
Abstract
Background
Hepatitis B virus (HBV) infection is one of the world's most important public health issues. Vaccination remains the mainstay for preventing HBV transmission. Among health care workers, adequate knowledge of HBV infection has the potential to induce the motivation to vaccinate against the disease. This study aimed to assess the knowledge of HBV and its influence on vaccination intentions.
Methods
A descriptive cross-sectional survey was undertaken, and healthcare workers were randomly recruited from two healthcare facilities. A pretested, structured questionnaire with three domains was used to collect data in a self-administered interview session. Data entry, cleaning, and analysis were performed using SPSS. Descriptive statistics were performed to summarize the data. Reliability tests, Pearson correlation analysis, and multiple linear regression analysis were performed to identify the correlation and predictive relationships.
Results
The mean age and mean period of professional experience were (SD 31.20 ± 5.25) years and 4.64 (±3.95) years, respectively. The overall reliability coefficient of the combined scale was α = .83. The participants demonstrated satisfactory knowledge of the disease and its causation, transmission, consequences, and prevention, giving correct responses predominantly on 12 out of 15 domains with a knowledge mean score of 11.65 ± 0.91. The participants also had good intentions for HBV vaccination (3.58 ± 0.22). There was a positive correlation between HBV knowledge and vaccination uptake intentions (r = .33, p < .01). Hepatitis B knowledge significantly predicted vaccination uptake intentions (β = .23, t = 2.88, p < .01).
Conclusion
The study found that healthcare workers had a satisfactory level of knowledge about HBV infection. Most participants correctly identified key aspects of the disease, including its causation, transmission, consequences, and prevention. Importantly, higher knowledge levels were significantly associated with stronger vaccination uptake intentions, as demonstrated by a positive correlation and a predictive relationship.
Introduction
Hepatitis B virus (HBV) is a DNA virus from the Hepadnaviridae family that primarily targets hepatocytes, leading to severe liver inflammation and damage, which can progress to cirrhosis, liver cancer, or death (Hu, 2019). Globally, an estimated 254 million people live with chronic HBV, with 1.2 million new infections and 1.3 million HBV-related deaths annually, making it the second leading infectious cause of death (World Health Organization, 2024a, 2024b).
HBV is transmitted both vertically (from mother to child during pregnancy, childbirth, or breastfeeding) and horizontally (through contact with infected blood or body fluids, unsafe injections, and contaminated instruments). This efficient transmission poses a significant occupational risk to healthcare workers (HCWs), who experience HBV prevalence rates ranging from 2.3% to 5.0% globally, with the highest rates reported in Africa (Coppola et al., 2016; Maamor et al., 2022; Mahamat et al., 2021). A meta-analysis estimated HBV prevalence among African HCWs to be 6.81% to 8.0% (Atlaw et al., 2021; Maamor et al., 2022), while a seroprevalence study in southern Ghana reported a 5.9% prevalence (Senoo-Dogbey et al., 2023a, 2023b).
To address this risk, the World Health Organization (WHO) and other international bodies recommend three key HBV prevention strategies for HCWs: preexposure prophylaxis (vaccination), postexposure prophylaxis, and adherence to standard precautions (Senoo-Dogbey et al., 2024a). Vaccination is the most effective preventive strategy, offering lifelong immunity to 90% to 95% of immunocompetent individuals who complete the three-dose regimen (Walayat et al., 2015)
Despite its efficacy, HBV vaccination uptake remains inadequate. Globally, only 56.6% of HCWs are fully vaccinated, with the highest rates in urban and high-income countries (Mahamat et al., 2021). In Africa, uptake is critically low at 13.4% (Auta et al., 2018). In Ghana, although 60.9% of HCWs have received at least one dose, only 46.8% have completed the full vaccination schedule (Senoo-Dogbey et al., 2024a). Barriers such as insufficient knowledge, limited vaccine availability, and high costs contribute to low uptake (Ansa et al., 2019; Senoo-Dogbey et al., 2024d). Evidence suggests that HCWs’ knowledge and awareness significantly influence their vaccination behavior (Iova et al., 2023). While several studies have shown a positive relationship between HBV knowledge and preventive practices such as vaccination (Akazong et al., 2020; Belete et al., 2022), none has directly examined the link between knowledge and vaccination intention. Furthermore, most studies were conducted in single institutions, limiting their generalizability. Therefore, a broader, multifacility study using inferential statistics is necessary to explore this relationship.
