
Abstract
Background
The utilization of skilled care before, during, and after childbirth can significantly reduce maternal mortality and save the lives of women and newborns. However, maternal and child mortality remain high and continue to pose a persistent challenge for low-income countries. Therefore, this study was conducted to identify individual- and community-level factors associated with institutional delivery in Ethiopia.
Methods
A cross-sectional study design with two-stage clustered sampling was employed using data from the 2016 Ethiopian Demographic and Health Survey (EDHS) to identify individual- and community-level factors associated with institutional delivery in Ethiopia. The study included 643 clusters (communities) and 7,091 women aged 15–49 years. Data were analyzed using two-level mixed-effects logistic regression to estimate the fixed effects of individual- and community-level factors and the random intercept for between-cluster variability, using R software version 3.5.3.
Results
In this study, over two-thirds (68%) of women gave birth at home. Institutional delivery was more likely among women with higher education, greater household wealth, frequent antenatal care attendance, and partners with secondary education. Conversely, it was less likely among women with more children and those perceiving long distances to health facilities as a barrier. At the community level, higher average education, media exposure, and recent use of health services were associated with greater institutional delivery use, while rural residence, perceived distance barriers, and regional disparities were linked to lower use.
Conclusions
Both individual- and community-level factors were significantly associated with institutional delivery, in both positive and negative directions. Therefore, the Government of Ethiopia and relevant stakeholders should give due attention to the key factors identified in this study.
Background
Every day, approximately 830 women die from preventable causes related to pregnancy and childbirth worldwide. Nearly all maternal deaths (99% of global deaths) occur in developing countries, with more than half taking place in sub-Saharan Africa (Onambele et al., 2023). As part of the Sustainable Development Goals, the global target between 2016 and 2030 is to reduce the maternal mortality ratio to fewer than 70 deaths per 100,000 live births. By 2030, no country should have a maternal mortality ratio higher than 140 per 100,000 live births, which is twice the global target (Moran et al., 2016).
Ethiopia has one of the highest maternal mortality ratios in sub-Saharan Africa, with 412 deaths per 100,000 live births, largely due to low maternal health service utilization particularly low rates of institutional delivery (Daniel G Belay, Alemu, Pereira, Lassi & Tessema, 2023). The majority of maternal deaths are preventable, as effective healthcare interventions to prevent or manage pregnancy-related complications are well established. Timely access to skilled care during pregnancy, childbirth, and the postpartum period can significantly reduce the risk of maternal mortality (Mustafa et al., 2016).
All women require access to antenatal care during pregnancy, skilled care during childbirth, and appropriate care and support in the weeks following delivery to ensure their health and well-being, as well as that of their newborns (Pathak et al., 2017). The utilization of skilled care before, during, and after childbirth is critical in reducing maternal mortality and saving the lives of both women and newborns. Skilled attendance during labor, delivery, and the early postpartum period is estimated to prevent between 13% and 33% of maternal deaths (Baral et al., 2010).The major complications responsible for nearly 75% of all maternal deaths include severe bleeding (primarily postpartum hemorrhage), infections (usually occurring after childbirth), high blood pressure during pregnancy (such as pre-eclampsia and eclampsia), complications during delivery, and unsafe abortion (Berhan & Berhan, 2014b).
It is especially crucial that all deliveries are attended by trained health experts, as timely care and treatment can mean the difference between life and death for both the mother and the baby (Ameh & Van Den Broek, 2015). The proportion of births attended by skilled health personnel is a key indicator under Sustainable Development Goal (SDG) 3, specifically Target 3.1, which aims to reduce the global maternal mortality ratio to less than 70 per 100,000 live births by 2030. Skilled attendance at birth is widely recognized as one of the most effective interventions for preventing maternal deaths, as it ensures timely management of complications during childbirth and the immediate postpartum period (Bhowmik et al., 2020). However, the majority of deliveries in Ethiopia particularly in rural communities still occur at home without the assistance of skilled birth attendants. According to a 2024 study, the prevalence of home delivery in rural Ethiopia was 58.72%, with a significant spatial variation across districts (D. B. Belay, Tilahun, Birhan, Tiku & Chen, 2025).
