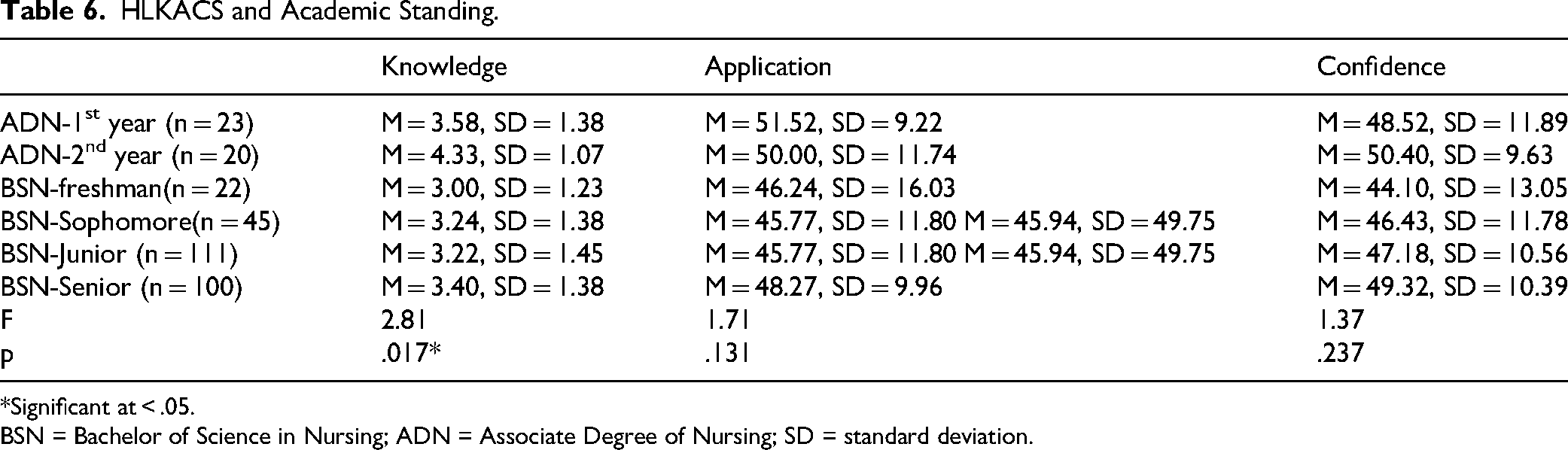
*Significant at < .05.
BSN = Bachelor of Science in Nursing; ADN = Associate Degree of Nursing; SD = standard deviation.
A one-way ANOVA was conducted to compare the knowledge, application, and confidence levels of ADN and BSN students at different academic standings. Normality checks and Levene's test were carried out, and the assumptions were met. There was a significant difference in mean knowledge (F (5,317) = 2.82, p = 0.017) between the ranks of BSN and ADN students. Post hoc comparisons were performed using the Tukey test. The post hoc results showed a significant difference between ADN (second year), ADN (first year), and BSN students (across all levels) in knowledge scores. In contrast, second-year ADN students scored an average of one point higher than any of the BSN students and one-half point higher than first-year ADN students. Although the second-year ADN students had better scores on the Knowledge subscale than their peers, their mean score of 4.33 was still less than half of the total score of the Knowledge scale (9). No statistical difference was detected among academic programs and levels in the Application or the Confidence.
Discussion
This study explored the health literacy knowledge, application, and confidence of BSN and ADN nursing students. The study's results showed that nursing students were able to apply health literacy application strategies; however, they struggled to identify appropriate reading levels for educational content, populations at risk for health literacy issues, and basic health literacy facts. This finding is consistent with earlier studies by Cormier and Kotrlik (2009), Torres and Nichols (2014), and Williamson and Chopak-Foss (2015), which also reported that nursing students lacked knowledge in these critical areas of health literacy. Associate degree nursing students were found to have a higher level of health literacy knowledge. It should also be noted that, although ADN students scored higher than BSN students, the mean score of second-year students on the knowledge subscale was still less than 50% of the total score that participants could obtain. This should raise concerns within both BSN and ADN education that the health literacy content within the curriculum needs to be evaluated. By addressing health literacy in the nursing curriculum, core competencies in health literacy can be further developed, having a direct impact on both patients and the healthcare system.
Health literacy strategies are not only necessary for understanding but also for engaging in action during the learning process. Nursing students lacking knowledge of health literacy often struggle to apply strategies in a way that ensures engaged learning with patients who have low health literacy. Balmer et al. (2020) reported that nursing students often develop their health literacy as they progress through their education. Ozan et al. (2019) and Mosley and Taylor (2017) support this, stating that the lack of individual health literacy has an impact on the long-term ability of healthcare providers to develop a sustainable, competent, and evidence-based healthcare system. The lack of individual health literacy can be another factor that interferes with the application of the health literacy strategies that have been learned. Recognizing that health literacy is still developing in students, it is essential to employ health literacy strategies when teaching nursing students about health literacy. Demonstration of the correct strategies and having time to practice are crucial.