Given their role in patient education and their high occupational exposure risk (Chen et al., 2019; Coppola et al., 2016), ensuring HCWs are knowledgeable about HBV and its prevention is essential for both self-protection and public health promotion. This study hypothesizes that increased HBV knowledge and awareness of vaccine efficacy will improve HCWs’ intention to vaccinate. Accordingly, a facility-based cross-sectional analytical study was conducted to examine the association between HBV knowledge and vaccination intentions among HCWs in Ghana's Oti Region.
Review of Literature
HBV remains a significant occupational hazard for HCWs, particularly in low- and middle-income countries where the disease burden is highest. Given their frequent exposure to blood and bodily fluids, HCWs are considered a high-risk group for HBV infection (Coppola et al., 2016). As such, international and national health authorities strongly recommend HBV vaccination for all HCWs as a cornerstone of occupational health and safety. The WHO recommends that all HCWs receive a full three-dose HBV vaccination series at 0, 1, and 6 months (WHO, 2024a). The vaccine is highly effective, with more than 90% of immunocompetent individuals achieving protective immunity following completion of the series (Walayat et al., 2015). In addition to vaccination, WHO outlines other preventive measures, including postexposure prophylaxis and adherence to standard precautions to reduce transmission risks.
Despite clear guidelines, vaccination coverage among HCWs remains uneven globally. For instance, a systematic review by Auta et al. (2018) reported that only 56.6% of HCWs globally had completed the full HBV vaccination series, with the lowest coverage observed in African countries (13.4%). Factors contributing to low uptake include vaccine unavailability, cost, lack of institutional support, and poor awareness of HBV risk and vaccine efficacy (Ansa et al., 2019). In Ghana, the national occupational health and safety policy recommends HBV vaccination for all HCWs; however, uptake remains suboptimal. A recent study by Senoo-Dogbey et al. (2024a) revealed that only 46.8% of HCWs had completed the full three-dose regimen, despite relatively high awareness of HBV transmission risks. HBV disease and vaccine knowledge encompasses understanding the disease transmission routes, symptoms, and long-term complications such as liver cirrhosis and cancer. Vaccine knowledge involves familiarity with the HBV vaccine's availability, recommended dosing schedule, and its role in preventing infection.
It also covers perceptions of vaccine safety and effectiveness. Such knowledge is commonly measured using structured questionnaires and knowledge scores.
Assessing HBV knowledge is critical for informing public health interventions and improving vaccination uptake.
Knowledge of HBV plays a critical role in shaping individuals’ intentions to receive the HBV vaccine. Studies consistently show that higher levels of HBV-related knowledge, particularly about transmission risks, disease severity, and vaccine benefits, are positively associated with increased willingness to get vaccinated. Improved knowledge helps dispel misconceptions and reduces vaccine hesitancy, especially in populations with limited access to healthcare information. In contrast, poor knowledge is linked to lower perceived risk and reduced motivation for preventive action (Nguyen et al., 2020). Evidence consistently shows that HCWs with greater knowledge about HBV are more likely to adhere to vaccination recommendations. Several studies have identified a positive correlation between knowledge levels and vaccination behavior. For instance, Akazong et al. (2020) and Belete et al. (2022) demonstrated that HCWs who were better informed about the modes of HBV transmission and consequences were more inclined to complete the vaccination series. This correlation was also supported in a study by Chen et al. (2019), which linked vaccine-specific knowledge to increased uptake of recommended vaccines.
Operational definition of terms:
Materials and Methods
Study Design
The study employed a descriptive cross-sectional study design in the first half of 2021 to determine the relationship or influence of HBV knowledge on HBV vaccination uptake intentions among HCWs in two healthcare facilities in the Oti Region of Ghana.
Research Questions
What is the influence of HBV knowledge on HBV vaccination intentions among HCWs in the Oti Region of Ghana?
Study Setting
This study recruited participants from two secondary-level facilities, namely St. Joseph's Catholic Hospital (SJCH) and Nkwanta-South Municipal Hospitals (NSMH) in the Nkwanta-South Municipality/District. NSMH has a 122-bed capacity and 108 outpatient visits per day. There are 263 HCWs in general, with 120 nurses and midwives, and the rest being physicians, laboratory technicians, radiology technicians, and other auxiliary staff. SJCH provides general healthcare services including internal medicine, maternal and child health, radiology, laboratory, pharmacy, and mortuary services with 238 HCWs in total and 89 nurses and midwives with various ranks.
