
Abstract
Objective
To explore the effects of massages administered by spouses on labor pain and delivery duration among primiparous women.
Methods
This quasi-experimental study included women who were selected to give birth at the researchers’ hospital and were assigned to either to an experimental or control group based on their willingness to participate. The experimental group received the massage during the latent and active phases of labor. Pain levels during labor were measured using the Visual Analog Scale.
Results
A total of 100 women, with 50 in each group, were included in the analysis. During both the latent and active phases of labor, the experimental group experienced greater reductions in pain levels compared with the control group (p < .001). Compared with the control group, fewer participants in the experimental group needed pain relief medication, although this difference was not statistically significant (36% in the experimental group vs. 56% in the control group, p = .07). The first stage of labor was significantly shorter for the experimental group (11.21 ± 5.25 h) than for the control group (16.06 ± 7.35 h, p < .001). However, no significant differences in the duration of the second and third stages were observed between the two groups.
Conclusion
The massage administered by spouses during labor significantly reduced labor pain and shorten the duration of the first stage of labor.
Introduction
Labor is very painful and can discourage women from pregnancy (Rafiei et al., 2018). The intensity of labor pain is influenced by several physiological and psychological factors. On the psychological side factors such as fear of labor pain, anxiety, and self-efficacy play a role, while physiological contributor include the mechanical stretching of the uterus and vagina, fetal positioning, maternal posture, and the strength and frequency of contractions (Zwelling et al., 2006). Anxiety and pain experienced during labor can cause prolonged labor due to increased cortisol and adrenaline levels, ultimately resulting in decreased uterine activity (Pawale & Salunkhe, 2020). Several risk factors, such as fetal mortality, postpartum infection, and fatigue, are linked to prolonged labor (Choudhary et al., 2021; Rafiei et al., 2018). Reducing labor pain is thus crucial from a clinical perspective.
Review of the Literature
Massage involves the manipulation of soft body tissues through kneading or stroking techniques to reduce pain and relieve stress. This technique is widely used in medicine to alleviate pain. According to multiple studies, massaging can effectively reduce labor pain (Karatopuk & Yarıcı, 2023; Maghalian et al., 2022; Shahbazzadegan & Nikjou, 2022; Taghinejad et al., 2010). Massages are frequently given by researchers or clinical staff. In perinatal care, spousal involvement is marked by empathy and responsiveness, which can enhance family functioning and mother–infant health (Mehran et al., 2020). After all, one does not feel the same affection toward the clinical staff as one does toward one's spouse. Therefore, massages administered by spouses for labor pain relief are likely to have clinical and psychological benefits. Previous studies have mainly looked at the effectiveness of massage given by nurses or other clinical staff, but this research focuses specifically on the role of spouse-administered massage during labor, highlighting the potential benefits of emotional closeness and support from a partner. The researchers believe that this perspective not only increases the clinical importance of the results of this study but also adds a new layer to the existing body of research on nonpharmacological pain management during childbirth.
However, the effects of massage administered by a spouse on labor pain remain unclear. The researchers hypothesized that spouse-administered massage would reduce labor pain and shorten the first stage of labor. Thus, in this study, the researchers explored the effects of massages administered by spouses on labor pain and delivery duration among primiparous women.
Methods
Study Design
Written informed consent was obtained from all participants prior to the commencement of the study. The study included women who decided to give birth at the researchers’ hospital between June 1, 2020, and June 31, 2021. This is a quasi-experimental study that examined the effects of the massage administered by spouses on labor pain and delivery duration. The included participants were divided into an experimental group and a control group. The experimental group received massage treatment during both the latent and active phases of labor, whereas the control group received standard care during the two phases. The main characteristics of the participants were recorded, including their age, height, prepregnancy body weight, current weight, gestational age, spouses’ education level and degree of menstrual pain. Pain levels were measured before and after the massage treatment, and the partogram period of giving birth was recorded. The researchers acknowledge the potential value in comparing the effectiveness of massage between healthcare professionals (nurses) and spouses. This comparison was beyond the scope of this current research design, and the researchers suggest that future studies include this additional group to assess potential disparities in the efficacy of massage between professional and nonprofessional caregivers. This could provide important insights into optimal care delivery and resource allocation.
