
Abstract
Background
Tracheal suctioning is a critical component of care for mechanically ventilated patients’ treatment. The effectiveness and associated complications of suctioning can vary depending on the depth of catheter insertion. Although several guidelines assist nurses in selecting the appropriate suctioning technique, while the optimal suctioning depth remains uncertain.
Purpose of the research
This study aimed to evaluate the impact of implementing shallow (insertion of the suction catheter to a depth limited to the end of the endotracheal tube) versus deep tracheal suctioning (insertion of the suction catheter approximately 1 cm above carina) techniques on cardiovascular indices and suction-induced complications among mechanically ventilated patients.
Methods
A randomized controlled trial (RCT) with two parallel groups at a 1:1 ratio was carried out in Intensive care units of a tertiary hospital. Adult mechanically ventilated patients requiring tracheal suctioning were randomly assigned to either the shallow tracheal suctioning group (intervention) or the deep tracheal suctioning group (control). Cardiovascular indices (such as heart rate, blood pressure, respiratory rate, and oxygen saturation) and suction-induced complications (as hypoxemia, cardiac dysrhythmia, tracheal tissue injury, and increased intracranial pressure) were assessed at four specific times: before suctioning, immediately after suctioning, 5 min postsuctioning, and 10 min postsuctioning.
Results
A total of 120 patients were enrolled in the study. Cardiovascular indices increased significantly following tracheal suctioning in the deep suctioning group compared to the shallow suctioning group (p < .05). Additionally, the incidence of suction-related complications was significantly lower in the shallow suctioning group (p < .05).
Conclusions
Shallow tracheal suctioning results in less pronounced alterations in cardiovascular indices and fewer suction-induced complications compared to deep suctioning. These findings support the adoption of shallow suctioing as a safer and more favorable technique for managing mechanically ventilated patients.
Keywords
Introduction
Mechanical ventilation (MV) is a lifesaving intervention for patients with critical illness. It involves the insertion of an artificial airway; either an endotracheal tube (ETT) or tracheostomy tube into the trachea to assist with ventilation assistance and facilitate the removal of respiratory secretions. Currently, artificial airway management constitute approximately 70% of care in intensive care units (ICU; Li et al., 2021; Wirth et al., 2016). The critical care nurses are responsible for delivering holistic care to mechanically ventilated patients (MVPs) including performing suctioning therapy based on evidence-based practice to enhance care quality and prevent procedure-related complications (Li et al., 2021; Yang et al., 2023).
Tracheal suctioning (TS) is a technique used to remove secretions from the respiratory tract with the aid of a suction machine. It is a vital component of airway management for MVPs. It is widely used and offers well-recognized benefits, including maintaining airway patency, improving oxygenation, facilitating timely removal of secretions, and preventing airway obstruction and pulmonary complications. MVPs often require repeated TS due to excessive accumulation of respiratory secretions, primarily caused by the tracheal tube's irritating effect on the mucociliary function of respiratory epithelium. Competent health professionals are essential to perform skillful TS and to minimize the risks and complications associated with the procedure in critically ill patients (Kostekli et al., 2022; Schults et al., 2020, 2021).
TS may lead to various complications that can prolong the length of hospitalization for critically ill patients (CIPs) and further compromise their physical condition. MV and TS increase the risk of nosocomial infections and ventilator associated pneumonia (VAP), which contributes to a 30% mortality rate among MVPs. Additionally, improper TS may lead to tracheal mucosal injury, pain, discomfort, infection, hemodynamic instability, impaired gas exchange, bronchospasm, alveolar collapse, elevated intracranial pressure (ICP), hypoxia and compromised peripheral and cerebral tissue perfusion. Therefore, it is essential to perform TS with highest level of accuracy, precision and using atraumatic techniques (Kostekli et al., 2022; Yang et al., 2023).
TS can be performed using either a shallow or deep technique, which is differentiated by the depth of suction catheter insertion. Deep tracheal suctioning (DTS) involves inserting the suction catheter until resistance is met at the carina, then withdrawing it approximately 1 cm to aspirate secretions from the proximal lower airway. In contrast, shallow tracheal suctioning (STS) targets secretions within the ETT only, without entering the lower airway (Kostekli et al., 2022).
The standard clinical approach to TS requires nurses to manually insert a suction catheter into the tracheal cannula, applying negative pressure, and withdraw it carefully upon encountering resistance. Despite its routine use, this technique poses a significant risk of injuring the tracheal carina. Contact between the suction catheter and the airway can elicit strong reactions and repeated friction, increasing the likelihood of mucosal irritation, erosion, and bleeding (Yang et al., 2023).
Literature Review
Limited studies have been conducted to evaluate the impact of DTS and STS among MVPs in ICUs. These studies demonstrated that both TS methods helped prevent respiratory complications resulting from secretion accumulation; however, they also induced hemodynamic instability and patient's discomfort (Khayer et al., 2020; Kostekli et al., 2022). Al-Mayetiazidy et al. (2024) investigated the effect of STS and DTS on physiological indices and endotracheal cuff pressure in 100 MVPs. They reported that DTS was more effective in clearing secretions and enhancing oxygenation, yet it led to more pronounced changes in hemodynamic parameters, including mean arterial pressure (MAP), heart rate (HR), systolic blood pressure (SBP), and ETT cuff pressure compared to STS.
Yang et al. (2023) investigated the clinical effectiveness of STS and DTS in 52 MVPs. They concluded that STS had a significantly milder impact on patients’ vital signs than DTS (p < .05). Moreover, patients who received STS showed a significantly lower frequency of suctioning, shorter MV duration, and hospital stay, and experienced less tracheal mucosal injury and few irritating cough episodes compared to those who underwent DTS. To mitigate the risks associated with tracheal suctioning, the 2010 guidelines of the American Association for Respiratory Care (AARC) recommended the use of superficial suctioning as a safer alternative to deep tracheal suctioning (Yang et al., 2023).
