
Abstract
Introduction
The healthcare sector is well known for being demanding and stressful, leading to high rates of burnout and decreased job satisfaction among healthcare professionals. Self-compassion has been identified as a potential preventive factor against burnout and may improve job satisfaction.
Objective
The current study aimed to assess the level of self-compassion, burnout, and job satisfaction among healthcare professionals; to explore the relationship between self-compassion, burnout and job satisfaction; and to examine the predictors of self-compassion.
Methods
A descriptive correlational design. A convenience sample of 403 healthcare professionals, including doctors and nurses, participated. Data were collected using a printed questionnaire. Correlation analyses and ANOVA were conducted.
Results
The study found moderate levels of self-compassion, burnout, and job satisfaction among healthcare professionals. Self-compassion was moderate, with a mean of 3.10, while burnout was 3.48, Job satisfaction was 2.88. A positive correlation was found between self-compassion and job satisfaction, while a negative correlation was found between burnout and self-compassion. The results show statistically significant differences in self-compassion based on educational attainment and years of experience
Conclusion
The study found a positive correlation between self-compassion and job satisfaction, while a negative one was found with burnout. Education and experience significantly influenced self-compassion, with participants holding a bachelor's degree and those with less experience reporting higher levels.
Introduction
Healthcare professionals face intense job demands—including rising workloads, complex technologies, and organizational pressures—that significantly threaten their well-being. The National Academy of Medicine (2019) report highlights increasing chronic stress, poor mental health, and burnout in healthcare settings. Burnout- defined by emotional exhaustion, depersonalization, and reduced personal accomplishment—compromises both well-being and patient care, undermining healthcare system performance (National Institutes of Health, 2021).
Review of Literature
Self-compassion offers a valuable tool in mitigating stress and promoting mental well-being among healthcare professionals. Defined by Kristin Neff and colleagues as comprising three interconnected elements—self-kindness (being gentle toward oneself in times of suffering), common humanity (recognizing that personal failure and suffering are part of the shared human condition), and mindfulness (holding experiences in balanced awareness without over-identifying)—self-compassion cultivates emotional resilience and reduces self-judgment, isolation, and over-identification (Neff et al., 2020). Professionals with higher self-compassion report lower levels of burnout and stress, alongside higher job satisfaction and emotional well-being (Amin, 2021). Importantly, self-compassion is learnable. Programs like Mindful Self-Compassion (Neff & Germer, 2013) and Compassion-Focused Therapy (Gilbert & Simos, 2022) reliably improve emotional resilience, reduce stress, and enhance well-being.
Despite this promising evidence, most research—particularly in Jordan—has focused on compassion fatigue, burnout, or job satisfaction among specific nursing subgroups (Alqarni et al., 2022; Athamneh, 2024; Hamdan et al., 2023; Nimer et al., 2021). Few studies have explicitly examined self-compassion, let alone compared healthcare roles such as nurses and physicians in general hospital settings. This lack of comparative investigation into self-compassion across professional groups represents a significant gap in the literature, as understanding these differences may inform tailored interventions.
Purpose of the Study
The current study aimed to assess the levels of self-compassion, burnout, and job satisfaction among healthcare professionals; to explore the relationships between self-compassion, burnout, and job satisfaction; and to examine predictors of self-compassion. Conducted in five hospitals in Irbid Governorate —one of Jordanian's most densely populated and diverse regions—this study addresses the identified gap by investigating self-compassion alongside burnout and job satisfaction among different healthcare professional groups. Northern Jordan is characterized by high patient loads, limited resources, and staffing shortages—particularly in public hospitals—making it a pertinent setting for exploring how self-compassion may mitigate occupational stress.
Conceptual Framework
Self-compassion enhances job satisfaction directly and indirectly by mitigating burnout (Alkhraishi et al., 2023), a factor that negatively affects job satisfaction. Burnout acts as a mediator, weakening the direct effect of self-compassion on job satisfaction. Understanding these relationships can help develop strategies to enhance healthcare professionals’ well-being by promoting self-compassion and reducing burnout. The framework's key relationships are as follows: Self-Compassion → Job Satisfaction (+); Self-Compassion → Burnout (−); Burnout → Job Satisfaction (−).
