
Abstract
Introduction
Critically ill patients experience various stressful symptoms of discomfort, including dyspnea, pain, and sleep disruption. Notably, ventilated patients have difficulty self-reporting discomfort symptoms. Nurses need to assess discomfort symptoms to alleviate them, but limited research exists on discomfort symptom assessment and management in critically ill patients.
Objective
To identify the practices, attitudes, and barriers among nurses related to the assessment of discomfort symptoms in mechanically ventilated patients.
Methods
Using a cross-sectional, descriptive study design, a web-based survey was conducted between May and June 2022 with critical care nurses sampled through Japanese academic societies and social networking services. The survey contained questions relative to the above-stated objective. Descriptive statistical analysis was performed without sample size calculation because of the descriptive and exploratory nature of this study.
Results
There were 267 respondents to the questionnaire. The discomfort symptoms that nurses perceived as important to assess were pain (median 100 [interquartile range, IQR 90–100]), insomnia (99 [80–100]), and dyspnea (96.5 [75–100]). Most participants (89.8%) routinely assessed pain in mechanically ventilated patients using a scale; however, other discomfort symptoms were assessed by less than 40% (dyspnea [28.4%], fatigue [8.1%], thirst [13.1%], insomnia [37.3%], and anxiety [13.6%]). Two major barriers to assessing discomfort symptoms were lack of assessment culture within the intensive care unit and lack of knowledge of the relevant evaluation scales.
Conclusions
Nurses were aware of the importance of using scales to assess the discomfort symptoms experienced by mechanically ventilated patients. However, except for pain, most nurses did not routinely use scales to assess discomfort symptoms. Barriers to routine discomfort symptom assessment included the lack of an assessment culture and the lack of knowledge of the assessment scales. Clinicians should be educated regarding the existence of validated rating scales and develop additional rating scales utilizable for minor discomforts in mechanically ventilated patients.
Introduction
Discomfort is an unpleasant physical or emotional feeling or sensation and physical or emotional negative state; and the natural response to it is to avoid or reduce the source of the unpleasant feeling by self-report either via verbal or nonverbal behavioral cues (Ashkenazy & DeKeyser Ganz, 2019). Critically ill patients experience a variety of stressful discomforts, including difficulty breathing, pain, and sleep disruption (Danielis et al., 2020). Nurses need to be attentive to these discomfort symptoms on a daily basis, and adequate assessment is necessary to alleviate them. Attending to various symptoms of discomfort is also important from a patient-centered care perspective. Vincent et al. (2016) emphasized patient-centered care as well as analgesia and sedation to manage and prevent pain, anxiety, agitation, delirium, and immobility, with early comfort as a clinical priority. Discomfort symptoms in critically ill patients are also affected by noise, lighting, and medical devices in the intensive care unit (ICU) (Baumstarck et al., 2019; Kalfon et al., 2016). Additionally, pain, one of the commonest symptoms of discomfort, can be exacerbated by procedures and care such as position changes, tracheal suctioning, drain removal, and arterial line insertion. These procedures and care have also been associated with emotional distress (Puntillo et al., 2018). Therefore, medical procedures and nursing practices may contribute to increased symptoms of discomfort. In a survey regarding unpleasant and pleasant memories administered to 250 patients with a history of receiving mechanical ventilation, of the 80% of patients who remembered being in the ICU, 70% reported recalling unpleasant memories (Samuelson, 2011). Additionally, in previous studies (Aitken et al., 2017; Baumstarck et al., 2019; Castillo et al., 2016; Puntillo et al., 2010, 2014), ICU patients reported experiencing uncomfortable symptoms such as pain, thirst, fatigue, dyspnea, anxiety, and sleep deprivation.
Furthermore, nurses’ care for patients’ discomfort symptoms is important not only for the short-term effects of their stay in the ICU but also for reducing long-term negative effects after they leave the ICU. This is because discomfort symptoms are known to have long-term adverse effects in critically ill patients, which are referred to as post-intensive care syndrome (PICS). PICS is defined as a new or worsening impairment of physical, cognitive, or mental health that occurs and persists after hospitalization for a critical illness (Needham et al., 2012). A previous study (Kalfon et al., 2019) reported that reducing discomfort in the ICU was effective in reducing posttraumatic stress disorder (PTSD) symptoms 1 year after ICU discharge. Therefore, nurses must address the discomfort symptoms of critically ill patients to optimize long-term outcomes and quality of life.
