
Abstract
Introduction
Although registered nurses are expected to treat patients with care and compassion, a variety of characteristics may influence their ability to express compassion.
Objectives
(1) To assess registered nurses’ level of compassion competence and compassion satisfaction, and; (2) to explore how individual-level, employment-related, and organization-level characteristics are associated with their level of compassion competence and compassion satisfaction.
Methods
Registered nurses working in any practice setting in Ontario, Canada, completed a cross-sectional electronic survey of valid and reliable measures. Descriptive statistics and multiple linear regression analyses were used to address study objectives.
Results
One hundred eighty-one registered nurses participated. Most identified as female (n = 157; 96.3%), Caucasian (n = 144; 88.3%), and completed baccalaureate training as their highest level of education (n = 80; 50.6%). Participants’ average compassion competence score was higher than average (4.18 on a 5-point scale), and most participants (n = 171, 98.3%) reported moderate to high levels of compassion satisfaction. Compassion satisfaction was the only significant predictor of compassion competence, which indicated a positive relationship (β = 0.344, p < .001). Compassion competence was among a variety of significantly positive predictors of compassion satisfaction (β = 0.652, p < .001). The other positive significant predictors of compassion satisfaction were higher than baccalaureate education (β = 0.363, p < .001), full-time work status (β = 0.253, p = .012), working in organizations with greater compassion practices (β = 0.114, p = .005), and organizations with higher climate for change (β = 0.292, p < .001).
Conclusions
Study findings illuminate varying degrees of significance for individual-level, employment-related, and organization-level characteristics and how these predict registered nurses’ levels of compassion. These distinctions have important implications for intervention development and future research in understanding compassionate care among nurses.
Introduction
Compassion is a professional value of ethical nursing practice (International Council of Nurses, 2021). Although varying definitions of compassion exist, one definition derived among health care providers, over half of whom were nurses, is: “a virtuous and intentional response to know a person to discern their needs and ameliorate their suffering through relational understanding and action” (Sinclair et al., 2018). This definition illuminates an expectation for individuals to engage with another, such as the engagement that occurs between nurse and patient or client. The positive impacts of compassionate care experiences for nurses and patients have been documented (Durkin et al., 2021; Moss et al., 2019; Sinclair et al., 2018); however, the provision of such care occurs within a broader context that can influence nurses’ behaviors and actions. For example, increased patient care loads and engaging in more procedural duties left nurses feeling as though they had less capacity for compassion (Ghafourifard et al., 2022). Such contextual considerations are described by Cometto et al.’ (2022) in their Compassionate and Respectful Care Framework. The authors claim that compassionate and respectful care by healthcare providers is enabled and reinforced by three concentric layers. The first involves the individual healthcare provider, whose motivation is determined by their environment that should foster the healthcare provider's fulfillment in their work (i.e., competency training and/or compassionate care incentives) (Cometto et al., 2022). These environments are directly influenced by a second layer, broader workforce policies and management, which dictate criteria for manageable workloads or improvements in the clinical care provided by healthcare providers. These workplace policies and management are influenced by the third and final concentric layer, system-wide service delivery and organization, which include regulation mechanisms and curricular and licensing requirements of healthcare providers (Cometto et al., 2022). Although Cometto et al.'s (2022) Framework refers to healthcare providers overall, individual, and organizational factors are specifically identified in the Compassionate Nursing Care Model (Ghafourifard et al., 2022) as important contributors to the compassionate care provided by nurses. In the Model, individual factors include nurses’ religiosity or personality traits (i.e., altruism) while organizational factors include heavy workloads, ineffective management, and lack of compassionate care strategies (Ghafourifard et al., 2022). The individual and organizational factors of the Compassionate Nursing Care Model (Ghafourifard et al., 2022) align with the first and second concentric layers of the Compassionate and Respectful Care Framework (individual health workers; broader workforce policy and management (Cometto et al., 2022)). This alignment illuminates the importance of these two factors/layers to the compassionate care provided by nurses. In what follows, the research literature is reviewed to determine what is known about nurses and compassion in regard to these two factors/layers.
Review of Literature
The level of compassion that nurses think they provide, referred to as compassion competence (Lee & Seomun, 2016a), was found to vary by characteristics of individual nurses as well as characteristics of their employment. The individual characteristics explored include age (Lee & Seomun, 2016c; Park & Park, 2021), marital status (Lee & Seomun, 2016c; Park & Park, 2021), level of education (Lee & Seomun, 2016c; Park & Park, 2021), and degree of spirituality (Lee & Yeom, 2022), all of which were positively associated with compassion competence. However, the relationships between nurses’ compassion competence and characteristics of their employment are more varied: years of clinical experience (Lee & Seomun, 2016c; Park & Park, 2021) were positively associated with compassion competence, whereas workplace incivility (Woo & Kim, 2020) and missed nursing care (Kim & Lee, 2020) were negatively associated. Although both individual and employment-related characteristics are outlined as important factors (Ghafourifard et al., 2022) or layers (Cometto et al., 2022) for compassionate care, the literature relating compassion competence with nurse's employment-related characteristics has focussed solely on interpersonal characteristics (e.g., incivility and nursing care). Such characteristics align with the organizational factors outlined in the Compassionate Nursing Care Model (Ghafourifard et al., 2022) but leave the impacts of organization-level characteristics (i.e., workforce policy and management) in the Compassionate and Respectful Care Framework (Cometto et al., 2022) unexplored.
