
Abstract
Introduction
The meaning in life (ML) is a significant predictor of the physical and mental health of patients with chronic diseases, and its construct is culturally specific.As a group between normal people and the patients with advanced cancer, patients with End-Stage Kidney Disease (ESKD) who are undergoing hemodialysis (HD) are often outside of research focus on ML.
Objectives
This study was to investigate the status of ML of patients on HD in Macau of China and to analyze the influence of social-demographic characteristics and disease-related factors on their ML. The study findings would inform the development of evidence-based interventions in nursing care for this patient population.
Methods
This study employed a cross-sectional survey design. Eligible participants were recruited by convenient sampling from the largest HD center in Macau in January 2020. The participants’ social-demographic and disease-related characteristics were collected, and their ML status was assessed by the Meaning in Life Scale for Hemodialysis Patients (MLSHP). SPSS 22.0 software was used to analyze the data.
Results
Questionnaires were distributed to 249 potential participants who were patients on HD, and 238 patients replied to the questionnaires effectively. The effective response rate was 95.58% (238/249). The average score of ML for the patients was 93.75 ± 10.00, which was 72% of the total score of 130 on the ML scale. Gender, religious belief, duration of dialysis treatment, and symptom-related distress had impacts on ML levels (p < .05), with religious belief being a particularly strong predictor (p < .001).
Conclusion
The level of ML for patients on HD in Macau is relatively high. Different demographic or disease-related factors impact participants’ ML, supporting or contradicting previous studies. While the study findings are meaningful under the local cultural contexts, they have implications for nurses in other places to develop evidence-based interventions for patients on HD.
Introduction
The meaning in life (ML) is the perceived life goal and significance of an individual's existence, and is affected by the moral conviction of society. While ML is cultivated in people's lifetime, it is dynamic, differing in various times and places that people live. ML is an important predictor of patients’ physiological and mental health with chronic diseases (Czekierda et al., 2017; Dezutter et al., 2015). A meta-analysis found that a positive attitude toward life can dramatically improve people's quality of life (QoL) and minimize their psychological stress, especially in their transitional period of life or in conditions of suffering chronic or life-threatening diseases (Vos & Vitali, 2018).
End-Stage Kidney Disease (ESKD) is an irreversible chronic disease, with increasing cases each year. According to the 2018 annual report of the United States Renal Data System (USRDS), ESKD cases increase at an average rate of 2% to 4% annually in nearly 30% of the countries worldwide (USRDS, 2018). Kidney replacement treatments, such as peritoneal dialysis, HD and kidney transplantation, are relatively effective for patients with ESKD, with HD accounting for the major replacement therapy mode. In China, there were 578,000 dialysis patients in 2016, and 26,039 candidates on the kidney transplant waiting list. Among the patients on dialysis, 91.94% were on HD (Zhang et al., 2020). Therefore, focus should be placed on patients on HD when we are studying the health and wellbeing of patients with ESKD.
Review of Literature
Previous studies have reported the impacts of HD on the life of ESKD patients. However, most of the studies focused on the impacts on QoL of the patients (Dąbrowska-Bender et al., 2018; Gomes Neto et al., 2018; Joshi et al., 2017). Some of the studies explored the relationships between the patients’ QoL and their levels of ML (Hajibabaei et al., 2020; Liu et al., 2021). Despite the confirmed relationships between ML and QoL of patients with chronic conditions, few studies have exclusively examined the ML status of the patients with ESKD, leaving a knowledge gap for future research exploration.
Studies on chronic diseases have found that patients’ ML levels are associated with their social-demographic and disease-related factors. However, there are no consistent findings about the impacts of the specific factors. For example, some studies found that age, gender, or marital status were the major determinants of the patients’ ML levels (Khurshid et al., 2018; Wang et al., 2016), while others found no association between patients’ ML levels and their demographic backgrounds (Liu et al., 2019; Saeedi et al., 2019). Since ML is culturally constructed, more local studies are needed to provide insights into context-related influencing factors. Such knowledge will contribute to a broad picture of ML construction and the influencing factors among patients with chronic diseases, including ESKD, for the health professionals in different places.