Methods
Study Design and Setting
A cross-sectional, descriptive, correlational study was conducted to identify associations between variables at one point in time. The study took place in five hospitals in northern Jordan, including three governmental (King Abdullah University Hospital (KAUH), Ramtha Hospital, and Prince Basma Hospital) and two private hospitals (Irbid Islamic Hospital, AL Qawasmi Hospital).
Participants
A convenience sampling method was used to recruit physicians and nurses meeting the inclusion criteria. Using G*Power analysis, a minimum sample size of 300 was required to ensure statistical power (0.80) at a significance level of 0.05.
Inclusion criteria: Physicians and nurses who had worked for more than 1 year in the selected hospitals and were directly involved in patient care. While, exclusion criteria: Individuals in managerial or supervisory roles and those with less than 1 year of work experience.
Considering dropout rates and variations in hospital participant numbers, 403 participants were recruited: 100 from KAUH Hospital, 110 from Ramtha Hospital, 100 from Prince Basma Hospital, 70 from Irbid Islamic Hospital, and 23 from AL Qawasmi Hospital. A total of 420 questionnaires were distributed, and 403 were returned, with 17 omitted due to incompleteness, yielding a final response rate of 95%.
Procedure
The printed questionnaires were self-administered in designated hospital settings (e.g., quiet meeting rooms) to minimize distractions and ensure privacy. Samples were collected between November 2024 and January 2025 according to a set schedule, with a research assistant holding a master's degree assigned to assist. The research assistant collected samples from KAUH Hospital and Ramtha Hospital, while the principal researcher collected data from hospitals Prince Basma Hospital, Irbid Islamic Hospital, and AL Qawasmi Hospital.
Questionnaires were administered three times per week on different days, each data collection period lasted two and a half hours, with a target of completing 15–20 questionnaires per data collection period. The study's objective and purpose were explained, and questionnaire items were clarified to the research assistant. Confidentiality of the collected information was emphasized. The questionnaires were kept strictly confidential between the principal researcher and the assistant, with any unclear responses were addressed. Thus, although the questionnaires were self-administered, trained staff were present during distribution and collection to assist with questions and to ensure proper conduct of the process.
The printed questionnaire included sections for informed consent, and demographic details (age, gender, marital status, educational level, hospital name, professional role, area of work, years of experience, and previous training on a self-compassion program), as well as scales for self-compassion, burnout, and job satisfaction. The researcher approached potential participants and explained the study's purpose, the inclusion and exclusion criteria, benefits, and the estimated time required to complete the questionnaire (approximately 10–15 min).
Measurements
The study's self-administered questionnaire comprised four sections: (1) demographic data, (2) Self-Compassion Scale, (3) Burnout Scale, and (4) Job Satisfaction Scale. The demographic data form, developed by the researcher based on the relevant literature, include age, gender, marital status, educational level, hospital name, professional role, area of working, years of experience, previous training in self-compassion programs.
The Self-Compassion Scale-Short-form (SCS-SF) comprises 12 items divided into Self-Disparagement and Self-Care subscales (6 items each). Self-Disparagement reflects self-criticism (impatience, disapproval, judgment), whereas Self-Care captures self-compassion (tenderness, patience, empathy). Scores are summed—after reverse scoring Self-Disparagement—to yield a total self-compassion score, where higher values indicate greater self-compassion. Mean scoring (average scores) is also reported (sum divided by number of items). The SCS-SF demonstrates strong internal consistency (α ≥ 0.86) and near-perfect correlation with the long form (r ≥ 0.97) (Raes et al., 2011).
The Maslach Burnout Inventory-Health Services Survey, developed by Maslach and Jackson (2013) to assess burnout in human services professionals, comprises 22 items across three dimensions: Emotional Exhaustion (9 items), Personal Accomplishment (8 items), and Depersonalization (5). Each item is rated on a seven-point frequency scale (0 = never to 6 = every day), with higher scores indicating greater burnout. The overall scale demonstrated good internal consistency (α = .80).
The Mueller and McClosky Satisfaction Scale, developed by Mueller and McCloskey (1990), includes 31 items across eight subscales: family/work balance (3 items); interaction (4); scheduling (6); extrinsic rewards (3); praise and recognition (4); work control/responsibility (5); professional opportunities (4); and co-workers (2). Items are rated on a five-point Likert scale (1 = very dissatisfied to 5 = very satisfied). The original scale demonstrated strong reliability (α = 0.89).