Study Population
This study was restricted to nurses and midwives only who were working in the two selected facilities within the Oti Region of Ghana. These categories of HCWs were in the majority compared to other cadres of staff. Nurses and midwives spend far more time with patients than other professional categories (Butler et al., 2018), thereby increasing their risk of biological hazards such as HBV. Nurses and midwives contribute 50% to the global workforce and investing in them is imperative to achieve an efficient, effective, sustainable resilient, and sustainable healthcare system (World Health Organization, 2024c). However, the two cadres were operationalized in this study as HCWs based on the WHO classification and the ability of these professionals to provide preventive, curative, and promotive health services to patients in their respective facilities (World Health Organization, 2006)
Inclusion and Exclusion Criteria
HCWs belonging to all ranks and levels of training in the nursing and midwifery profession, working in the selected hospitals, and providing direct patient care services to patients, including those infected with and living with HBV. These professionals are at risk of exposure to blood and body fluids. HCWs with a known positive HBV status were excluded as their HBsAg status does not offer them the opportunity to vaccinate or have. Additionally, student nurses, student midwives, and interns with less than 1 year of experience in a healthcare setting were excluded from the study due to their limited exposure and patient contact.
Sample Size and Sampling Method
The sample size for this study was estimated using the Yamane (1967) formula. Considering a 10% nonresponse rate, a minimum sample size of 190 HCWs was deemed appropriate for this study. The estimated sample size was allocated to the two facilities using a proportional allocation of sample procedure based on average daily outpatient attendance, giving a 45.1% and 54.9% distribution per facility. The HCWs were recruited using a simple random procedure, specifically the lottery method.
Data Collection Tool
A standardized and pretested structured questionnaire was utilized for the data collection. The tool is grounded on literature specific to HBV disease, transmission prevention, treatment, and so on (Shrestha et al., 2020) (Supplemental file). The instrument focused on (a) sociodemographic information (age, sex, marital status, level of education, rank, etc.), (b) knowledge of HBV (e.g., “HBV affects the liver”) and knowledge of HBV vaccine, and (c) HBV vaccination intentions. The questions on knowledge were dichotomous questions which were close-ended and scored as “1” for correct answer and “0” for incorrect answer. The HBV knowledge subsection of the instrument had 15 items. A score of 0–5 was interpreted as poor, 6–10 was fair, and 11–15 was interpreted as good (Senoo-Dogbey, 2022).
The vaccination intention scale had four items also measured as dichotomous variables and scored as “1” for the correct answer and “0” for the incorrect answer. The vaccination intention was assumed to measure prospective intentions HCWs yet to vaccinate against HBV or retrospective (for HCWs who have already received at least one dose of the HBV vaccine). The instrument was pretested among 30 HCWs at Krachi West Municipal Hospital, a facility with the same characteristics as the study sites. The reliability of the instrument was determined after the pretesting, and it was found to be reliable as the overall alpha was 0.82. The instrument's validity was ensured by subjecting it to expert review.
Data Collection Procedure
The administrators and nurse managers of the selected facilities were contacted, and access was granted after all the administrative procedures were completed. Before the data collection began, the ward in-charge was formally notified. The potential participants were then briefed on the purpose of the study as documented clearly on the study's information sheet. The participants were provided with written informed consent forms to sign to indicate their willingness and readiness to be part of the study. Protocols for preventing COVID-19 were strictly followed. Two research assistants were recruited and trained on the consent and questionnaire administration procedures. The instrument was prepared in English and self-administered in all cases in the English language. The HCWs filled out the questionnaires in the nurses’ resting rooms, nurses’ stations, and consulting rooms. The field/research assistants were around to provide support and clarifications for the HCWs during the data collection periods. The answering of the questions took 20–25 min on average.
Data Analysis
The completed surveys were verified for completeness, coded, and entered using IBM SPSS version 23.0 software. To find any erroneous entries or omissions in the data set, frequencies of the data were computed for all the variables. Data cleaning resulted in a total of 160 sample units for data analysis. Categorical variables were summarized using descriptive statistics, and also skewness, kurtosis, mean, and standard deviations were computed for quantitative variables. A reliability test was performed, and Cronbach's alpha was computed and documented. To analyze the relationships between knowledge scale and HBV vaccine uptake intentions, Pearson correlation was utilized, and the correlation coefficient (r) was computed. A linear multiple regression analysis was performed to determine the predictive power of HBV knowledge on HBV vaccination uptake intentions with a level of significance set at .05.
Ethical Considerations
Ethical approval was obtained, and hospital management granted permission for participant recruitment. Participants were informed about the study's purpose, procedures, risks, and benefits, with the right to ask questions before signing the consent form. Voluntary participation, confidentiality, and the right to withdraw without consequences were emphasized. Personal data were de-identified and securely stored, accessible only to authorized personnel.