Rashwan et al. (2022) found that 83.3% of patients who underwent STS exhibited no signs of airway mucosal injury, as indicated by clear secretions. In contrast, 44.4% of patients in the DTS group experienced severe airway mucosal injury characterized by bloody secretions. Additionally, 71.1% of patients subjected to DTS reported high stress levels, compared to only 10% in the STS group.
Kostekli et al. (2022) also found no statistically significant differences between the two suctioning methods. However, they noted that STS caused fewer fluctuations in blood pressure (BP) and HR and had more favorable effects on SaO2 levels, pain intensity, and mucosal trauma compared to DTS. Li et al. (2021) studied the impact of both techniques on 144 MVPs and reported greater fluctuations of vital signs (HR, respiratory rate [RR], and pulse pressure) and more frequent airway bleeding in the DTS group than in the STS group. They found no significant differences between the two groups in postsuctioning oxygen saturation (SpO2) and pain level, although tracheal clearance appeared to be more effective in the DTS group. Ahmed et al. (2017) evaluated the effects of STS versus DTS on the hemodynamic parameters of 60 MVPs. They reported no significant differences in pulse, BP, PaCo2, HCo3 and PaO2 between the two techniques; however, significant differences were found in SaO2 and RR (21.20 ± 4.745 vs. 17.27 ± 2.651, respectively).
Ensuring the safe and effective implementation of TS in MVPs remains a critical challenge. Considering the limited number of comparative studies, there is insufficient evidence to determine the superiority of one suctioning technique over the other. Furthermore, the literature provides little insight into which method better preserves tissue perfusion and cardiovascular stability in CIPs. Therefore, this study was conducted to evaluate the effects of DTS and STS on cardiovascular indices and suction-induced complications among mechanically ventilated patients.
Specific Objectives
To compare the effects of shallow tracheal suctioning and deep tracheal suctioning on cardiovascular parameters specifically heart rate, blood pressure, respiratory rate, and oxygen saturation in mechanically ventilated patients.
To evaluate the incidence of suction-induced complications, including hypoxemia, cardiac dysrhythmia, tracheal tissue injury, and increased intracranial pressure, associated with shallow versus deep tracheal suctioning.
Methods
This study was conducted and reported in accordance with the CONSORT (Consolidated Standards of Reporting Trials) guidelines to ensure transparency and completeness of reporting.
Study Design
A randomized controlled trial (RCT) with a pretest/post-test equivalent control group design was conducted to compare the effects of DTS and STS on cardiovascular indices in mechanically ventilated ICU patients. This design was selected to ensure a rigorous comparison between the two suctioning techniques while minimizing selection bias through randomization. A true experimental approach was essential to establish cause-and-effect relationships between the suctioning techniques and patients’ physiological responses.
Study Setting
The study was conducted in three trauma ICUs at a tertiary-care teaching hospital located in [El-Mansoura, Egypt]. These units specialize in admitting critically ill adult patients of both genders presenting with a wide range of traumatic injuries, including neurological, thoracic, abdominal, and musculoskeletal traumas. On average, each unit includes 10 beds and admits approximately 50 to 60 ICU patients per month, and have a 1:2 nurse to patient ratio.
Research questions
What are the effects of DTS compared to STS on cardiovascular indices among mechanically ventilated patients in the ICU? Does the incidence of suction-induced complications differ between patients undergoing DTS and those receiving STS?
Sample and Sampling Technique
A total sample of 120 mechanically ventilated patients was recruited from the three ICUs for the study. Specifically, 39 patients were enrolled from trauma ICU 1, 38 patients from trauma ICU 2, and 43 patients from trauma ICU 3. The required sample size for the two study groups (STS and DTS), accounting for an anticipated dropout rate of 15%, was calculated using the results of Ahmed et al. (2017) and Clinical Statistical Software and based on the primary outcome of mean change in heart rate. The calculation was based on a statistical power of 85%, a significance level (alpha) of 0.05, an expected mean of 42.40 with a standard deviation of 8.745 in the first group, and an expected mean of 34.54 in the second group. A simple random sampling was utilized without replacement, where each eligible patient had an equal chance of being assigned to either the shallow or deep tracheal suctioning group. A computer-generated random sequence was created in a 1:1 allocation ratio. To maintain strict allocation concealment, assignments were placed into sequentially numbered, opaque, sealed envelopes (SNOSE), which were only opened after each participant provided informed consent and was confirmed to meet the eligibility criteria.
Inclusion Criteria
Participants included in the study were intubated, mechanically ventilated patients aged 18 years or older who volunteered to participate. Eligible patients had a CVP catheter, stable vital signs, normal SpO2, adequate urine output, and normal serum sodium, potassium and chloride levels.
Exclusion Criteria
Patients diagnosed with thrombotic-lung disease, cardiac dysrhythmia, or those requiring blood transfusion were excluded from the study. Also, patients receiving inotropic support were excluded from the study.
Ethical Considerations
This study was conducted in accordance with the ethical standards outlined in the Declaration of Helsinki and was approved by the institutional Review Board at the College of Nursing (Ref No: 0589). Informed consent was obtained from all eligible patients prior to participation. For patients who were cognitively unable to provide consent due to sedation, delirium, or coma, informed consent was obtained from their legally authorized representatives (typically close family members), in accordance with institutional ethical guidelines. This consent included the participants’ agreement to take part in the study and their understanding of their right to withdraw at any time without consequence. Participation was entirely voluntary, and patients were assured of their right to withdraw at any time without affecting their care. Data privacy, anonymity, and confidentiality were rigorously maintained throughout the study. All personal identifying information was removed from the data, and participant identifiers were replaced with unique codes to ensure anonymity. Only authorized personnel involved in the study had access to the data. Data were stored securely in encrypted digital files on password-protected devices, and physical copies of data were stored in locked cabinets. In addition, we informed all participants (or their legal representatives) about the study's data protection measures and their right to withdraw at any time without consequence. All data were used exclusively for research purposes and were not shared with any third party.