Ethical Consideration
Approvals were obtained from the Institutional Review Board (IRB) at Jordan University of Science and Technology (JUST) and KAUH Hospital, as well as from the Jordan Ministry of health for governmental hospitals Ramtha Hospital and Prince Basma Hospital. For private hospitals Irbid Islamic Hospital, and AL Qawasmi Hospital, permission was granted by the directors. Participants were asked to sign a consent form before completing a printed questionnaire after the study's purpose and aims had been explained. They were informed that participation was voluntary and that they had the right to withdraw at any time. Anonymity, privacy, and confidentiality were maintained throughout all study phases, with being data de-identified, securely stored, and accessible only to the researcher in locked cabinets.
Statistical Analysis
SPSS® version 25 (SPSS Inc., Chicago, IL) was used for the statistical analysis. Descriptive statistics were conducted to assess the levels of self-compassion, burnout, and job satisfaction among healthcare professionals, with means and standard deviations calculated for each scales. The Pearson correlation coefficient was used to determine relationships between self-compassion, burnout, and job satisfaction. An ANOVA was performed to analyze differences in self-compassion based on gender, age, educational level, marital status, professional role, area of work, years of experience, and previous training in self-compassion programs. The Scheffé test was used for post-hoc comparisons of educational level and years of experience, with a significance level of 0.05 and statistical power of 0.80 or 0.90.
Results
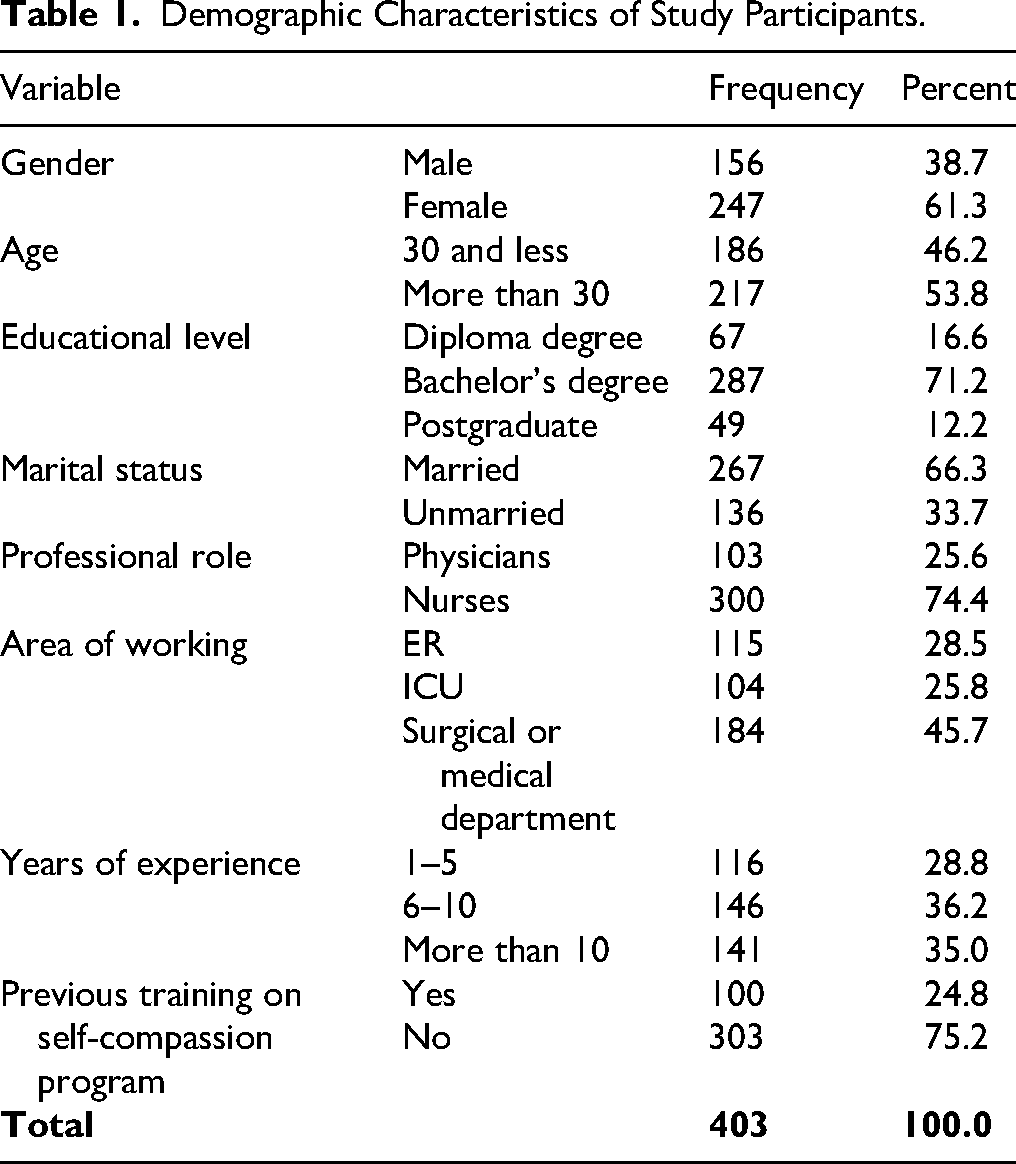
In the current study there were 403 participants, of whom 156 were men (38.7%) and 247 were women (61.3%). Regarding age, there were 186 participants, (46.2%), were under 30 years old, while 217 participants, (53.8%), were over 30 years. A bachelor's degree was the most common among participants 287 participants (71.2%), followed by diploma degree 67 participants (16.6%), and postgraduate degree 49 participants (12.2%). In terms of marital status, 267 individuals, (66.3%), were married, while 136 participants, (33.7%) were single. Regarding to their professional role, 300 individuals (74.4%) were nurse 103 participants (25.6%) were doctors. For the area of working, 184 participants (45.7%) including in surgical or medical departments, 104 participants (25.8%) in the intensive care unit, and in the emergency rooms 115 participants (28.5%).