Results
Sociodemographic Characteristics of Nurses
Data analysis was based on 160 completed questionnaires, yielding a response rate of 84.2%. According to Cook et al. (2009), response rates among HCWs tend to be low and are likely declining. However, the 84% response rate observed in this study exceeds the recommended mean response rate of 52.7 ± 21.2% for surveys targeting individuals, which typically necessitates an explanation of variance (Cook et al., 2009).
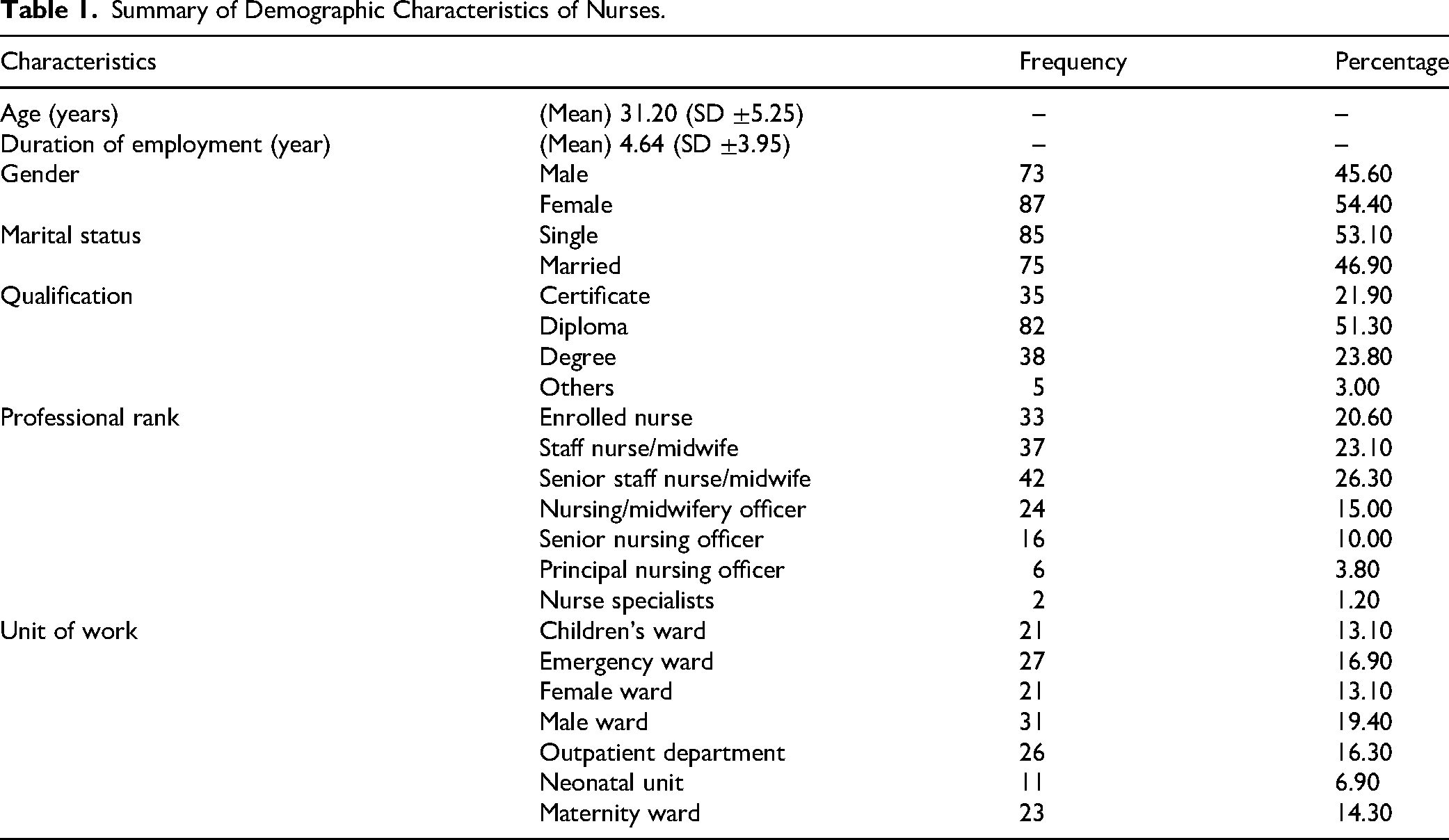
The age of the study participants ranged from 22 to 52 years, with a mean age of 31.20 (SD ±5.25). The duration of employment as a nurse or midwife also ranged from 1 to 22 years, with an average professional working experience of 4.64 (SD ±3.95) years. More female HCWs participated in the study (54.4%). The majority of the HCWs were single (53.1%). Most of the participants were diploma holders (51.3%). All professional nursing and midwifery grades were represented in the study sample, with the majority being senior staff nurses and midwives (26.30%) and working in the male ward (19.40%) (Table 1).