Studies show that skilled delivery is influenced by factors like socio-economic status, education, access to care, and cultural beliefs. While some factors are universal, others depend on local systems and norms (Freedman et al., 2005). Understanding these diverse factors is crucial for designing targeted interventions that can improve maternal healthcare utilization in specific contexts (Hill et al., 2023). In Ethiopia, institutional delivery is limited by poor access to health facilities, especially in rural areas, cultural preference for home births, and concerns over the quality of care (Roro et al., 2014). The factors influencing one behavior often differ from those influencing another, and the most effective interventions are those that target specific behaviors with tailored strategies (Noar et al., 2007).
In Ethiopia, the goal of ensuring that all births occur in health facilities attended by skilled health professionals remains a significant challenge. Institutional delivery service utilization has historically been low (Berhan & Berhan, 2014a) (N. Kebede et al., 2023). For instance, in 2014, only 16% of births were attended in health facilities (Berhan & Berhan, 2014a), a rate significantly lower than in many other developing countries.
Literature Review
Home births remain highly prevalent among poor women in sub-Saharan Africa (SSA), South Asia, and Southeast Asia, where 74.7–89.9% of women in the lowest two wealth quintiles give birth at home. In SSA, the poorest women are more than three times as likely to deliver at home as the richest (77.7% vs. 22.4%). In Ethiopia, only 2% of deliveries in the poorest households were attended by skilled personnel, compared to 46% in the wealthiest (Montagu et al., 2011; UNICEF; Worku, Yalew & Afework, 2013). According to the 2016 EDHS, approximately 74% of births occurred at home without skilled attendance (Demographic, 2016).
Institutional delivery plays a critical role in reducing maternal and perinatal mortality. Studies indicate that up to 14 perinatal deaths per 1,000 births can be averted by delivering at health facilities (Chinkhumba et al., 2014). Moreover, 16–33% of maternal deaths are preventable through skilled attendance that addresses complications such as obstructed labor, eclampsia, puerperal sepsis, and hemorrhage. The presence of skilled health workers, backed by emergency referral systems, is crucial for improving maternal outcomes (Kinney et al., 2010).
However, many deliveries still occur at home. A multi-country DHS analysis across 48 developing countries found that more than half of births take place without skilled attendance (Montagu et al., 2011). Interestingly, countries like Peru, Tunisia, Egypt, and Namibia report relatively low maternal mortality despite low skilled attendance, possibly due to effective emergency care. In contrast, countries such as Ghana, Malawi, Bolivia, and Zambia have high skilled attendance but also high maternal mortality, likely due to poor healthcare quality or unskilled providers. Therefore, skilled attendance must involve both competent professionals and supportive infrastructure (Chinkhumba et al., 2014; Graham et al., 2001).
Numerous individual factors influence institutional delivery. Studies from the Awi and Hadiya zones indicate that younger mothers (under 25 years old) are more likely to deliver at health facilities. In contrast, studies from Cambodia suggest that older women are more likely to use health institutions for delivery. Wealth status is also a significant determinant; women from wealthier households are more likely to utilize health facilities, as evidenced by studies from Wolaita and other regions in Ethiopia. Antenatal care (ANC) is a consistent predictor of institutional delivery. Women who attend ANC particularly those with four or more visits are up to four times more likely to give birth in a health facility (Asseffa et al., 2016; Wolelie et al., 2014).
Education plays a crucial role as well. Women with at least primary education are more likely to deliver in health institutions. Similarly, a husband's educational status influences delivery location; women whose husbands have no formal education are less likely to use health facilities for childbirth. Other individual factors such as prior experience with facility-based delivery, pregnancy planning, and complications in previous pregnancies also increase the likelihood of institutional delivery. Media exposure likewise promotes the use of health facilities (Ahmed et al., 2018; Sagna & Sunil, 2012).
Community-level factors are equally important. Women living in communities with high levels of female education and ANC utilization are significantly more likely to deliver at health institutions (Mekonnen et al., 2015). Moreover, residing in areas with lower poverty rates and greater media exposure is associated with higher rates of institutional delivery.
