
Abstract
Introduction
Hemodialysis often leads to complications related to the arteriovenous fistula (AVF), the primary vascular access for dialysis. AVF complications, such as thrombosis and infection, are common and can disrupt treatment, increase morbidity, and diminish patients’ quality of life. Effective self-care and management of AVF are essential to minimize these risks, but many patients lack adequate knowledge and skills to perform necessary self-care practices.
Objective
To evaluate a fistula self-care bundle's effect on hemodialysis patients’ complications
Methods
Quasi-experimental design (study/control) study was conducted in the dialysis unit at Assiut University Hospital. Sample: A purposeful sample of sixty adult patients with an AVF on regular hemodialysis was assigned equally into two groups. Study tools: tool I; an interview questionnaire sheet to assess demographic data, medical history, tool II; patient complications assessment sheet, tool III; and a scale of assessment of self-care behaviors with AVF in hemodialysis.
Findings
Following the intervention, the overall self-care behavior score increased significantly (p = .000; d = 1.79). Furthermore, specific behaviors such as washing the fistula arm, controlling fluid intake, and avoiding tight clothing showed significant improvements (p < .001). Importantly, there was a notable reduction in the frequency of complications such as infection, thrombosis, and steal syndrome in the study group post-intervention.
Conclusion
The findings demonstrated that the implementation of the fistula self-care bundle led to a significant reduction in vascular access complications among hemodialysis patients.
Introduction
Chronic kidney disease (CKD) was a significant global health issue that impacts over 750 million individuals worldwide (Crews et al., 2019). Approximately 2.62 million patients were undergoing renal replacement therapy (RRT), projected to double by 2030 (Luyckx et al., 2018). Among RRT modalities, hemodialysis (HD) is the most commonly utilized, effectively removing toxic metabolites and extending the lifespan of patients with end-stage renal disease (ESRD). Due to its efficacy and safety, an arteriovenous fistula (AVF) remains HD's preferred vascular access method (Askeroğlu et al., 2021; Mokhtari, 2020; National Kidney Foundation, n.d.).
In alignment with global trends, Egypt experienced a 36% increase in the burden of CKD between 2009 and 2019. During this period, CKD ranked as the fifth leading cause of death. As of 2019, the most recent estimates indicate a dialysis prevalence of 0.61 per 1,000 individuals and an incidence rate of 0.19 per 1,000 individuals (Bello et al., 2019; Center for Economic and Social Rights, 2021; University of Washington Center for Health Trends and Forecasts, 2021).
Patients with AVFs experienced fewer complications and reduced treatment costs than those utilizing other vascular access methods (Al-Balas et al., 2019; Shamasneh et al., 2020). The role of the vascular access coordinator is critical in enhancing AVF utilization rates, lowering central venous catheter use, and decreasing hospitalizations related to vascular access complications. Optimized vascular access management led by coordinators can substantially reduce AVF-related complications (Sousa et al., 2024; Dwyer et al., 2012). Additionally, patients must actively participate in their AVF care and improve their self-care practices to maintain the effectiveness of this vascular access (Casey et al., 2014; Saran et al., 2019).
In 2018, the United States Renal Data System (USRDS) reported that 63% of HD patients used AVF, 17.5% utilized arteriovenous grafts (AVGs), and 19.6% relied on catheters. The increase in AVF usage was primarily attributed to a decline in AVG use, while the reduction in catheter use was comparatively modest. Due to concerns regarding catheter-related morbidity, the “Fistula First, Catheter Last” initiative was introduced in 2014 to promote safer and more effective vascular access (Franco, 2021; Saran et al., 2020).
AVF-related complications are an adverse outcome of medical intervention that may negatively impact prognosis among HD patients (Kouchoukos et al., 2013). These complications generally include worsening of the severity of the disease, the development of new signs or symptoms, or pathological changes that may become widespread throughout the body and affect other organ systems. Infection, thrombosis, and stenosis pose significant risks to HD patients, potentially leading to decreased quality of life and increased mortality (Mokhtari, 2020).
By implementing a self-care bundle, which includes practices such as patient education, hygiene maintenance, and regular monitoring, patients can become more adept at managing their AVF health. Evidence suggests that adherence to self-care practices can reduce the frequency of these complications, leading to improved clinical outcomes, enhanced patient well-being, and prolonged AVF functionality (Jin et al., 2021; Lee et al., 2022)
Additionally, complications related to AVFs often result in frequent hospitalizations and additional medical interventions, contributing to higher healthcare costs (Saran et al., 2019). Effective self-care bundles can decrease the incidence of these complications, thereby reducing the need for emergency treatments and hospital visits. This alleviates the financial burden on healthcare systems and reduces the overall cost of dialysis care (KDOQI, 2017).