Summary of Demographic Characteristics of Nurses.
Participants’ Knowledge of HBV Infection (Disease, Transmission, Consequences, and Vaccination)
As seen in Table 2, the overwhelming majority of the HCWs correctly answered 12 out of 15 domains or items that assessed HBV knowledge but provided incorrect responses for three out of the domains or items in the knowledge scale (HBV can be spread by sharing eating utensils like spoons, the HBV vaccination is useful for the prevention of HBV infection, and HBV can be prevented by avoiding contaminated water/food). These incorrect responses from the majority of the participants give a clue to the numerous misconceptions about the transmission mechanism of the disease. The incorrect response to the question on the effectiveness of the vaccine also points to the general lack of confidence in the HBV vaccine.
Summary of Knowledge of Hepatitis B and HBV Vaccination of Study Participants.
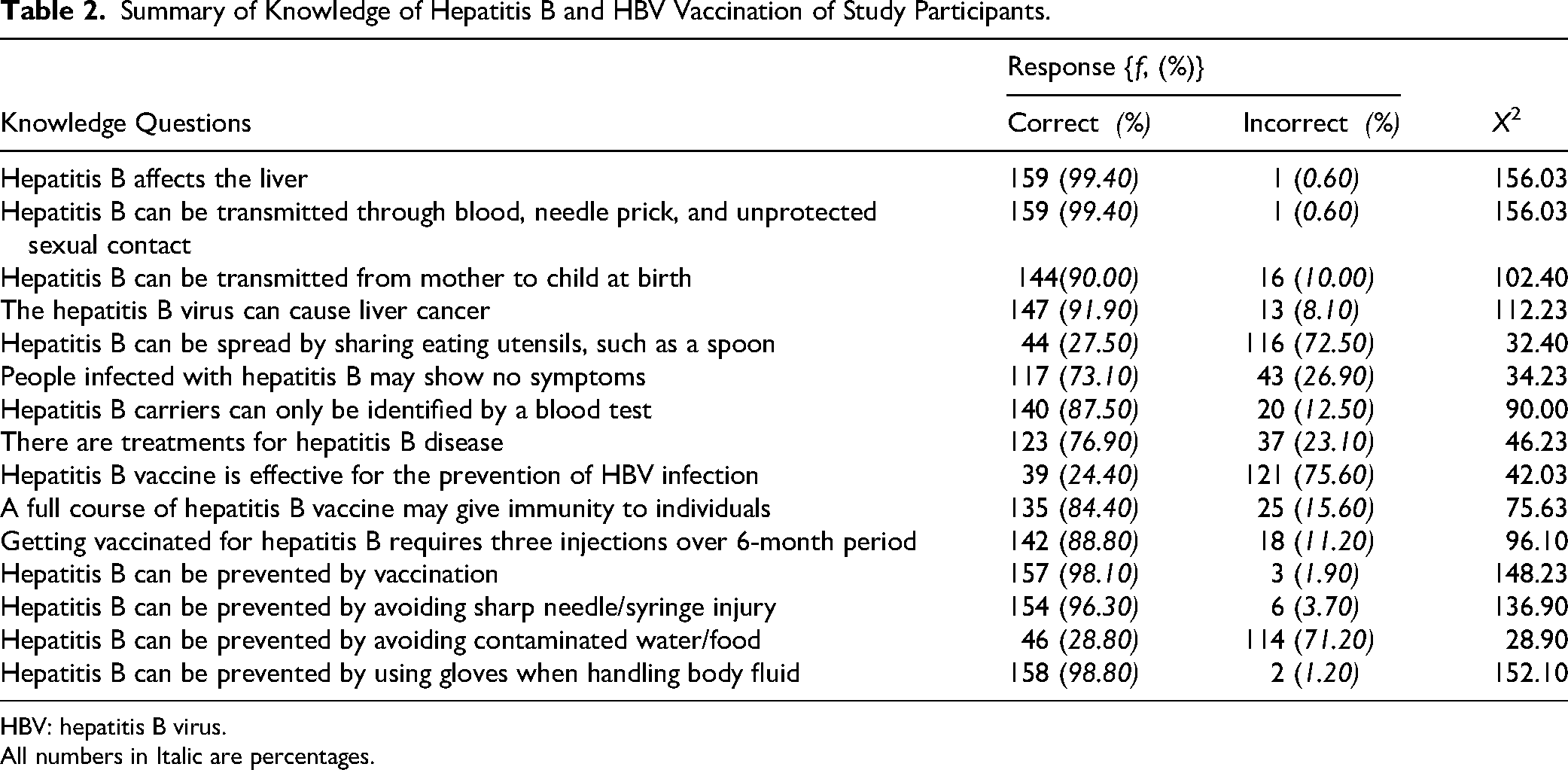
HBV: hepatitis B virus.