Review of Literature
To alleviate discomfort symptoms in critically ill patients and prevent long-term complications, nurses must use discomfort symptom assessment tools. Chanques et al. (2015) suggest that key symptoms such as pain, thirst, anxiety, dyspnea, and insomnia should be evaluated daily. The Visual Analog Scale and Numerical Rating Scale can be used to assess pain, thirst, anxiety, dyspnea, and insomnia in patients who are able to self-report (Chanques et al., 2015). In addition, specific discomfort symptom tools include the Richards-Campbell Sleep Questionnaire (RCSQ; Richards et al., 2000) for sleep and the Hospital Anxiety Depression Scale (HADS; Zigmond & Snaith, 1983) for anxiety. For patients who cannot self-report, the Critical Care Pain Observation Tool (CPOT; Gélinas et al., 2006) and Behavioral Pain Scale (BPS; Payen et al., 2001) can be used to assess pain. The Respiratory Distress Observation Scale (RDOS) is used to assess dyspnea (Campbell et al., 2010). In addition, patients who are unable to communicate or are deeply sedated have difficulty self-reporting, so objective assessment tools such as CPOT and BPS should be used with these patients.
Detecting the signs and symptoms of discomfort allows nurses to recognize patient problems early and provide targeted interventions (Randen et al., 2013). However, mechanically ventilated patients are unable to verbally express themselves. It is difficult for them to self-report symptoms of discomfort. Therefore, the patient depends on their discomfort and related symptoms to be assessed and controlled by the caregivers. It has been reported that discomfort symptoms are easily missed by caregivers; there is a perception gap between caregivers and patients, and many discomfort symptoms, such as pain, anxiety, delirium, and breathing difficulties, are underestimated (Binks et al., 2017; Randen et al., 2013). This suggests the need for standardization of the methods for assessing discomfort symptoms in patients who are unable to self-report them verbally.
On the other hand, nurses do not adequately assess even pain, one of the most prevalent and distressing physical symptoms experienced by critically ill patients. Regardless of whether patients can self-report their pain or not, the practices and barriers to pain assessment and management for critically ill patients have been identified. Rose et al. (2011) reported that nurses recognized the importance of assessment tools for patients who could not self-report their pain, although they reported that assessment tools were used infrequently. A systematic review (Rababa et al., 2021) identified several barriers perceived by nurses when assessing and managing pain in critically ill patients; these included a lack of knowledge about the use of pain assessment tools, inability to communicate with patients, prescription of analgesics by physicians unrelated to pain score assessment, and lack of standard guidelines and protocols for pain assessment and management. Mechanically ventilated patients experience a variety of discomfort symptoms in addition to pain. Therefore, we focused our attention on the assessment of pain and other discomfort symptoms.
Studies on nurses’ practices and attitudes regarding the assessment of discomfort symptoms other than pain are lacking. Although subjective and objective assessment tools have been developed for discomfort symptoms such as dyspnea, fatigue, thirst, insomnia, and anxiety in critically ill patients, the extent of their actual use is unknown. Therefore, this study aimed to clarify the status of discomfort symptom assessment in mechanically ventilated patients by critical care nurses; this includes identifying the practices, attitudes, and barriers of nurses regarding the assessment of discomfort symptoms. The results of this study may improve the quality of symptom management in patients receiving mechanical ventilation.
Methods
Design
A cross-sectional, anonymous web-based survey was conducted. We collected data from critical care nurses regarding their attitudes, practices, and barriers in assessing discomfort symptoms in mechanically ventilated patients.
Research Questions
What are nurses’ attitudes toward assessing discomfort symptoms in mechanically ventilated patients?
How do nurses practice discomfort symptom assessment in mechanically ventilated patients?
What barriers against discomfort symptom assessment do nurses perceive in mechanically ventilated patients?
