
Abstract
Introduction and Purpose
Geriatric patients, who are fed by nasogastric tube (NG), may suffer from complications. Therefore, this study was conducted to evaluate the effect of abdominal massage on Gastric residual volume (GRV), distension, vomiting, and defecation in geriatric patients, who were hospitalized in intensive care unit and fed by NG.
Methods
The quasi-experimental study was conducted in intensive care units. The researcher applied abdominal massage to patients in the intervention group (n = 30) twice a day for 15–20 minutes before feeding. The data of the study were collected by using a questionnaire and a parameter questionnaire.
Results
GRV decreased significantly in the intervention group and increased significantly in the control group (p < 0.05). The frequency of defecation significantly increased in intervention group (p < 0.05). It was found that there was no positive effect of abdominal massage on vomiting (p > 0.05).
Conclusion
It was observed that while abdominal massage reduced high GRV and distension incidence, it increased the incidence of defecation.
With the aging of the population in the world, the incidence of chronic diseases is increasing rapidly. With the advancement of age, physiological changes occur. Due to these changes, the body’s resistance to diseases decreases and the incidence of chronic diseases increases (Bakır & Akın, 2019). Of the patients hospitalized in intensive care unit in Turkey, 41.5 percent are elderly patients (Turkish Ministry of Health [TMH], 2015). In a prevalence study, it was stated that the mean age of patients admitted to intensive care was 64. In another study, the mean age of patients in intensive care unit was reported to be 71 (Yıldız et al., 2019).
Generally, elderly patients are hospitalized in the intensive care unit due to cardiovascular diseases, acute respiratory failure, sepsis or trauma (Ülger & Cankurtaran, 2006). Such patients in the intensive care unit may not be fed orally because of neuromuscular, gastrointestinal, and cardiovascular diseases as well as trauma, mechanical ventilation, and risk of aspiration. Therefore, parenteral or enteral feeding is used to meet their daily energy needs. Methods of enteral feeding include nasogastric tube, nasojejunal tube or gastrostomy (Gök Metin & Özdemir, 2015). However, these feeding methods lead to some problems such as constipation, abdominal distention, diarrhea, and vomiting (Saka, 2010).
Contamination of nutritional solutions, their administration at inappropriate temperatures or speed, side effects of antibiotics given to patients, and inactivity in intensive care patients cause these problems (Gök Metin & Özdemir, 2015) Elderly patients frequently take multiple medications which can affect the absorption, digestion and metabolism of nutrients. Gastrointestinal side effects are more common in the elderly due to the simultaneous administration of enteral nutrition and medication (Yeşildemir & Tek, 2018). Patients should not have abdominal distension, pain or high gastric residual volume. In addition, adequate bowel sounds and defecation counts are indicators of nutritional tolerance (Köse & Ayhan, 2018).
Numerous studies have reported that complications such as GRV increase (Elpern et al., 2004; Mentec et al., 2001), digestive intolerance (Mentec et al., 2001), constipation, abdominal distension and vomiting develop in enterally fed patients (Montejo, 1999; Uysal et al., 2012). Additionally, in their study, Kuslapuu et al. (2015). stated that high GRV reduced or ceased enteral nutrition. Abdominal massage is useful especially in patients fed by tube in order to prevent these problems and maintain feeding (Olgun, 2016). During abdominal massage, intra-abdominal pressure is changed and pressure is directed to the rectum so that the intestines are stimulated mechanically. The effect of the massage stimulates peristalsis, thus resulting in shortened transition time of nutrients through the gastrointestinal tract and accelerated bowel movement (Turan & Aştı, 2015). In addition, abdominal massage reduces feelings of discomfort (Sinclair, 2011; Turan & Aştı, 2015) and enhances the quality of life since it is easy-to-apply (Turan & Aştı, 2015) and has no known side effects (Harrington & Haskvitz, 2006; Lamas et al., 2009; Turan & Aştı, 2015). In their study, Kim et al. (2005) stated that abdominal massage along with aromatherapy reduced constipation levels of geriatric patients. Also, in their study, Liu et al. (2005) stated that abdominal massage stimulated rectal waves, thus causing defecation in patients with myopathy. The studies conducted with patients who were suffering from multiple sclerosis and fed by intubation and enteral feeding have revealed that abdominal massage has positive effects such as alleviating constipation and decreasing GRV (Kahraman & Özdemir, 2015; McClurg et al., 2011). Bromley (2014) stated that abdominal massage alleviated constipation symptoms and reduced the use of laxative drugs in children with mental and physical disabilities. In addition, there are studies indicating that abdominal massage reduces vomiting (Tekgündüz et al., 2014; Uysal et al., 2012). It is seen that although there is a great number of studies examining the effect of abdominal massage on complications related to enteral feeding in different patient groups, there is a limited number of studies evaluating the effect of abdominal massage in geriatric patients.