The findings from this study could contribute to evidence-based guidelines and policies for managing AVF complications. As the healthcare landscape increasingly emphasizes patient-centered care and self-management, demonstrating the efficacy of self-care bundles aligns with contemporary approaches to chronic disease management. This research could inform policy changes and support integrating self-care practices into standard care protocols (Jin et al., 2021).
Review of Literature
Self-care is an individual's active engagement in maintaining health and well-being (Amin et al., 2024; The Center for Economic and Social Rights, 2021). According to Sousa, self-care behaviors encompass deliberate actions aimed at preserving health, including ensuring the functionality of the AVF in patients undergoing HD. Acquiring self-care competencies enables HD patients to identify when professional assistance is necessary for AVF-related issues, protect their fistulas, and minimize or avoid complications (University of Washington Center for Health Trends and Forecasts, 2021). Despite its importance, evidence suggests that the self-care behaviors of HD patients remain suboptimal. Studies by Sousa et al. (2014–2017) corroborate this, highlighting insufficient self-care practices among HD patients and underscoring the need for structured educational interventions to enhance AVF-related self-care behaviors.
In this respect, patient education is pivotal in promoting self-care, with nurses playing a critical role in this process. Written educational materials, such as booklets, are particularly effective among various educational approaches. These materials offer patients easy access to vital information, empowering them to internalize and implement self-care practices (Sousa et al., 2017). Existing literature includes multiple training programs addressing diverse aspects of HD care, such as fluid management, dietary modifications, and psychosocial issues like insomnia, fatigue, pain, and anxiety (Sousa et al., 2014, 2015). However, there is a notable scarcity of studies focusing exclusively on AVF care education.
Regarding literature, the results of a review conducted by Pessoa et al. (2020) identified essential care practices for maintaining arteriovenous fistula (AVF) functionality, which were categorized into three key areas. First, they highlighted actions that should be avoided to preserve the AVF, such as checking blood pressure, performing punctures, sleeping on the arm, carrying excessive weight, and consuming too many fluids. Next, they identified actions for preventing and monitoring AVF complications, including monitoring for steal syndrome and observing for issues such as hemorrhage, thrombosis, and infections. Additionally, they discussed measures for preventing infections and treating hematomas. In addition to the practices for preserving the vascular network, and performing fistula arm exercises both before and after vascular access. Also covered in this category were guidelines for caring for the surgical dressing.
In their prospective and observational study, Sousa, Marujo, et al. (2020), Sousa, Paquete, et al. (2020) emphasized the importance of educating and training patients with ESRD to manage their AVF care. The goal of this education was to foster the development of effective self-care behaviors related to vascular access. The research was designed to identify clinically significant self-care behavior profiles among HD patients. By identifying these profiles, healthcare providers can tailor educational programs to better align with the specific characteristics of each patient, thereby enhancing the effectiveness of self-care strategies.
Previous research has provided guidance on best practices for AVF bundles. Staaf et al. (2021) conducted a cohort study and found that the buttonhole shallow (BHs) technique was the most commonly used cannulation method, applied in 55% of AVFs during their functional patency. Other techniques, such as buttonhole blunt (BHb), rope ladder (RL), and area puncture (AP), were used less frequently, 29%, 13%, and 3%, respectively. The study revealed that BHb was associated with the lowest risk of complications, including a significantly lower incidence of stenosis, infiltration, and cannulation difficulties compared to RL and BHs. Cannulation difficulties were notably more common with the AP technique. Importantly, the buttonhole technique did not show a significant increase in infection rates. The authors concluded that in dialysis units with low infection rates, the buttonhole technique remains a viable option due to its overall lower complication risk.
In addition, Costa Pessoa et al. (2020) emphasized the importance of self-care actions in maintaining AVF functionality. Their findings suggest that such actions are critical for guiding nursing care policies and protocols aimed at preventing complications. However, they also highlighted the need for further high-quality studies to better identify effective self-care practices and the factors influencing their implementation.
Research Gap and Significance of the Research
While prior research has identified the inadequate self-care practices of HD patients, few studies have systematically evaluated interventions tailored to AVF care. The proposed intervention bridges this gap by introducing a novel self-care bundle to reduce AVF complications.