Overall, improving maternal health outcomes requires addressing both individual and community-level determinants through integrated health and social interventions (Mekonnen et al., 2015; Sagna & Sunil, 2012). However, there is limited recent evidence on the progress made or challenges that persist in institutional delivery utilization. Therefore, this study aimed to identify individual and community-level factors associated with institutional delivery in Ethiopia, using data from the 2016 Ethiopia Demographic and Health Survey. The findings are intended to inform maternal health advocates, policymakers, and planners in designing targeted strategies to improve the utilization of skilled delivery services across the country.
Methods and Materials
Study Design, Period, and Setting
Ethiopia is the second most populous country in Africa after Nigeria, with a population of over 114 million. It is bordered by Eritrea, South Sudan, Sudan, Djibouti, and Somalia (Leong et al., 2018). Administratively, Ethiopia is divided into nine regional states (Tigray, Afar, Amhara, Oromia, Somali, Benishangul-Gumuz, SNNPR, Gambella, and Harari) and two chartered cities, Addis Ababa and Dire Dawa. The country has a three-tier health care delivery system. The first level includes primary care facilities district hospitals, health centers, and their satellite health posts. While district hospitals and health centers provide both curative and preventive services, health posts primarily focus on preventive care. The second level consists of general hospitals, and the third level comprises specialized hospitals, both of which primarily offer curative services. The 2016 Ethiopian Demographic and Health Survey (EDHS) was a nationally representative, population-based cross-sectional study conducted from January 18 to June 27, 2016 (Geremew et al., 2018).
Data Source
In this study, the dataset was obtained from the MEASURE DHS database, available at http://dhsprogram.com/data/(supplemental file 1). Access to the 2016 Ethiopian Demographic and Health Survey (EDHS) dataset was granted through an official authorization letter from the DHS Program Office. The 2016 EDHS is the fourth nationally representative and comprehensive survey conducted in Ethiopia, aimed at providing up-to-date information on population health indicators, including fertility, maternal and child health, nutrition, and health service utilization. The data are collected using standardized methodologies, allowing for both national and regional-level comparisons and supporting evidence-based decision-making in health policy and program development.
Sampling Procedures
In the 2016 Ethiopian Demographic and Health Survey (EDHS), each region of the country was first stratified into urban and rural areas, resulting in 21 distinct sampling strata. The sample was selected using a two-stage stratified sampling design. In the first stage, a total of 645 enumeration areas (also referred to as clusters) 202 urban and 443 rural were randomly selected using probability proportional to the size of households within each stratum. In the second stage, 28 households were systematically selected from each cluster (Daniel Gashaneh Belay et al., 2022).
A representative sample of 18,008 households was initially selected, and interviews were successfully completed in 16,650 households. From these households, 16,583 eligible women aged 15–49 were identified for individual interviews, and completed interviews were conducted with 15,683 of them (Moran et al., 2016). For the purpose of this study, a weighted sample of 7,091 eligible women aged 15–49 years, who had given birth within the five years preceding the 2016 EDHS and who delivered either at a health facility or at home, were included in the analysis.
Study Variables
Data Analysis
Two-level mixed-effects logistic regression analysis was conducted using R software version 3.5.3 to account for the hierarchical nature of the 2016 EDHS data. Initially, bivariate analyses were performed to assess the association between each independent variable and the outcome. Variables with a p-value < 0.25 in the bivariate analysis were included in the final multivariable model. Adjusted odds ratios (AOR) with 95% confidence intervals were used to identify factors independently associated with institutional delivery, with statistical significance set at p < 0.05. Fixed effects estimated associations at the individual and community levels, while random effects assessed between-cluster variation. All analyses were weighted, and frequency tables were generated for both individual- and community-level variables.
Results
Individual Level Characteristics
The study included 7,091 women who had given birth in the five years preceding the 2016 Ethiopian Demographic and Health Survey (EDHS). The majority of women
In terms of socioeconomic status, 33.7% belonged to the poorest wealth quintile, while 23.0% were in the richest category. Regarding reproductive history, 41.0% had fewer than three living children, and 8.8% reported a history of abortion. Slightly more than half
Concerning husband's education
Individual Variables of Women who had Birth in the Five Years Preceding the 2016, EDHS (n = 7,091).