Nurses’ level of compassion competence is positively associated with their level of compassion satisfaction (Kim & Lee, 2020; Lee & Seomun, 2016c), which is the satisfaction or pleasure that one feels from being able to do good work on the job (Stamm, 2010). Like compassion competence, compassion satisfaction has been explored in relation to nurses’ individual and employment-related characteristics: Three meta-analyses are useful to illuminate these relationships (Xie et al., 2021; Zhang, Han et al., 2018; Zhang, Zhang et al., 2018). Although no significant associations were found between compassion satisfaction and nurses’ individual characteristics (e.g., age, marital status, and religion; Zhang, Zhang et al., 2018), and nurses’ levels of compassion satisfaction varied by continent (Xie et al., 2021). This variation suggests that there may be a matter of cultural or geographical importance to explore. Employment-related characteristics (e.g., years of clinical experience, job satisfaction) were also insignificant with compassion satisfaction (Zhang, Zhang et al., 2018). However, the prevalence of nurses’ compassion satisfaction was found to be 48% (Zhang, Han et al., 2018), that is, nearly 1 in 2 nurses are not satisfied with their ability to do good work at work. The practice settings wherein nurses work may be the reason for this prevalence since levels of compassion satisfaction have been found to vary by practice setting. For example, those working in Intensive Care Units had the highest levels of compassion satisfaction while those working in Psychiatry units had the lowest (Xie et al., 2021). These findings illuminate the importance of individual and employment-related characteristics as important to compassionate nursing care (Ghafourifard et al., 2022) and the provision of quality, compassionate, and respectful care (Cometto et al., 2022). However, as seen with compassion competence literature described above, organizational-level characteristics (i.e., workforce policy and management (Cometto et al., 2022)) remain unexplored in relation to compassion satisfaction.
Problem Statement and Objectives
As indicated in the preceding paragraphs, nurses’ individual and employment-related characteristics are important and have been variably explored in relation to compassion competence and compassion satisfaction, and organizational-level characteristics (i.e., compassionate care strategies (Ghafourifard et al., 2022) or compassionate care incentives (Cometto et al., 2022)) have been explored to a lesser extent. According to the Compassionate and Respectful Care Framework (Cometto et al., 2022), management and operating environments of organizations are important to enable and enhance compassionate and respectful care. Examples include, but are not limited to, organizational and structural shifts to incorporate compassion into care, and interventions to promote compassionate and respectful care: These organizational-level features have largely been overlooked in the research about nurses and compassion. Furthermore, the prevalence of nurses’ compassion satisfaction (Zhang, Han et al., 2018) and the varying levels of nurses’ compassion satisfaction by practice setting (Xie et al., 2021) suggest that changes in some workplaces may be necessary to promote conversations about and expression of compassionate care. Given that it is incomplete to explore employees’ behavior (e.g., levels of compassion) in the absence of factors wherein they work (Guo & Zhu, 2022), the relationships between organization-level characteristics and nurses’ levels of compassion competence and compassion satisfaction were examined.
It is noteworthy to acknowledge that most of the research about nurses and compassion has occurred outside of North America. For example, when considering the three formerly cited systematic reviews (Xie et al., 2021; Zhang, Han et al., 2018; Zhang, Zhang et al., 2018), 25 (26%) of the 96 distinct studies were conducted within North America, two of which were conducted in Canada. In considering the geographical dispersion of research conducted to understand compassion among nurses, an additional goal for the current manuscript is to add to the literature by exploring compassion competence and compassion satisfaction among a sample of Canadian nurses. Considering the information presented above, the objectives of this study were:
To assess nurses’ level of compassion competence and compassion satisfaction. To explore individual, employment-related, and organization-level characteristics and how these characteristics are associated with nurses’ level of compassion competence and compassion satisfaction.
Methods and Procedures
Study Design and Setting
A cross-sectional electronic survey design was used. A convenience sample of Registered Nurses (RNs) was eligible to participate if they were currently practicing within Ontario, Canada, and were able to read and understand English. Ontario is one of Canada's 13 provinces or territories and located in east-central Canada with a land area of 892,411.76 square kilometres (Statistics Canada, 2022). At the time of this study, there were 14,223,942 people living in Ontario, most of whom (n = 65.6%) were of working age (15–64 years) with nearly equal percentages of men and women (66.2% and 65%, respectively). Although English, Irish, and Scottish ancestry 1 were the most frequently reported ethnic or cultural origin (totaling 6,284,690 [44.2%]), 4,817,360 (34.3%) of people living in Ontario were from a visible minority group 2 (Statistics Canada, 2022). At the time of this study, the vast majority of Ontarians (90%; n = 1,424,102) lived within a metropolitan area, which was higher than the national rate (83.9%), while 10% of Ontarians lived outside of a metropolitan area (Statistics Canada, 2022).
In Ontario, nursing practice is regulated through licensure from the College of Nurses of Ontario that maintains annual statistics about membership (College of Nurses of Ontario, 2024). At the time of this study, there were 108,976 RNs in Ontario (College of Nurses of Ontario, 2025), most of whom were between 18 and 64 years of age (n = 103,400, 95%) and completed their entry-to-practice nursing education within Ontario (n = 90,492, 87.4%). 3 A large percentage of RNs worked full time (n = 68,578, 69%), most commonly in an acute hospital setting (n = 65,170, 55.5%).3 Information about the gender, ethnicity, years in practice, or highest level of education for Ontario RNs were not publicly available.