Instruments
A structured observational flowsheet was used for data collection. The flowsheet consisted of four parts: (1) patient baseline characteristics, (2) suction-related practices, (3) cardiovascular indices flowchart, and (4) suction-related complications. The first part, baseline characteristics, involved demographic information (e.g., age and gender) and clinical data (e.g., admission date, diagnosis, ventilator mode, type and size of TT, and sedation received). The second part, suction-related practices, was used to document suctioning procedures for each patient, including the suction method, suction depth, frequency of suctioning, and hyperoxygenation used. The third part was a cardiovascular indices flowchart, which recorded patients’ cardiovascular parameters at four times: before suctioning, immediately after, 5 min after, and 10 min after suctioning. Parameters included HR, SBP, DBP, SpO2, mean arterial pressure (MAP), RR, partial pressure of end-tidal carbon dioxide (etCO2), and CVP. The fourth part was an observational sheet documenting suction-related complications, including hypoxemia, cardiac dysrhythmia, and tracheal tissue injury (as reflected by visible blood in suction catheter or ETT).
The study tool's content validity was established through review by a panel of 3 specialists in critical care, who assessed the relevance, clarity, and comprehensiveness of the items. Construct validity was assessed through a combination of expert feedback and statistical techniques, such as factor analysis, to ensure the tool accurately measures the intended constructs. The reliability of the tool was assessed using Cronbach's α coefficient, which yielded an acceptable value of 0.815.
Data Collection
Data were collected from January to October 2024. Following informed consent, baseline demographic and clinical data were obtained directly by the researchers from patients’ medical records. All suction-related practices were assessed by the researchers prior to suctioning. Cardiovascular parameters were monitored and recorded by the researchers using a standardized flowchart at four intervals: before suctioning, immediately after, 5 min after, and 10 min after suctioning. Importantly, only one standardized suction procedure per patient, performed by the research team, was assessed and included in the data analysis. This procedure was conducted once patients met the clinical indication for suctioning and after confirming their eligibility and stability. Suctioning procedures conducted by other ICU staff throughout the patient's stay were not controlled by the study and may have varied in technique. Additionally, suction-related complications were observed and documented by the researchers during and after each suctioning procedure based on clinical signs and routine ICU assessments. These included changes in respiratory status, auscultation findings, oxygen saturation, hemodynamic instability, or the presence of visible blood in secretions. All researchers involved in data collection were trained in standardized administration procedures to ensure consistency and reliability.
Intervention
Ethical committee approval and institutional permission were obtained prior to initiating the study. Informed consent was secured from all eligible patients or their legal representatives after explaining the study's purpose, procedures, potential risks, and benefits. Patients who met the inclusion criteria were randomized into two groups (DTS and STS) using a computer-generated randomization list prepared by an independent research assistant who was not involved in patient recruitment or data collection. Demographic and clinical data were extracted from patient medical records by the researchers.
Subsequently, 60 patients in the control group received DTS, while 60 patients in the intervention group underwent STS. Cardiovascular indices were assessed by the researchers at four specific times: before suctioning, immediately after suctioning, 5 min postsuctioning, and 10 min postsuctioning.
All suctioning procedures were single, standardized procedures performed by the research team only following the American Association for Respiratory Care (AARC, 2010) guidelines. Prior to suctioning, all patients were allowed to rest for 15 min without exposure to painful stimuli. Suctioning was initiated when clinical signs such as crackles, elevated RR, HR, BP, coughing, cyanosis, sweating, restlessness, or visible secretions in the ETT were observed. All patients were pre-oxygenated with 100% oxygen for 2 min before the procedure. A standardized suction pressure (100–120 mmHg) was applied for all participants to ensure consistency and safety (Al-Mayetiazidy et al., 2024; Kostekli et al., 2022).
For the STS group, the 14 French (14 Fr) suction catheter was inserted to the predetermined depth of 33 cm. In this study the ETT internal diameter which was used for all patients enrolled in the study ranging from 7.0 to 8.0 mm and ETT length of 33 cm. Consistent with standard clinical practice for adult patients, which recommend that the suction catheter should not exceed half the internal diameter of the ETT, a 14 Fr catheter was selected (Liao et al., 2019; Li et al., 2021).
For the STS group, the suction catheter was inserted to a depth of approximately 33 cm corresponding to the full length of the ETT. This depth was based on evidence-based recommendations for STS, which advise that the catheter should not extend beyond the proximal end of the ETT. This approach ensured that the catheter remained entirely within the ETT lumen, thereby avoiding contact with the tracheal wall and minimizing the risk of mucosal injury (Shamali et al., 2019). In contrast, DTS was performed by advancing the catheter until resistance was felt at the carina, then withdrawing it approximately 1 cm before applying suction, also for no more than 10 s prevent hypoxia and other adverse effects (Al-Mayetiazidy et al., 2024). A second or third suction attempt was performed, if necessary, until the patient's vital signs stabilized. Following suctioning, all patients were hyperoxygenated with 100% oxygen for 1 min.