This study was conducted in Macau Special Administrative Region (SAR), China, a city with unique social-economic features. Macau is an advanced economy with approximately 86,000 USD GDP per capita in 2019, making it among the world's highest GDP per capita regions (The World Bank, 2019). People in Macau enjoy a comprehensive social welfare system, including low payment subsidiaries, financial support for the impaired or disabled, social housing or public housing schemes for low-income families, etc.
Macau has witnessed a steady increase in the number of patients on HD in the past decade. The number of patients who underwent HD increased by 4.9% in 2019 over the previous year, another upward trend for the last ten consecutive years (Statistics and Census Service of Macao SAR, 2019a). While the welfare system ensures that the Macanese citizens live a decent life in most circumstances, how have the social-economic conditions and personal factors of the local patients on HD affected their ML status?
Research Objectives
This study aims to investigate the ML levels of patients in Macau who suffer from ESKD and are undergoing HD as a treatment for their disease. It will also identify the associations between the patients’ ML levels and their demographic characteristics and disease-related factors.
Methods
Design
This study employs a descriptive cross-sectional survey design. Questionnaires were used to assess the ML levels of the patients on HD.
Participants
There were approximately 750 patients on HD in Macau in December 2018. They had their HD treatment in one of the three HD centers in three respective local hospitals. The treatment was free of charge and patients could freely choose one of the three centers. Therefore, the demographic and disease-related characteristics of the patients in one center might not be different from those in another center. Out of the 750 patients, about 550 (73%) had treatment at the HD center in the largest private hospital in Macau because of more places available there. In addition, the primary researcher (Y.L.) was a nurse in the largest center and the researchers could relatively easily gain access to the patients in the center to conduct the study. Therefore, convenient sampling was chosen to recruit participants from the largest center.
Sample size
The formula for calculating the minimum sample size was: N = (tα/2 S/δ)2. Based on the findings from a previous study using the same instrument as in this study, the baseline ML level was 96.77 ± 14.36 (Liang, 2010). The confidence level was set at [(1 − α) = .95]. The allowable error was set as 2(δ = 2). The above data were input into PASS (Power Analysis & Sample Size) 11 software, and it was calculated that the minimum sample size was 199. The participation response rate was estimated at 80%. As a result, the total number of participants would be 249.
Inclusion and exclusion criteria of participants
Patients who were eligible for the study were: (1) recipients of HD due to ESKD for at least six months, (2) aged 18 or above, and (3) able to read, listen, speak, and write the Chinese language.
Excluded in the study were patients (1) diagnosed with mental illness or cognitive impairment, or (2) with severe cardiovascular complications or other major diseases in the previous three months, such as acute heart failure, cerebral hemorrhage, cerebral infarction, advanced cancer, etc. These patients were either too fragile to participate or unable to provide reliable information.
Instruments
A 26-item questionnaire, the Meaning in Life Scale for Hemodialysis Patients (MLSHP)) (Appendix 1), was used to assess the ML levels of the patients who participated in the study. MLSHP is a ML assessment instrument in traditional Chinese, which was developed by a scholar in Taiwan, where as in Macau, traditional Chinese, rather than simplified Chinese, is the official language. The instrument contains four dimensions: goal of life (Items 1–7), value of life (Items 8–14), self-concept (Items 15–20), and spirituality (Items 21–26). A five-point Likert scale was used, ranging from Strongly Disagree (1 point), Disagree (2 points), On fence (3 points), Agree (4 points), to Strongly Agree (5 points). The total score on the scale is 130. The instrument has an excellent internal consistency (Cronbach's alpha = .94) and stability (Cumulative explanatory variation = 57.05%) (Liang, 2010).
The researchers also developed a general information questionnaire to collect the participants’ demographic and disease-related information. The information questionnaire had ten items, including Part 1-social-demographic characteristics (age, gender, residence status, marital status, level of education, monthly personal income, religious belief) and Part 2-disease-related factors (duration of dialysis treatment, symptom-related distress, existence of other chronic diseases).
Data Collection
The participants were recruited in January 2020. The primary researcher approached the potential participants in the HD center and explained the purposes of the study. If the patients agreed to participate, they were asked to sign a consent form and complete the information questionnaire and MLSHP, which usually took them 15 min to complete. For patients who were not able to fill the questionnaires, the researcher read out the questionnaires and then filled them after the patients gave the answers.