Sample
This study utilized a web-based survey conducted from May 30 to June 30, 2022. Critical care nurses were sampled through various professional associations, including the mailing lists of the Japanese Society of Intensive Care Medicine, the Japanese Society of Education for Physicians and Trainees in Intensive Care, and social networking services. We confirmed compliance with the inclusion criteria through the responses to the facility and other questions. The sample size was not calculated a priori because of the descriptive and exploratory nature of this study.
Inclusion/Exclusion Criteria
The inclusion criteria comprised nurses working in an ICU or high-dependency care unit (HDU) who routinely care for adult mechanically ventilated patients. HDUs are hospital units in which patient care levels and costs are between levels found in the ICU and general ward (Ohbe et al., 2021). The following participants were excluded: (a) nurses working in hospitals outside of Japan, (b) nurses not directly involved in ICU/HDU, and (c) nurses working in ICUs where only patients under 18 years of age are admitted.
Ethical Considerations
This study was approved by the Institutional Review Board (approval number: E17). Participants were informed that they would only be asked to complete the questionnaire if they agreed with the purpose of the survey. If they did not consent to participate, they were informed that they could choose not to respond or that they could exit the survey before it was sent.
Variables
All data were collected using the web-based application SurveyMonkey®. The survey consisted of (a) participants’ characteristics (qualifications, education, years of nursing experience, region, facility, department, and number of beds), (b) nurses’ attitudes regarding discomfort symptoms using the scale, and (c) nurses’ practices and barriers in rating each discomfort symptom using the scale. Data collection items related to nurses’ characteristics and facilities were based on previous studies (Alnajar et al., 2021; Hamdan et al., 2022; Kizza & Muliira, 2015; Rose et al., 2011). Each nurse's attitude toward the assessment of discomfort symptoms in patients was rated on a scale from 0 (completely disagree) to 100 (strongly agree) in response to the question “Do you think it is important to assess using a scale?” for each symptom. In addition, respondents were asked, in a closed question format, whether they routinely assessed for each discomfort symptom using a scale. Respondents who did not routinely assess discomfort symptoms were asked about barriers to the assessment of discomfort symptoms (including no culture of assessing, do not know of any tools, low priority of assessing, large workload and/or little time to assess, and no need to assess) (Alnajar et al., 2021; Hamdan et al., 2022; Rababa et al., 2021; Rose et al., 2011).
Data Source (Questionnaire)
As no appropriate surveys were available, an original questionnaire consisting of 28 items was developed to investigate nurses’ attitudes, practices, and barriers in assessing discomfort symptoms in mechanically ventilated patients. The questionnaire was developed by reviewing the relevant literature on discomfort symptoms in mechanically ventilated patients (Alnajar et al., 2021; Chanques et al., 2015; Kizza & Muliira, 2015; Rose et al., 2011; Van Der Woude et al., 2016). Based on the literature, six discomfort symptoms (pain, dyspnea, fatigue, thirst, insomnia, and anxiety) were defined. Questionnaire content validity was reviewed among the researchers. Eight researchers assessed the questionnaire on three issues: relevance, comprehensiveness, and balance (Polit & Beck, 2017), and the eight researchers agreed on all items. All research members had extensive clinical experience in intensive care; five were affiliated with universities and have experience in clinical research. Three of the study members were certified nurse specialists in critical care or certified nurses in intensive care by the Japan Nursing Association.
The questionnaire was then piloted with healthcare professionals experienced in caring for mechanically ventilated patients. The clinical and academic backgrounds and settings of the healthcare professionals who participated in the pilot are shown in Supplemental Table S1. The draft questionnaire was created by all researchers designing the web-based application SurveyMonkey®. A questionnaire for the pilot survey was created using SurveyMonkey®, and the survey link was distributed to the healthcare professionals via email. The results were then collected on the web, and feedback was collected directly from the healthcare professionals. After reviewing their feedback, the number of items was reduced from a maximum of 39–28. As a result, response time was reduced. The final questionnaire was designed and distributed through the web-based application SurveyMonkey®. The survey questionnaire took respondents approximately 6–8 min to complete. The survey link was attached to an email and distributed to the mailing lists of the Japanese Society of Intensive Care Medicine, the Japanese Society of Intensive Care Education and Research, and to social networking services.