The findings of this study have significant implications for clinical practice and health policy, particularly in nephrology. By enhancing patient education and self-care behaviors, the intervention can improve patient outcomes, reduce healthcare costs associated with AVF complications, and inform self-care protocols at a systemic level. In Egypt, where HD prevalence remains high and access to specialized care is often limited (The Center for Economic and Social Rights, 2021; University of Washington Center for Health Trends and Forecasts, 2021), this intervention could serve as a model for resource-limited settings. Global data also highlight the urgent need for improved HD care, as nearly 4 million individuals worldwide require regular dialysis, with significant disparities in care quality across regions (Bello et al., 2019).
This study explicitly measured the bundle's effectiveness in improving patient outcomes using validated tools for self-care assessment, AVF functionality, and complication rates.
Operational Definitions
The Study
Research Hypotheses
Method
Research Design
This study employed a quasi-experimental one-group pretest–posttest design to evaluate the effectiveness of a fistula self-care bundle on reducing complications among HD patients. The design involved assessing patients’ self-care behaviors and the incidence of AVF.
Study Variable
The independent variable was the self-care bundle for AVF, while the dependent variable was the incidence of complications experienced by patients. Therefore, the design is most appropriate for evaluating a self-care bundle's effect on HD patients’ complications.
Setting
The study was conducted at the dialysis unit of Assiut Hospital, which was chosen for its status as a major referral center serving Assiut governorate. This unit is located on the ground floor of the Assiut hospital. This unit consists of two halls, each divided into four sectors containing 10 HD machines.
Sample
A purposive sample of 60 patients undergoing regular HD was recruited. The sample was randomly and alternately divided into two equal groups: 30 patients in the study group and 30 in the control group.
Group I (study group): Received the self-care bundle and routine hospital care.
Group II (control group): Received only routine hospital care.
Routine hospital care included checking the patient's vital signs, engaging in conversations to assess their condition, measuring weight, conducting necessary investigations, and providing care before, during, and after medical procedures.
Randomization Technique
After reviewing the frequency schedule for patients undergoing HD throughout the week from Saturday to Thursday, patients in the morning period were assigned to the study group, and patients in the evening period were assigned to a control group. Thus, the study group received the self-care bundle throughout the study period, while the control group received routine care in the hospital.
Inclusion criteria:
Age between 20 and 65 years. Presence of (AVF) and undergoing regular HD. No significant memory problems. Medically stable.
Exclusion criteria:
Patients with dual vascular access (both a central venous catheter and an AVF). Patients who declined to participate.
The sample size formula used the following equation to select the 60 HD patients (Steven & Thompson, 2012). At Assiut University Hospitals, N is the total number of patients (120) receiving regular HD. One hundred twenty HD patients participated in the sessions. Z confidence levels are 0.95 and 1.96, respectively. Neutral is 0.50, P is the property availability ratio, and D is the error ratio of 0.05.
Tools
To achieve the study's objectives, three tools were used for data collection:
The original tool (2015) was developed to verify the lack of tools to evaluate self-care behaviors with AVF performed by patients. The ASBHD-AVF scale has undergone cross-cultural validation and psychometric evaluation in several countries, confirming its reliability and applicability across diverse healthcare settings. These include Türkiye (İkiz et al., 2021), Brazil (Lira et al., 2021), Morocco (Loubna et al., 2025), Iran (Sharif-Nia et al., 2024), and China (Yang et al., 2019). These validations confirm the scale's adaptability and robustness across various cultural contexts, enhancing its utility for international research and clinical practice in nephrology nursing.
This is a scale composed of two subscales: management of signs and symptoms and prevention of complications. The first subscale consists of six items with a Cronbach's alpha value of .797, and the second subscale consists of 10 items with a Cronbach's alpha value of .722. The ASBHD-AVF revealed properties that allow its use to assess the self-care behaviors of patients on HD in the maintenance and upkeep of the AVF. Then classified into two categories: inadequate self-care < 60% and adequate self-care > 60%. Higher scores indicate better self-care for AVF access.