Potential participants self-determined their eligibility based upon details provided in a Letter of Information sent by the research team. Initially, a snowball recruitment strategy was used whereby the Letter of Information was emailed and/or tweeted to persons within the research teams’ networks. The Letter of Information was also posted on the Queen's University research webpage and shared via newsletters and Facebook groups of associations wherein Ontario RNs are members. The Letter of Information was deployed on four biweekly intervals. Queen's University Health Sciences Research Ethics Board approved all study processes prior to recruitment and data collection (# 6032541).
Data Collection
The Letter of Information contained a hyperlink to an electronic survey (via the Qualtrics platform, Xm, 2022) to assess the variables described below. Data were collected anonymously; however, participants were able to indicate their email address if they wanted to be included in a draw for an honorarium. Email information was not linked with study data. The survey was available to be completed between July and December 2021.
Variables
The electronic survey was comprised of a demographic form created for this study, as well as existing scales that are publicly available (details below). In total, participants completed 54 items in the electronic survey.
Compassion competence: The 17-item Compassion Competence Scale (Lee & Seomun, 2016b) measures the level of compassion providers think they provide. It is comprised of three factors (communication, sensitivity, and insight 4 ) to which respondents indicate their degree of agreement to each item on a 5-point Likert-type scale (1 = Strongly Disagree, 5 = Strongly Agree). The mean scores of the items for both the subscales and overall scores were calculated. The validity and reliability for the total scale have been established (Lee & Seomun, 2016b); in the current study Cronbach's alpha was 0.90.
Compassion satisfaction: The Compassion Satisfaction subscale is one within the Professional Quality of Life Scale (Stamm, 2010) that is comprised of 10 5-point Likert-scale items (1 = Strongly Disagree, 5 = Strongly Agree). The mean scores of the items for both the subscales and overall scores were calculated. The overall score was calculated as the average of 10 items and categorized as low (≤2.2), moderate (2.3–4.1), or high (≥4.2) levels of compassion satisfaction (Stamm, 2010). Higher scores reflect greater satisfaction or pleasure from being able to do good work on the job (Stamm, 2010). The validity and reliability of the Compassion Satisfaction subscale have been determined (Stamm, 2010), and in the current study, the Cronbach's alpha was 0.92.
Individual-level characteristics: Seven items on the demographic form were used to collect individual-level characteristics: age, gender, ethnicity, location of nursing education (in Ontario, in Canada [but outside Ontario], or International), highest level of nursing education, year highest education conferred, and first three characters of postal code. Canada Post’s postal code system uses the first three characters to identify geographical districts (i.e., location in Ontario) and urban and rural settings (Canada Post Corporation, n.d.).
Employment-related characteristics: Four items on the demographic form were used to collect employment-related characteristics: employment status (full-time or part-time/casual; permanent or temporary), years in nursing practice, and practice setting.
Organization-level characteristics: Two measures were used to assess organization-level characteristics: (1) The Compassion Practices Scale to assess organizational support for compassionate care, and; (2) the Organizational Climate for Change subscale to assess organizational climate for change. The Compassion Practices Scale (Mcclelland & Vogus, 2014) is useful to evaluate the extent to which a hospital uses award programs to recognize acts of caring shown by employees’ to patients, families, and other employees, and the degree to which the hospital provides support for employees and departments to manage occupational stress. For the purposes of this project, “the hospital” was changed to “your organization” in order to be applicable to the diversity of settings wherein nurses work. The scale comprises five items measured on a 7-point Likert-type scale. An exploratory factor analysis showed all five items loaded onto a single factor with a Cronbach's alpha of 0.82 (Mcclelland & Vogus, 2014), and the current study's reliability coefficient was 0.89.
The 10-item Organizational Climate for Change, a subscale of the Organizational Readiness for Knowledge Translation (Gagnon et al., 2018), assesses an organization's dynamics that support trust and cooperation between staff in four subdimensions: staff cohesion, work-related stress, communication about change, and manager's openness to change (Grandes et al., 2017). The 10 items are summed for an overall score and then transformed on a 100 scale (personal communication with M. Pierre-Gagnon on June 2, 2022). Scores ≤50 are deemed as low, scores 51–79 are deemed as medium, and ≥80 are high (personal communication with M. Pierre-Gagnon on June 2, 2022). In the current study, the average of the 10 5-point scale items was used as the overall score, where scores ≤2.5 were deemed as low, scores 2.6–3.9 as medium, and ≥4 as high. The validity (Gagnon et al., 2018) and factor structure of the measure and subscales are supported (Grandes et al., 2017). In the current study, the Cronbach's alpha was 0.75.
Data Analysis and Sample Size
R version 4.2.1 (R Foundation, n.d.) was used to conduct study analyses. Descriptive analyses were used to address Objective 1. Thereafter, to address Objective 2, two separate multiple linear regression analyses were conducted to investigate these relationships. Given the current understanding of compassion (see “Introduction” section), the following independent variables were used in both regression models: individual characteristics included ethnicity, rural or urban, and level of education; employment-related characteristics included employment status, years in nursing practice and practice setting, 5 and; organizational-level characteristics included the organizational support for compassionate care and organizational climate for change variables. Given the positive association between compassion competence and compassion satisfaction (Kim & Lee, 2020; Lee & Seomun, 2016c), these variables were included in each other’s model (e.g., compassion satisfaction was included in the compassion competence model and vice versa). The remaining variables were used to describe the overall sample characteristics. The pattern and extent of missing data were assessed prior to analysis. Observations with missing values were excluded under the assumption of missing completely at random. Missingness patterns were summarized to support this approach.