Quality Control
Several measures were taken to enhance the quality of the study. Firstly, the participants were asked to complete the questionnaires without asking other people's advice to avoid bias from others. Secondly, the researcher performed an on-site check-up to ensure that the participants had clearly and fully answered the questionnaires. Finally, after data collection, another check-up was performed by the researcher to identify any vague or careless answers to the questionnaire items.
Statistical Analysis
The SPSS (Statistical Product and Service Solutions) 22.0 statistical package was used to analyze the data. Frequency, percentage, arithmetic mean, standard deviation (SD), minimum value, and maximum value were used for the descriptive statistics of the variables. Spearman correlation was applied to determine the association between the patients’ age and their ML levels. Comparisons of ML levels between the patients with different demographic and disease-related characteristics were made using T-test or One-way analysis (ANOVA). Multivariate linear regression analysis was performed to identify the determinants of patients’ ML. Bilateral significance level α was set as .05. Statistical significance was taken as p < .05.
Ethics Consideration
The protocol of this study was approved by the research committee of a nursing college in Macau and the hospital that the HD center affiliated to. The participants were provided with sufficient time to raise their concerns and confusions, and the informed consent was obtained from all participants before they answered the questionnaires. The data from the participants were only accessible to the researchers and the patients’ identity were kept confidential. The participants were informed of their rights to withdraw from the study whenever they wished without any adverse effects on their received service in the HD center.
Results
Demographic Characteristics and Disease-related Conditions of the Patients
A total of 255 patients were contacted in the recruitment stage, and six of them refused to participate in the study. Of the 249 questionnaires collected from the patients, five had unanswered items, three had vague answers, and three had unnecessary multiple choices. After the 11 questionnaires were excluded, the remaining 238 questionnaires were included in data analysis. Therefore, the effective response rate was 95.58%.
Among the 238 patients on HD, the youngest was 23, and the oldest was 93, with an average age of 62.82 ± 12.73. Other demographic characteristics and disease-related conditions of the patients are shown in Table 1.