Inclusion and Exclusion Criteria
Pregnant women in their third trimester were included in the study. Those who agreed to receive the massage treatment were allocated to the experimental group, whereas those who did not were allocated to the control group. Women who met the following criteria were enrolled in the study: (1) being a primipara, (2) having a gestational age exceeding 32 weeks, (3) having a singleton pregnancy, (4) planning for a vaginal delivery, and (5) having a spouse present throughout the childbirth process. Individuals meeting the following criteria were excluded from the study: (1) experiencing symptoms indicative of a high-risk pregnancy or (2) requesting a cesarean section for any reason.
Treatment During the Latent and Active Phases
For usual care, birthing balls were provided in the delivery room for use based on individual needs. A birthing ball was positioned on the bed, allowing the patient to lean on it as needed. During pain, participants were instructed in slow, deep breathing techniques and given massage tools (such as tennis balls or massage sticks) to target pain points. The usual care group served as a comparison for those who received the massage, with the assumption that the massage group would experience greater benefits. In the experimental group, the spouses received standardized training in the massage techniques before the intervention. The training was adapted from a modified version of Kimber's guidelines (Shahbazzadegan & Nikjou, 2022) and included both theoretical instruction and supervised hands-on practice to ensure consistency and accuracy in technique. The massage were performed in the delivery room under the supervision of trained nursing professionals. During the procedure, the expectant mother assumed a standing position with her feet shoulder-width apart and knees slightly bent. A birthing ball was placed on the bed to support her upper body without applying pressure to the abdomen. The woman's posture and bed height were adjusted as needed to ensure comfort and muscle relaxation. The spouse assumed an archer's stance, warmed the massage oil by rubbing it between both hands, and applied it evenly to the woman's lower back and buttocks, including the sacral area. Firm, steady pressure was applied as the hands moved upward from the sacral region to the waist, with intensity adjusted according to the woman's comfort. The woman was instructed to inhale during this movement. Next, the partner rotated both arms outward by 90 degrees without applying pressure. As the woman exhaled slowly, the partner maintained contact with the skin and gently glided the hands outward to the iliac (hip) regions. Then, the hands were rotated another 90 degrees so that the fingertips pointed toward the woman's head, followed by a gentle downward stroke returning to the sacral area. This sequence constituted one massage cycle and lasted approximately 60 s. The massage was repeated for five cycles. At the conclusion of the fifth cycle, gentle pressure was applied to the sacral area using one palm. This massage protocol was administered during both the latent and active phases of labor. In the control group, usual care was provided during both labor phases and included nonpharmacological options such as birthing balls, breathing techniques, and massage tools based on individual needs.
Clinical Outcome Measurement
Labor pain levels were assessed via the Visual Analog Scale (VAS), a self-reported pain measurement with ratings spanning from 0 to 10, with higher scores signifying increased pain intensity. Pain levels were recorded before and after each treatment (massage or usual care). The three stages of the labor period were recorded. In addition, whether any pain relief medication was used during delivery was documented.
Sample Size Calculation
In a previous study, they used a massage treatment to reduce pain during labor (Shahbazzadegan & Nikjou, 2022). They reported average VAS scores of 4.79 ± 1.18 for the experimental group and 7.17 ± 1.37 for the control group. In this study, the researchers calculated the minimum sample size using the G-power 3.2 software. A two-sample t-test was conducted to determine the differences between the two groups. Assuming a statistical power of 80% and a two-sided significance level of .05, the researchers determined that at least 12 participants per group were required. The researchers recruited 50 participants per group to obtain results with greater statistical power and to buffer for a 20% dropout rate.
Statistical Analysis
All statistical analyses were conducted using IBM SPSS Statistics version 28.0 software for Windows (IBM, Armonk, NY, USA). Continuous variables are presented as means and standard deviations, and categorical variables are presented as frequencies and percentages. A paired t-test was conducted to identify differences before and after treatment. A two-sample t-test was also conducted to determine the differences in the continuous variables between the two groups. A chi-square test was used to evaluate the distribution of categorical variables across the two groups. A sensitivity analysis was performed by excluding participants who received additional or alternative treatments. The p-values for multiple comparisons were adjusted using the Bonferroni correction. A multiple linear regression analysis was conducted to adjust for potential confounding factors.
Results
Of the 135 women who met the inclusion criteria, 72 expressed interest in receiving massages, whereas 63 did not (Figure 1). In the experimental group, 22 women gave birth through cesarean section and were therefore excluded from the study. In the control group, 13 women were excluded from the study: 12 women gave birth through cesarean section, and one woman withdrew from the study. The rate of assisted vaginal delivery was 31% for the experimental group and 19% for the control group. Ultimately, 100 women (50 in the experimental group and 50 in the control group) were included in the analysis. The mean age of these women was 29.9 ± 4.3 years, and their gestational age was 38.8 ± 0.9 weeks. No significant differences were observed in age, height, prepregnancy body weight, current weight, gestational age, spouses’ education level, and degree of menstrual pain between the two groups (Table 1).