ANC = Antenatal care visits, HF = Health Facility, n = number of study participants, %= percent
Community Level Characteristics
The analysis of community-level factors among 7,091 the highest proportions of women resided in Oromia (14.4%)
Media exposure was limited, with 69.8% of women in communities classified as having low media access, likely reducing health awareness. Antenatal care (ANC) utilization was also suboptimal at the community level, with 69.1% of women in clusters with low ANC visit rates. However, a majority (63.4%) lived in areas with higher health facility visitation rates in the past year, suggesting some degree of healthcare engagement [Table 2].
Community Level Variables of Women who had Birth in the Five Years Preceding the 2016 EDHS, [n = 7,091].

ANC = Antenatal care visits, HF = Health Facility, n = number of study participants, SNNPR = South Nations, Nationalities and People's Region, %= percent.
Two Level Mixed Effects Logistic Regression Results
The between-cluster variability declined progressively across successive models, from 64% in the empty model to 24% in the individual-level only model, 19% in the community-level only model, and 16% in the combined model. Consequently, the combined model incorporating both individual-level and community-level factors was selected for predicting women's place of delivery. The intraclass correlation coefficient (ICC) in the empty model indicated that 64% of the total variance in institutional delivery utilization was attributable to differences across clusters (communities). In Model I, which included only individual factors, results showed that education level, wealth index, perceived distance as a barrier to medical care, husband's education level, number of living children, ANC visits, and health facility visits in the past 12 months were significantly associated with institutional delivery. Model II, incorporating only community-level variables, demonstrated that 24% of variation was attributable to community differences, with individual-level characteristics explaining 63% of the variance (PCV = 63%). This model revealed that region, place of residence, community-level women's education, perceived distance, media exposure, ANC visits, and health facility visits were significantly associated with the outcome variable. The community-level variation accounted for 19% (ICC = 19%) of the dependent variable's variance, with community characteristics explaining 70% of institutional delivery utilization (PCV = 70%). The final model (Model III) included both individual and community-level characteristics simultaneously. Results indicated that women's education level, wealth index, perceived distance, husband's education, number of living children, health facility visits, region, and place of residence remained significantly associated with institutional delivery. After adjustment, women with primary education had 1.37 times higher odds (AOR = 1.37; 95% CI:1.13–1.66) of institutional delivery compared to uneducated women, with progressively stronger effects for secondary (AOR = 2.24; 1.56–3.22) and higher education (AOR = 3.83; 2.0–7.35). Wealthier women showed increased utilization, with the richest having 1.83 times higher odds than the poorest. Women perceiving distance as problematic had 24% lower odds (AOR = 0.76; 0.62–0.93) of institutional delivery. Those with husbands having secondary or higher education were nearly twice as likely to deliver in facilities. Multiparous women showed significantly reduced utilization. A strong dose-response relationship emerged for ANC visits, with women completing 4 + visits having 7.6 times higher odds than those with none. Regional disparities were pronounced, with Afar (AOR = 0.15; 0.06–0.38) and Gambella (AOR = 0.21; 0.09–0.51) showing substantially lower utilization than Addis Ababa. Rural women had 64% lower odds (AOR = 0.36; 0.24–0.55) than urban residents. Community-level education (AOR = 1.36; 1.09–1.71), media exposure (AOR = 1.54; 1.14–2.08), and ANC utilization (AOR = 1.60; 1.18–2.08) all positively influenced institutional delivery rates [Table 3].
The ICC shows that 64% of the variability in institutional delivery was attributable to differences between communities in the empty model. This variability progressively declined with the inclusion of individual- and community-level factors, indicating improved model performance. The proportional change in variance and Akaike Information Criterion values further support the final model (Model III) as the best-fitting model, incorporating both individual and community determinants [Table 4].
Two Level Mixed Effect Regression Results of Individual and Community Level Factors Associated with Institutional Delivery in Ethiopia, 2016 EDHS.