Preventing enteral nutrition complications and participating in treatment when they arise is one of the nursing roles (Koçhan & Akın, 2018). When enteral feeding complications such as constipation, abdominal distention and vomiting occur, nurses may resort to abdominal massage (Ayaş et al., 2006; Çevik et al., 2018; Dehghan et al., 2018; Momenfar et al., 2018; Uysal et al., 2012). Abdominal massage is one of the non-pharmacological methods that can be applied by nurses (Ayaş et al., 2006; Kahraman & Özdemir, 2015, Uysal et al., 2012).
In the literature, studies evaluating the effect of abdominal massage performed by nurses are limited. Thus, the aim of this study was to determine the effect of abdominal massage on parameters of enteral nutrition tolerance in geriatric ICU patients.
Methods
Design, Setting and Sample
The study was conducted with a quasi-experimental design in the reanimation, internal medicine, neurology, and pulmonary intensive care units of a state hospital between March and August 2017. The number of patients to be included in each group was calculated in the computer program based on the method used in a previous, related study (Uysal et al., 2012) (using average GRV) and power analysis. As a result of the calculation, the number of patients to be included in each group was determined to be 30.
Flow of the Study
The patients who met the inclusion criteria were given numbers according to the order of their hospitalization and while odd numbers were assigned to the control group (n = 37), even numbers were assigned to the intervention group (n = 38). The single blind method was used to hide the group of patients. Since 7 patients from the control group and 8 patients from the intervention group were excluded from the study during the follow-up, the study was finished with 60 patients. The CONSORT flow diagram shows the inclusion process of the patients (Figure 1).
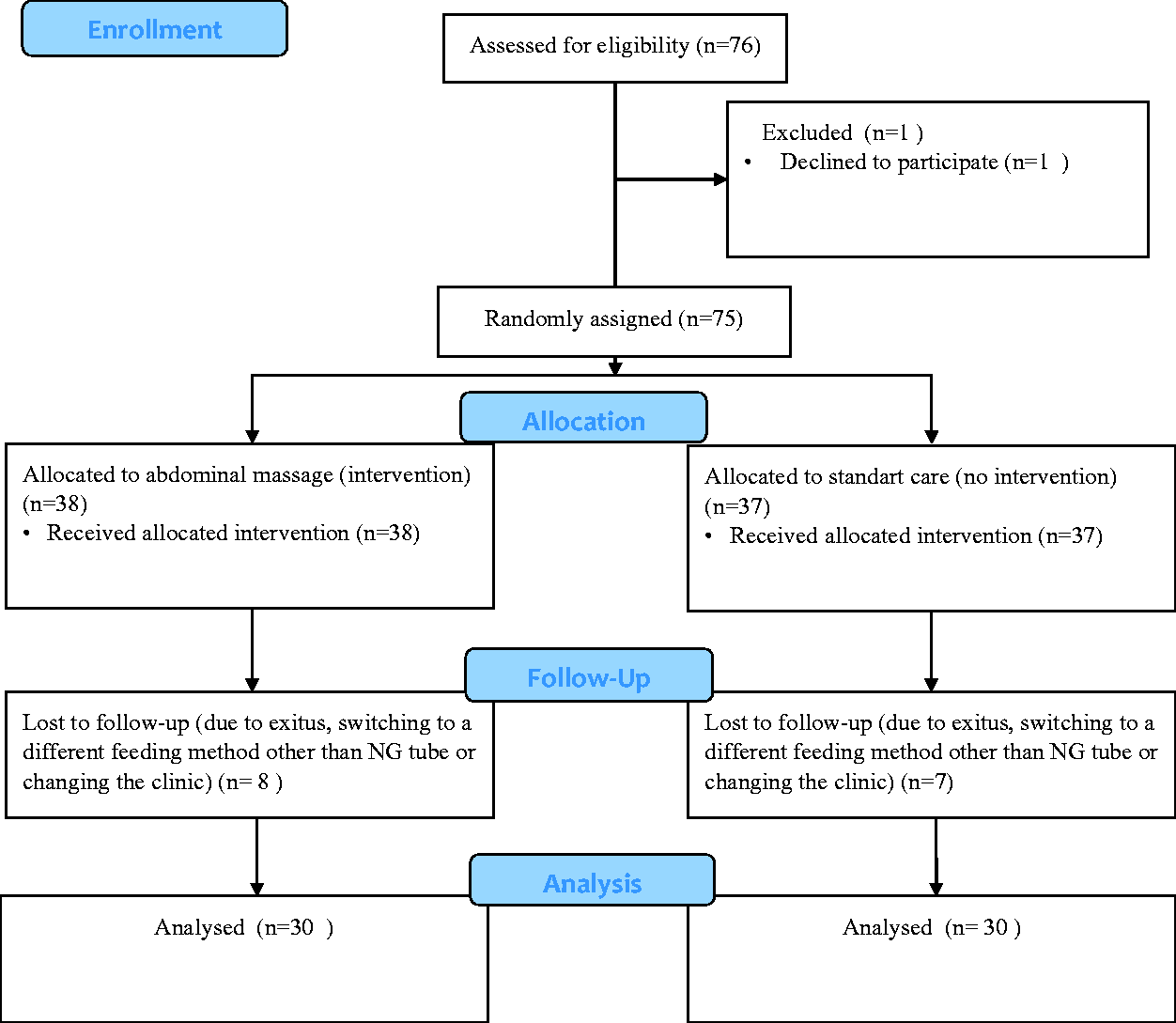
CONSORT Flow Diagram of the Participants.
The sample size was calculated as a total of 60 patients at an effect size of d = 0.78, error margin of 5% and power of 84% (α = 0.05, 1−β = 0.83). Afterwards, the researcher conducted interviews with the patients and their relatives, received information about the patients and started the follow-up process. The inclusion criteria of the study were being 65 years