Regarding years of experience, 116 participants (28.8%) had 1–5 years, 146 participants (36.2%) had 6–10 years, and 141 participants (35%) had more than 10 years. Among the participants, 100 participants (24.8%) had previously participated in a self-compassion program, whereas 303 participants (75.2%) had not. Table 1 shows the demographic characteristics of the study participants.
Demographic Characteristics of Study Participants.
Level of Self-Compassion, Burnout, and Job Satisfaction Among Healthcare Professionals
The levels of self-compassion, burnout, and job satisfaction among healthcare professionals were described using actual mean scores and supported by benchmark cut-offs. The average score for self-compassion was 3.10, with subscale scores ranging from 3.07 to 3.14, which falls into the “moderate” category based on suggested thresholds (1-2.49 = low; 2.5-3.5 = moderate; 3.51-5 = high). For burnout, the overall mean score was 3.48, with subscale scores ranging from 3.32 to 3.60, which also aligns with the “moderate” category using similar cut-offs (e.g., 2.5-3.5 or up to 3.99 as moderate). Job satisfaction had a total mean of 2.88, with subscale scores between 2.54 and 3.05. According to comparable interpretation ranges (e.g., 1.67-3.32 as moderate), these scores indicate a moderate level of satisfaction, where the subscale with the lowest score was family/work balance, and the co-workers’ subscale was the one with the highest score. This average score of 2.88 indicates somewhat satisfied with their jobs, slightly higher than the healthcare professionals’ satisfaction level, with aspects needing attention in family/work balance (mean = 2.54), which was the lowest subscale score, as scores between 1.67 and 3.32 indicate moderate job satisfaction. The means and standard deviations of the sample responses were calculated for the scales of self-compassion, burnout, and job satisfaction among healthcare professionals. Table 2 shows the results.
The Means and Standard Deviations of the Self-Compassion, Burnout, and Job Satisfaction among Healthcare Professionals.

Relationship at the Level of Significance (α = 0.05) between Self-compassion, Burnout and Job Satisfaction Among Health Care Professionals
Pearson correlation coefficients were used between self-compassion, burnout and job satisfaction among health care professionals. Table 3 shows a positive, statistically significant correlation between self-compassion and job satisfaction. The correlation coefficient was r = 0.115. Also, there were a negative, statistically significant correlations between burnout and both self-compassion and job satisfaction. The correlation coefficient between burnout and self-compassion was r = −0.596, and the correlation coefficient between burnout and job satisfaction was r = −0.110.