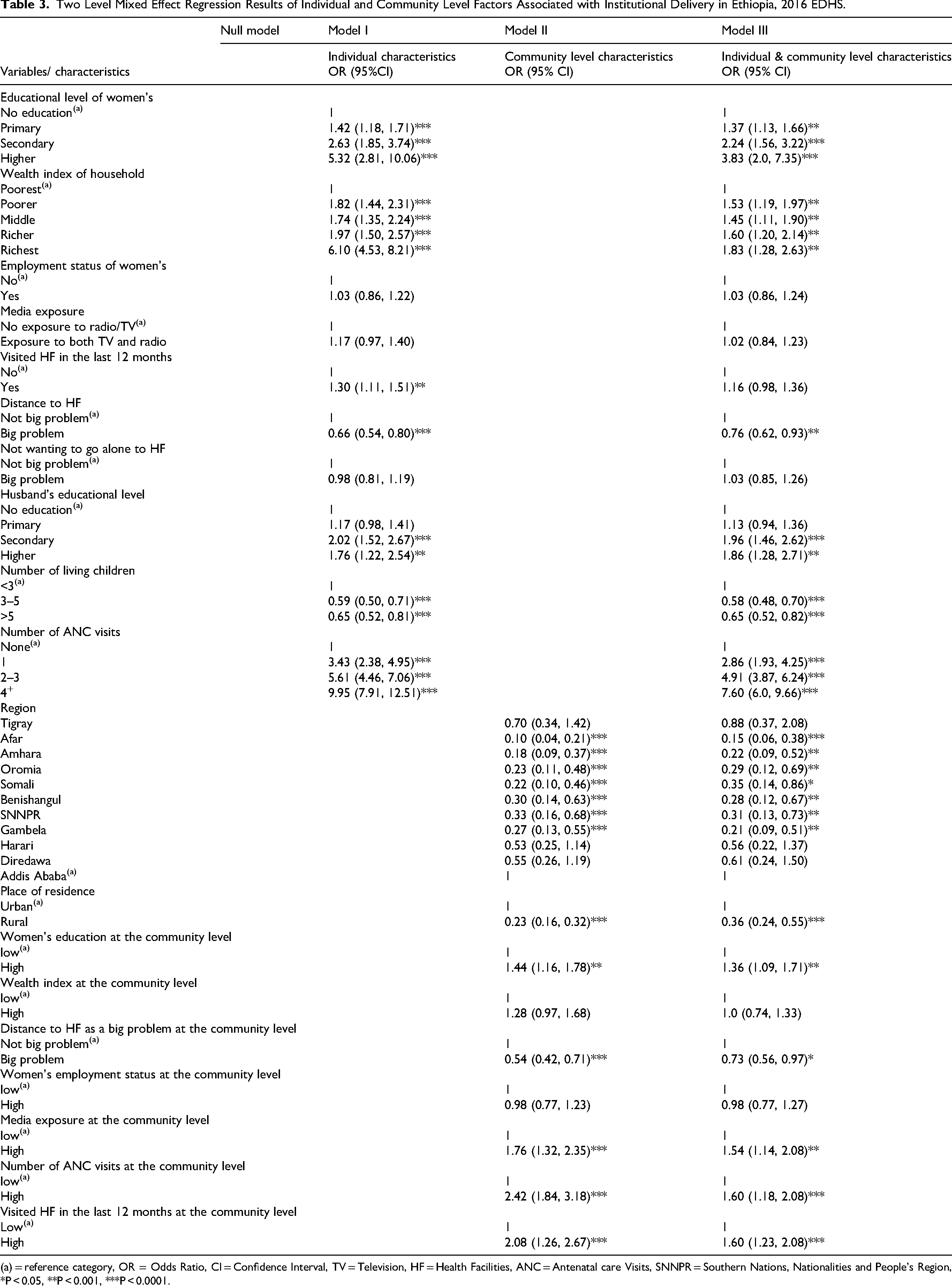
(a) = reference category, OR = Odds Ratio, CI = Confidence Interval, TV = Television, HF = Health Facilities, ANC = Antenatal care Visits, SNNPR = Southern Nations, Nationalities and People's Region, *P < 0.05, **P < 0.001, ***P < 0.0001.