and over, being admitted to intensive care unit, having just started receiving nasogastric feeding, having no contraindication for abdominal massage (recent radiotherapy or abdominal surgery, obstruction, having an open wound on the abdominal area), being continuously fed by enteral feeding (20 hours), and agreeing to participate in the study. For the patients who were unable to give consent for participation, the consent was obtained from their first-degree relatives.
The patients were expected to reach the specified target calories. They were followed up for 3 days after reaching the target calorie in order to see possible complications. Since each patient reached the target calories at different times, their follow-up period also varied. The mean follow-up period was 6 days.
Data Collection
The data of the study were collected by using a questionnaire and a parameter questionnaire.
Questionnaire: This questionnaire is composed of questions about age, marital status, occupation, income status, number of children, regularly taken drugs, and presence of chronic diseases. The patients or their first-degree relatives were interviewed and informed comprehensively about the study, their consents were obtained, and they filled the questionnaire using the face-to-face interview method.
Parameter questionnaire: The questionnaire was prepared according to the studies conducted by Sevinç (2007) and by Montejo (1999) and by taking expert opinions. This questionnaire, prepared by the researchers in the light of these studies, includes the gastric residual volume, abdominal circumference, number of vomiting, number of defecation, nutrients taken, amount-speed of nutrients, drugs taken, and necessary and recommended calorie amounts for the patients. Amount speed is the speed at which a nutrition solution is administered to a patient over the period of an hour. Essential calories refer to the patient’s daily calorie intake calculated by a dietician. Recommended calories, on the other hand, refer to the amount of calories prescribed by a doctor for the patient. It has no scale-type scoring system. In this questionnaire, the follow-up times of the patients were listed and the changes occurring during these times were recorded. In the study conducted by Uysal et al. (2012) on effects of abdominal massage, a similar questionnaire was used.