At a significance level of 0.05, with a power of 0.8 and an effect size of Cohen's f² = 0.15 (medium effect) (Cohen, 1988), the required sample size for the intended multiple linear regression models (see below), calculated using G*Power (Faul et al., 2009), was 135. Additionally, Harrell (2001) suggests that a linear regression model is generally reliable when the number of predictors is less than n/10, where n is the sample size. These conditions were satisfied for the current analyses.
Results
A total of 181 RNs across Ontario participated in the survey. Most identified as female (n = 157, 96.3%), from European or white descent (n = 144, 88.3%), and were, on average, 42 years of age (range 23–77 years). Participants predominantly lived in urban settings (n = 133, 87.5%) located in Eastern (n = 54, 35.5%) and Central (n = 34, 22.4%) Ontario. Most participants were employed in one workplace (n = 118, 72.0%) as permanent full-time employees (n = 107, 65.6%). The most common practice settings wherein participants worked were acute (n = 59, 36.0%) or critical care (n = 55, 33.5%). Full sample details can be found in Table 1. Details on the extent and pattern of missing data are reported below Tables 1 to 3.
Individual-Level and Employment-Related Characteristics of Participants (N = 163).
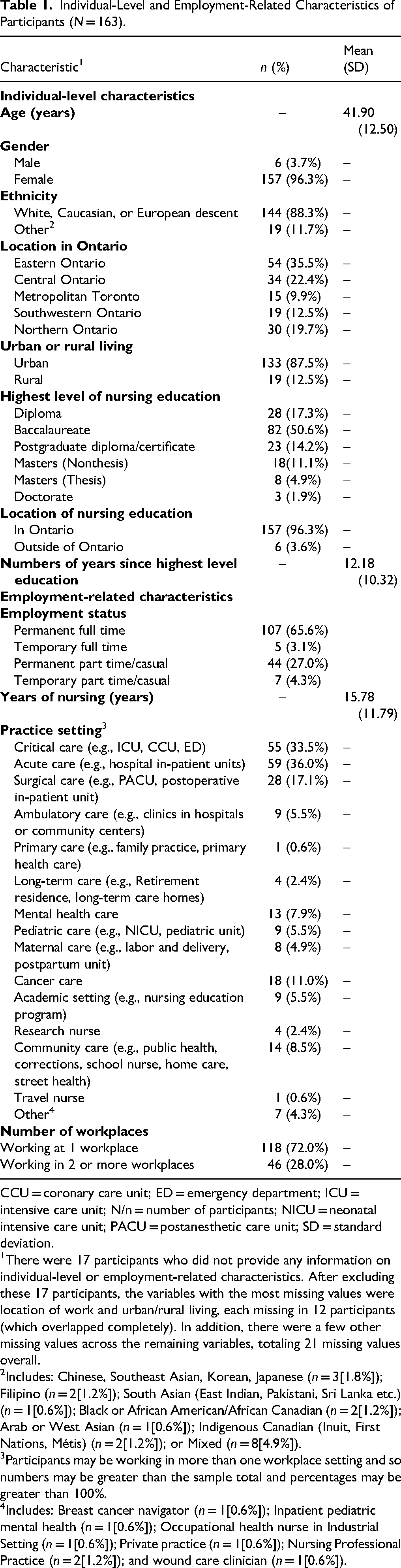
CCU = coronary care unit; ED = emergency department; ICU = intensive care unit; N/n = number of participants; NICU = neonatal intensive care unit; PACU = postanesthetic care unit; SD = standard deviation.
There were 17 participants who did not provide any information on individual-level or employment-related characteristics. After excluding these 17 participants, the variables with the most missing values were location of work and urban/rural living, each missing in 12 participants (which overlapped completely). In addition, there were a few other missing values across the remaining variables, totaling 21 missing values overall.
Includes: Chinese, Southeast Asian, Korean, Japanese (n = 3[1.8%]); Filipino (n = 2[1.2%]); South Asian (East Indian, Pakistani, Sri Lanka etc.) (n = 1[0.6%]); Black or African American/African Canadian (n = 2[1.2%]); Arab or West Asian (n = 1[0.6%]); Indigenous Canadian (Inuit, First Nations, Métis) (n = 2[1.2%]); or Mixed (n = 8[4.9%]).
Participants may be working in more than one workplace setting and so numbers may be greater than the sample total and percentages may be greater than 100%.
Includes: Breast cancer navigator (n = 1[0.6%]); Inpatient pediatric mental health (n = 1[0.6%]); Occupational health nurse in Industrial Setting (n = 1[0.6%]); Private practice (n = 1[0.6%]); Nursing Professional Practice (n = 2[1.2%]); and wound care clinician (n = 1[0.6%]).
Descriptive Results for the Measures.

N/n = number of participants; SD = standard deviation.
For this 17-item scale, 5 participants were missing 1 item and 1 participant was missing 2 items.
For this 10-item scale, 7 participants did not respond to any items, 2 participants missed 1 item, and 1 participant missed 2 items.
For this 5-item scale, 117 participants had no missing items. Among the remaining participants, most were missing 1–3 items, with 17 missing all the 5 items.