Model Fit Statistics and Random Effects for Multilevel Logistic Regression Analysis of Factors Associated with Institutional Delivery in Ethiopia, EDHS 2016.

AIC = Akaike Information Criterion, ICC = Intera Class Correlation, PCV = Proportional Change in Variances.
Discussion
This study aimed to explore the key factors influencing the use of institutional delivery services in Ethiopia by analyzing data from the 2016 EDHS. Given the hierarchical structure of the data, a multilevel logistic regression analysis was applied to account for variations at different levels and to identify significant predictors of institutional delivery utilization. This study revealed that more than two-thirds (68%) of Ethiopian women did not give birth in a health facility. The finding was lower than reports from Nepal (55%) (Shah et al., 2015), sub-Saharan Africa (66%) (Adde et al., 2020), and Uganda (90.2%) (Mugambe et al., 2021). This difference could be explained by the relatively low educational attainment among women in Ethiopia, as well as limited access to health care facilities and maternal health services compared to those countries. On the other hand, the result was higher than those reported in earlier studies from Ethiopia (Tesema et al., 2020) and Kenya (Tesema et al., 2020). This improvement might be linked to the government's intensified efforts to expand maternal health services through initiatives such as enhancing the Health Extension Program, establishing health development armies, constructing additional health infrastructure, training skilled health professionals, and improving the overall quality of care.
The findings of this study indicate that institutional delivery in Ethiopia is influenced by a range of individual and community-level factors. Positive predictors of institutional delivery included women's level of education, frequency of antenatal care visits, household wealth, husbands’ educational background, media exposure, and the general educational status of the community. Conversely, factors such as region, rural residence, higher number of living children, and perceived distance to health facilities were found to be negatively associated with the use of institutional delivery services. This study found that women residing in communities with higher educational levels were more likely to utilize institutional delivery services compared to those in less-educated communities. Likewise, individual women with higher education had increased odds of delivering in health institutions. This finding aligns with previous studies in Ethiopia and beyond ((Kruk et al., 2015; Mekonnen et al., 2015; Weldemariam et al., 2018). Education likely improves awareness of maternal health, recognition of pregnancy-related risks, and decision-making power (Namdeo, 2017). It is evident that educated women have greater confidence and capability to take action regarding their health. In addition, living in a community with a high or low level of education also plays an important role in the utilization of institutional delivery.
In this study, women living in communities with high antenatal care (ANC) utilization rates were more likely to give birth at health facilities compared to those in communities with low ANC utilization. This finding is consistent with previous studies conducted in Ethiopia and other African countries, where community-level ANC utilization was found to influence individual mothers’ decisions to seek institutional delivery services (Demilew et al., 2016; Kuteyi et al., 2011; Mekonnen et al., 2015; Stephenson et al., 2006). One possible explanation is that ANC visits increase women's awareness of the risks associated with pregnancy and childbirth and promote better birth preparedness, thereby encouraging facility-based deliveries (Kuteyi et al., 2011). Additionally, the health education, counseling, and treatment services provided during ANC visits may lead to positive behavioral changes and enhance the perceived benefits of delivering at health institutions (Mekonnen et al., 2015).
This finding aligns with evidence from other studies (Babalola & Fatusi, 2009; A. Kebede et al., 2016; Mekonnen et al., 2015), which also identified household wealth as a key factor influencing institutional delivery. Similar patterns have been observed, where mothers from wealthier households were more likely to utilize health facilities for childbirth compared to those from poorer households. These may be because better economic status may increase healthcare-seeking behavior and autonomy of healthcare decision-making as they are capable of paying the required medical and transport costs (Mamdani & Bangser, 2004).
Media plays a vital role in promoting health service utilization. In this study, women in communities with high media exposure were more likely to use institutional delivery services than those in low-exposure areas. This aligns with findings from Ethiopia (A. Kebede et al., 2016), highlighting media as a key factor. The possible reason is that health information may improve health-seeking habits via various electronic and print media, as information about what services are available, where and when to get them, as well as the benefits and risks of accessing specific services, can be communicated via such media (Mamdani & Bangser, 2004).