General Characteristics of Participants, N = 238.

Note: *MOP: Macanese pataca (1MOP = 0.98CNY = 0.12USD).
The ML Levels of the Patients
MLSHP measured the ML levels of the patients. The lowest ML score was 71, and the highest was 117, with an average score of 93.75 ± 10.00, accounting for 72.1% of the total score of 130 on MLSHP.
The Association between Patients’ ML Levels and their Demographic and Disease-related Factors
Bivariate analysis results
Bivariate analysis showed that two of the seven demographic variables were associated with ML levels (Table 2). Female patients had higher scores than male patients (p < .05). Religious belief constituted a strong indicator of the ML levels. Patients with religious belief had a higher score of 98.12 than those without religious belief who scored 90.74 (p < .001).
Bivariate Analysis of Participants’ Demographic and Disease-Related Characteristics and ML Levels, N = 238.
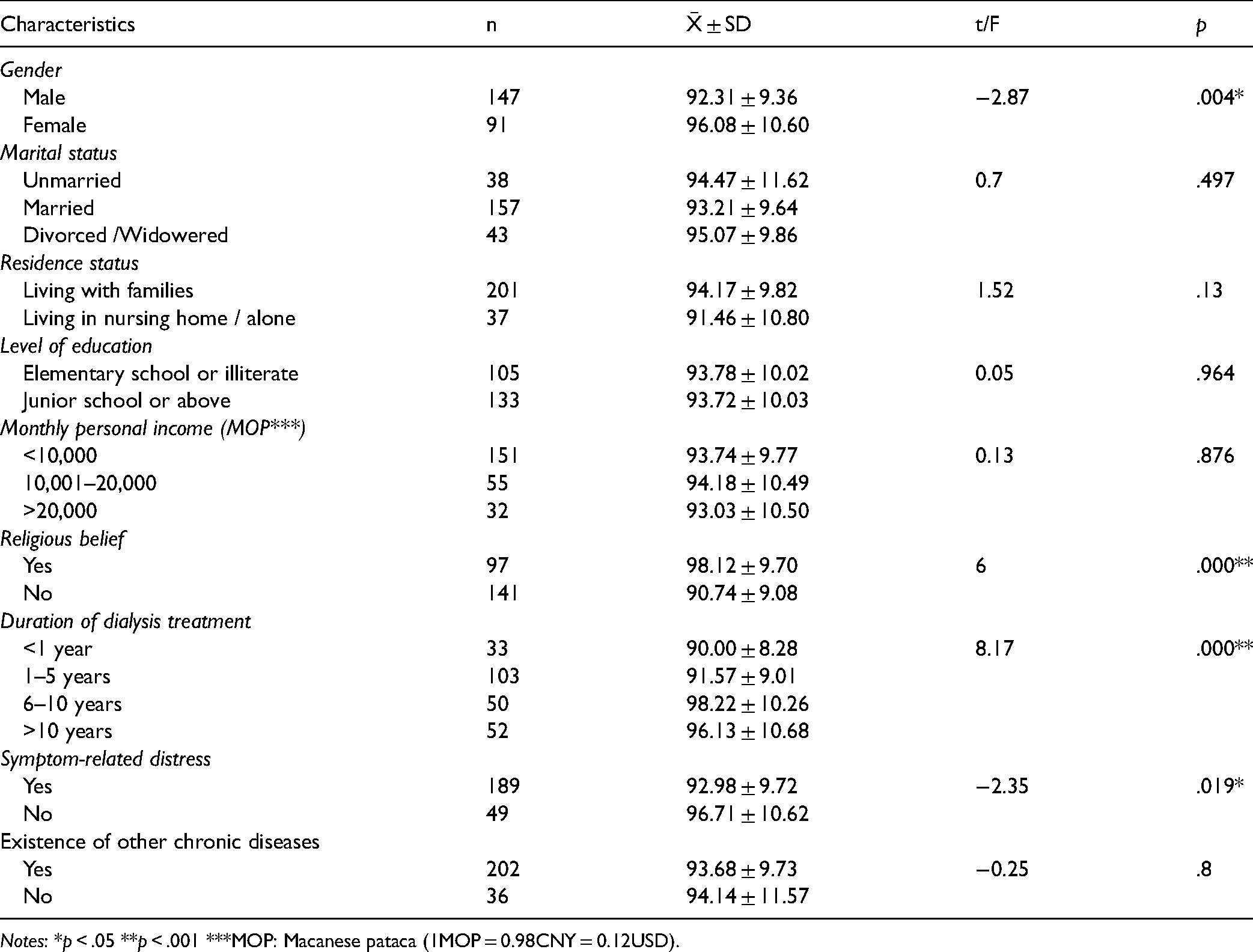
Notes: *p < .05 **p < .001 ***MOP: Macanese pataca (1MOP = 0.98CNY = 0.12USD).
Bivariate analysis also indicated that two disease-related variables were associated with ML levels (Table 2). Those who did not have symptom-related distress scored higher than those who had symptomatic distress (p < .05). In addition, those with a duration of HD treatment for 6–10 years had higher scores than other patients with either shorter or longer duration (p < .05).
Multivariate linear regression analysis results
Multivariate linear regression analysis was performed to predict the determinants of ML levels of the patients. The ML score of the patients was taken as the dependent variable, and the proved determinants in bivariate analysis were taken as independent variables, including gender, religious belief, duration of dialysis treatment, and symptom-related distress. Age was the only quantitative variable in this study and, to verify its impact on ML, it was taken as an independent variable in the linear regression analysis.
The regression analysis confirmed four independent variables as the determinants influencing patients’ ML, namely gender, religious belief, symptom-related distress, and duration of dialysis treatment. Based on the Beta coefficient, religious belief was the strongest determinant on patients’ ML, followed by the duration of dialysis treatment, symptomatic-related distress, and gender. Age had no association with ML scores (Table 3).
Multiple Linear Regression Analysis of HD Patients’ Influencing Factors, N = 238.