Alsubaie and Salem (2019) found that even nurses with moderate health literacy knowledge and skills often underestimate the effect of low health literacy and do not fully appreciate the impact of low health literacy on their patients. More importantly, nurses may not realize that they are not meeting the health literacy needs of their patients. Students with limited knowledge of health literacy are at risk of entering practice with an insufficient understanding of this concept, which has a substantial impact on their patients’ ability to meet their own self-care needs. Even more importantly, little is known about the confidence level of healthcare professionals or students in using health literacy skills and strategies. The HLKACS scale is the only health literacy instrument that evaluates not only knowledge and application but also confidence in dealing with health literacy. In this study, results showed that nursing students who reported more confidence also reported using more health literacy strategies. The Dunning-Kruger Effect was also a possible issue. Students early in the programs often reported higher confidence levels and higher application rates. This may be due to their inability to assess their own skills, resulting from a lack of knowledge about the required skills and an inadequate understanding of what these skills entail. The areas of deficiency reported by study participants included recognizing tools for screening patients, basic facts about health literacy, and the requirements of educational materials to meet health literacy standards.
There was a strong correlation between application and confidence, and a modest correlation between knowledge and application. For nursing students, it is unlikely that they will apply strategies effectively without proper knowledge of health literacy. While knowledge is not directly correlated with confidence, the strong correlation between application and confidence suggests that students may develop confidence in the process of applying health literacy strategies. Knowledge alone does not provide students with the skills needed to feel confident in addressing health literacy, but confidence is gained through the practice and application of this knowledge. This highlights the need not only to include knowledge in the curriculum but also to incorporate practical experience in applying health literacy strategies and skills in the clinical setting. Student nurses need to acquire the necessary health literacy knowledge and apply it in practice, guided by experts, to ensure they possess the appropriate level of knowledge and application to support confidence in addressing health literacy issues among patients.
The findings of this study support the three levels of Nutbeam's conceptual framework of health literacy (Nutbeam & Lloyd, 2021). As Nutbeam discussed, basic functional health literacy precedes the development of interactive and critical health literacy. The data from this study suggest that students require a basic understanding of health literacy before applying health literacy skills and strategies in practice. Confidence is gained through the application and practice of those skills.
Health literacy knowledge and the ability to apply the strategies are vital within the nursing curriculum. Hernes and Ott (2018) issued a call to action for developing basic competencies in health literacy within the nursing curriculum. Additionally, no core concepts in the curriculum or evaluation criteria were identified in the literature. Today's healthcare arena requires nurses to understand what a patient is capable of learning and how to facilitate it. By addressing health literacy issues, patient outcomes can be improved while reducing healthcare costs. Teaching patients about their health is an expected function of a practicing nurse, and the competency needs to be obtained in nursing school. One way this can be accomplished is by adopting the eight health literacy practices defined by Coleman et al. (2017) as a framework for nursing curricula, thereby developing further strategies for integrating content and evaluation methods into the curricula.
Limitations
Limitations of the study include the use of an instrument that has not been previously validated and the possibility that participants may have a desire to learn more about the topic being explored. Possible sources of constant error included social desirability and acquiescent responses. Confounding factors, such as history, acquiescent responses, and social desirability, were controlled by limiting the data collection time and using answers that reflected percentages instead of absolute numbers.
The use of a convenience sample may limit the generalizability of the results to the entire nursing student population. The study relied on deans, directors, and faculty to distribute the survey. This also limits our ability to assess curricular differences in programs, as the program attended was not specified. As a result, selection bias is possible due to the survey nature of the research project. However, the sample population may be more representative of the larger population due to the use of a whole state as the sampling frame.
Strengths
The current HLKACS not only measures health literacy knowledge but also assesses application and confidence, thereby adding depth to the research on health literacy among healthcare professionals. Additionally, the HLKACS proved to be a valid and reliable tool. Although Part I of the instrument, specifically the Knowledge subscale, had low reliability (α = 0.39), item analysis of the items demonstrated acceptable scores for the items in this subscale. The subscales of Application and Confidence demonstrated excellent internal consistency, with Cronbach's alpha values of 0.91 and 0.92, respectively. The use of the HLKACS enables the exploration of a complex phenomenon, facilitating further research. The HLKACS enables the investigation and implementation of health literacy curricula, as well as the evaluation of their effectiveness, assisting in the development of a robust health literacy curriculum that can be incorporated into nursing education.