Bias
The study utilized an anonymous web survey and participants were recruited via a mailing list; therefore, a selection bias may have existed. Selection bias due to variations in the number of participants per region was addressed by asking the participants about their region. In addition, to minimize response bias, the survey was sent twice during the study period via mail, including reminders. The participants accessed the website URL of the survey attached to the email, and if they consented, they completed the survey. In order to avoid repeated responses, the respondents could only answer the questionnaire once from any device. Furthermore, the respondents were told not to answer the questionnaire if they had already done so.
Statistical Analysis
This study aimed to determine the status of the assessment of symptoms of discomfort in ventilated patients by critical care nurses. A descriptive statistical analysis was performed. Characteristics were presented as numbers and percentages for binary variables and as means and standard deviations (SD) or medians and interquartile ranges (IQR) for continuous variables. Statistical analyses were performed using SPSS version 28.0.1 for Windows (IBM Corp., Armonk, NY, USA). Participants who did not respond to any of the items were excluded from the analysis, and a complete case analysis was conducted.
Results
Sample Characteristics
There were 267 respondents to the questionnaire. Of these, 31 were excluded because of withdrawal from participation (n = 1) or not engaging in ICUs (n = 30). In total, 236 participants were included in this study (Figure 1). Table 1 presents the demographic characteristics of the participants. More than 50% of participants were critical care professionals certified by the Japanese Nursing Association (n = 147, 62.3%). Most participants (n = 208, 88.1%) worked in the ICU. Of these, 193 (81.8%) had more than 6 years of ICU experience. Figure 2 shows the geographic distribution of the facilities where respondents worked.