This scale comprises 16 items as the following consequence (I address the nurse if the hand of the fistula arm start to hurt, I address nurses if the hand of the fistula arm appear with wounds, I address the nurse when I get a headache and chest during HD, I address the nurse when I have cramps during HD, I do compression at home at puncture site if bleeding occurs, I protect the fistula arm from bumps and shocks, I check every day if the hand of the fistula arm cools, I feel the thrill at the site of the fistula twice a day, I immediately go to hospital or a clinic if fistula has not thrill, I check every day if the color of the hand from the fistula arm changes, I do compression of puncture sites with the fingers (hemostasis), I allow blood sampling in the fistula arm*), I apply ointment when hematoma occurs, I protect the fistula arm from scratches, cuts and wounds, I observe signs of redness and swelling at the puncture sites, I avoid getting into places with different temperatures.
Tools Validity and Reliability
To ensure the validity of the data collection tools, a content validity evaluation was conducted with a panel of five experts, including one medical staff member from the dialysis unit and four nursing staff specializing in medical-surgical nursing. These experts, comprising professors and assistant professors from the faculties of nursing and medicine, assessed the tools for relevance, clarity, applicability, and completeness.
The content validity index (CVI) for Tool II (Patient Complications Assessment Sheet) was 0.94, indicating excellent validity, based on the experts’ feedback, minor modifications were made, including rephrasing certain items for clarity and rearranging items for better logical flow, ensuring the tools were tailored to the study's objectives and user-friendly for participants.
The reliability of the ASBHD-AVF scale was demonstrated with a Cronbach's α of .920, indicating high internal consistency for measuring self-care behaviors related to AVF.
Pilot Study
A pilot study was conducted with 10% of the study population, involving six patients from the dialysis unit, to evaluate the feasibility, clarity, and applicability of the tools and estimate the time required for data collection. The results indicated that the tools were clear, straightforward, and easy to complete. Tool II required 5–7 min to complete, while Tool III required 15–20 min on average. Participants or the research team reported no significant issues or ambiguities. The pilot study confirmed the appropriateness of the tools for assessing patient complications and self-care behaviors related to AVF. As no modifications were necessary, the data from the pilot study were included in the primary study analysis. These findings enhance the credibility and rigor of the tools used in this study.
Ethical Considerations
Approval for the research was obtained from the ethical committee of the Faculty of Nursing, Assiut University, with an Institutional Review Protocol (IRP) ethical code No. 1120230550 on January 29, 2023. The head of the dialysis unit granted formal permission at Assiut University Hospital and the Dean of the Faculty of Nursing before both the pilot study and the main study commenced. The researchers clearly explained the study's aim and purpose to the participants. Confidentiality was maintained using patient codes instead of names. Participants were informed of their right to decline participation or withdraw from the study at any time without consequence. Written informed consent was obtained from all participants. The study was designed to ensure no harm to the patients, and privacy during data collection was rigorously upheld.
Fieldwork Description
Data collection took place at the dialysis unit of Assiut University Hospital over 10 months, from March 2023 to December 2023, during both morning and afternoon shifts.
Procedure
The study was conducted in the following phases:
Assessment Phase
Plan of data collection: Only one researcher collected the data in this study.
The researcher's intervention in the control group: At the beginning, the researcher who collected the data in this study introduced herself to initiate a line of communication, explained the nature and purpose of the study, and filled out the tool's parts for the control group.
The researcher met with eligible patients from the study group. Each patient was informed about the purpose and nature of the study, and written consent was obtained. Data was collected through participant interviews; baseline data, including demographic and medical information, were collected using Tool (I). Self-care behaviors were assessed using Tool II. The study tool-filling process took ∼15–20 min, depending on each patient's responses.
Planning Phase
The researchers developed the self-care bundle based on assessing the study subjects and an extensive review of relevant literature. The bundle included various instructional materials and media, such as photos, videos, handouts, and PowerPoint presentations. The researchers prepared a designated training area and organized a teaching schedule aligned with the content of the educational booklet and the patients’ availability.
Implementation Phase
During the implementation phase, the researcher conducted interviews with each patient. Patients in the study group received the self-care bundle, which included illustrated images created by the researchers and standard hospital instructions. Patients in the control group received only the standard hospital instructions without the additional self-care bundle.
Self-Care Bundle
The researchers developed the fistula self-care bundle based on a thorough literature review (Bayoumi & Khonji, 2020; Ramezani et al., 2019; Sousa, Marujo, et al., 2020; Sousa, Paquete, et al., 2020). It was created in simplified Arabic and supported by photo illustrations to enhance understanding.
Patients in the study group received a single training session and the initial assessment interview. During this session, the researchers highlighted the objectives of the self-care bundle and its relevance to improving patient outcomes, including self-care and reduction in complications.
