
Abstract
Background
Due to the rapid spread of monkeypox (Mpox), raising public awareness, ensuring effective information dissemination, and early monitoring of public health are crucial in controlling its transmission.
Objectives
The aim of this study was to assess knowledge, attitude, and associated factors towards Mpox infection among residents.
Method
A community-based cross-sectional study was conducted from August 17 to September 15, 2024, targeting local residents using a simple random sampling technique. A total sample size of 403 was calculated using a single population proportion formula. Data on Mpox-related knowledge, attitudes, and various socio-demographic factors were collected from the participants. Binary and multivariate logistic regression analyses were employed to identify factors associated with knowledge and attitudes toward Mpox.
Result
A total of 403 subjects were recruited for this study, with a mean age of 39.73 ± 11.22 (SD) years. Among the participants, 33.7% demonstrated good knowledge of Mpox, while 57.3% exhibited positive attitudes toward the disease. Key factors were identified which significantly affect the knowledge of residents including age (adjusted odds ratio (AOR):0.262, confidence interval (CI):0.100–0.685, p = 0.006), level of education (AOR:0.603, CI: 0.328–1.108, p = 0.001), marital status (AOR:1.151, CI:0.357–3.758, p = 0.029), and source of information (AOR: 1.164, CI:0.543 −2.495, p = 0.043). In same vein, the variables include, occupation, sex and educational status were significantly influencing resident's attitude.
Conclusion
This study revealed that overall knowledge about Mpox among residents was low. However, reasonable level of public attitude was identified. Overall, equitable public health interventions are needed to enhance public understanding and attitudes toward Mpox.
Background
Monkeypox (Mpox) is a viral zoonotic disease, a member of the Orthopoxvirus genus, first discovered in 1958 in Copenhagen, Denmark (Ladnyj et al., 1972). Later on, it was frequently reported in Central and West African countries and has since spread globally (Dou et al., 2023; Huang et al., 2022). The virus is primarily harbored in animals, such as rodents, and can be transmitted to humans through direct contact (Orok et al., 2024). Human-to-human transmission occurs primarily through close contact with an infected individual, with respiratory secretions and lesions of infected individuals considered the most likely routes, especially in densely populated areas (Mileto et al., 2022; Wang & Lun, 2023). Apart from clinical resemblance to smallpox, Mpox manifests with fever, a characteristic rash, lymphadenopathy, and myalgia (Aynalem et al., 2024; Bunge et al., 2022; Hoff et al., 2017).
Mpox has become a public health concern across different regions of the world, including Europe and North America, apart from the endemic region (Dou et al., 2023; Endo et al., 2022). Since 2022, WHO has declared it a global outbreak and public health emergency, emphasizing the need for urgent intervention (WHO, 2022). As of June 2023, an estimated 87,792 cases have been reported globally, resulting in 147 deaths (WHO). Of these cases, 59,480 were reported in the Americas, 25,912 in Europe, 1,741 in Africa, and 84 in the Southeast Asia region (Jahromi et al., 2024). This highlights the need for assessing the community's knowledge, attitudes, and preventive practices to implement targeted intervention early. Due to the greater risk, it presents for populations, especially children, pregnant women, and individuals with compromised immune systems(Velavan & Meyer, 2022), further research should be conducted specifically in regions with poor socioeconomic and healthcare services.
Studies have reported a widespread lack of knowledge about Mpox among the population, particularly among healthcare professionals (HCPs), which could hinder infection control efforts. For example, low levels of knowledge were found among general practitioners in Indonesia (10%), doctors in Bangladesh (30.59%), and community members in Turkey (37.7%) (Arayici et al., 2025; Harapan et al., 2020; Hasan et al., 2023). Another study in Ethiopia revealed that only 28.13% of participants demonstrated good knowledge, and 37.76% exhibited favorable attitudes toward Mpox (Kiros et al., 2025). Furthermore, a recent study conducted among HCPs at the University of Gondar Comprehensive and Specialized Hospital revealed that less than half demonstrated good knowledge (48.4%) and positive attitudes (49.2%) (Beyna et al., 2025). This poor level of understanding and attitude imposes a significant burden on healthcare systems, increasing associated costs. Therefore, this rapidly growing viral disease must be addressed with early population awareness.
To effectively control the disease, the community's level of awareness and attitude must be assessed to implement early measures. Public awareness and attitude towards Mpox symptoms, transmission routes, and mitigation methods heavily impact public health strategies, including timely diagnosis, isolation protocols, and risk communication (F. Amer et al., 2023). To date, no community-based studies have been conducted to assess the knowledge and attitudes regarding Mpox among communities in Ethiopia or most regions of Africa. In resource-limited countries, the spread of the virus is exacerbated by poor hygiene practices, close contact with animals, and other socioeconomic factors. Moreover, the current study area, Bahir Dar city, is the capital of the Amhara regional state, located near Lake Tana, a popular destination of tourists and is therefore probably exposed to various zoonotic diseases. Hence, the present study was designed and conducted to assess the knowledge, attitudes, and associated factors related to Mpox infection among residents in Bahir Dar city, Northwest Ethiopia, in 2024.