Implementation Process
The patients meeting the inclusion criteria were determined among the patients for whom the nutritional team decided to start enteral feeding. The patients were given numbers (1 to 60) based on order of admission to the intensive care unit. While the patients with an odd number were included in the control group, the patients with an even number were included in the intervention group.
In the specified intensive care units, the type of enteral feeding is “continuous enteral feeding”. The feeding starts at 12:00 pm and continues with a 30-minute break at 12:00-16:00-20:00-24:00-08:00 hours. Distension, examined by palpation and the measurement of abdominal girth, and GRV are recorded. Feeding is finished at 10:00 am and starts again at 12:00 pm. In the present study, distention examined by palpation and the measurement of abdominal circumference at the same hours were recorded on the parameter questionnaire. The patients in the intervention group received abdominal massage during the follow-up period at 11:00 am and 19:00 pm in addition to the interventions in the control group. Enteral feeding was finished 30 minutes before the massage in order to eliminate the contents of the stomach. Abdominal massage was applied for 15–20 minutes twice a day for 5–7 days until the target calorie was reached, in accordance with the literature (Montejo, 1999; Uysal et al., 2012). After the patients in both groups reached the target calories, they were followed-up for three additional days.
The researcher did not hold an abdominal massage certificate, however received massage training during nursing education. The physiotherapist of the hospital was consulted on the application of abdominal massage (Figure 2).
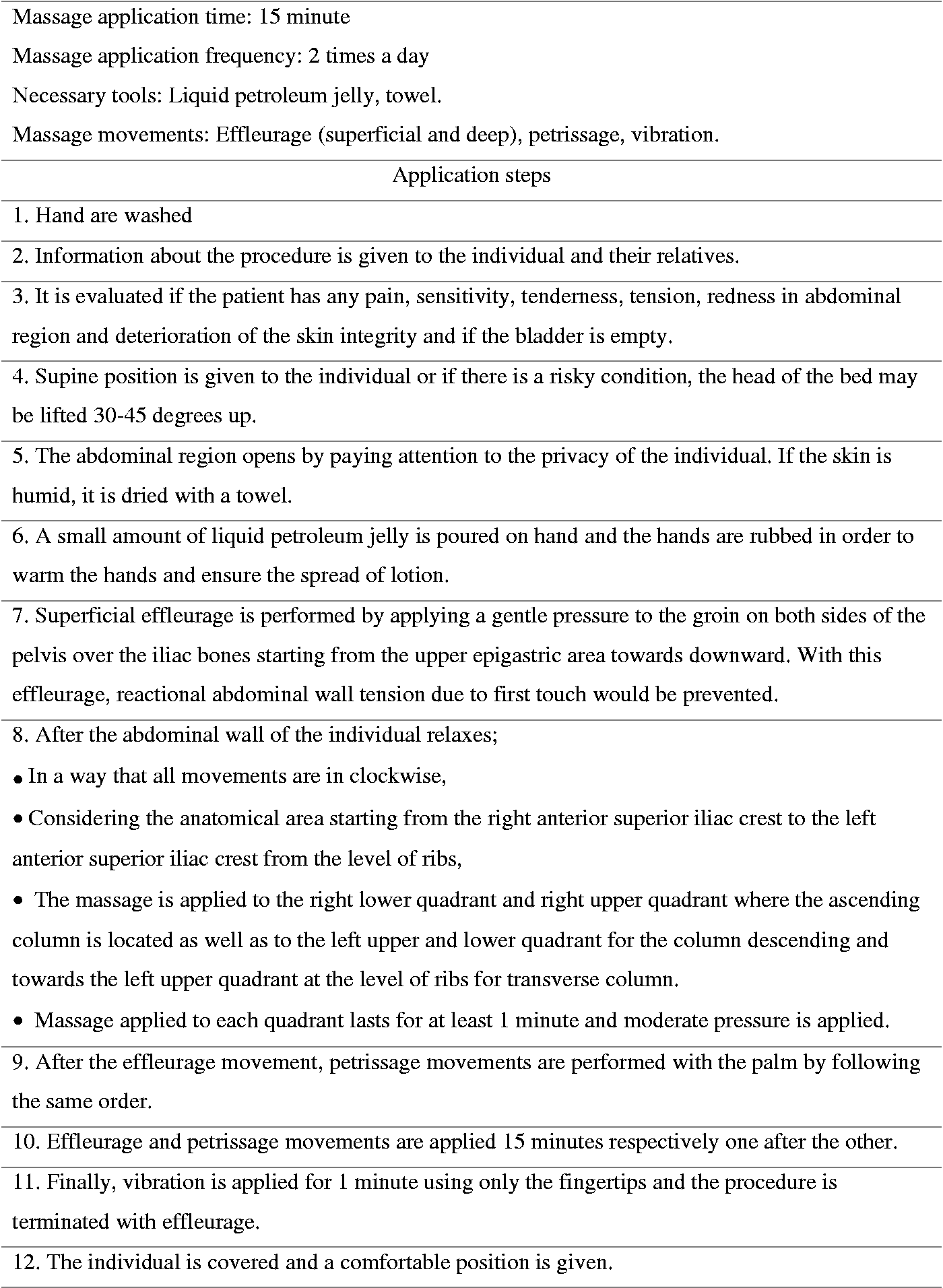
Abdominal Massage Instructions.