Pearson Correlation Coefficient Values Between Self-Compassion, Burnout, and Job Satisfaction among Health Care Professionals.

**Correlation is significant at the 0.01 level (two-tailed).
*Correlation is significant at the 0.05 level (two-tailed).
Differences at the Level of Significance (α = 0.05) in Self-compassion Among Healthcare Professionals due to Demographic Variable
Means and standard deviations were extracted for the self-compassion among healthcare professionals according to gender, age, educational level, marital status, professional role, area of working, years of experience, and previous training on self-compassion program. Table 4 shows that there are apparent differences in the mean of the self-compassion due to gender, age, educational level, marital status, professional role, area of working, years of experience, and previous training on self-compassion program.
Means and Standard Deviations of the Self-Compassion due to Gender, Age, Educational Level, Marital Status, Professional Role, Area of Working, Years of Experience, and Previous Training on Self-Compassion Program.

To determine whether these apparent differences are statistically significant, an 8-way ANOVA was used. The findings shown in Table 5 emphasize the factors affecting self-compassion in healthcare professionals, including gender, age, education level, marital status, job role, work area, years of experience, and past training in self-compassion programs.
8-way ANOVA Results for the Differences in Self-Compassion due to Gender, Age, Educational Level, Marital status, Professional Role, Area of Working, Years of Experience, and Previous Training on Self-Compassion Program.

**Correlation is significant at the 0.01 level (two-tailed).
*Correlation is significant at the 0.05 level (two-tailed).
Bolded values are significant.
To begin with, gender, age, marital status, job position, work area, and past training in self-compassion programs did not reveal statistically significant variances in self-compassion at the p < 0.05 significance threshold. This indicates that, according to the data, these factors do not greatly influence healthcare professionals’ levels of self-compassion. The F-values for these variables were not significant, suggesting there were no substantial differences among the groups in these categories.
The 8-way ANOVA statistical analysis showed both significant and non-significant differences in self-compassion related to these variables. There are statistically significant differences at the level (α = 0.05) in self-compassion based on educational level and years of experience, as the F-values were significant. Table 5 shows these findings.
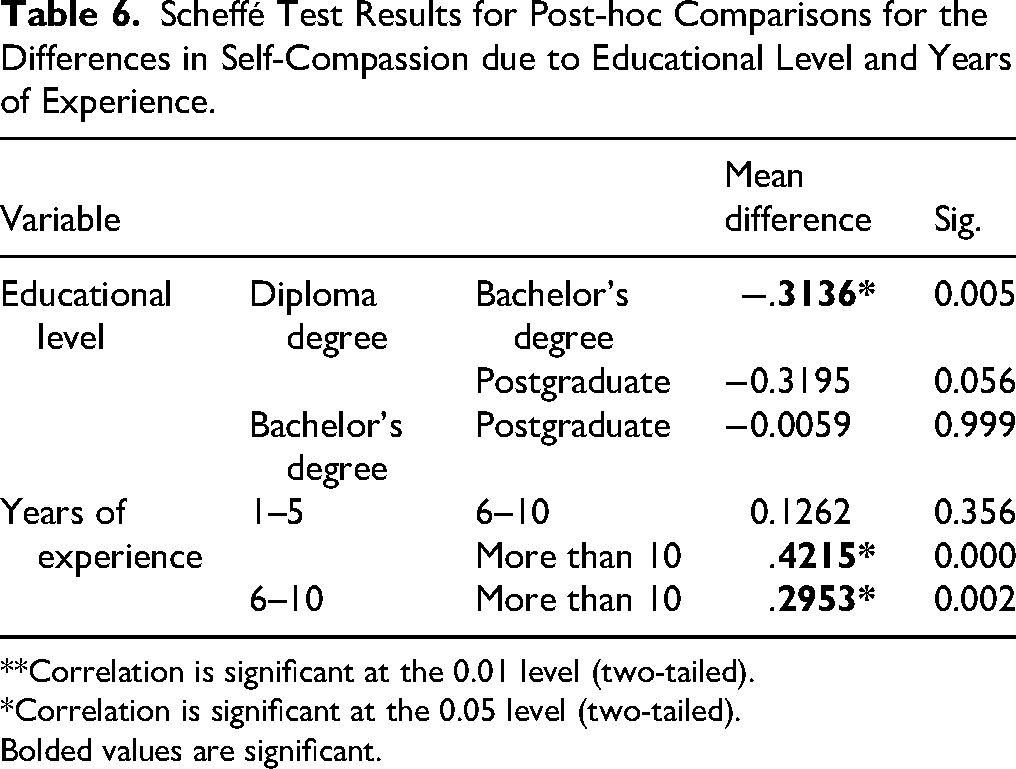
To determine which groups accounted for these differences, the Scheffé test was used for post-hoc comparisons. Table 6 shows statistically significant differences at (α = 0.05) in self-compassion based on educational level in favor for bachelor's degree compare with diploma degree. Also, there are statistically significant differences at (α = 0.05) in self-compassion due to years of experience in favor for 1–5 and 6–10 compare with more than 10.