Regional variation significantly affected institutional delivery, with lower utilization observed in peripheral areas. The developing regions of Afar and Gambella had the lowest rates, possibly due to weak health infrastructure, limited resource allocation, and low prioritization capacity (Bobo et al., 2017). Additionally, disparities in infrastructure and literacy levels may hinder access to maternal health services. This finding is consistent with studies from Ethiopia and Bangladesh, which also showed regional differences in health service utilization among women (Kamal, 2013; Mekonnen et al., 2015).
Perceptions of distance to health facilities significantly influenced the use of institutional delivery services. Long travel distances, especially when combined with limited transportation options, create major challenges for pregnant women. Similar findings have been reported in studies conducted in Ethiopia and other African countries (Doctor & Dahiru, 2010; Mekonnen et al., 2015; Utomo et al., 2011). These barriers can prevent timely access to care, even when the decision to seek institutional delivery has been made. In communities where reaching a facility was seen as difficult, fewer women gave birth at health institutions.
This study also revealed that women living in communities with frequent health facility visits in the past 12 months were more likely to utilize institutional delivery. Similar findings were reported in previous studies (Aremu et al., 2012; Yebyo et al., 2014), which showed that visiting health facilities increases the likelihood of giving birth at health institutions. Frequent visits may reflect greater familiarity with health services and provide opportunities to receive important health information from providers, thereby encouraging the use of institutional delivery.
Limitations of the Study
One limitation of this study is the use of clusters as the higher-level unit of analysis, despite some clusters containing too few individual women to reliably generate aggregated community-level characteristics. Additionally, a considerable portion of the variability in the model remains unexplained. Due to data constraints, the study did not include a variable for the distance to health care facilities, which could have provided a better explanation for the variation in institutional delivery rates at the community level.
Implications for Practice
This study underscores critical areas for intervention to improve institutional delivery rates in Ethiopia. Health practitioners, program planners, and policymakers should prioritize targeted efforts to enhance women's education, increase antenatal care attendance, and expand community awareness through media and health service outreach. Addressing geographic and financial barriers especially in rural and underserved regions should be a strategic focus, ensuring equitable access to maternal health services. Engaging male partners in maternal health education and empowering communities through improved service delivery can further encourage institutional births. These findings support the need for integrated, multi-level strategies that respond to both individual needs and broader community contexts to reduce maternal and neonatal mortality.
Conclusion
Our findings revealed that institutional delivery rates in Ethiopia remain suboptimal. The analysis identified both individual and community-level factors significantly influencing delivery location. Institutional delivery utilization showed positive associations with maternal education level, household wealth status, paternal education, ANC visit frequency, media exposure, and regular health facility attendance. Conversely, utilization was reduced by perceived distance barriers, higher parity with three or more children, rural residence, and regional disparities particularly evident in Afar and Gambella regions. The substantial community-level effects underscore the importance of contextual factors in healthcare utilization patterns. We recommend that the Ethiopian government and health partners implement targeted interventions through education campaigns, transportation solutions for remote areas, equitable resource allocation across regions, and strengthened ANC-to-delivery care continuity, with particular focus on high-parity women and rural populations.
Supplemental Material
sj-docx-1-son-10.1177_23779608251358700 - Supplemental material for Multilevel Analysis of Individual and Community Level Factors Associated with Institutional Delivery in Ethiopia, 2016 Ethiopian Demography and Health Survey
Supplemental material, sj-docx-1-son-10.1177_23779608251358700 for Multilevel Analysis of Individual and Community Level Factors Associated with Institutional Delivery in Ethiopia, 2016 Ethiopian Demography and Health Survey by Masrie Getnet, Addis Temie, Tilahun Fufa, Lake Kumlachew and Abraham Teym in SAGE Open Nursing
Footnotes
Acknowledgments
We would like to acknowledge the Demographic Health Survey program office for the realization of this finding by authorizes the data.
Ethics Approval and Consent to Participate
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.