For this 10-item scale, 3 participants were missing 1, 2, or 6 items, and 18 were missing all 10 items.
For each measure, the scale total score for each participant was computed as the mean of their available item responses. Participants who did not respond to any items were excluded, as no scale total score could be computed.
Predictors of Compassion Competence and Compassion Satisfaction.

R2 = 0.32, F(13, 134) = 4.87, p < .001; R2 = 0.50, F(13, 134) = 10.48, p < .001.
For categorical variables, results are shown for the nonreference levels. 1For White, Caucasian, or European descent; the reference is all other ethnicities. 2For Urban living; the reference is rural living. 3For higher than baccalaureate education, the reference is baccalaureate or lower. 4For permanent work status; the reference is temporary positions. 5For full-time work status, the reference is part-time employment. 6Other includes those working in settings other than critical, acute, and surgical care. Note: Since RNs can work in multiple settings, practice setting indicators are not mutually exclusive. Each variable indicates whether the RN works in that setting (1 = yes, 0 = no).
In the regression analysis, only complete observations were used (n = 148). As noted in Table 1, 17 participants did not provide any information on their characteristics. We compared compassion competence and compassion satisfaction scores between participants who provided at least some characteristic information and those who provided none. Based on formal two-sample t-tests and visual inspection via histograms, we did not find any systematic differences between the two groups (compassion competence: mean difference = 0.2, 95% CI [−0.44, 0.84]; compassion satisfaction: mean difference = −0.12, 95% CI [−0.48, 0.23]).
After excluding these 17 cases, 16 participants had partial missingness in the covariates. Among them, 10 were missing only the urban/rural variable. To assess the sensitivity of excluding these cases, we reran the analysis by coding an additional “missing” category for the urban/rural variable. The results were essentially unchanged. For the remaining six cases, which involved a total of nine missing values, we conducted a sensitivity check by imputing missing values using the median for categorical variables and the mean for continuous variables. The regression results remained consistent. These six cases represent a small proportion relative to the complete sample.
Objective 1 Results
The descriptive results for the measures are presented in Table 2, and the distributions of the Compassion Competence and Compassion Satisfaction scores are shown in Figures 1 and 2, respectively. The average of the overall Compassion Competence scores of participants was 4.18 (SD ± 0.46) on a 5-point scale indicating that these providers believe they provide a higher-than-average level of compassion. In the Compassion Satisfaction Scale scores, most participants (n = 129, 74.14%) indicated a moderate level of compassion satisfaction and one quarter of the sample (n = 42, 24.14%) had high levels of compassion satisfaction, indicating a greater level of satisfaction related to their ability to do good work on the job.

Distribution of Compassion Competence Scores.
Distribution of Compassion Satisfaction Scores.
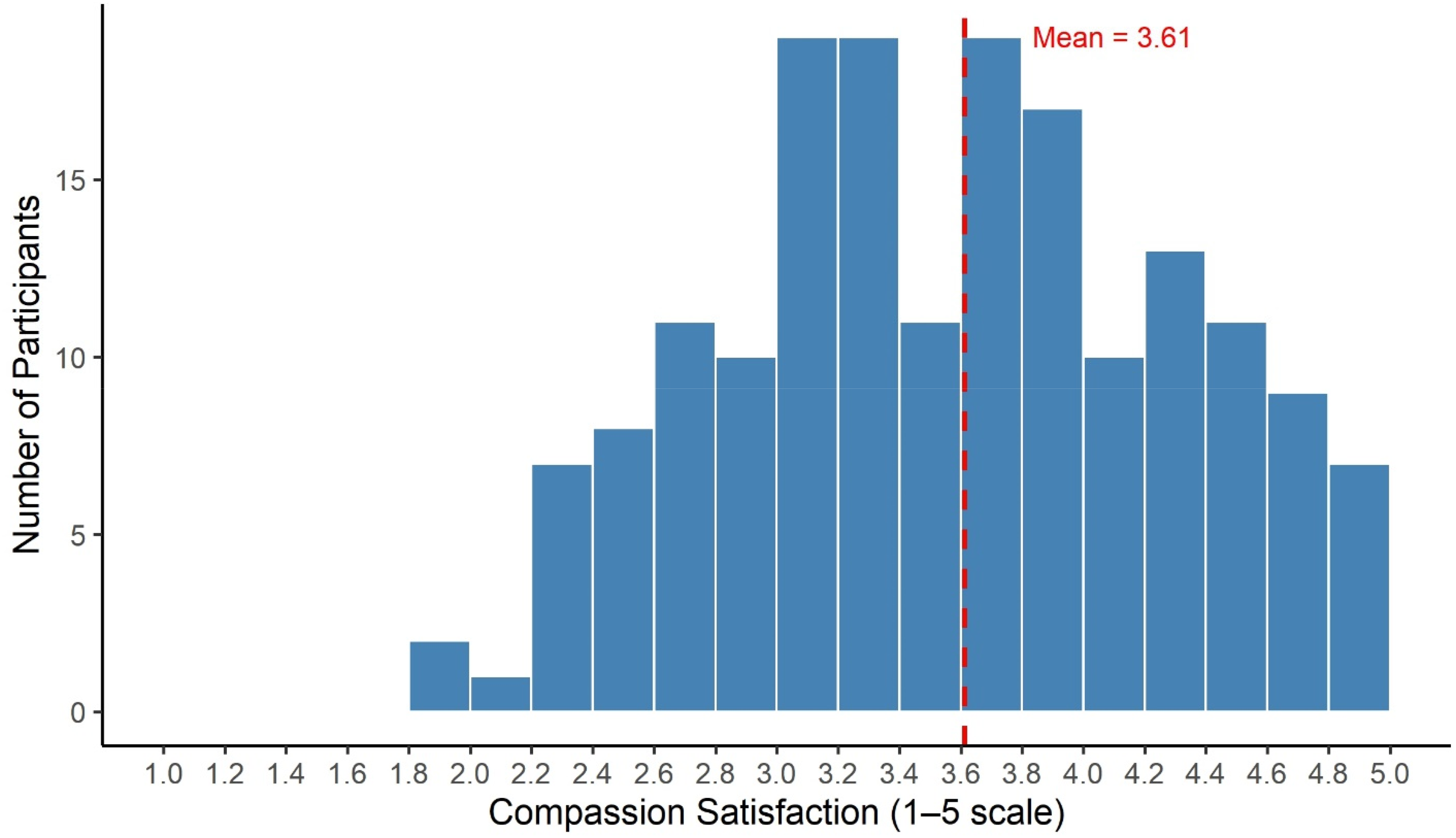
Notably, the average of the overall Compassion Practices Scale score was 3.61 (SD ± 0.72) on a 5-point scale suggesting that participants’ places of work placed some acknowledgment toward acts of caring. Nevertheless, the scores for most participants’ (n = 130, 79.75%) scores on the Organizational Climate for Change measure were between 2.6 and 3.9 indicating a medium level of trust and cooperation among staff in their organization.
Objective 2 Results
Multiple linear regression analyses revealed one statistically significant predictor of compassion competence: compassion satisfaction (β = 0.344, p < .001). None of the individual-level, employment-related, or organizational-level characteristics were statistically significant. Full regression results about compassion competence are displayed in Table 3.
Results of another multiple linear regression revealed five statistically significant predictors of compassion satisfaction. Participants who had higher levels of compassion competence (β = 0.652, p < .001), higher than baccalaureate education (β = 0.363, p < .001), and full-time work status (β = 0.253, p = .012) had higher compassion satisfaction. Furthermore, those who worked in organizations with greater compassion practices (β = 0.114, p = .005) and a higher climate for change (β = 0.292, p = .001) tended to have higher levels of compassion satisfaction. None of the other individual-level, employment-related, or organizational-level characteristics were statistically significant. Full regression results about compassion satisfaction are displayed in Table 3.