Data Analysis
Collected data were analyzed using the SPSS software program (version 20.0). Frequencies, percentages, means, and standard deviations were used to describe patients’ baseline characteristics and measurement outcomes. Comparisons between patients’ demographic and clinical data were performed using the Chi-square test and independent-sample t-tests. The normality of the data was assessed using the Kolmogorov-Smirnov test. Independent samples t-test were also used to compare continuous variables between the two study groups. To assess the impact of suctioning technique and time on physiological responses, a two-way analysis of variance (ANOVA) was conducted. The independent variables were suctioning technique (deep vs. superficial) and time (presuctioning, and immediately, 5 min, and 10 min postsuctioning), while the dependent variables included cardiovascular indices such as HR, MAP, RR, and SpO₂. The Greenhouse-Geisser correction was applied in cases where the assumption of sphericity was violated, as indicated by a statistically significant Mauchly's sphericity test (p < .05). Repeated measures analysis of variance was used to assess changes in cardiovascular variables including HR, MAP, RR, and SpO₂ across different time points (presuctioning, immediately, 5 min, and 10 min postsuctioning) and between suctioning techniques (deep vs. superficial). Statistical significance was set at p < .05 for all analyses.
Results
Patient's Baseline Characteristics
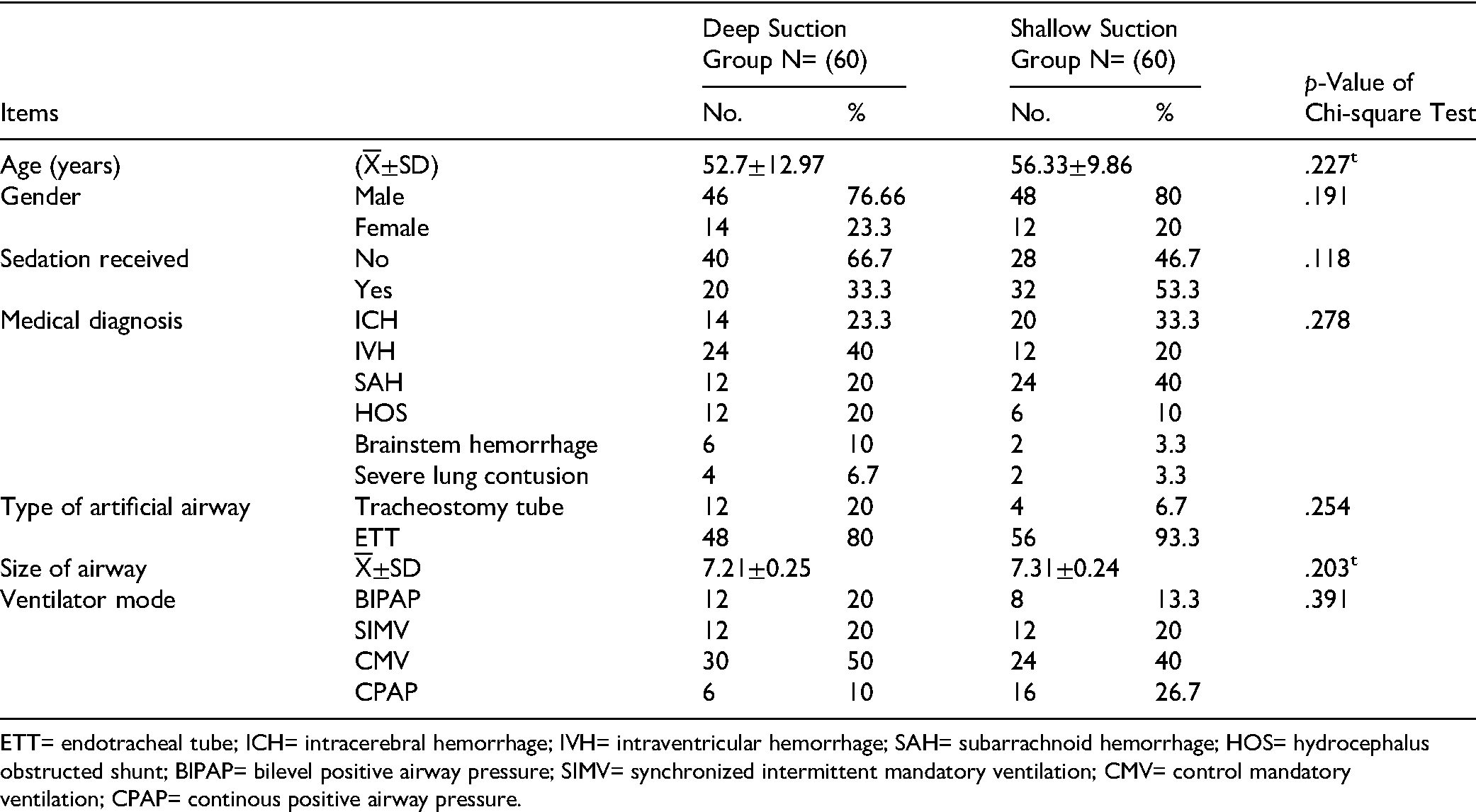
Table 1 shows that male patients were predominant in both groups, with 60% in the DTS group and 80% in the STS group. The mean age was 52.7 ± 12.97 years in the DTS group and 56.33 ± 9.86 years in the STS group. The most common medical diagnosis was intraventricular hemorrhage in the DTS group and traumatic subarachnoid hemorrhage in the STS group (40% in each group). Regarding sedation, 66.7% of DTS participants did not receive sedation, whereas 53.3% of STS participants did. Approximately half of the patients were on CMV mode (50% in DTS vs. 40% in STS). Most participants in both groups had endotracheal artificial airways (80% in DTS and 93.3% in STS), with a mean airway size of 7.21 ± 0.25 mm for DTS and 7.31 ± 0.24 mm for STS. The table illustrates that there were no statistically significant differences between the two groups regarding baseline characteristics, as assessed by the chi-square test for categorical variables and the independent t-test for continuous variables such as mean age and suction catheter size.
Distribution of the Participants According to Patients’ Baseline Data.