Flow Chart on the Study. Note. Flow chart of the study population selection. Those who withdrew from the study and were not directly involved in ICU/HDU nursing were excluded. In total, 236 respondents were included in the analysis.

The Geographical Distribution of the Facilities for the Participants. Note. This figure shows the geographical distribution at the prefectural level for the facilities of the 236 participants.
Characteristics of the Participants (N = 236).
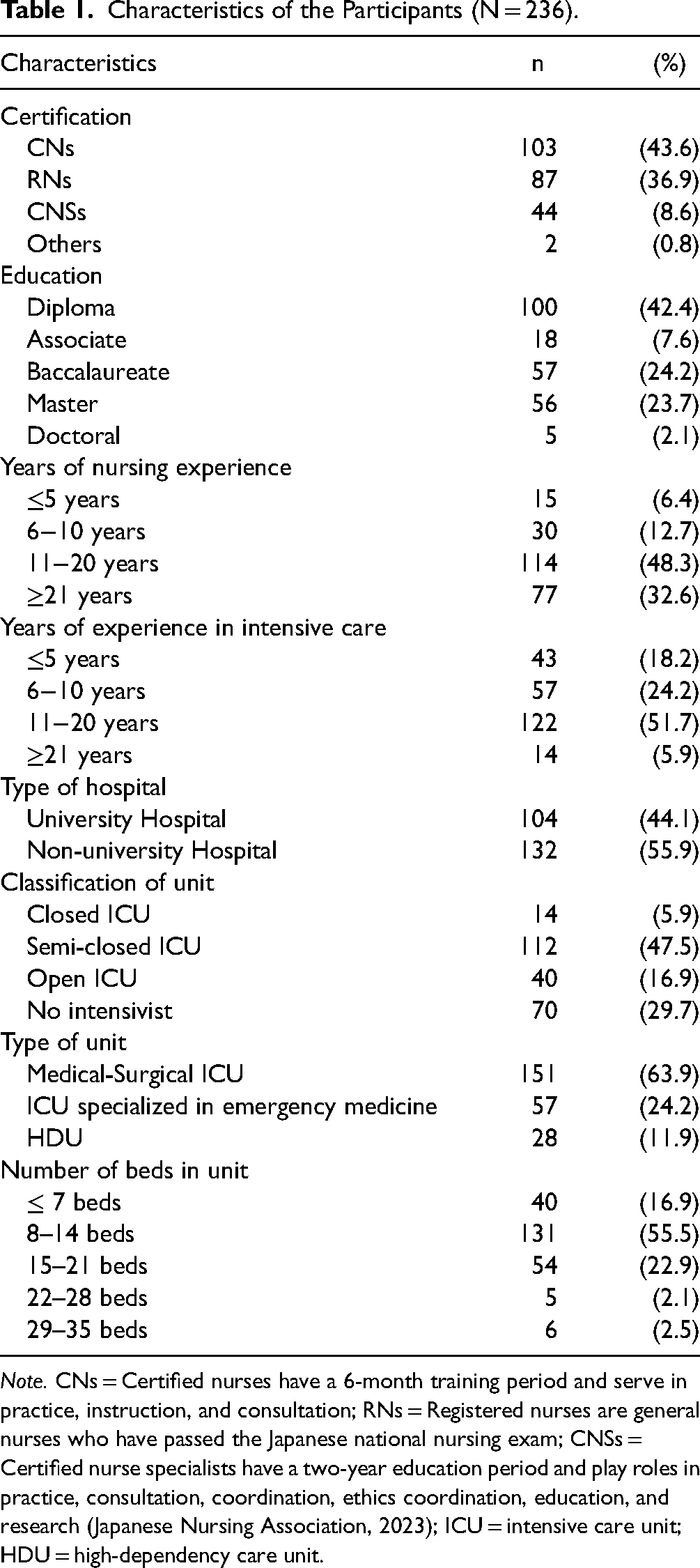
Note. CNs = Certified nurses have a 6-month training period and serve in practice, instruction, and consultation; RNs = Registered nurses are general nurses who have passed the Japanese national nursing exam; CNSs = Certified nurse specialists have a two-year education period and play roles in practice, consultation, coordination, ethics coordination, education, and research (Japanese Nursing Association, 2023); ICU = intensive care unit; HDU = high-dependency care unit.
Nurses’ Attitudes and Practice in the Assessment of Discomfort Symptoms for Mechanically Ventilated Patients
Table 2 shows the nurses’ perceptions of the importance of using the scale to assess discomfort symptoms (pain, dyspnea, fatigue, thirst, insomnia, and anxiety) in mechanically ventilated patients. The discomfort symptoms that nurses perceived as important to assess were pain (median 100 [IQR 90–100]), insomnia (median 99 [IQR 80–100]), and dyspnea (median 96.5 [IQR 75–100]).
Nurses’ Perception of the Importance of Evaluating Symptoms Using a Scale to Assess Discomfort Symptoms in Mechanically Ventilated Patients.
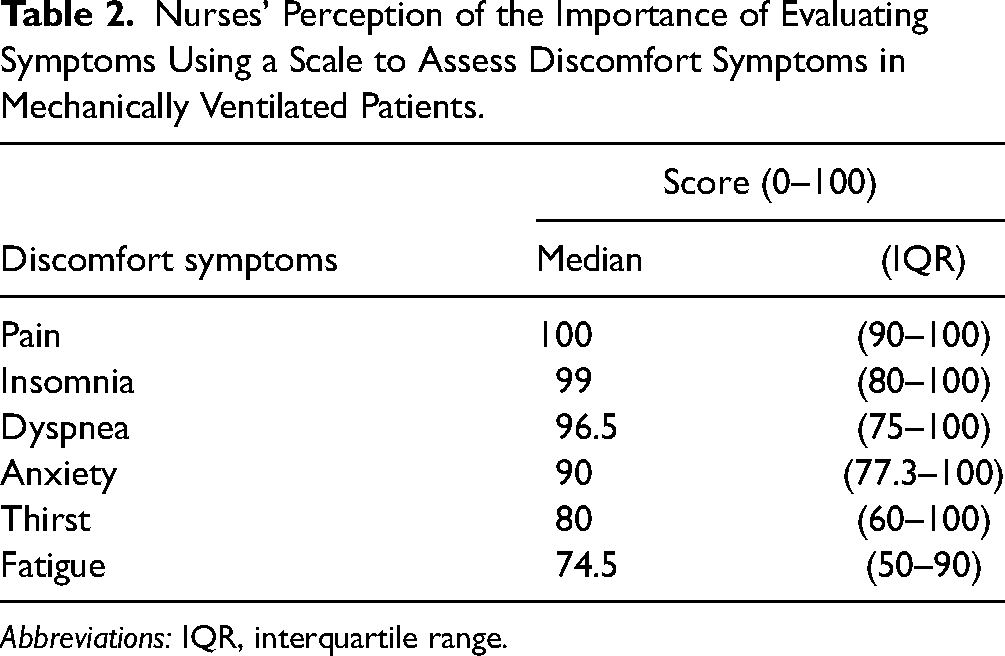
Abbreviations: IQR, interquartile range.