Scheffé Test Results for Post-hoc Comparisons for the Differences in Self-Compassion due to Educational Level and Years of Experience.
**Correlation is significant at the 0.01 level (two-tailed).
*Correlation is significant at the 0.05 level (two-tailed).
Bolded values are significant.
The results show statistically significant differences in self-compassion based on educational attainment and years of experience. Healthcare professionals with a bachelor's degree exhibit significantly higher self-compassion than those with a diploma (mean difference = −0.3136, p = 0.005), while no significant difference is found between those with a bachelor's and postgraduate qualifications. These findings suggest that attaining at least a bachelor's degree may be associated with greater self-compassion.
Regarding years of experience, professionals with 1–5 and 6–10 years of experience show significantly higher self-compassion than those with over 10 years. The mean differences are 0.4215 (1–5 vs. >10 years, p = 0.000) and 0.2953 (6–10 vs. >10 years, p = 0.002). These findings suggest that less experienced professionals may have higher self-compassion, possibly due to a lower risk of burnout or disillusionment from prolonged exposure to the healthcare field
Regression and Mediation Analyses
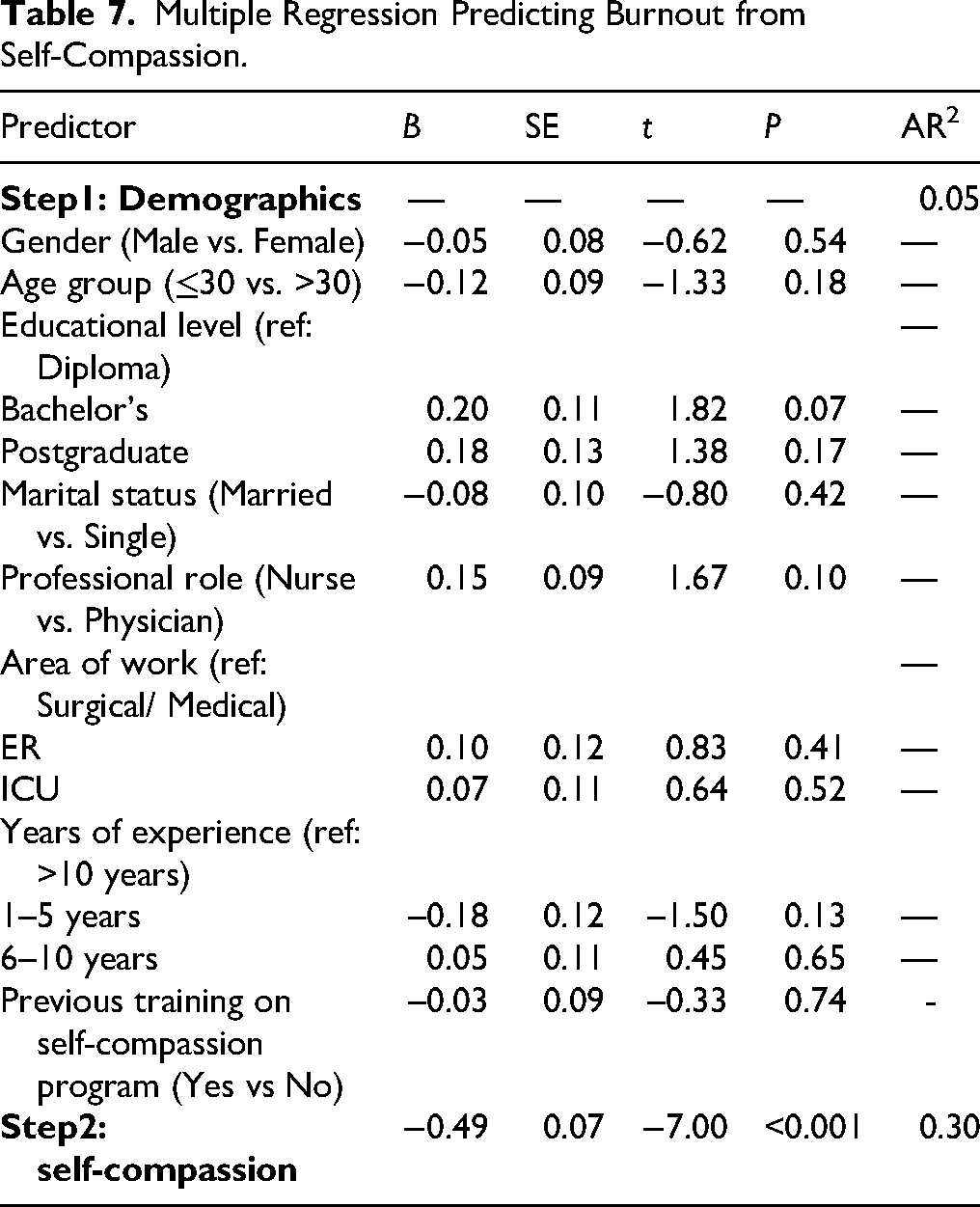
We conducted a hierarchical regression to examine whether self-compassion significantly predicts burnout when controlling for demographics. Table 7 shows that self-compassion was a significant negative predictor of burnout (β = −.49, t = −7.00, p < .001), accounting for an additional 30% of variance beyond demographics. This aligns with Lyon et al., where self-compassion predicted reductions in burnout (β ≈ −0.492).
Multiple Regression Predicting Burnout from Self-Compassion.
A similar model was tested with job satisfaction as the outcome. Table 8 shows that self-compassion remained a significant positive predictor of job satisfaction (β = .15, p = .013), explaining an additional 2% of variance. Though the effect size is smaller, this supports the correlation observed between self-compassion and job satisfaction (r = .115, p = .021).