All numbers in Italic are percentages.
HCWs Hepatitis B Vaccination Uptake Intentions
The participants’ HBV vaccine uptake intentions (prospective or retrospective intention) were assessed using four items, which assessed a person's willingness to accept, initiate, and receive the recommended number of vaccine doses and subsequently complete the three-dose vaccination cycle. The responses from the participants, as presented in Table 3, indicate that they are willing to receive the vaccine (98.80%) and ready to complete the three-dose vaccination series (100%). This indicates that the participants had a positive HBV vaccination intention.
Assessment of Hepatitis B Vaccination Uptake Intentions.

N = 160.
All numbers in Italic are percentages.
Performance of the HBV Knowledge and HBV Vaccination Uptake Intention Scales
Skewness and kurtosis were used to test for the normality of the responses generated from the two scales. As shown in Table 4, the scores of HBV knowledge and HBV vaccination intentions were both normally distributed, with skewness and kurtosis falling within ±1. The overall reliability coefficient (α) of the questionnaire was .83 (.65 and .96 for knowledge and vaccination intentions, respectively).
Summary of Normality and Reliability Coefficient (α) of the Study Variables.
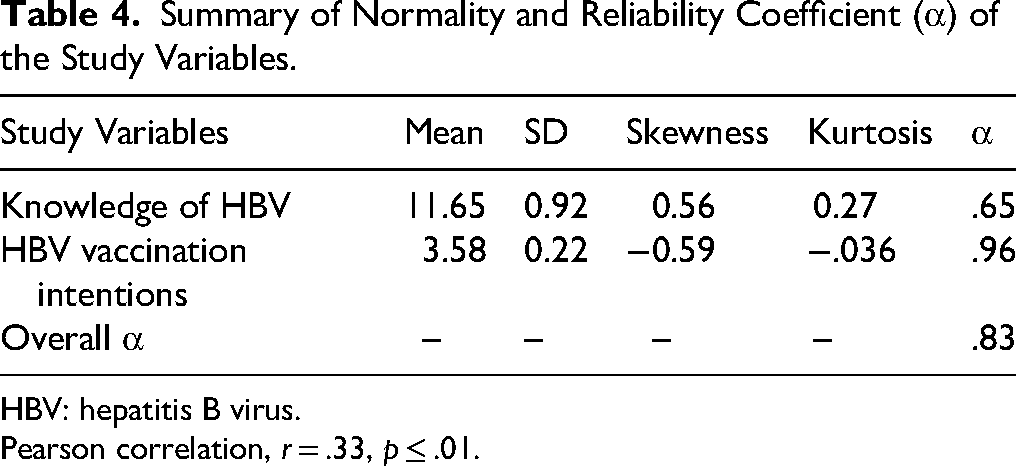
HBV: hepatitis B virus.
Pearson correlation, r = .33, p ≤ .01.
The Pearson correlation analysis, which was performed to determine the correlation between HBV knowledge and HBV vaccination intentions, revealed a positive and significant correlation between participants’ knowledge of HBV and HBV vaccination uptake intention (r = .33, p < .01). This shows that an increase in knowledge of HBV produces a corresponding increase in HBV vaccination uptake.
Influence of HBV Knowledge on HBV Vaccination Uptake Intentions
As presented in Table 5, a linear regression analysis produced a model which was significant (F(2, 157) = 13.55, p = .00, adjusted R2 = .14). Knowledge contributed 14% in explaining the variation of the HBV vaccination uptake intention. The unstandardized B coefficient for knowledge (B = 0.07) explains that as participants’ knowledge increases by one point, their hepatitis B vaccination uptake intentions increase by an additional 0.07 points. This means that for every extra increase in individuals’ knowledge level, there is a corresponding increase in HBV vaccination uptake intentions. The standardized coefficient for knowledge is 0.23, which provides important evidence about how knowledge has performed in predicting HBV vaccination uptake intentions and contributes to the significant model observed. This outcome shows that HBV knowledge predicts participants’ HBV vaccination uptake intentions (β = .23, t = 2.88, p = 0.01).
HBV Knowledge as a Predictor of HBV Vaccination Intentions.

HBV: hepatitis B virus.