The following table shows the actual assessment of discomfort symptoms in mechanically ventilated patients by the participants (Table 3). Most responders (89.8%) routinely assessed pain in mechanically ventilated patients using a scale; however, other discomfort symptoms were reportedly routinely assessed by less than 40% of the participants (dyspnea [28.4%]; fatigue [8.1%]; thirst [13.1%]; insomnia [37.3%]; and anxiety [13.6%]).
Proportion of Each Symptom Routinely Evaluated Using the Scale.

Note. n (%) Percentage of respondents who answered that they assessed each discomfort symptom using the scale.
Barriers to Routine Assessment Using Scales for Discomfort Symptoms in Ventilated Patients
Table 4 shows the barriers for participants who reported not practicing routine assessment of discomfort symptoms using scales in mechanically ventilated patients. Two major barriers to the assessment of discomfort symptoms were the lack of an assessment culture within the ICU and a lack of knowledge of the scales used to assess discomfort symptoms. Regarding the lack of culture to assess for discomfort symptoms, the most commonly reported symptom relating to this issue was pain (75.0%), followed by dyspnea (63.3%). Regarding the lack of knowledge of assessment tools, thirst (74.6%), fatigue (72.4%), anxiety (70.6%), and insomnia (59.5%) were the commonest symptoms related to this issue. Low priority placed on assessments, increased workload, and a lack of need to assess were relatively minor barriers.
Percentage of Barriers to Conduct Evaluation of Perceived Symptoms.
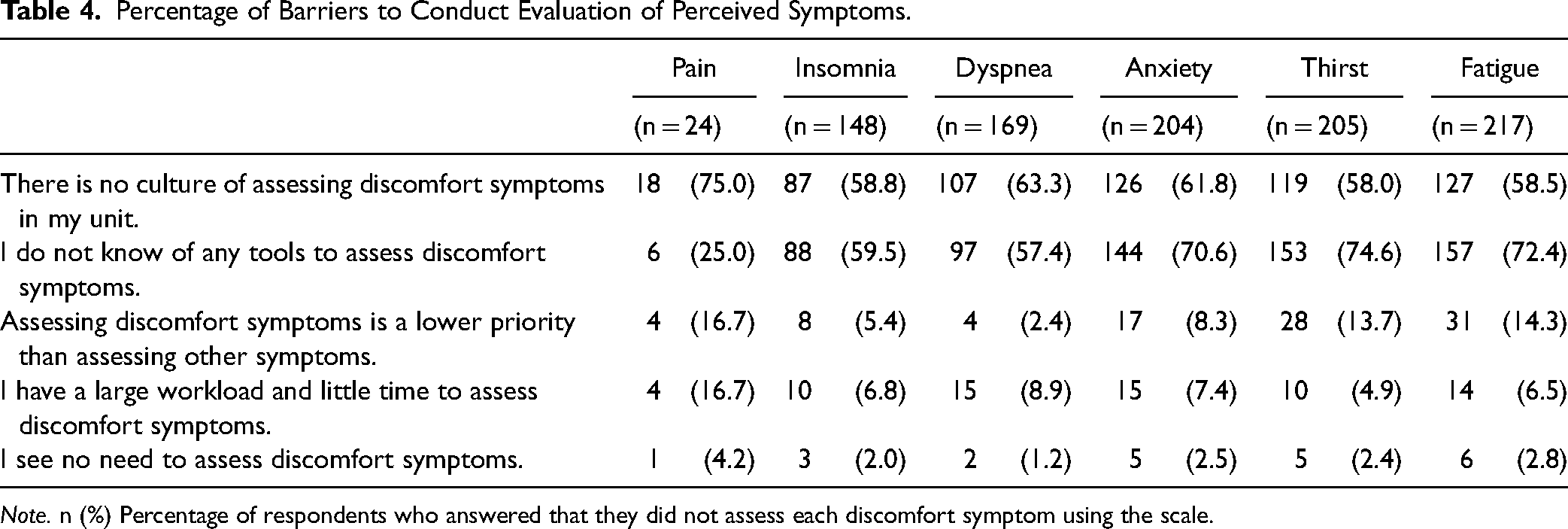
Note. n (%) Percentage of respondents who answered that they did not assess each discomfort symptom using the scale.