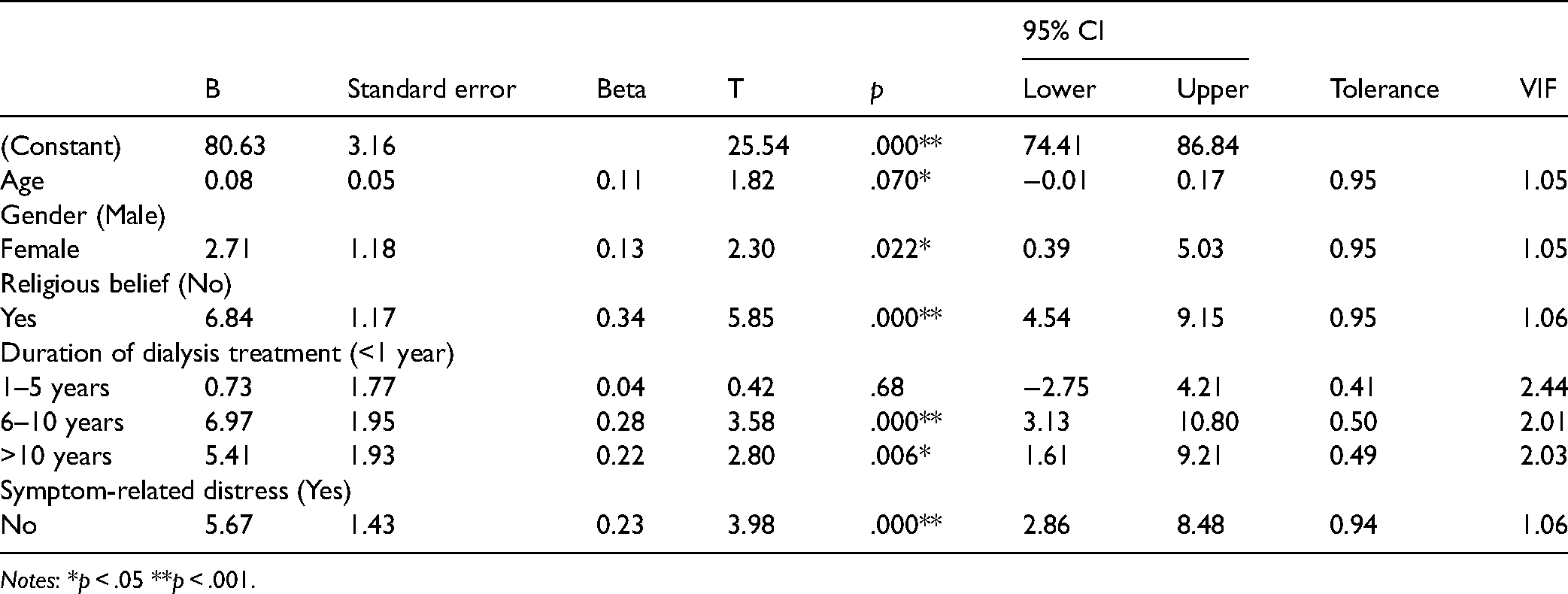
Notes: *p < .05 **p < .001.
Discussion
This study has yielded interesting findings, some of which align with previous studies, while others contradict previous ones. Moreover, these findings can be interpreted under the context of local social-economic conditions.
The ML Levels of the Patients on HD
The study revealed that the average ML score (93.95) among the patients on HD in Macau was above the median level on MLSHP, indicating the patients’ positive attitudes toward life. The average ML level among patients on HD in Macau was similar to that of those on HD in Taiwan (96.77), who were assessed by the same MLSHP instrument of the current study (Liang, 2010). Researchers in mainland China who used different ML instruments reported their HD patients’ ML around the median levels (Deng et al., 2011; Tao et al., 2018). In other words, the patients on HD in Macau held more positive attitudes toward life than their counterparts in mainland China.
The high ML levels of the patients on HD in Macau may be attributed to Macau's comprehensive and inclusive welfare system. Studies have found economic struggles among patients on HD due to medical expenses and productivity loss (Hashemi et al., 2018; Jeon et al., 2020). Similarly, the economic stress was observed in our study. In Macau, the average monthly income of an employee is about 17,000 MOP (1,868 USD) (Statistics and Census Service of Macao SAR, 2019b), while more than half of the patients on HD in this study had a monthly income less than 10,000 MOP (1,245 USD). However, the low-income patients in this study might have received the support of medical subsidies and the economic assistance provided by the government. When people have their basic needs secured, they tend to be optimistic about life (Norris, 2020). Our findings have implications for policymakers in other places. Patients on HD are vulnerable to economic constraints and they should be supported financially by governments for their health and wellbeing.