The Theoretical Framework of the HD Self-Care Bundle
Bundle is one of the first theories utilized in healthcare from the behavioral sciences to explain human behavior and the influences that assist in modifying unwanted behavior. In the scope of this study, the bundle included detailed instructions on managing an AVF and preventing complications. Key components of the bundle were:
Hygiene and monitoring: The emphasis was on keeping the fistula clean, monitoring for signs of redness, swelling, or pain, and promptly notifying a healthcare provider if any issues arise. Pretreatment care: Patients were instructed to wash and dry the fistula arm thoroughly before each treatment, avoid applying excessive pressure to reduce the risk of blood clots, and refrain from wearing tight clothing or jewelry that could restrict blood flow. Daily care: Using the nonfistula arm for blood pressure measurements is recommended, as avoiding resting the head on the fistula while sitting or sleeping, and checking blood flow through the AVF daily.
For managing symptoms, the bundle advised:
Emergency symptoms: Contact a nurse if experiencing cramps, headaches, or chest pain during HD. Fistula care: Reporting any pain in the fistula arm, controlling fluid intake at home, applying ointment or ice to hematomas, and monitoring the hand of the fistula arm for changes in temperature or signs of redness and swelling at puncture sites.
At the end of the session, patients were provided with a colored hard booklet in plain Arabic to help them assimilate and retain the information. Before discharge, patients were instructed to continue the self-care practices initiated in the hospital once they returned home.
Phase III: Evaluation Phase
In this phase, patient evaluations were conducted three months after the initial intervention. Researchers collected patients’ phone numbers or those of their relatives during the first interview to facilitate follow-up. Phone calls were made to assess patient adherence to the self-care bundle. Patient evaluations utilized Tool (II) and Tool (III).
Statistical Design
Data analysis was performed using the Statistical Package for Social Sciences (SPSS) Version 26 (IBM Corp., Armonk, NY, USA), following the guidelines outlined by Altman and Bland (1994). Normality of continuous variables was evaluated using both the Shapiro-Wilk and Kolmogorov-Smirnov tests, accompanied by visual assessments through histograms and Q-Q plots to ensure the appropriate choice of parametric or nonparametric tests. Categorical variables were summarized using frequencies and percentages, while continuous variables were described by means and standard deviations.
To compare categorical variables, chi-square tests were employed. In cases where the assumptions of chi-square were violated (i.e., when expected frequencies were < 5 in ≥ 20% of cells), Fisher's exact test was used to enhance accuracy. Additionally, effect sizes were calculated to better interpret the practical significance of results: Cramér's V was used for chi-square tests, with interpretation thresholds defined as small (0.1), medium (0.3), and large (0.5). For continuous variables analyzed using t-tests, Cohen's d was reported to assess effect size, with thresholds of small (0.2), medium (0.5), and large (0.8). A p-value of < .05 was considered statistically significant throughout all analyses.
Results
The age distribution across both groups is relatively balanced (X² = 1.41, p = .704), with most participants in the 50–60 years range, the mean ages for the study and control groups are 46.57 ± 15.73 and 48.70 ± 14.58 years, respectively, with a combined mean of 47.63 ± 15.08 years (p = .588). The sex distribution is evenly matched, with 53.3% male and 46.7% female participants in both groups (p = 1.000), eliminating potential bias based on gender. Marital status is also identical, with 80% married and 20% single in each group (p = 1.000), indicating that social support dynamics are comparable. Educational levels are varied but show no statistically significant differences (X² = 0.83, p = .842), with many participants having intermediate education, potentially influencing their understanding of self-care instructions. Regarding occupation, most participants are non-working (60% in the study group and 66.7% in the control group, p = .864). Residence is also varied, but the two groups have no significant differences (X² = 0.075, p = .784).
The demographic characteristics of the study and control groups, as presented in Table 1, showed no significant differences, ensuring comparability and reducing the potential for confounding variables.
Frequency and Percentage Distribution of Demographic Data for Studied Patients (n = 60).

The chi-square test for qualitative data between the two groups.
Independent t-test of quantitative data between the two groups.
* p < .05. ** p < .01.
Table 2 presents the frequency and percentage distribution of medical data for the studied patients, comparing the study and control groups. The data indicated that the etiology of ESRD was fairly distributed between the two groups, with no significant differences in the prevalence of hypertension (HTN) only, diabetes mellitus (DM) only, hypertension and diabetes (HTN and DM), glomerulonephritis, or HTN, and polycystic kidney disease (X² = 2.80, p = .592). Regarding dialysis duration, both groups showed comparable distributions, with no significant difference in the time patients had been on dialysis (X² = 0.578, p = .749). The duration of using the present AVF also showed no significant differences between the groups (X² = 1.08, p = .581).