Discussion
This study investigated the practice of assessing the symptoms of discomfort in mechanically ventilated patients, and nurses’ attitudes toward symptom assessment. The results of the administered survey showed that nurses were highly aware of the importance of objectively assessing the six discomfort symptoms commonly experienced by patients undergoing mechanical ventilation. Most respondents (89.8%) routinely used a scale to assess pain in patients on ventilation. In contrast, less than 40% of participants used a scale to assess symptoms other than pain. There were two major barriers to the practice of routine assessment of discomfort symptoms in patients undergoing mechanical ventilation. First, there was no discomfort symptom assessment culture at their institution. Second, there was a lack of knowledge regarding rating scales for assessing discomfort symptoms.
This is the first study to survey the attitudes toward symptoms in ventilated patients. Most nurses believed that it was important to objectively assess the six evaluated discomfort symptoms in ventilated patients. Due to the lack of prior research, it is difficult to compare nurses’ attitudes toward these symptoms with previous research. Regarding pain assessment, previous studies have reported that nurses perceived the importance of pain assessment and documentation for patients regardless of the ability of the patient to self-report (Rose et al., 2011). In guidelines for symptom management in critically ill patients, pain, agitation/sedation, delirium, immobility, and sleep (PADIS) were highlighted (Devlin et al., 2018). Nurses appear to be highly concerned about these symptoms in their patients, and this is corroborated by the results of this study.
Despite the perceived importance of assessing discomfort symptoms, nurses do not routinely assess discomfort symptoms using scales except for pain. The pain, agitation, and delirium guidelines were published in 2013 (Devlin et al., 2018). For symptoms not discussed in the guidelines, such as dry mouth, anxiety, fatigue, and dyspnea, results are lacking. Therefore, it is not possible to compare the results of our study with those of previous studies despite suggestions by some researchers of the need to assess these symptoms (Chanques et al., 2015).
The main barriers to assessing discomfort symptoms using the scales were the lack of the culture in their departments to assess discomfort symptoms and a lack of awareness of the specific assessment scales. While a high workload was the main barrier identified in a previous study (Kizza & Muliira, 2015), the results of this study were different. According to a previous study, the median number of nurses per bed in Japanese ICUs was 3.25, compared with 4.7 ± 1.2 in New Zealand and 4.2 ± 1.4 in Australia (Rose et al., 2008). Compared to other countries, the ratio of patients to nurses in Japan is not high (Unoki et al., 2021). Despite an insufficient workforce, a large workload was not reported by participants as a major barrier in this study. The lack of a culture of assessing discomfort symptoms in their departments and lack of awareness about assessment scales were the main barriers. The Respiratory Distress Observation Scale (Sakuramoto et al., 2021) for assessing dyspnea and the Richards–Campbell Sleep Questionnaire (Murata et al., 2019) for assessing sleep have only recently been translated to Japanese. Therefore, Japanese nurses who rarely speak English may not have had the opportunity to learn about the validated rating scales. These barriers may be ameliorated by the development of standard protocols and guidelines for symptom relief that are broader than the current guidelines (Devlin et al., 2018).