Implications for Practice
The results of this study indicate that nursing students reported a deficiency in health literacy knowledge, application, and confidence. The effectiveness of nursing incorporating health literacy content into the nursing curriculum needs to be further explored. There is little evidence of how health literacy is incorporated into the curriculum and whether it is effective. It is also less clear how health literacy is being incorporated into the clinical component of education. It is essential to note that policy is necessary to drive changes in nursing curricula, ensuring that health literacy is incorporated into the curricular requirements. This may be achieved by incorporating health literacy as a priority in accreditation requirements by the National League for Nursing (NLN) and the American Association of Colleges of Nursing (AACN). AACN has addressed the need for health literacy in the updated Essentials (American Association of Colleges of Nursing, AACN, 2025).
Delineating priority content in the nursing curriculum has been a constant challenge as technology advances and new developments in health emerge. Nursing programs are designed to produce graduates who are prepared as generalists and can acquire additional practice knowledge in the workforce. However, the expectations in the practice setting have evolved to require graduates to be prepared to implement independent practice with minimal support from the healthcare organization. The integration of health literacy knowledge and skills into the nursing curriculum should be a key focus, accompanied by further research to ensure that health literacy is effectively integrated and practiced after graduation.
There is limited research on the most effective strategies for teaching health literacy to nursing students. There is also limited discussion on what content needs to be included in the curriculum. As nursing education shifts toward competency-based education, health literacy must be a priority competency. However, practical applications can be employed, such as role-playing, simulation, case studies, teach-back, plain language content, and viewing videos of health literacy interactions in didactic courses (Ali et al., 2014; Coleman et al., 2017; Epstein, 2023; Kim, 2022; Mosley & Taylor, 2017; Weekes & Phillips, 2015; Zanchetta et al., 2013). Nursing education can expand pedagogical strategies by providing case scenarios and studies that include activities to promote screening patients for low health literacy, incorporating content related to the costs of low health literacy into didactic content, and developing activities that allow students to critique health education materials for health literacy requirements. This can be done through role-playing or the development and evaluation of healthcare materials as a class assignment related to the care of patients with complex health conditions. Exploring the social determinants of health within the case study and identifying the barriers to accessing healthcare can help students develop assessment skills for health literacy. These activities can be integrated into both didactic and clinical settings, enabling students to work with real individuals or through high-fidelity simulation. High-fidelity simulation, virtual simulation, or standardized patient simulation can allow the student to practice assessing health literacy and applying strategies for addressing health literacy. Kim (2022) found that well-designed simulation learning can be effectively used for health literacy development in nursing student education. Through these activities, students can gain confidence in caring for patients with low health literacy. The use of health literacy screening tools can be incorporated into role-playing and simulation opportunities to enhance understanding of their application. These tools can also be used in the clinical setting to screen real patients during their clinical experiences.
It is well known that the teach-back method used in patient education enhances patient interactions and learning experiences, particularly for those with low health literacy (Coleman et al., 2017). Incorporating structured assignments that utilize the teach-back method can enhance students’ ability to use it effectively. Teach-back is recommended as a health literacy-based communication approach; however, it is not consistently used due to a lack of training, time, or organizational support (Talevski et al., 2020). We must ensure students have been taught the correct method of using teach-back and can practice it in both didactic and clinical settings. Health literacy knowledge and strategies are important, but repetitive and consistent integration of these concepts across the curriculum is imperative due to the evolving knowledge levels and health literacy abilities of students.
Conclusion
Health disparities in the United States are consistently identified within healthcare systems. Declining literacy, increasing diversity, and a large expectation for knowledge-intensive work environments are contributing to what can be called a “perfect storm” for quality improvement in health literacy. By identifying the level of health literacy possessed, the educator can determine if the health literacy content in the curriculum is sufficient. This study reveals that we are still not meeting the competency levels required to enter practice and make a meaningful impact on the healthcare system and the individual's health literacy needs. There is a need to integrate health literacy content into nursing curricula and to develop core competencies and evaluation methods to ensure nursing students are prepared to meet the health literacy demands of patients upon graduation. Due to the limited research on strategies for teaching health literacy education to healthcare professionals, further research in this area is necessary.
Footnotes
Acknowledgements
The authors would like to thank the students who participated in this study.
Ethical Approval and Consent to Participate
Permission was obtained from the Human Subjects Review Committee at Eastern Michigan University, IRB#819809. Data collection, consent, and security complied with the Eastern Michigan University Office of Research Development's statement on online surveys.
Consent for Publication
I affirm this work is original and has not been published elsewhere, except as noted in the manuscript.
Funding
Publication made possible in part by support from Eastern Michigan University’s Faculty Open Access Publishing Fund, administered by the Associate Provost and Vice President for Graduate Studies and Research, with assistance of the EMU Library.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of Data and Materials
Datasets generated and/or analyzed in this study are available from the corresponding author with a reasonable request.
Use of AI Software
I affirm that originality and integrity of this work are entirely the authors’ and are not influenced by AI technology.