Frequency and Percentage Distribution of Medical Data for Studied Patients (n = 60).

Abbreviations: ESRD = end-stage renal disease; HTN = hypertension; DM = diabetic mellitus; AVF = arteriovenous fistula.
* p < .05. ** p < .01.
The data presented in Table 3 compared the self-care behaviors of patients with AVFs in HD between the study and control groups. The analysis showed no significant differences between the two groups for most self-care activities, such as washing the fistula arm, addressing nurses during complications, performing compression at puncture sites, and protecting the fistula arm from injury. The p-values for these activities exceeded .05, indicating similar engagement in these behaviors across both groups. For example, items such as “I addressed the nurse when I had cramps during hemodialysis” (p = .132) and “I performed compression of puncture sites with my fingers” (p = .066) showed no statistically significant differences, despite slight variations in mean scores.
Comparison Between Study and Control Group Before Self-Care Bundles With Arteriovenous Fistula in Hemodialysis (n = 60).

Independent t-test of quantitative data between the two groups.
* p < .05. ** p < .01.
Table 4 compares self-care behaviors before and after the self-care bundle intervention for patients with AVFs in HD (n = 60). There were significant improvements in several behaviors, with the most notable changes observed in practices related to fistula care and fluid intake control. For example, washing the fistula arm before entering the HD room increased substantially in adherence, from 1.53 ± 0.73 preintervention to 2.57 ± 0.68 postintervention (p = .000). Similarly, controlling fluid intake at home improved significantly, from 1.63 ± 0.81 to 2.4 ± 0.77 (p = .000).
Comparison Between Pre- and Postself-Care Bundles With Arteriovenous Fistula in Hemodialysis for Study Group (n = 60).

Independent t-test of quantitative data between the two groups.
* p < .05. ** p < .01.
Table 5 compares self-care behaviors between the study and control groups before the educational intervention. Both groups demonstrated inadequate self-care, with 100% of participants in each group scoring below 60% on the self-care behaviors scale. The mean scores for the study group (71.4 ± 3.94) and the control group (71.97 ± 3.86) were very similar, with no significant difference observed (p = .576).
Comparison Between Study and Control Group-Related Self-Care Behaviors With Arteriovenous Fistula in Hemodialysis (ASBHD-AVF) Before Education (n = 60).

Independent t-test of quantitative data between the two groups.
The chi-square test for qualitative data between the two groups.
* p < .05. ** p < .01.
Table 6 illustrates a dramatic improvement in the study group following the educational intervention. Initially, all 30 participants (100%) in the study group demonstrated inadequate self-care. However, after the intervention, 53.3% of participants improved to the level of adequate self-care behaviors, with a statistically significant shift observed in the chi-square test (p < .001). The total mean score for self-care behaviors in the study group increased significantly from 71.4 ± 3.94 to 87.43 ± 10.76 (p < .001.
Comparison Between Study Group Patients Pre- and Posteducation Related Self-Care Behaviors Among Hemodialysis Patients With Arteriovenous Fistula (n = 30).

Independent t-test of quantitative data between the two groups.
The chi-square test for qualitative data between the two groups.
* p < .05. ** p < .01.
Table 7 compares the complications associated with AVF between the study and control groups among HD patients. The findings revealed a significant reduction in thrombosis (clotting) within the study group, with only 6.7% of patients affected compared to 30% in the control group (X² = 5.46, p = .020). However, no statistically significant differences were observed in the occurrence of other AVF-related complications. For example, stenosis (narrowing) occurred in 3.3% of patients in the control group, while no cases were reported in the study group (X² = 1.02, p = .313). Both groups recorded a single case of ischemic neuropathy (acute arterial occlusion), with no significant difference (X² = 0.00, p = 1.000). The incidence of steal syndrome was slightly higher in the control group (6.7%) compared to the study group (3.3%), but the difference was not significant (X² = 0.35, p = .554). Additionally, no cases of aneurysm or bleeding complications were reported in either group. Catheter-related infection occurred in 3.3% of the study group and 6.7% of the control group, yet this difference also lacked statistical significance (X² = 0.35, p = .554).
Comparison Between Study and Control Group Related Complications of Arteriovenous Fistula Among Hemodialysis Patients (n = 60).