Discussion
In this study, the research team examined nurses’ level of compassion competence and satisfaction and how these may be influenced by their individual-level, employment-related, and organization-level characteristics. This sample of RNs believed that they provided a higher-than-average level of compassion (compassion competence) and most felt higher levels of satisfaction related to their ability to do good work on the job (compassion satisfaction). Results also illuminated the various individual-level, employment-related, and organization-level characteristics that were associated with these compassion concepts which were informed by the conceptualizations of compassion used to inform this study (Cometto et al., 2022; Ghafourifard et al., 2022). In the following paragraphs, study results are compared to those within the literature.
When comparing this study's compassion competence results to others, it was found that the level of compassion competence revealed in the current sample was amid those reported in the literature. Notably, these collective results have been determined across a range of practice settings. For instance, the current sample included nurses working in a variety of practice settings within and beyond hospital environments, whereas the available literature has only included samples working within hospitals (Kim & Lee, 2020; Lee & Yeom, 2022; Lee & Seomun, 2016c; Park & Park, 2021; Woo & Kim, 2020). In this way, the current results extend what is known about nurses’ level of compassion competence, or the level of compassion that nurses think they provide, in regard to a broader range of practice settings. However, despite these consistent levels of compassion competence, the current results contradict the documented associations between individual-level, employment-related, organizational-level, and compassion competence (Kim & Lee, 2020; Lee & Yeom, 2022; Lee & Seomun, 2016c; Park & Park, 2021; Woo & Kim, 2020). In reviewing the literature to plan the current study (see Introduction), a range of results were reported for individual-level and employment-related characteristics and no known literature had examined organizational-level characteristics. In this way, the current study's results provide the first known examination between organizational-level characteristics and compassion competence and add to what is known about its associations with individual-level and employment-related characteristics. This study's results indicate that conceptual factors (Ghafourifard et al., 2022) or layers (Cometto et al., 2022) may not be as important as previously thought for the compassion that nurses think they provide (compassion competence). However, a possible reason for these inconsistent results may be the global location wherein they were ascertained: The former results were determined in South Korea, whereas current results were determined in Canada. This inconsistency may suggest that there are cultural variations in regard to what influences nurses’ compassion competence. Although the current study's sample included nurses who identified with a variety of ethnic backgrounds (see Table 1), the sample was largely Caucasian, and ethnicity did not predict compassion competence. Nevertheless, the variability across study results may indicate that there are important cultural interpretations in regard to nurses’ compassion competence suggesting a need for further research to explore these associations.
The finding that most nurses reported moderate to high levels of compassion satisfaction is consistent with results from nurses working in emergency departments (O'callaghan et al., 2020; Ruiz-Fernandez et al., 2021) and intensive care areas (Jakimowicz et al., 2018). However, as with compassion competence (discussed above), the current study's results extend what is known about nurses’ level of compassion satisfaction, or their level of satisfaction related to their ability to do good work on the job, to beyond hospital settings. Based upon the geographical location of the sample (Canada), the current study's results also align with meta-analytic results (Xie et al., 2021), which have identified nurses working in the Americas as having higher levels of compassion satisfaction than those in other continents.