Discussion
The study assessed the knowledge of HCWs on hepatitis B and its influence on HBV vaccination intentions in two periurban healthcare facilities in the Oti Region of Ghana. The findings of this study indicated that HCWs had good and satisfactory knowledge of most of the domains assessed by the knowledge scale designed for the study. This finding is consistent with several recent studies that also assessed the level of knowledge of HCWs on HBV disease, its transmission and prevention by use of HBV vaccine (Ajaz et al., 2021; Aniaku et al., 2019; Mursy & Mohamed, 2019; Singh et al., 2020). HCWs are important sources of vaccine information for their patients; thus, having correct vaccine information is essential (Chen et al., 2019). Therefore, the relatively greater knowledge of HBV infection and vaccination among HCWs as recorded in this study may perhaps be due to the increasing awareness being created and publicity that the disease is gaining in the public domain in most endemic countries.
The study was conducted during the peak of the COVID-19 pandemic, a period when HCWs worldwide received extensive training and education on preventing hospital-acquired infections. This heightened awareness, along with strong advocacy for vaccination and preventive measures to reduce occupational exposures, may have contributed to the high levels of knowledge demonstrated by participants in this study.
The finding of this study on knowledge is, however, at variance with some related studies which observed relatively undesirable knowledge of hepatitis B infection, its transmission, and vaccination (Adekanle et al., 2015; Ajaz et al., 2021; Chao et al., 2012). Specifically, Adelenke and colleagues reported in their study that over 33% of participants HCWs had unsatisfactory knowledge of HBV in Nigeria (Adekanle et al., 2015). These observations were attributed to inadequate access to educational materials on hepatitis B disease and inaccurate self-reported activities among the perinatal nurses. Inadequate knowledge by HCWs may result in the transfer of false information to patients and the public. In Ghana, anecdotal evidence suggests that HCWs are seemingly perceived as one of the main sources of health information and possibly need to be abreast with current hepatitis B information. There is therefore the need to enhance HBV knowledge and vaccine information for nurses.
This study observed a positive HBV vaccination uptake intention among the participants, with an overwhelming majority accepting to take the vaccine, return for the second and third doses and complete the vaccination series. This observation is a little divergent from what has been reported among Ghanaian HCWs that only 60.9% received at least one dose of the HBV vaccine and 46.7% completed the three-dose vaccination series (Senoo-Dogbey et al., 2024a). This disparity in HBV vaccination intention and actual vaccination behavior is an indication of a gap in HBV vaccination uptake intentions and actual vaccination practice. This is also a clear indication that HBV vaccination intentions did not translate into actual practice. Complete vaccination against HBV measured by the receipt of three vaccine doses at the recommended schedule is important for the development of protective immunity against HBV (Senoo-Dogbey et al., 2024d) therefore HCWs need to be supported by instituting measures that are tailored to removing structural or institutional level as well as personal level barriers to optimal HBV vaccination to help these at-risk population translate vaccine uptake intentions to optimum vaccination practice.
Additionally, this study revealed that HBV knowledge had a positive and significant correlation with HCWs’ HBV vaccination uptake intention, and this is consistent with a study from the United States (Chao et al., 2015). This finding implies that adequate knowledge could determine HBV vaccination uptake intentions among HCWs. This finding agrees with a study that documented that generally, the vaccination intentions of HCWs are determined by their knowledge of the recommended vaccines such as HBV, influenza, measles, mumps, rubella, varicella, and diphtheria, tetanus, pertussis vaccines (Chen et al., 2019). In that study, the researchers further reported that knowledge about vaccination is critical for maintaining good vaccination uptake and HCWs’ commitment to providing vaccination information to vulnerable patient groups and high-risk persons.
Strengths and Limitations of the Study
This study employs simple random sampling to minimize selection bias and ensure representativeness. By examining HBV knowledge and vaccination intentions among HCWs, the study addresses a critical public health issue. Conducting the study in two healthcare facilities enhances the relevance of the findings. The results can inform targeted interventions to improve HBV vaccination uptake and HBV infection control.
This study has some limitations. The initial sample size was 190, but only 160 participants took part. The study only included trained nurses and midwives, excluding students and HBV-positive individuals. This limits the generalizability of the results to a broader population. The study was confined to two healthcare facilities in Ghana's Oti Region. This geographical restriction may limit the applicability of the findings to other settings. The reliance on self-administered questionnaires may introduce response bias. Participants may provide socially desirable answers rather than accurate reflections of their knowledge and intentions. The study did not control for other covariates such as vaccination status and sociodemographic variables, and the authors admit this as a limitation. These limitations should be considered when interpreting the study's findings.