Strengths and Limitations
To the best of our knowledge, this is the first study to describe nurses’ attitudes and practices regarding the importance of using a scale to assess the major discomfort symptoms in mechanically ventilated patients. First, as our survey was conducted via mail lists and social networking sites, a selection bias may exist. However, the respondents were nurses working in settings with a wide range of ICU characteristics; they had different numbers of ICU beds and years of experience, worked in different types of hospitals (university vs. non-university), and in different geographic regions. Second, nurses are required to choose the method of assessing discomfort symptoms depending on the patient's level of consciousness, sedation status, and ability to self-report. However, this study did not consider this. Third, although the number of nurses may have affected the assessment of discomfort symptoms, our study did not examine nurse-to-patient ratios in the ICU. However, in this study, we included nurses working in ICUs with nurse-to-patient ratios of at least 1:2 at any given time. Additionally, the percentage of respondents who indicated that workload was a barrier to assessment in the results of this study was low. Fourth, because the questionnaire options were not designed to address patient-related barriers, the reasons for not using the rating scale may not have been exhaustively collected. However, considering that the questionnaire options allowed multiple responses, we believe this limitation did not influence our results. Finally, due to the descriptive and exploratory nature of this study, the sample size was not calculated; therefore, the reliability of the results may be limited.
Implications for Practice
Although nurses perceived the importance of assessing discomfort symptoms using the scale, this study suggested that the percentage of nurses assessing discomfort symptoms other than pain was low because of a lack of knowledge of the rating scales and a culture of assessing discomfort symptoms. Japanese versions of sleep and dyspnea rating scales with established reliability and validity have recently been developed and introduced (Murata et al., 2019; Sakuramoto et al., 2021). However, awareness of these scales is poor in current Japanese clinical practice. Clinicians should be educated about the existence of validated rating scales that can readily be used to assess discomfort symptoms.
Implications for Further Research
One of the main reasons for the lack of the practice of assessing discomfort symptoms other than pain is a lack of knowledge regarding the existence of scales. This suggests not only the lack of a Japanese version but also the lack of effective scales developed internationally to assess discomfort symptoms. For example, the Hospital Anxiety and Depression Scale (Bjelland et al., 2002) for assessing anxiety and depression is not suitable for use in critically ill patients admitted to the ICU because of difficulties in verbal communication due to unconsciousness and other factors. Therefore, it is necessary to develop a simple ICU version of the scale that guarantees reliability and validity for anxiety, fatigue, and dry mouth, which can be used in mechanically ventilated patients.
Conclusions
In this study, it was found that nurses were highly aware of the importance of using scales to assess the six discomfort symptoms experienced by mechanically ventilated patients. In addition, most nurses routinely used scales to assess pain in ventilated patients. Barriers to the routine assessment of discomfort symptoms in mechanically ventilated patients include a lack of culture for assessing discomfort symptoms and a lack of knowledge about rating scales for assessing discomfort symptoms.
Supplemental Material
sj-docx-1-son-10.1177_23779608241245209 - Supplemental material for Nurses’ Attitudes, Practices, and Barriers to Assessing Symptoms of Discomfort in Mechanically Ventilated Patients: A Cross-Sectional Study
Supplemental material, sj-docx-1-son-10.1177_23779608241245209 for Nurses’ Attitudes, Practices, and Barriers to Assessing Symptoms of Discomfort in Mechanically Ventilated Patients: A Cross-Sectional Study by Tomohiko Takahashi, Yusuke Oyama, Hideaki Sakuramoto, Mitsuhiro Tamoto, Tomoo Sato, Yuko Nanjo, Sayaka Hosoi and Takeshi Unoki in SAGE Open Nursing
Footnotes
Acknowledgment
We sincerely thank all the participants in this study.
Authors’ Contributions
TT, YO, and HS contributed to the study's design, statistical analysis, interpretation of the results, and writing the manuscript. MT contributed to the statistical analysis and design of the study and critically reviewed the manuscript. TS, YN, and SH contributed to the design of the study and interpretation of the result and critically reviewed the manuscript. TU was the supervising author and contributed to the interpretation of the results and the critical review of the manuscript. All authors finally approved the final version of the manuscript.
Data Availability
Due to the nature of this research, the study participants did not agree that their data should be shared publicly; therefore, supporting data are not available.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval (Approval # E17) was obtained from the Research Ethics Committee of the Faculty of Nursing and Medical Care at Keio University on May 16, 2022.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Japan Society for the Promotion of Science, Tokyo, Japan (JSPS KAKENHI Grant Number JP 22K10909).
Patient Consent
Informed consent was obtained from all study participants.
Permission to Reproduce Material from Other Sources
Nothing is reproduced from other sources.
Trial Registration
This was an observational study and was not registered as a clinical trial.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.