GRV Check
In the literature, it is stated that GRV should be checked every four hours (Dikmen & Yavuz, 2013; Gürkan & Gülseven, 2013; Uysal et al., 2011). Accordingly, in this study, GRV was checked every four hours using disposable gloves and 50 ml injectors based on the routine practice of the clinic. Upon the procedure, the amount was measured and recorded in the parameter questionnaire (Uysal et al., 2012). In this study, the presence of gastric content which was greater than 200 ml was accepted as “GRV present” since a high threshold value of GRV is not clearly stated in the literature (Tekin et al., 2019; Uysal et al., 2012) and a gastric content which is greater than 200 ml is considered as high GRV in the clinic. The nurses working in the clinic performed the GRV follow-up. During the follow-up, the nurses were blinded.
Abdominal Distension Check and Abdominal Circumference Measurement
Based on the literature information, abdominal distention check and abdominal circumference measurement were performed every four hours (Uysal et al., 2012). While the related values of the control group were evaluated 30 minutes after the feeding, the related values of the intervention group were evaluated 30 minutes after the feeding and following the massage treatments at 08:00-12:00-16:00-20:00-24:00 hours. Abdominal distention was examined by palpation. It was considered as “no distention” when there was no abdominal sensitivity, muscle stiffness or contraction in palpation and the abdomen was relaxed (McClurg et al., 2011). In addition, a nurse or doctor from the clinic supported the determination of whether there was distention. A 150-cm inflexible tape measurer was used to measure abdominal circumference. The measurement data were recorded in the parameter questionnaire.
Data Analysis
The Shapiro-Wilk test was used to check whether or not continuous variables were normally distributed. The data were compared using Student’s t-test or Mann-Whitney U test. The other tests used included the Chi-square test for determining the correlations between categorical variables such as defecation or distension, and the McNemar test, a non-parametric test, for comparing characteristics of dependent two categories such as first day GRV and last day GRV. The value of p < 0.05 was accepted as statistically significant.
Ethical Considerations
In order to conduct the study, approval was obtained from the Ethics Committee of Çukurova University in Turkey (03.03.2017- No. 62–22). The study was conducted in accordance with the Declaration of Helsinki. In addition, written permission was obtained from the institution where the study would be conducted. The healthcare professionals working in the clinic where the study was conducted were informed about the study. After the patients were informed about the purpose of the study and content of the questionnaire and parameter questionnaire, their written consents for participation were obtained.
Results
Descriptive Characteristics and Health History
The patient groups had similar descriptive characteristics and health history (Table 1).
Sociodemographic Characteristics and Health History Results of Patients.

aIndepented sample t test.
bChi square.
The mean age of the intervention group was 78.6 ± 7.3 and 40% were male. In the control group, the mean age was 77.1 ± 7.5 and 56.7% were male. Most of the patients in both groups had a history of at least one chronic disease but no history of gastrointestinal disorder. Most of them were hospitalized in the intensive care unit due to cerebrovascular disease (p > 0.05).