Further, before the study began, 150 patients were assessed for eligibility. Twenty-four were excluded for not meeting the inclusion criteria. During the allocation phase, one patient in the STS group and three patients in the DTS group were excluded due to hemodynamic instability before the suctioning procedure. During follow up, two patients in the STS group were excluded because they required deep suctioning due to excessive respiratory secretions (Figure 1).

Patients’ Flow Process.
Suction-Related Practices
Table 2 indicates that there were no statistically significant differences between the DTS and STS groups regarding all suction-related practices, as determined by the chi-square test. All patients underwent open TS. The majority received mechanical hyperoxygenation, with 80% in the DTS group and 60% in the STS group. Additionally, the number of suction catheter insertions ranged from two to three times in both groups, with the majority undergoing a maximum of two insertions (80% in the DTS group and 90% in the STS group). A smaller percentage in each group required a third insertion.
Comparison of Postsuctioning Complication Rate Between Shallow and Deep Tracheal Suction Groups.

N=number; NA=not applicable.
Cardiovascular Indices
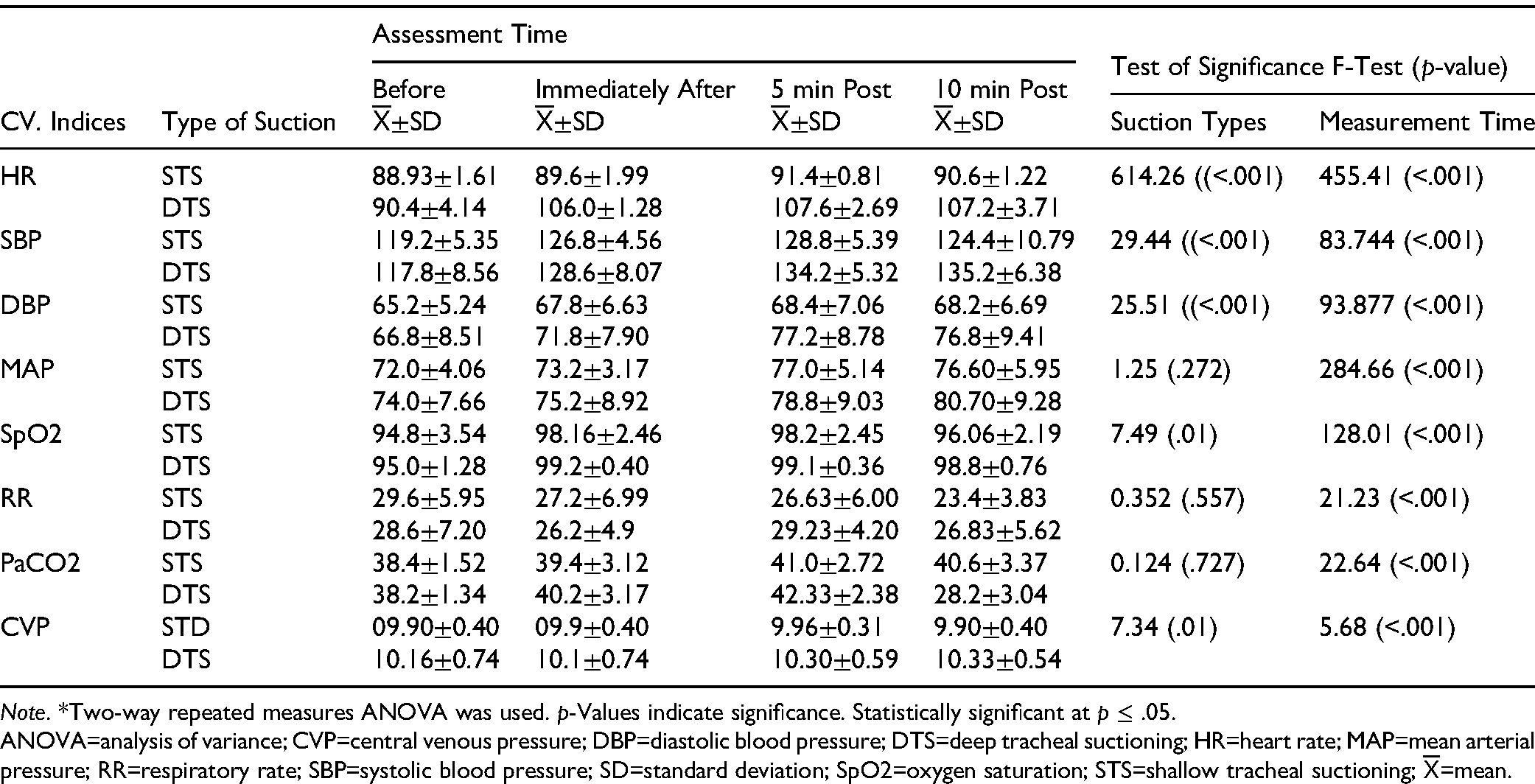
Table 3 shows that, based on independent sample t-test results, HR and DBP were significantly elevated in the DTS group immediately, 5 min, and 10 min postsuctioning compared to the STS group (p = .001). Statistically significant differences in SBP and RR were observed between the groups at 5 and 10 min postsuctioning (p < .001). SpO₂ values were higher in the DTS group at all three time points (p = .027, .027, and .001, respectively). MAP was also significantly higher in the DTS group at 10 min postsuctioning (80.70 ± 9.28 vs. 76.60 ± 5.95). Conversely, CVP was significantly lower in the STS group at 5 min and 10 min postsuctioning (p = .009 and .001, respectively). Finally, PaCO₂ levels increased significantly in the DTS group by 5 min postsuctioning and then significantly decreased by 10 min.
Comparison of Mean Cardiovascular Indices Throughout Tracheal Suctioning Between Deep and Shallow Suctioning Groups.