It is noteworthy that compassion satisfaction was significantly associated with each of the conceptual factors (Ghafourifard et al., 2022) or layers (Cometto et al., 2022) used to inform the current study; however, not all variables used to assess these factors or layers were significant in this study's results. The only individual-level characteristic associated with compassion satisfaction was level of education, meaning that nurses who completed higher than baccalaureate education had higher levels of compassion satisfaction. This finding corroborates with that of Jakimowicz et al. (2018) who found that nurses with postgraduate qualifications had statistically significantly higher compassion satisfaction scores than those without such qualifications (Jakimowicz et al., 2018). The insignificance found in the current study between other individual-level characteristics and compassion satisfaction is largely consistent with that presented in a systematic review (Zhang, Zhang et al., 2018). However, contrary to the available literature, one employment-related variable (full-time work status) was associated with compassion satisfaction in the current study where comparable employment-related variables have only been insignificant (Zhang, Zhang et al., 2018). Nurses with permanent roles working in a variety of settings and organizations have been found to have higher levels of job satisfaction, organizational commitment, and empowerment than nurses working in temporary roles (Han et al., 2009). This understanding of employment status indicates the positive impact of having permanent work for nurses. It is possible that nurses may feel more established and comfortable in their work environment when in a full-time position allowing them to focus on incorporating compassion into their practice.
Both organization-level variables assessed in the current study were significantly associated with compassion satisfaction, indicating the importance of organizational-level characteristics for nurses’ satisfaction with their ability to do good work. In the current study, compassion satisfaction was higher among participants who worked in organizations that recognized acts of caring among employees (assessed as Compassion Practices). Similar results have been found among intensive care nurses working in environments that acknowledged and prioritized compassionate practices: These environments were found to facilitate nurses’ efficiency to deliver compassionate care (Naseri et al., 2022). Specific to compassion satisfaction, higher levels have been observed among nurses working in locations where there was financial and social recognition at work (Higashibata et al., 2023). Also found in the current study was that compassion satisfaction was higher among participants who worked in organizations that had higher climates for change (e.g., staff cohesion, lower work-related stress). The current sample's organizational climate for change scores indicated a medium level of trust and cooperation among staff members within their organizations. The importance of a positive organizational culture—characterized by teamwork, open communication, respect, and support (Körner et al., 2015)—has been found to foster a sense of belonging and job satisfaction among healthcare professionals (Körner et al., 2015). Specific to nurses, such supportive environments facilitate their ability to provide compassionate care (Horsburgh & Ross, 2013). Higher levels of compassion satisfaction have been found among nurses who have greater supervisor and coworker support (Maillet & Read, 2021) and quality social interactions at work (Higashibata et al., 2023). Nurses with higher compassion satisfaction also had greater ability to make decisions at work (Higashibata et al., 2023) and reported fewer psychological demands (Maillet & Read, 2021) and amount of work to be completed (Higashibata et al., 2023). These collective findings indicate the importance of building trust, cooperation, and sense of community where employees can feel supported at work and seek support from their organization as needed. Undoubtedly, these workplace attributes have long-term implications, particularly given that the practice environment has been found to have a statistically significant and inverse relationship with nurses’ turnover intention and that compassion satisfaction mediated this relationship (Gong et al., 2022). Furthermore, given the need for nursing retention efforts (Pressley & Garside, 2023; Sawatzky et al., 2015) and higher nurse to patient ratios have been inversely associated with Iranian nurses’ level of compassion (Naseri et al., 2022), indicate that organizational characteristics are of utmost importance to address as a nursing retention strategy.
While the discussion above has focussed on comparing results to the factors and layers of compassion identified in the conceptual and research literature, it is important to discuss the associations of compassion variables explored in the current study. Although other authors have reported a significant positive association between compassion competence and compassion satisfaction (Kim & Lee, 2020; Lee & Seomun, 2016c), the current study's findings further the relational understanding between the concepts particularly in regard to their prediction. In the current study and others (Kim & Lee, 2020; Lee & Seomun, 2016c), compassion competence significantly and positively predicted compassion satisfaction. However, the current study is the first known to explore and report that compassion satisfaction positively predicts compassion competence, suggesting a recursive relationship between the concepts that may not have been formerly appreciated. Nevertheless, it is acknowledged that such relationships cannot be determined using cross-sectional data, such as that used in the current study and illuminates a topic for future research.
Strengths and Limitations
Considering the limited number of studies focused on nurses working in North America (Xie et al., 2021), the current study fills a geographic gap in literature by providing valuable insights into Canadian RNs levels of compassion. Secondly, the individual-level, employment-related and organization-level characteristics assessed in the current study were informed by theoretical conceptualizations of compassion (Cometto et al., 2022; Ghafourifard et al., 2022) as well as a review of research about nurses and compassion. Thirdly, the current study included RNs across various practice settings, shedding light on how such settings may influence compassion. These findings permit the development of tailored interventions for improving compassion competence and satisfaction across workplace settings.