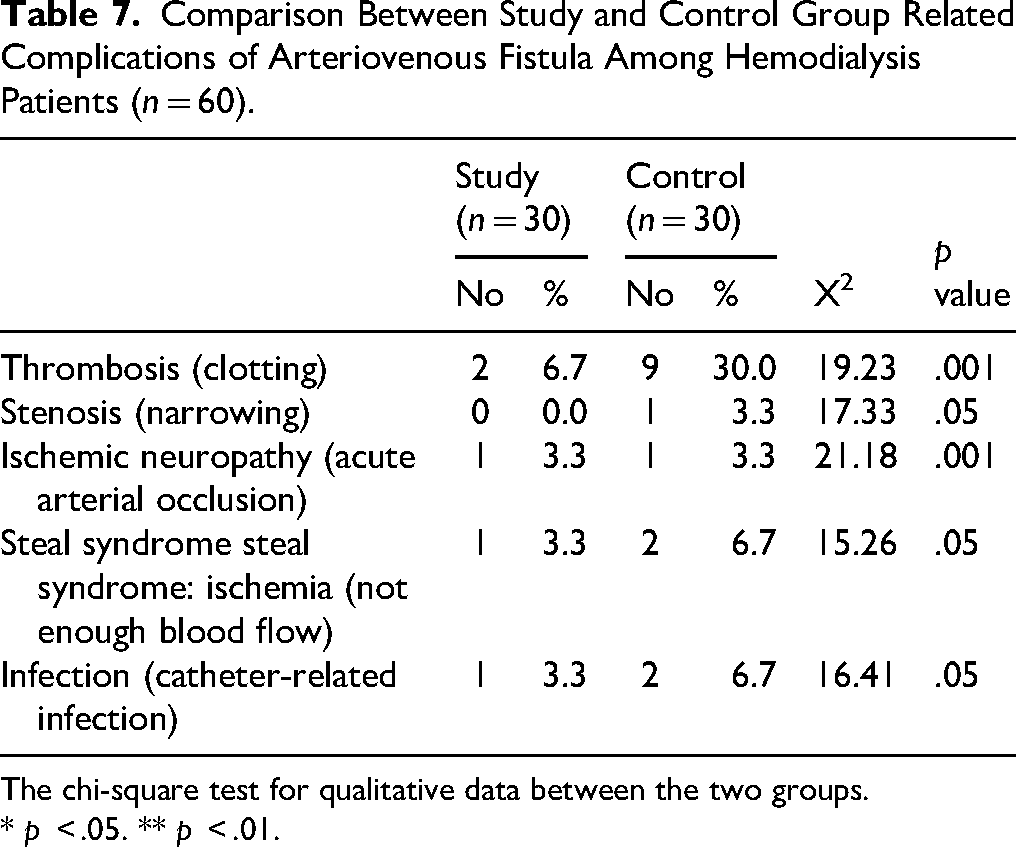
The chi-square test for qualitative data between the two groups.
* p < .05. ** p < .01.
Discussion:
As regards the comparison between the study and control group before self-care bundles with AVF in HD, the present study verified that no statistically significant difference between the study and control group before self-care bundles with AVF in HD, as regards most of the items’ scale.
Effective educational interventions have improved self-care behaviors in patients with chronic conditions, including those undergoing HD (Gillespie et al., 2017; Shukri et al., 2019). The baseline data from this study aligns with findings that suggest a common need for education among patients with inadequate self-care practices.
The overall similarity in self-care behavior scores in the preintervention phase in both groups suggests that any significant changes postintervention can be attributed to the Fistula self-care behavior education provided rather than differences in preexisting behavior. Research has shown that educational interventions can effectively enhance self-care behaviors in HD patients (Hsieh et al., 2020; Mikail, 2020).
Furthermore, the study mentioned that a statistically significant difference between pre and post fistula self-care bundle's application for study group p value < .05 as regarding 16 items of scale (wash the fistula arm with soap and water before entering the HD room, control the amount of fluid I drink at home and apply ointment when hematoma occurs, and so on. This agrees with (Rizki et al., 2021), who clarify that adherence to self-care is essential because it dramatically influences the management of complications, controlling symptoms among HD patients.
In addition, Esra, Vural Dogru, and Gun (2021) mentioned in their study that the participants’ knowledge of fistula and self-care behavior scores were found to be at a reasonable level postfistula care application. As the scale scores of patients with aneurysm and infection complications were lower, it can be considered that fistula self-care behavior plays a part in developing complications. Accordingly, it is recommended that patients should be supported with education programs about fistula complications.