Table 4 demonstrates significant changes in cardiovascular and respiratory parameters across the study time points for both groups, as assessed by a two-way repeated measures analysis of variance (ANOVA). This analysis assessed the effects of suctioning technique (DTS vs. STS), time (before, immediately after, 5 min, and 10 min postsuctioning), and their interaction on cardiovascular and respiratory parameters. The mean HR was significantly higher immediately, 5 min, and 10 min postsuctioning compared to presuctioning in both groups, with a more pronounced increase in the DTS group (p = .001). Mean DBP and SBP values remained consistently higher in the DTS group than in the STS group across all postsuctioning measurements (p = .001). SaO2 levels increased immediately, at 5 min, and at 10 min postsuctioning compared to presuctioning in both groups; however, a decline was observed at 10 min postsuctioning, showing a highly significant difference (p < .001). RR was highest before suctioning and significantly decreased at 5 min and 10 min postsuctioning in the STS group, with a highly significant difference (p < .001).
Comparison of Cardiovascular Indices at Different Measurement Times According to Endotracheal Suctioning Types.
Suction-Related Complications
As only a single suctioning procedure per patient was assessed in this study, complications that typically develop over multiple suctioning events or longer ICU stays, such as VAP, bronchospasm, and atelectasis, were not considered direct outcomes of this study and have been excluded from the analysis.
However, immediate suction-related complications observable during or shortly after the single suction procedure, such as hypoxemia, tracheal tissue injury, and cardiac dysrhythmia, were monitored and are reported here.
The Chi-square test was employed to examine differences in suction-related complications between the DTS and STS groups. Figure 2 illustrates that tracheal tissue injury occurred in 100% of patients in the DTS group versus 46.7% in the STS group, and this difference was also statistically significant (p < .001).
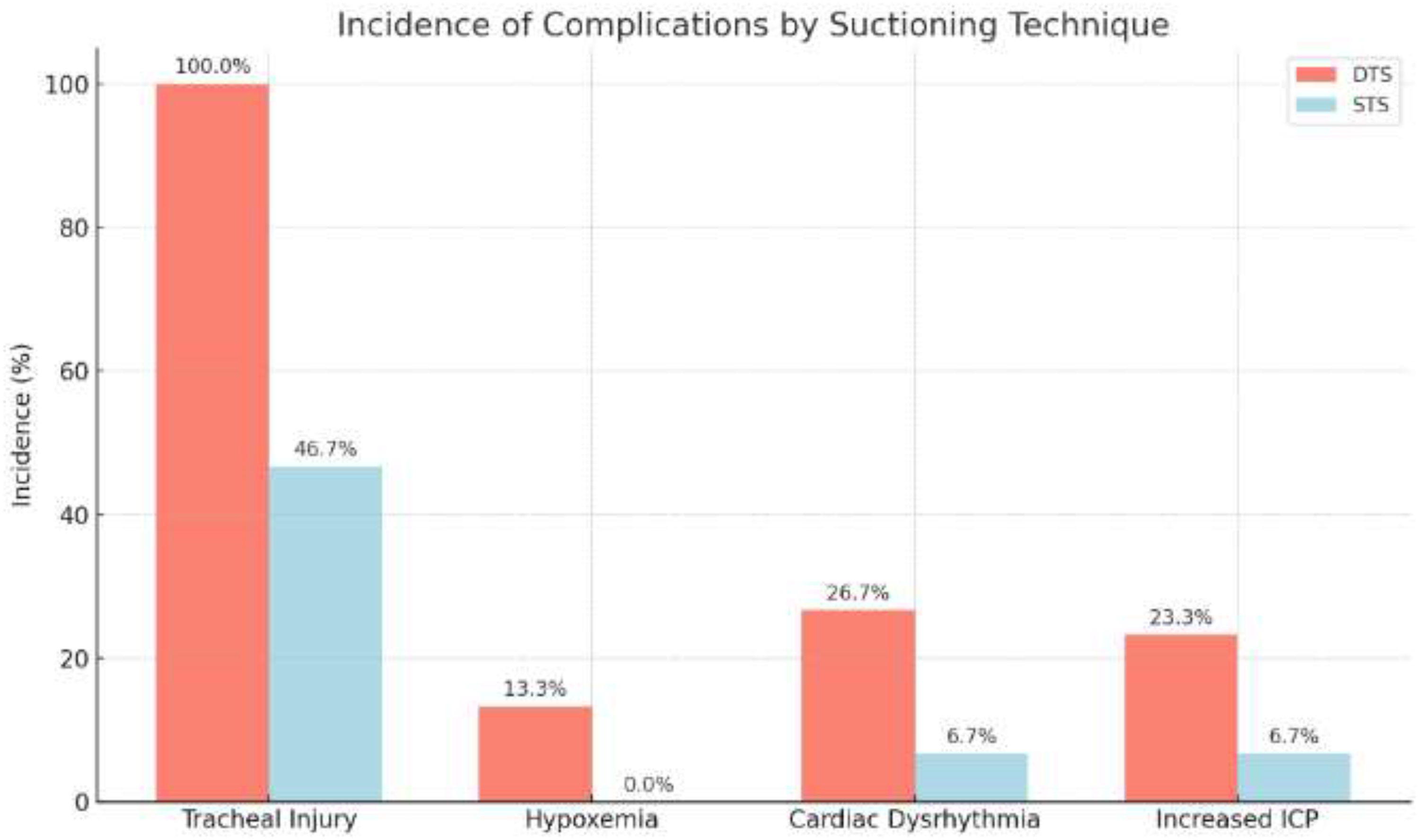
Comparison of Postsuctioning Complication Rate Between Shallow and Deep Tracheal Suction Groups.
The incidence of hypoxemia was significantly higher in the DTS group (13.3%) compared to 0.0% in the STS group (p = .040). A Chi-square test also revealed a statistically significant difference in the occurrence of cardiac dysrhythmia, affecting 26.7% of the DTS group and 6.7% of the STS group (p = .038).