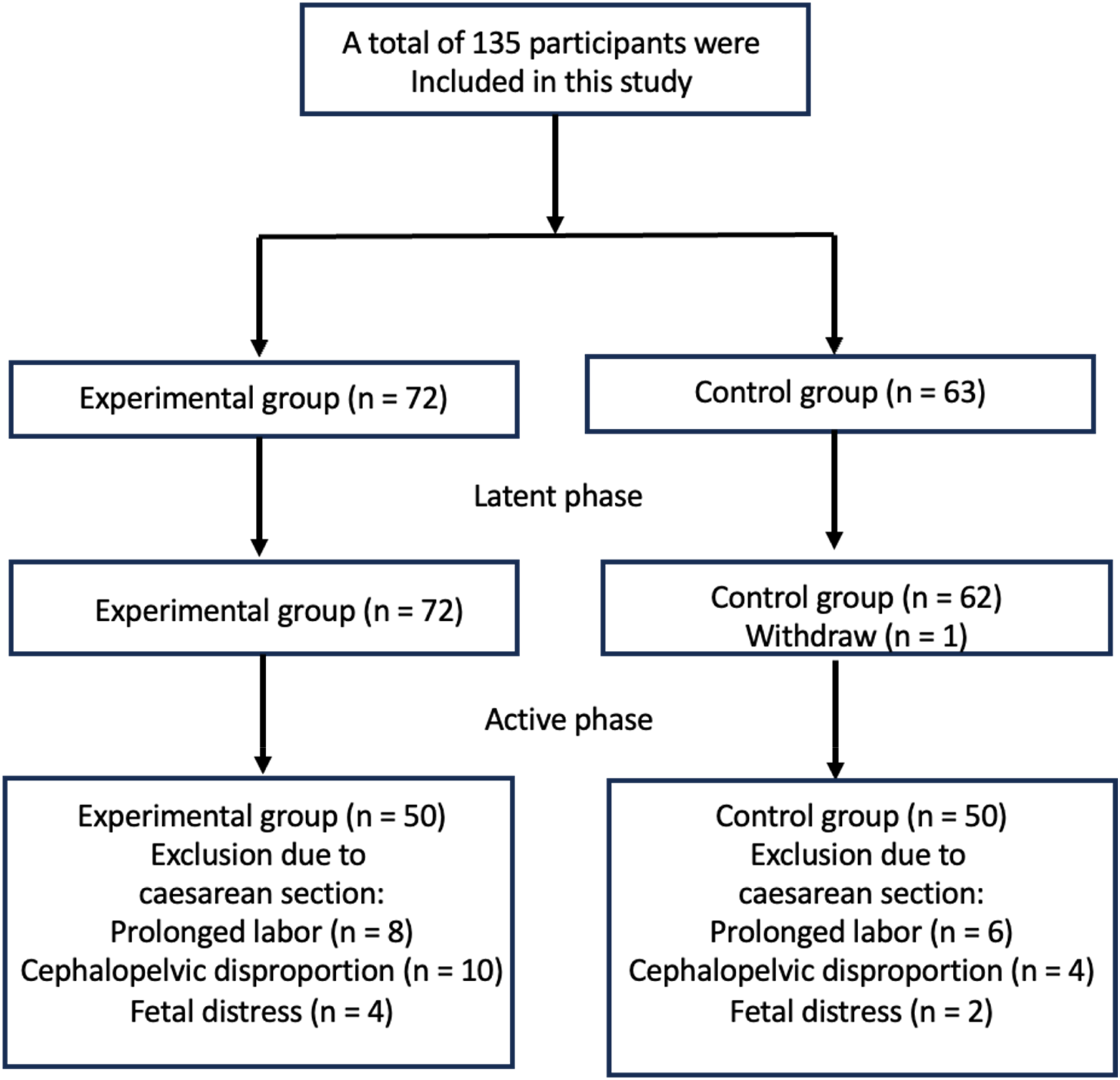
Flowchart of the Participant Recruitment Process.