GRV, Distention, Vomiting, and Defecation of the Patients according to the Follow-Up Days
Up to the day 5, the groups had a similar incidence of high GRV, distension, and vomiting. On the fifth day, defecation was determined in 63.3% of the patients in the intervention group and in 30.0% of the patients in the control group (p < 0.05). On the sixth day, it was observed that none of the patients in the intervention group had GRV, distension or vomiting; whereas, 81.5% had defecation. In the control group, 18.5% of the patients had GRV, 29.6% had distension and 33.3% had defecation. Additionally, on the sixth day, a significant difference was determined between the groups in terms of GRV, distension and defecation (p < 0.05). In addition, the groups were similar regarding the incidence of vomiting throughout the follow-up days (Table 2).
Comparison of GRV, Distention, Vomiting and Defecation of Patients in Terms of Follow-Up Days.

Note. GRV = Gastric residual volume.
aChi square.
*p < 0.05.
Comparison of GRV, Distention, Vomiting, and Defecation of the Patients on the First and Sixth Days
On day 6, the number of patients reaching the target calories was 54. Therefore, 54 patients were evaluated to compare the groups in terms of the parameters of the first and sixth days (Table 3).
Comparison of GRV, Distention, Vomiting and Defecation of the Patients on the First and Sixth Days.

aMcNemar test.
*p < 0.05.
When the intervention and control groups were compared in terms of GRV, distension, vomiting, and defecation on the first and sixth days, no statistically significant difference was found between the groups in terms of GRV; however, there was a significant difference between them in terms of distension and defecation (p < 0.05) (Table 3).
Comparison of GRV and Abdominal Circumference Mean Values of the Patients according to the Follow-Up Days
It was found that there was no significant difference between the intervention and control groups in terms of the GRV amount and abdominal circumference on the fifth day (p > 0.05), but on the sixth day, there was no GRV in the intervention group and the mean abdominal circumference in the intervention group was lower compared to the control group (p < 0.05) (Table 4).
Comparison of GRV and Abdominal Circumference Mean Values of the Patients According to the Follow-Up Days.

Note. GRV = Gastric residual volume.
aMann Whitney U test.
bIndepented sample t test.*p < 0.05.
Discussion
This study was conducted to assess the effect of abdominal massage on GRV, defecation, distention, and vomiting in geriatric patients receiving treatment in the intensive care unit. The constipation and abdominal distention frequency significantly decreased and the defecation frequency significantly increased in the intervention group in comparison with those of the control group. It was determined that GRV was not observed in the intervention group while it increased in the control group. Vomiting was observed in one patient in the intervention group; whereas, the patients in the control group had no vomiting. The results showed that the massage reduced high GRV and had a positive effect on defecation and distention. However, it did not have a positive effect on vomiting.
Many studies have revealed that abdominal massage reduced GRV (Kahraman & Özdemir, 2015; Momenfar et al., 2018; Tekgündüz et al., 2014; Uysal, 2017; Uysal et al., 2012). In contrast to the results of the present study, Dehghan et al. (2018) study showed that the mean gastric residual volume in the abdominal massage group which was 20 ml before the study significantly decreased to 11 ml at the end of the third day of the study. In the control group, the mean gastric residual volume which was 13 ml before the study significantly increased to 34 ml at the end of the third day of the study. However, it was stated that there was no significant difference between the groups and this result could be associated with the fact that abdominal massage application and patient follow-up lasted for only three days. As these studies have been conducted with different patient groups, it is seen that there is a need for studies evaluating the effect of abdominal massage on GRV, especially in geriatric patients. This need is supported by the fact that, upon the literature review, we have encountered no study investigating the effect of abdominal massage on GRV in geriatric patients. Thus, the present study is thought to be an original study conducted with the geriatric patient group.