A Chi-square test showed no statistically significant difference in the incidence of increased ICP between the DTS group (23.3%) and the STS group (6.7%) (p = .145).
Discussion
This randomized controlled trial compared the effects of DTS and STS on cardiovascular indices and suction-induced complications among mechanically ventilated patients. The findings revealed that DTS was associated with significantly higher elevations in heart rate, blood pressure, and incidence of hypoxemia and tracheal injury compared to STS.
Suction-Related Practices
The open suction technique was the primary method used for respiratory secretions removal in selected ICUs. The current study found no statistically significant difference between the DTS and STS groups regarding the frequency of suctioning required to effectively clear the airway. These results may suggest that institutional practices play a more influential role than individual technique selection alone. It is possible that a standard ICU culture of frequent open suctioning, as seen in many lower-resource settings, may mask subtle differences in technique-related suction frequency. Future studies should examine how unit-specific protocols and caregiver training shape these practices. This finding is consistent with Shamali et al. (2019), who also reported no significant difference in suction frequency between the two techniques. In contrast, a study by Ahmed et al. (2017) demonstrated that the STS group required catheter insertions three to four times more than the DTS group, with a statistically significant difference reported.
Patients’ Cardiovascular Indices Throughout TS
The current study demonstrated that HR increased following suctioning in both groups. However, in the STS group, HR returned to baseline within 10 min, whereas it remained elevated in the DTS group. This finding aligns with evidence indicating that suctioning activates the sympathetic nervous system, leading to increased HR (Doumit et al., 2016). While these findings are in line with sympathetic nervous system activation, they raise further questions about patient-specific vulnerability. For instance, do patients with autonomic dysfunction, traumatic brain injury, or pre-existing hypertension respond more adversely to DTS? These subgroups could be at greater risk from the hemodynamic stress induced by deep suctioning and warrant separate evaluation. Similarly, Li et al. (2021) reported greater HR fluctuations in the DTS group compared to STS. Consistently, Kostekli et al. (2022) observed increased SBP and HR at 1 and 5 min postsuctioning, which normalizing within 30 min for both groups. Additionally, Al-mayetiazidy et al. (2024) reported that HR significantly increased immediately after DTS more than STS, returning to normal after 10 min. Conversely, Shamali et al. (2019), found no significant differences in mean HR between the two groups before, immediately after, and 10 min following suctioning.
The current study found statistically significant differences in participants’ BP between the DTS and STS groups at 5 and 10 min postsuctioning. This increase may be attributed to the stimulation of adrenaline and noradrenaline secretion (Afenigus et al., 2021). Similarly, Liao et al. (2019) reported significant differences SBP between patients undergoing DTS and STS. Conversely, Li et al. (2021) observed higher mean SBP in the STS group compared to the DTS group. In line with the current findings, Al-Mayetiazidy et al. (2024) reported that both SBP and MAP significantly increased immediately after DTS compared to STS but returned to baseline after 10 min.
The present study found that postsuctioning SpO2 values were significantly higher in the DTS group compared to the STS group, possibly due to bronchospasm and atelectasis associated with shallow technique. This contrasts with the findings of Al-Mayetiazidy et al. (2024) and Ahmed et al. (2017), who reported a significant improvement in oxygen saturation immediately after suctioning in the STS group. Similarly, Kostekli et al. (2022) found no significant difference in SaO2 levels elevation between the two techniques (p > .05). A paradox worth exploring is whether transient SpO₂ gains from DTS offset its risks in specific clinical scenarios, such as in patients with critical secretion loads. Should a tiered suctioning protocol be designed—where STS is the first line and DTS is reserved only for failure of clearance? These are key research questions that future clinical trials could investigate.
In terms of RR, this study observed a significant reduction in both groups following suctioning when compared to presuctioning values. This decrease is likely attributable to improved airway clearance and the effect of hyperventilation during the procedure, which helped alleviate respiratory distress caused by TT obstruction. These results are consistent with Ahmed et al. (2017), who also noted a significant difference in RR between the two groups immediately after suctioning. On the other hand, Al-Mayetiazidy et al. (2024) observed an increase in RR after suctioning in both groups compared to presuctioning values.
Suction-Related Complications
This study assessed the immediate impact of a single suctioning procedure per patient. Therefore, findings related to complications reflect only those that can be clinically detected directly during or shortly after a single suctioning event. The current study observed a significantly higher incidence of tracheal tissue injury in the DTS group than in the STS group. This could be due to the deeper catheter insertion and the stronger negative pressure applied during DTS, increasing the risk of trauma to the tracheal wall. These findings are consistent with the work of Rashwan et al. (2022) and Shamali et al. (2019), who all reported higher rates of tracheal injury associated with DTS compared to minimally invasive suction techniques. These findings are matched with those of Abdallah et al. (2021), who noted that DTS can irritate the tracheal mucosa, resulting in bronchial edema, inflammation, severe coughing, and airway stenosis, spasm and even bleeding. Furthermore, Elmansoury and Said (2017) and Eid et al. (2022) demonstrated that deep tracheal suctioning may lead to severe complications such as mucosal trauma, potential tracheal or bronchial perforation, bleeding, as well as notable cardiovascular disturbances including bradycardia and hypotension.
Moreover, the study found that VAP was prevalent in both groups, likely due to bacteria translocation from the upper to the lower airways during suctioning.
Finally, the incidence of hypoxemia was significantly greater in the DTS group than in the STS group. This is supported by previous study (Shamali et al., 2019), which reported that STS is associated with fewer complications such as bleeding, less airway trauma, hemodynamic instability, and hypoxemia. However, Li et al. (2021) found no significant differences between DTS and STS in terms of oxygen saturation, analgesia, or sedation scores.