Baseline Characteristics of the Participants in the Experimental and Control Groups.a
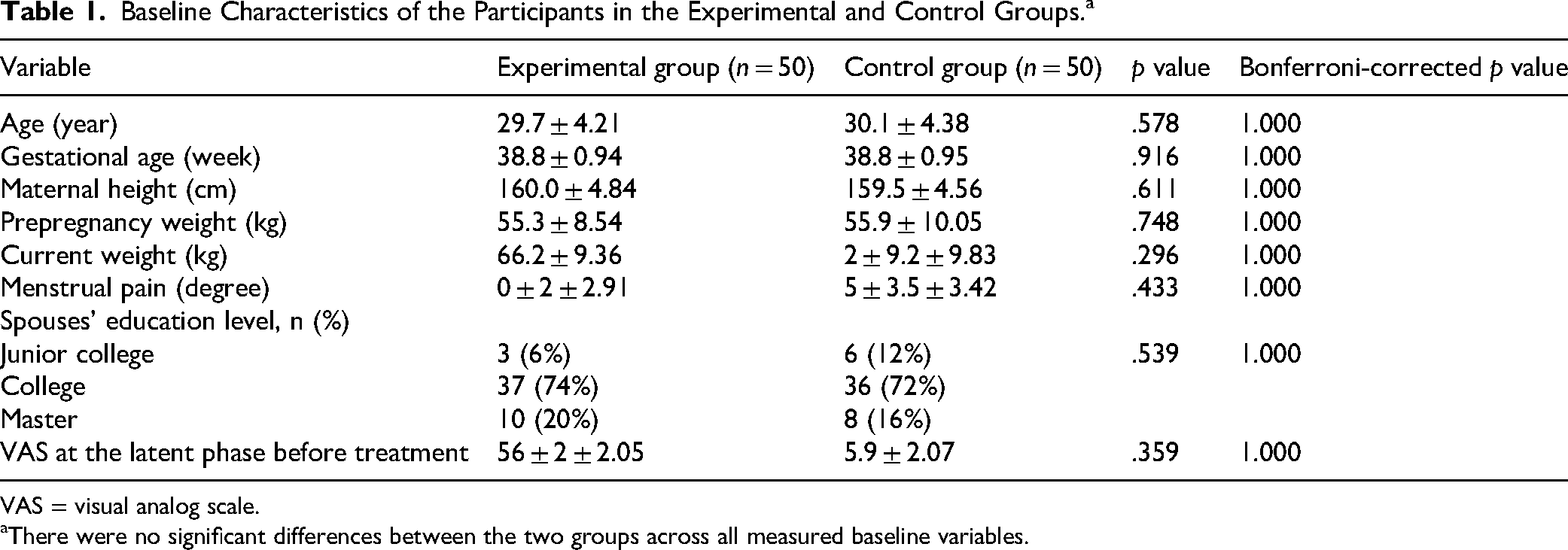
VAS = visual analog scale.
There were no significant differences between the two groups across all measured baseline variables.
During both the latent and active phases of labor, the levels of pain significantly decreased after treatment in the two groups (Table 2). In addition, the experimental group exhibited a greater reduction in pain levels than the control group (p < .001, Figure 2). In the experimental group, some women received usual care in addition to massages during the latent phase. Research found no significant differences in pain levels between women who received massages and those who received massages along with the usual care (p = .827), suggesting that adding the usual care to the massage did not lower pain levels (Figure 3). During the active phase, nine women did not receive the massage. When the women in question were left out of the analysis, a more significant decrease in pain levels was observed in the group that received the treatment than in the group that did not (p < .001, Figure 4). Moreover, the researchers excluded women who received the massage combined with the usual care. Women receiving massages reported significantly more pain relief than those receiving usual care, with higher pain relief during both the latent phase (experimental group −2.07 ± 1.94 vs. usual care −0.86 ± 1.34, p = .002) and active phase (experimental group −2.22 ± 2.56 vs. usual care −0.79 ± 1.44, p = .011). Multiple regression analysis was used to adjust for potential confounding factors. The results showed that the experimental group had significantly decreased pain levels during both the latent and active phases (Table 3). Some women received pain relief medications during the active phase. A smaller percentage of women in the experimental group (36%) received pain relief medications compared with the control group (54%, p = .07). There was no significant difference in pain relief between those who received epidural analgesia and those who did not (p = .701). Findings from a comparison of labor duration between the two groups showed that participants in the experimental group experienced a shorter first stage labor duration of 11.21 ± 5.25 h compared to those in the control group, whose labor duration was 16.06 ± 7.35 h, with a statistically significant difference (p_correction = .004, as listed in Table 4). No notable differences were found in the second and third stages between the two groups (Table 4). On the whole, the experimental group had a shorter labor duration (12.59 ± 5.31 h) compared with the control group (17.87 ± 7.95 h, p_correction = .004, Table 4).