In this study, it was determined that abdominal massage increased the frequency of defecation and prevented constipation. The study conducted by Okuyan and Bilgili (2019) with elderly people showed that when the post-test constipation status of individuals in the massage and control groups were compared, the constipation status of the massage group decreased with a significant difference between the groups. Similarly, the study conducted by Çevik et al. (2018) with twenty-two elderly patients residing in rest homes showed that the mean scores for the number of defecation were 0.43, 0.57, and 0.76 before, during, and after the application, respectively. There was a statistically significant difference between pre-application and application days, application and post-application days, and pre- and post-application days (Çevik et al., 2018). The results of these studies are in line with the present study and confirm the results of the present study based on the effectiveness of abdominal massage on increasing the numbers of defecation and preventing constipation. Furthermore, different studies which did not include geriatric groups showed that abdominal massage increased the intestinal movements and the frequency of defecation (Ayaş et al., 2006; Dehghan et al., 2018) especially by reducing the severity of gastrointestinal symptoms such as constipation and abdominal pain syndrome (Lamas et al., 2009).
The results of the current study showed that the mean abdomen circumference in the control group on the first day and sixth day was 102.4 cm and 104 cm, respectively. The mean abdomen circumference in the intervention group on the first day and sixth day was 95.2 cm, 94.7 cm, respectively and there was a statistically significant difference between the two groups (p < 0.05). In addition, none of the patients in the intervention group had distension on the sixth day; whereas, 8 patients (29.6%) in the control group had distension on the sixth day and a statistically significant difference was determined (p < 0.05). Similar to the results of the present study, Kahraman and Özdemir (2015) showed that the difference between the means of the last and the first abdominal circumference was -2.1 for the intervention group and 5.3 for the control group. There was a statistically significant difference between the two groups. The results of Ayaş et al. (2006) study showed that in phase I, 11 (45.8%) of the 24 patients had abdominal distention. In phase II (massage group), three (12.5%) patients had abdominal distention and there was a significant difference between the two groups. Uysal et al. (2012) reported that patients in the control group developed more abdominal distension (25%) than those in the massage group (7.5%) and the difference was statistically significant. Similarly, Dehghan et al. (2018) reported that the difference of abdominal circumference before and after the study were -0.59 and 0.91 in massage and control group, respectively. The abdominal circumference significantly decreased after the study in the massage group while it significantly increased in the control group. There was a significant difference between the two groups. The study conducted by Uysal (2017) showed that abdominal distension developed in 6.0% of the intervention group patients and in 30% of control group patients, and the difference between the two groups was statistically significant. The present study and the aforementioned studies showed that abdominal massage had a positive effect on reducing abdominal circumference and preventing distension.
In the current study, vomiting was not found to be clinically significant in the massage group. Similarly, Uysal et al. (2012) reported that there was not a statistically significant difference between the massage and control groups in terms of vomiting. In contrast to the results of the present study, Tekgündüz et al. (2014) study showed that there was a difference in the frequency of vomiting of the infants in the massage group between the first day (2.14) and the last day (0.35). In addition, the study conducted by Uysal (2017) revealed that vomiting developed in 16.0% of the patients in the control group and in 2.0% of the patients in the intervention group, and the difference between them was found to be statistically significant. The reasons for the differences in the results of the present study with those of other studies can be due to low sample size (Tekgündüz et al., 2014) or the type of society under study (neonates and patients under sixty-five years) (Tekgündüz et al., 2014; Uysal, 2017). Another possible reason for this difference can be the frequency of massage (five days) (Uysal, 2017).
The literature and the findings obtained in this study show that abdominal massage is an economical non-pharmacological practice with no side effects and which can be easily applied by nurses.
Limitations of the Study
The important limitation of this study is that the study evaluated the effectiveness of abdominal massage only in patients over the age of 65 years; thus, the results cannot be generalized to other age groups. In addition, another limitation is that the study was a non-randomized trial.
Conclusion
In the current study, it was determined that abdominal massage decreased GRV and distension while it increased the frequency of defecations, and had no effect on vomiting in enterally fed geriatric patients. Also, the abdominal massage was observed to have no side effect. Accordingly, it is suggested that randomized controlled and double blind studies be conducted examining the effect of abdominal massage on GRV, distension, frequency of defecations and vomiting especially in enterally fed geriatric patient groups. Furthermore, it is recommended that abdominal massage be performed by intensive care nurses on geriatric patients.
Footnotes
Acknowledgments
We would like to thank all the patients who agreed to participate in the study. All authors have contributed significantly, and that all authors are in agreement with the content of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.