From the researcher's point of view, improved fistula self-care behaviors of patients contribute to the healthy functioning of the AVF and minimize complications.
Educational interventions have been demonstrated to improve self-care behaviors in chronic disease management, including in HD patients (Al-Kandari et al., 2018; Higginbotham et al., 2016). The improvements observed in this study are consistent with the findings. The substantial increase in the proportion of patients demonstrating adequate self-care and the significant rise in the total self-care score strongly suggest that the educational program was highly effective. This aligns with the broader literature supporting the role of educational interventions in improving self-care in chronic disease management (Atta et al., 2025; Milani et al., 2017; Nicolaisen et al., 2020).
The reduction in thrombosis is a positive outcome that underscores the importance of educational programs in managing AVFs. This result suggests that similar educational interventions could be beneficial in preventing thrombosis in other patient populations.
Berman and Mendez (2020) and Lee and Kim (2019) reported that thrombosis is a well-documented complication of AVFs in HD patients. It occurs when blood clots form within the fistula, leading to reduced blood flow and potential loss of fistula function. Studies have consistently highlighted thrombosis as a leading cause of AVF failure. For instance, a study by Schanzer and Gupta (2009) found that thrombosis is the most common complication requiring intervention in AVF patients, with an incidence rate that significantly impacts long-term fistula patency. Additionally, Pessoa et al. (2020) reported that thrombosis is often associated with poor self-care practices and suboptimal management of the AVF.
Infection is another significant complication, particularly regarding access points used for HD. If not managed promptly, it can lead to more severe conditions, including sepsis. According to Al-Jaishi et al. (2016), infections in AVFs are relatively common and are a substantial cause of morbidity. The increased risk of infection may be attributed to repeated cannulation and potential breaches in aseptic technique.
Steal syndrome occurs when blood is diverted away from the distal part of the limb due to high flow through the AVF, causing ischemia and potential tissue damage. Although less common than thrombosis and infection, steal syndrome is a critical complication that requires careful monitoring and management.
Ischemic neuropathy and stenosis were observed less frequently in the study. Ischemic neuropathy results from inadequate blood flow to the nerves and is often linked to severe or chronic complications of AVF (Amin et al., 2025; Yeh et al., 2019). Conversely, stenosis involves narrowing the blood vessel within or adjacent to the AVF, which can impede blood flow and complicate fistula function (Khan et al., 2020). Although these complications are less common, their management is crucial to maintaining AVF function and patient quality of life.
Limitations and Strengths
The study was not conducted as a randomized controlled trial (RCT), which limits the ability to establish causal relationships and introduces the potential for selection bias. Additionally, the small sample size of 60 participants may restrict the generalizability of the findings to more extensive and diverse populations. Another limitation is the short follow-up period, which did not allow for assessing the intervention's long-term sustainability or impact on complications over an extended timeframe. Despite these limitations, the study has several notable strengths. It employed a comprehensive fistula self-care bundle that addressed multiple aspects of care, including hygiene, monitoring, pre-treatment care, and emergency management, providing a holistic approach to AVF management.
Implications for Practice
Based on our results, the implementation of the fistula self-care bundle significantly reduced vascular access complications among HD patients, indicating that structured, patient-centered self-care interventions are both feasible and effective in routine clinical practice. These findings emphasize the importance of integrating self-care education into dialysis care protocols to enhance vascular access outcomes. Further research should explore the underlying factors that influence adherence to AVF self-care behaviors, such as patient knowledge, motivation, and support systems. Additionally, conducting studies in different geographic regions and across dialysis centers of varying capacities is essential to validate and generalize the effectiveness of the intervention and ensure its adaptability across diverse clinical contexts.
Conclusion
The findings demonstrate that the implementation of the fistula self-care bundle led to a significant reduction in vascular access complications among HD patients, underscoring its effectiveness and the critical role of structured self-care interventions in improving patient outcomes.
Footnotes
Acknowledgments
This study is supported by funding from Prince Sattam bin Abdulaziz University's project number (PSAU/2025/R/1447).
Ethical Approval
The research was approved by the ethical committee of the Faculty of Nursing, Assiut University, Egypt, with an Institutional Review Protocol (IRP) ethical code No. 1120230550 on January 29, 2023.
Authors’ Contributions
MNAE, HAA, SAA, and MHRA: find the research problem, data collection, and methodology, and write and edit the first draft.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.