Pain Relief After Treatment in the Experimental Group (n=50) and Control Group (n=50) During the Latent Phase (A) and Active Phase (B) of Labor. In Both Phases, the Experimental Group Demonstrated Significantly Greater Pain Reduction Compared to the Control Group (p < .001). Error Bars Indicate±Standard Deviation.

In Women Who Received the Massage Only (n=27) and Women Who Received the Massage Combined with the Usual Care (n=23) During the Latent Phase of Labor, No Significant Difference in Pain Relief was Found Between the Two Groups (p=.827). Error Bars Indicate±Standard Deviation.

Labor Pain Relief After Treatment in the Experimental Group (Excluding Nine Women Who did Not Receive the Massage) and the Control Group During the Active Phase of Labor. The Experimental Group Showed Significantly Greater Pain Reduction Than the Control Group (p < .001). Error Bars Indicate±Standard Deviation.
Pain Levels Before and After the Massage Treatment During the Latent and Active Phases of Labor.

Bold font indicates statistical significance.
Multiple Linear Regression Analysis of Factors Associated with Pain Relief Following Intervention During the Latent and Active Phases of Labor.

Ref = reference; β = coefficient.
Bold font indicates statistical significance.
Duration of Labor in the Experimental and Control Groups.

Bold font indicates statistical significance.
Discussion
This quasi-experimental study investigated the effects of the spouse-administered massage on labor pain and the duration of labor. The results demonstrated that participants in the experimental group experienced greater reductions in pain intensity during both the latent and active phases of labor compared with those in the control group. Furthermore, a lower proportion of women in the experimental group (36%) required pharmacological pain relief during the active phase, compared with 54% in the control group. The first stage of labor was also significantly shorter in the experimental group. Overall, these findings suggest that the massage provided by spouses were an effective nonpharmacological intervention for alleviating labor pain and reducing the duration of the first stage of labor.
This study employed a quasi-experimental design, which offers greater methodological rigor than observational studies but lacks the robustness of randomized controlled trials. No significant differences were found in the key baseline characteristics between the experimental and control groups (Table 1), indicating successful group comparability. To further control for potential confounding factors, the researchers conducted multiple regression analysis (Table 3), which confirmed that the experimental group experienced significantly greater pain relief than the control group. The sensitivity analysis excluding participants who received combined treatments yielded consistent results, reinforcing the robustness of the findings. These outcomes suggest that the massage intervention is associated with significantly greater pain relief. Nonetheless, future randomized controlled trials are needed to validate these results and establish a stronger causal inference.
A previous study identified 7 cm of cervical dilation as the optimal time point for the massage to effectively relieve labor pain, with no significant effect observed at 5 or 9 cm (Shahbazzadegan & Nikjou, 2022). A previous study identified 7 cm of cervical dilation as the optimal time point for massage to effectively relieve labor pain, with no significant effect observed at 5 or 9 cm (Vehviläinen-Julkunen & Emelonye, 2014), which may partly explain the effectiveness observed in the findings of this study. The added emotional support and intimacy of partner-administered massage may contribute to greater relaxation and pain relief. However, because the researchers did not include a comparison group receiving the massage from nurses, the researchers were unable to evaluate whether the spousal massage offers superior benefits. Future studies should directly compare the effectiveness of the massage administered by spouses versus healthcare providers.
Although the difference in pain relief medication use between the experimental and control groups did not reach statistical significance (p = .07), the observed trend may still hold clinical relevance. Participants in the experimental group showed a reduced tendency to request or require pharmacological analgesia during labor. This finding aligns with the broader goal of promoting nonpharmacological pain management strategies, particularly in low-risk pregnancies where minimizing medical interventions is often preferred (Mrayan et al., 2024). Despite the lack of statistical significance, the trend may reflect a meaningful impact on maternal experience and care preferences. Reduced reliance on analgesics is associated with fewer side effects (Arendt et al., 2012), reduced monitoring requirements, and improved postpartum recovery. Further studies with larger sample sizes are needed to determine whether this trend persists and reaches clinical and statistical significance.