Despite the aforementioned strengths of the current study, there are also limitations, the first of which is in regard to the methods used. At the time of the current study, there were 108,976 RNs in Ontario (College of Nurses of Ontario, 2025) and a response rate between 25% and 30% (Menon & Muraleedharan, 2020), or at least 27,244 participants, was anticipated: This was not the case despite using multiple recruitment strategies (snowball emails and posting the survey on a university website) therefore negatively affecting the intended generalizability of study results. It is also possible that individuals with greater interest in this topic, or those who worked in places where active discussions about compassionate care take place may have been more likely to participate. Data collection occurred during the fourth wave of COVID-19 pandemic (Canadian Institute for Health Information (CIHI), 2022) when nurses were experiencing high degrees of pandemic-induced stress and burnout (Moons, 2023) and may be a more plausible reason for the low rate of study participation. These points illuminate the possibility of response bias, one of many limitations in the chosen cross-sectional design (Wang & Cheng, 2020). Among those who did participate in this study, the COVID-19 pandemic may have impacted their responses to survey items (i.e., response bias): however, COVID-19-related matters were not specifically addressed within the survey items.
The second notable limitation of the current study is in regard to the statistical analyses. Although compassion competence and compassion satisfaction are conceptually related, they were modeled separately using two multiple linear regressions. One model treated compassion competence as the outcome and compassion satisfaction as a predictor, and the other reversed this structure. While a joint modeling framework such as path analysis or structural equation modeling would allow for the simultaneous estimation of reciprocal effects and properly account for the endogeneity between the two variables, these authors opted for separate models due to sample size constraints and the number of parameters involved. Although this approach improves estimation stability and interpretability as recommended by Kline (2023, 5th ed.), it is acknowledged that the moderate R2 values of the overall models (R2 = 0.32 for compassion competence and R2 = 0.50 for compassion satisfaction) suggest that other relevant variables may not have been included in the models.
Study Implications
Despite the challenges of measuring compassion, the concept is increasingly identified as a key component of quality care that is important to monitor, evaluate, and improve upon (Sinclair et al., 2017). For example, the finding that compassion satisfaction mediates the relationship between nurses’ practice environments and their turnover intention (Gong et al., 2022) adds to the importance of monitoring and evaluating compassion within settings wherein RNs practice. The current study's results can be used to inform workplace setting–specific initiatives, including policy, to facilitate RNs compassion. Using the variables assessed in the current study, such initiatives could include award programs that recognize acts of caring by employees to their patients and coworkers. Drawing from other literature, such initiatives could also include initiatives to promote greater compassion to one's self, known as self-compassion. These suggestions align with that identified in the literature, wherein self-compassion, support at the workplace, and health and safety at the workplace are identified as important starting points for interventions (Muller et al., 2023). Such interventions need not be limited to the organizations wherein nurses provide clinical care but could be incorporated into nursing curricula. This would permit discussions about compassion among early-career nurses and provide them with opportunities to observe, experience, and practice incorporating compassion into their daily lives and nursing care.
As alluded to throughout this Discussion, there are many questions that remain about compassion among nurses that could be used to inform future research. For example, future research can build upon these results in order to better understand how and what specific attributes of RNs’ work environments support their compassion practices. This understanding could be useful to promote the highest quality of patient care. Future investigations with large and diverse samples, conducted over an extended period, could provide a more comprehensive understanding about the relationships among healthcare practice environments, compassion competence, and compassion satisfaction.
Conclusion
The current study reveals insight into the associations between nurses’ characteristics and their level of compassion competence and satisfaction. Most participants believed they provided a higher-than-average level of compassion (compassion competence) and reported moderate to high levels of compassion satisfaction. However, the associations of characteristics that reflected individual-level, employment-related and organizational-levels varied by the concept of compassion examined (compassion competence or compassion satisfaction). These results highlight the importance of varying characteristics on RNs levels of compassion. These distinctions have important implications for intervention development and future research.
Supplemental Material
sj-docx-1-son-10.1177_23779608251367257 - Supplemental material for Registered Nurses’ Characteristics and Their Levels of Compassion Competence and Satisfaction: A Cross-Sectional Survey
Supplemental material, sj-docx-1-son-10.1177_23779608251367257 for Registered Nurses’ Characteristics and Their Levels of Compassion Competence and Satisfaction: A Cross-Sectional Survey by Jacqueline Galica, Stephanie Saunders, Chiamaka Madu, Ziwei Pan, Hok Kan Ling, Jennifer Waite, Denise Neumann-Fuhr and Erna Snelgrove-Clarke in SAGE Open Nursing
Footnotes
Authors’ Note
Ethical Considerations: Queen's University Research Ethics Board approved the study (# 6032541). Consent to Participate: All participants provided implied consent by their completion of the e-survey. Data Availability: The data collected as part of this study is not available due to ethical compliance.
Acknowledgement
This project was financially supported by the Margaret Leith Bruce Faculty Award in Compassionate Care awarded to Jacqueline Galica.
Author Contributions
JG: Conceptualization, methodology, investigation, project administration, writing—original draft, writing—review & editing, and funding acquisition. SS: Investigation, writing—original draft, and writing—review & editing. AM: Writing—original draft and writing—review & editing. ZP: Formal analysis and writing—review & editing. HKL: Formal analysis and writing—review & editing. JW: Conceptualization and writing—review & editing. DNF: Conceptualization and writing—review & editing. ESC: Supervision and writing—review & editing.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was financially supported by the Margaret Leith Bruce Faculty Award in Compassionate Care awarded to Jacqueline Galica (grant number 2021).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.