In summary, while this study adds to the existing body of knowledge by reinforcing that STS is safer and better tolerated than DTS in terms of short-term outcomes, it also opens the door to new hypotheses. Future research should focus on: (1) patient-specific predictors of tolerance to DTS, (2) the impact of ICU protocols and suctioning culture on outcomes, (3) longitudinal effects of repeated suctioning techniques, and (4) developing hybrid or escalation suctioning models that balance safety and efficacy.
Study Strength
This study provides a comprehensive comparison of deep and shallow tracheal suctioning techniques, offering valuable insights into their effects on cardiovascular indices and suction-induced complications in mechanically ventilated patients. By utilizing objective physiological measurements, the study ensures accuracy and reliability in assessing patient responses. The findings highlight the clinical significance of shallow suctioning in reducing complications such as hypoxemia, cardiac dysrhythmia, ventilator-associated pneumonia, and tracheal injury, thereby promoting safer nursing interventions. Additionally, this research contributes to evidence-based practice, supporting ICU nurses in optimizing suctioning protocols to enhance patient safety and care quality. The results have important implications for nursing education, clinical practice, and policy development, advocating for standardized suctioning guidelines in critical care settings.
Study Limitations
This study has some limitations that should be considered. First, it was conducted in a single clinical setting, which may limit the generalizability of the findings to other healthcare institutions with different patient populations and protocols. Second, while efforts were made to control confounding variables, individual patient differences in disease severity and underlying conditions could have influenced the outcomes. Third, the study focused on short-term cardiovascular responses and suction-induced complications, so the long-term effects of deep versus shallow suctioning were not assessed. Lastly, the study relied on clinical observations and physiological measurements without incorporating patient-reported outcomes, which could provide additional insights into the comfort and tolerability of different suctioning techniques. Future research with multicenter trials, repeated procedure assessments and longer follow-up periods is recommended to validate and expand upon these findings.
Implications for Practice
The findings of this study have important implications for nursing practice, particularly in critical care settings. By demonstrating that shallow tracheal suctioning effectively clears secretions while minimizing cardiovascular alterations and suction-induced complications, this research supports the adoption of evidence-based suctioning techniques that enhance patient safety and comfort. Implementing shallow suctioning as a standard practice in ICUs can reduce the risk of hypoxemia, cardiac dysrhythmia, ventilator-associated pneumonia, and tracheal injury, ultimately improving patient outcomes. Additionally, these findings can inform nursing education and training programs, ensuring that critical care nurses are equipped with best practices for airway management. The study also highlights the need for updated clinical guidelines and institutional protocols that prioritize less invasive suctioning methods to optimize care quality for mechanically ventilated patients.
Conclusions
This study examined the impact of STS versus DTS on cardiovascular indices and suction-induced complications among MVPs in ICUs. The results demonstrated that STS was associated with lower incidence rates of suction-induced complications such as VAP, tracheal tissue injury, hypoxemia, and cardiac dysrhythmia, compared to DTS, which had significantly higher complication rates. Cardiovascular parameters, including HR, BP, and RR, showed significant fluctuations in the DTS group immediately postsuctioning, whereas changes in the STS group were less pronounced. The incidence of increased ICP was higher in the DTS group, although not statistically significant, while the incidence of bronchospasm was notably higher in the STS group. These findings support the clinical benefit of STS in minimizing the adverse effects associated with suctioning, making it a preferable technique for patients in critical care. Based on the observed benefits, we recommend the implementation of STS in ICU settings, particularly for patients at risk for suction-induced complications. Future studies could expand on these findings by exploring the effectiveness of both techniques in nontrauma ICU patients.
Supplemental Material
sj-docx-1-son-10.1177_23779608251374140 - Supplemental material for Impact of Deep Versus Shallow Tracheal Suctioning on Cardiovascular Indices and Suction Induced Complications Among Mechanically Ventilated Patients
Supplemental material, sj-docx-1-son-10.1177_23779608251374140 for Impact of Deep Versus Shallow Tracheal Suctioning on Cardiovascular Indices and Suction Induced Complications Among Mechanically Ventilated Patients by Mona Mohamed El-Hady, Lisa Babkair, Ruba M Alharazi, Sohad Mohammad wally Noorsaeed and Marwa Mehrez Mahmoud Ali in SAGE Open Nursing
Supplemental Material
sj-rar-2-son-10.1177_23779608251374140 - Supplemental material for Impact of Deep Versus Shallow Tracheal Suctioning on Cardiovascular Indices and Suction Induced Complications Among Mechanically Ventilated Patients
Supplemental material, sj-rar-2-son-10.1177_23779608251374140 for Impact of Deep Versus Shallow Tracheal Suctioning on Cardiovascular Indices and Suction Induced Complications Among Mechanically Ventilated Patients by Mona Mohamed El-Hady, Lisa Babkair, Ruba M Alharazi, Sohad Mohammad wally Noorsaeed and Marwa Mehrez Mahmoud Ali in SAGE Open Nursing
Footnotes
Acknowledgments
The authors would like to acknowledge and thank the participating institution and all participants.
ORCID iDs
Ethics Approval Statement
This study was conducted in accordance with ethical standards outlined in Declaration of Helsinki and approved by ethical approval committee at Nursing college—Mansoura University—Egypt (Ref No 0589). Also an official institutional approval from Emergency Hospital and Main Mansoura University Hospital was obtained to carry out the study.
Informed Consent Statement
Written informed consent was obtained from all participants prior to their inclusion in study.
Author Contributions
ME-H and MM was involved in conceptualization, data collection, formal analysis, original draft, writing—review & editing, and supervision; LB, RA, and SN in conceptualization, formal analysis, writing original draft, and visualization.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.