The findings of this study indicate that the massage treatment significantly shortened the duration of the first stage of labor but had no notable effect on the second or third stages. The first stage is characterized by cervical dilation, which depends on coordinated uterine contractions and can be influenced by the mother's emotional and physiological state (Victoria, 2024). Prior research has shown that massage reduces maternal stress and anxiety, leading to decreased levels of circulating catecholamines—such as adrenaline and noradrenaline—which are known to inhibit uterine contractility and delay cervical dilation (Selian et al., 2024). Furthermore, back massage may activate the parasympathetic nervous system, stimulating oxytocin release, promoting relaxation, lowering adrenaline levels, and enhancing the strength and coordination of uterine contractions (Ferina, 2023). These combined physiological effects support the conclusion that massage contributes to a more efficient and synchronized first stage of labor, thereby potentially reducing its length.
Strength and Limitations
Strengths of this study include its quasi-experimental design, which offers improved control over potential confounding factors compared to observational studies, while maintaining feasibility in a clinical setting. The use of standardized massage techniques administered by spouses who received structured training ensured consistency in the intervention. Pain levels were assessed at two critical phases of labor using a validated instrument (VAS), and labor stages were objectively recorded using partogram data, enhancing the reliability of outcome measurement. Furthermore, the study employed multiple statistical approaches—including sensitivity analyses and regression modeling—to strengthen the validity and robustness of the findings. The incorporation of both physiological and behavioral outcomes (pain reduction, labor duration, analgesic use) provided a comprehensive evaluation of the intervention's effects.
This study has several limitations. First, although the researchers employed a quasi-experimental design—which offers stronger evidence than observational studies—it lacks the methodological rigor of a randomized controlled trial. The group assignment was based on participant preference, which may limit generalizability and introduce bias related to participant motivation or expectations. While no significant differences were found in the key baseline characteristics between the groups, and multiple regression analysis was used to adjust for potential confounders, the findings should be confirmed through future randomized controlled trials. Second, the usual care provided to the control group was not standardized and included a variety of interventions such as birthing balls, deep breathing exercises, and massage tools. Not all participants received the same combination of care, which may have introduced variability and made it more difficult to isolate the specific effects of spouse-administered massage. Third, the massage in the experimental group was performed by spouses, who although trained, were not professional massage therapists. This may have led to inconsistencies in the massage technique and introduced potential bias in evaluating the intervention's effectiveness. Future studies should aim to minimize these limitations by implementing randomized designs, standardizing control interventions, and comparing the effects of massage delivered by different caregivers—including trained professionals or healthcare staff—to more accurately assess the impact of massage on labor pain relief.
Implications for Practice
The findings of this study suggest that integrating spouse-administered massage into standard labor care protocols may offer significant clinical benefits. Given its effectiveness in reducing pain intensity and shortening the first stage of labor, spousal massage represents a viable, low-cost, and nonpharmacological intervention that can enhance the childbirth experience for primiparous women. Encouraging spousal participation not only promotes emotional bonding and support but also empowers partners to play an active role in labor and delivery, potentially improving family dynamics and postpartum outcomes. Hospitals and maternity centers may consider implementing structured educational programs to train partners in massage techniques prior to labor. This approach could be especially advantageous in settings with limited access to pharmacological pain relief or where women prefer minimal medical intervention. By promoting greater involvement of family members and reducing reliance on analgesics, this practice aligns with broader goals of personalized and holistic maternal care. Future policies should consider formalizing such partner-inclusive interventions as part of antenatal education and delivery room protocols.
Conclusion
The findings of this study suggest that spouse-administered massage therapy is an effective nonpharmacological intervention for reducing both labor pain and labor duration of the first stage. Given its ease of implementation, low cost, and potential to enhance partner involvement during childbirth, the massage therapy could be integrated into standard maternity care. Further high-quality randomized controlled trials are required to verify these advantages and compare the efficacy of massages administered by various caregivers, including nurses or professional therapists. Validating massage therapy could make it a viable pain management option for laboring women, especially in areas where medication for pain relief is scarce.
Footnotes
Ethical Statement
The present study was approved by the Ethics Committee of the Ditmanson Medical Foundation Chia-Yi Christian Hospital (permit number: IRB2020020).
Author Contributions
Conceptualization, P.-H. C.; Data Curation, C.-H. K. and S.-C. G.; Formal analysis: P. W. and C.-L. S.; Funding acquisition, P.-H. C.; Investigation, P.-H. C. and C.-L. S.; Methodology, C.-L. S.; Writing – original draft, P.-H. C. and C.-L. S.; Writing – review & editing, P.-H. C. and C.-L. S.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Ditmanson Medical Foundation Chia-Yi Christian Hospital (Grant No. R109-12) and the National Science and Technology Council, Taiwan (Grant No. NSTC 114-2320-B-705-001).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.