The Influencing Factors of ML among Patients on HD
Our study discovered that ML was influenced by multiple factors, including gender, religious belief, duration of dialysis treatment, and symptom-related distress, with religious belief being the most significant determinant. A plethora of other studies supported the association between religious belief and patients’ ML (Dar & Iqbal, 2019; Hsiao et al., 2007; Testoni et al., 2018; Volkert et al., 2019).
Religious belief is a way of expressing and practicing individuals’ spiritual experience (Alcorn et al., 2010; Chu, 2018; Hage, 2006), while spirituality can be interpreted as the meaning and purpose of life. Religious belief and spirituality can improve health outcomes, such as health-related QoL, even during terminal disease. Whereas residents in Macau have freedom of religious belief, this study showed that nearly 60% of the participants did not have a religious belief.
Gender is another influencing factor, with female patients having higher ML levels than male patients, indicating that female patients held a more positive attitude toward life. The result is similar to the findings reported by Wang et al. (2016) in a study with cancer patients, in which female patients showed a greater level of meaning creation than male patients. Other studies with healthy populations found that females seemed to be more thoughtful and empathetic than males (Abe et al., 2018; Reker, 2005). As a result, they were more likely to receive support and encouragement from people around them. Among the participants in this study, 81.32% of the female patients lived with their families, which was an obvious contrast to male patients, of whom only 18.68% lived with families. This may indicate better support from families the females obtain than males, and family support can elevate patients’ optimism when they encounter difficulties (Al-bakr et al., 2017; Lee et al., 2019).
In addition to demographic factors, two disease-related factors were also associated with the ML levels of the patients on HD, namely symptom-related distress and duration of dialysis treatment. The majority (79.4%) of the patients in this study had symptom-related distress, including sleep disorders, fatigue, muscle spasm, and pruritus. The symptom-related distress was also reported by other researchers (Göriş et al., 2016; Mi-Kyoung et al., 2018; Yong et al., 2009). Under some circumstances, symptom-related distress has more impacts on patients’ QoL than changes in their vital signs or lab results (Li et al., 2016; Saini et al., 2006).
This study uncovered that patients who had been receiving HD treatment for 6–10 years had the highest ML level compared with other patients who had either shorter or longer treatment duration. Patients who are new on HD treatment may be in the adjustment process. They may be anxious and frustrated due to their limited knowledge of the disease and treatment, leading to negative attitudes toward life (Tian et al., 2015; Tsai et al., 2019). After undergoing dialysis treatment for several years, the patients may have learned how to live with HD and eventually reconstruct their meaning of self-worth and regain their ML. However, disease or treatment-related complications occur with disease progressing, and patients become more fragile physically and more distressful psychologically. As a result, they become increasingly pessimistic about their future (Weng et al., 2003; Zhang et al., 2019), leading to lower ML levels.
Implication of Practice
Compared with patients who have no religious belief, patients with religious beliefs hold more positive attitudes toward life. Therefore, nurses in dialysis centers should pay more attention to the patients without religious belief, who may account for greater proportion in populations such as Macau and mainland China. Moreover, scholars have advocated spiritual care for all the patients (Batstone et al., 2020; Cabaço et al., 2018) because spirituality is a broad concept that transcends religion, and the nurses in the dialysis centers should deliver universal love-based holistic care to their patients regardless of their religion. Nurses can enhance communications between patients with and without religious belief by holding group discussions to promote reflections on ML and the nature of one's existence. In addition, multidisciplinary approaches among nurses and other professionals, such as physicians, preachers, psychologists, etc., are effective interventions to improve the ML levels of patients with terminal illnesses (Murgia et al., 2020). In the hospital where the study was conducted, these interventions had been implemented in the hospice ward. Whereas spiritual care or meaning-centered interventions for cancer patients are flourishing, efforts are needed in nursing to expand the experiences gained from working with cancer patients to caring for patients on HD. Furthermore, spiritual care should be valued in every region because of the substantial number of patients without religion.
Research has continuously reported the sex and gender differences in the epidemiology and outcomes of chronic kidney diseases (Carrero et al., 2018), calling for gender-based or gender-sensitive interventions. This study also found higher ML levels with female patients than male patients. Therefore, female patients on HD can be encouraged to share their adjustments to dialysis treatment with their male counterparts. In addition, open communications should be encouraged between male patients and their family members to promote the intimacy of the patients with their families because social support from family members is vital for patients’ resilience to difficulties and challenges (Sousa et al., 2019).