Novelty and Contributions to Knowledge
This study is probably the first empirical link between HBV knowledge and vaccination intentions in Ghanaian HCWs. While many prior studies have assessed HBV knowledge and vaccination status separately, this study is one of the first in Ghana and among very few globally to quantitatively examine the predictive relationship between knowledge of HBV and vaccination uptake intentions among HCWs. This study bridges an important gap between knowledge and behavioral intention in occupational health research.
Implications/Recommendations for Practice and Research
The positive correlation between HBV knowledge and vaccination intentions in this study highlights the critical role of health education in improving vaccine uptake. Public health practitioners should prioritize culturally and linguistically tailored educational interventions to increase awareness of HBV transmission, risks, and the benefits of vaccination.
Future research should examine the relationship between HCWs’ vaccination status and their knowledge of HBV, as this could inform targeted vaccination campaigns. Additionally, studies should investigate differences in knowledge of HBV vaccine uptake intentions based on demographic and professional characteristics. Identifying knowledge gaps within specific subgroups will help design tailored interventions. Such research could improve strategies to increase vaccine uptake.
Conclusion
HCWs who participated in this study demonstrated adequate knowledge of HBV infection and HBV vaccine. The study also observed that the participants had positive intentions for accepting the HBV vaccine, receiving the second and third doses and completing the three-cycle vaccination series. HBV knowledge correlated linearly and positively with HBV vaccination. Knowledge of HBV had a positive influence on HCWs’ HBV vaccination uptake intentions such that a unit increase in knowledge produced a corresponding increase in HBV vaccination uptake intentions. This study has highlighted the importance of HBV knowledge and literacy in promoting HCWs’ HBV vaccination uptake. In highly endemic areas where HCWs’ HBV vaccination uptake is suboptimal, facility managers, health policymakers, and stakeholders should endorse education of all cadres of HCWs on HBV disease, its transmission and the severity of consequences as well as information on the efficacy of the HBV vaccine. This strategy could promote HBV vaccination uptake intentions and subsequently translate into positive HBV vaccination behavior and practice.
Supplemental Material
sj-docx-1-son-10.1177_23779608251352409 - Supplemental material for Hepatitis B Virus Infection Knowledge as a Predictor of Vaccination Uptake Intentions Among Healthcare Workers in the Oti Region, Ghana
Supplemental material, sj-docx-1-son-10.1177_23779608251352409 for Hepatitis B Virus Infection Knowledge as a Predictor of Vaccination Uptake Intentions Among Healthcare Workers in the Oti Region, Ghana by Solomon Tagbor, Lillian Akorfa Ohene, Charles Ampong Adjei, Vivian Efua Senoo-Dogbey and Josephine Mpomaa Kyei in SAGE Open Nursing
Supplemental Material
sj-docx-2-son-10.1177_23779608251352409 - Supplemental material for Hepatitis B Virus Infection Knowledge as a Predictor of Vaccination Uptake Intentions Among Healthcare Workers in the Oti Region, Ghana
Supplemental material, sj-docx-2-son-10.1177_23779608251352409 for Hepatitis B Virus Infection Knowledge as a Predictor of Vaccination Uptake Intentions Among Healthcare Workers in the Oti Region, Ghana by Solomon Tagbor, Lillian Akorfa Ohene, Charles Ampong Adjei, Vivian Efua Senoo-Dogbey and Josephine Mpomaa Kyei in SAGE Open Nursing
Footnotes
Acknowledgments
The authors are most grateful to all the healthcare workers who voluntarily participated in the study.
Ethical Considerations
Ethical approval was obtained from the Ghana Health Service Ethical Review Committee (GH-ERC-041/09/20), and hospital management granted permission for participant recruitment. Participants were informed about the study's purpose, procedures, risks, and benefits, with the right to ask questions before signing the consent form. Voluntary participation, confidentiality, and the right to withdraw without consequences were emphasized. Personal data were de-identified and securely stored, accessible only to authorized personnel. The management of the two municipal hospitals was contacted for study area approval before participant recruitment began. Following a thorough description of the study's goal, the participants were allowed to sign the consent form after a thorough explanation of the study's goals, procedures risks, and benefits were clarified. The right to withdraw or discontinue from the study as well as the right to refuse participation were respected. Privacy and anonymity were upheld throughout the data collection, analysis, and dissemination phases of the project.
Author Contributions
S.T.: conceptualization, methodology, data collection, data analysis, writing—original draft, and preparation of manuscript. L.A.O. and C.A.A.: methodology, supervision, writing—original draft, and preparation of manuscript. V.S.-D. and J.M.K.: methodology, supervision, writing—original draft, and preparation of manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data on which this study's conclusions were drawn have been published in this document as the results/findings of the study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.