Multiple Regression Predicting Job Satisfaction (Controlled for Demographics).

Mediation Analysis: Burnout Mediates the SC → JS Link
Using bootstrapped mediation with 5,000 resamples, the self-compassion's effect on job satisfaction through burnout was tested:
Path a Path b Indirect effect (a × b): β = .054, 95% CI [.020, .095], indicating significant mediation
Discussion
Emotional exhaustion emerged as the most pronounced component of burnout, while family/work balance received the lowest satisfaction rating—an organizational concern of considerable importance.
The current study found moderate baseline levels of self-compassion, burnout, and job satisfaction. These findings suggest neither particularly low nor particularly high levels of self-compassion, burnout, or satisfaction among participants. Comparing our sample—comprised of both nurses (74%) and physicians (26%)—with broader research suggests some nuance: in New Zealand samples, nurses appeared to derive greater protective benefit from self-compassion as a stress buffer, while physicians did not show the same moderation effect (Dev et al., 2020). This may reflect professional cultural differences, as nursing often prioritizes compassion, whereas medicine leans toward a perfectionist, biomedical outlook (Bedir & Eliüşük-Bülbül, 2023; Dev et al., 2019).
The correlation analyses revealed a significant negative correlation between self-compassion and burnout, which aligns with findings among Lebanese healthcare professionals who reported similar patterns of variance across burnout dimensions (Hashem & Zeinoun, 2020). Moreover, hierarchical regression and mediation models confirmed that self-compassion is a meaningful negative predictor of burnout, which in turn partially mediates its positive impact on job satisfaction. Future subgroup analyses could investigate whether these mechanisms operate differently in nurses versus physicians, a question raised by comparative studies (Chemali et al., 2019; Dev et al., 2020).