The management of symptom-related distress should be a treatment priority for patients on HD, as found in this study and echoed by other studies (Goh & Griva, 2018). Particular attention should be paid to the patients who are new on HD treatment or who have had decade-long HD treatment. Regarding the volatile nature of the physiological and psychological conditions of the patients on HD, the National Kidney Foundation of the United States has recently advocated a life plan for all ESKD patients who receive the kidney replacement modality (Lok et al., 2020). This plan should be individualized, taking into account patients’ current and anticipated medical and life circumstances and presences. The life plan should be regularly re-evaluated, given expected changes in a patient's life circumstances. Other scholars proposed that, while early identification of ESKD-induced symptoms is paramount, the patients’ mental health conditions should be evaluated biannually (Goh & Griva, 2018). In the long journey of managing ESKD and treatments, patients and their families should be encouraged to be actively involved in the decision-making process with their doctors and nurses (Årestedt et al., 2019).
Limitations
The small sample size of the participants from a single dialysis center was undoubtedly a shortcoming of the study design. Although participants of this study were selected from the largest dialysis center in Macau, they could not represent all patients on HD in the local area. Convenient sampling also limited the generalization of the study findings. Whereas the number of participants in this study exceeded the minimum sample size, the number of participants in some sub-groups was too small, resulting in the combination of the sub-groups. For example, the sub-group “living in nursing home” had only four patients. Hence, it had to be combined with the sub-group “living alone” to satisfy statistical analysis conditions. Such combinations weakened the richness of the data to a certain extent. Future research should be more rigorously designed with larger sample sizes from more recruitment sites.
Conclusion
This study explored ML status and the influencing factors among HD patients in Macau of China. The study's findings added to the richness of the influencing factors behind the ML of the patients on HD or with other terminal illnesses. While the findings from this study might not be new, they confirmed some findings from other locally conducted studies. More importantly, this study set the meaning of its findings under local economic and cultural conditions, thus suggesting evidence-based and culturally fit interventions for nurses in dialysis centers. The four determinants to patients’ ML identified in the study supported ML as physiologically, psychologically, and spiritually constructed. Along with the discussions on physiological and psychological factors, such as symptom management and family support, the study emphasized spiritual care for the patients who did not have a religious belief. These discussions have implications for the nurses in dialysis centers in other places when working with non-religious patients.
Footnotes
Abbreviations
Acknowledgments
The authors would like to thank the participants who joined in the study in order to provide data for this study. In addition, the authors would like to thank Kiang Wu Nursing College of Macau and Kiang Wu Hospital in Macau for supporting this study.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the first author and/or the corresponding author based on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Research Ethics and Patient Consent
The researchers gained ethics approval from the research committees of Kiang Wu Nursing College of Macau and Kiang Wu Hospital. A written consent form was obtained from participants before they filled the questionnaires.
Appendix 1
Meaning in Life Scale for Hemodialysis Patients
Appendix 2
Authors’ translation of Meaning in Life Scale for Hemodialysis Patients (Please note that the translation is only for the international readers to understand the contents of the scale and does not indicate that there is an English version of the scale)
Strongly Agree (5 points), Agree (4 points), On fence (3 points), Disagree (2 points), Strongly Disagree (1 point)
Life is a way of learning. The ultimate meaning of life is to live without regret and die without regret. Recalling back, I deeply feel that my life is meaningful. The meaning of life lies in knowing, cherishing and benefiting. I can accept other people's shortcomings. I regard difficulties as opportunities for challenges. My life is in my own hands. Suffering experience can make me better understand the meaning and value of life. I value those ordinary people in society who do good deeds silently. I do good deeds whenever possible and help others. I am sure that everyone's existence has its unique significance and value. I am grateful every day. I make myself happy. I respect my life and seem to be reborn after treatment. The meaning of life lies in individuals’ responsibility to be fully carried out during the lifetime. I am a responsible person. I can accept myself. I am a lucky person. I am involved in human affairs, have a destiny, and live in the present. I am active and energetic. Pursuing spiritual growth in life is an ideal life. I believe that human nature is good. I think all things in nature have spirituality. I believe that everything has a cause and a result. Religious belief contributes to spiritual growth. Religion can calm your mind.