As expected, higher burnout was correlated with lower job satisfaction, consistent with regional data connecting emotional exhaustion to dissatisfaction (Hashem & Zeinoun, 2020; Nimer et al., 2021). However, the direct positive effect of self-compassion on job satisfaction was modest—yet significant—and appeared largely indirect, functioning through its buffering effect on burnout (Babenko et al., 2019).
Demographic analysis did not show significant variations in self-compassion by gender, age, or previous training. However, education and experience emerged as significant predictors: individuals with a bachelor's degree exhibited higher self-compassion than those with diploma-level qualifications, and professionals with less than 10 years in practice demonstrated higher self-compassion than their more experienced peers. This could reflect early-career resilience or motivations maintained during foundational training.
These findings support our conceptual framework, confirming self-compassion's role in reducing burnout and enhancing job satisfaction. Prior research (Amin, 2021; Eriksson et al., 2018; Vaillancourt & Wasylkiw, 2020) has similarly identified self-compassion as a protective factor in high-stress roles. The observed patterns are also consistent with self-determination theory, which emphasizes the role of self-compassion in intrinsic motivation and engagement (Khamisa et al., 2015; Manninen et al., 2022), and with evidence that burnout mediates the self-compassion—job satisfaction relationship (Giorgi et al., 2018; Vaillancourt & Wasylkiw, 2020). In practice, developing organizational strategies—such as structured self-compassion training, stress-management workshops, and peer-support systems—may help strengthen resilience and well-being among healthcare professionals.
Strengths and Limitations
The cross-sectional design limits causal inference between self-compassion, burnout, and job satisfaction. Additionally, reliance on self-report questionnaires introduces recall bias and social desirability bias. The use of convenience sampling within a specific geographic and cultural context may limit generalizability to broader and different healthcare populations. Finally, the observational nature of the study leaves open the possibility of unmeasured confounding variables, such as workload, personal coping styles, organizational support, or baseline mental health—that could influence the observed associations. Future research employing longitudinal or intervention-based designs, randomized or stratified sampling, and rigorous control for potential confounders is recommended to strengthen causal inference, reduce bias, and improve generalizability.
Implications for Practice
These findings suggest potential opportunities for nursing leadership to consider implementing interventions that may enhance self-compassion, reduce burnout, and improve job satisfaction among nursing staff. For example, institutions might explore the introduction of self-compassion training programs, stress-management workshops, or peer-support groups to foster a more supportive work environment. Ongoing assessments of staff well-being and burnout could help identify concerns and inform tailored interventions. Adopting policies that promote work-life balance, flexible scheduling, and adequate staffing levels may alleviate workload-related stress. Recognition and fair rewards may support personal accomplishment and job satisfaction. Incorporating principles of self-compassion into leadership training could further support morale, retention, and organizational effectiveness.
Conclusion
One of the most notable findings was that educational level and years of experience were significantly associated with self-compassion. Specifically, participants with a bachelor's degree demonstrated higher levels of self-compassion compared to those with a diploma, and healthcare professionals with fewer years of experience reported higher self-compassion than those with more than 10 years in practice. While previous literature has linked demographic factors to self-compassion in general, this study is among the first to identify educational level as a specific predictor of variance in self-compassion within this regional healthcare context. Furthermore, burnout was found to partially mediate the relationship between self-compassion and job satisfaction.
Footnotes
Acknowledgments
The authors acknowledge the study participants for their valuable participation.
Ethics Approval and Consent to Participate
Ethical approval was obtained from the Jordan University of Science and Technology Ethical Review Committee before data collection. Participation was voluntary, requiring written informed consent for the survey. The participants’ rights were clearly outlined in the consent forms and reiterated verbally before their participation, including the option to withdraw at any time. All data were anonymized to ensure confidentiality.
Authors Contributions
HD contributed to conceptualization, methodology, investigation, data curation, resources, funding acquisition, writing—original draft, and writing—review and editing. BS, HD, AD, and AA contributed methodology, investigation, formal analysis, project administration, and supervision. BS, HD, AD, and AA contributed to conceptualization, methodology, software, validation, investigation, data curation, formal analysis, writing—original draft, and writing—review and editing. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Deanship of Research at Jordan University of Science & Technology (Grant no. 20230518; JD 800).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used during the current study are available from the corresponding author upon reasonable request.
Study Approval Number
The study approval number (ref. number: 10/20/2024).