Literature Review
While most research on Mpox has identified a significant gap in understanding this viral infection, the majority has focused on HCPs. Knowledge rates among HCPs in studies conducted in the United States of America (Bates & Knowledge, 2022), University of Gondar (Beyna et al., 2025), Injibara University (Aynalem et al., 2024), Nigeria (Orok et al., 2024), and Syria (Al-Deeb et al., 2025) were 40%, 48.4%, 38.5%, 22.5%, and 41.1%, respectively. Despite the commandability of research focused on HCPs, considering community members is also important for enhancing their perception of Mpox. Studies conducted in Turkey (37.7%), Malaysia (25.5%), and Saudi Arabia (48%), less than half of general public's demonstrate good knowledge of Mpox (Alshahrani, Alzahrani, et al. 2022; Arayici et al., 2025; Kumareswaran et al., 2022). Meanwhile, some studies for instance, peoples in Nepal (53.8%), China (56.5%), and Nigeria (58.7%) showed good knowledge about noted viral disease (Al-Mustapha et al., 2023; Das et al., 2024; Ren et al., 2023).
Within the existing body of knowledge on Mpox, only a limited number of studies have examined public attitudes. Fewer than half of the individuals surveyed in Pakistan and Iraq expressed a positive attitude towards the disease (Chandran et al., 2022; Hafeez et al., 2024). Such a low proportion of positive attitude towards Mpox within the population needs urgent intervention. Given the lack of community-based studies on Mpox in Ethiopia, the present study aimed to uncover significant gaps in knowledge and attitudes among community members.
Methods
Study Design, Area and Period
A community-based cross-sectional survey was conducted from August 17 to September 15, 2024, among residents at Bahir Dar city. Bahir Dar is a capital city of Amhara regional state, located 563 km far from Addis Abeba, capital of Ethiopia.
Populations
The source population includes residents living in Bahir Dar city, while the study population consists of individuals who were randomly allocated and recruited for this study.
Inclusion and Exclusion Criteria
The study recruited community members (residents) aged 18 years and above who had lived in the area for at least six months and were willing to participate voluntarily. However, residents with any psychiatric illness, hearing loss or those who refused to complete the survey were excluded from the study. As individuals with psychiatric illness or hearing loss might have challenges in obtaining accurate data.
Sample Size Determination
The Raosoft sample size calculator was used to determine the sample size. The total population of Bahir Dar is estimated to be 332,865, based on the recent data (CSA, 2021). No prior studies have been conducted to evaluate general public's knowledge and attitudes regarding Mpox infection in Ethiopia. Consequently, we employed a 95% confidence level, a 5% margin of error, and assumed a population proportion of 50%. Based on these parameters, the representative sample size was calculated to be 384. Accounting for a 5% non-response rate, the final sample size was adjusted to 403.
The study area, Bahir Dar city, comprised six sub-cities and 26 kebeles. For this study, three sub-cities; Fasilo, Gisha Abay, and Tana were randomly selected. Thereafter, two kebeles from each of these sub-cities were chosen using a lottery method. These included the 02 and 03 kebeles from Fasilo sub-city, Abinet and Hidasse kebeles from Gisha Abay, and Shimbet and Ras Agez kebeles from Tana sub-city. Afterwards, households were recruited using a simple random sampling method to ensure all households had an equal chance of being selected (Ahmed, 2024). This sampling approach to involve households was employed due to the difficulty in obtaining recent household lists from most administrative kebele offices, as reported by the officials. Within each household, the one study participants were selected with lottery method regardless of family size to minimize response biases. In each selected kebele, one major street was taken as a reference or starting point to avoid dual recruitments of households.
Data Collection Tools, and Procedures
Data collection was carried out using a structured questionnaire adapted from previously published articles, with necessary modifications made to ensure alignment with the study's objectives (Al-Mustapha et al., 2023; Aynalem et al., 2024; Geremew et al., 2022; Harapan et al., 2020; Hasan et al., 2023). The reproducibility of this questionnaire was validated by three research experts.
Initially, the instrument was developed in English and subsequently translated into Amharic, the language spoken by the study participants, prior to the commencement of data collection. To ensure consistency in data collection, it was back-translated into English. This language translation was done by two bilingual speaker experts. Before starting survey, participants were asked to provide their informed consent, affirming their willingness to take part. The written informed consent document thoroughly detailed the study's objectives and purpose and obtained the necessary signatures. In cases where participants were illiterate, informed consent was obtained through their representatives (assigned by respondents), who were responsible for explaining the details of the study and ensuring that the participants fully understood the information conveyed. The data collection process then commenced once their responses were received. Each study participant was interviewed face-to-face to reduce response biases through clarify unclear points.
The questionnaire was divided into three sections: socio-demographic characteristics, knowledge, and attitude. This tool contained a total of 29 items, distributed across a socio-demographic section (7 items), a knowledge section (16 items), and an attitude section (6 items). For the knowledge part, respondents had two possible answers: “Yes” or “No”, which were scored as 1 and 0, respectively. Respondents who correctly answered 50% or more of the questions were classified as having a good level of knowledge. In terms of attitude, a five-point Likert scale was employed, with response options including “Strongly Agree,” “Agree,” “Neutral,” “Disagree,” and “Strongly Disagree.” These responses were assigned values as follows: “Strongly Agree” received 5 points, “Agree” 4 points, “Neutral” 3 points, “Disagree” 2 points, and “Strongly Disagree” 1 point. The total attitude scores ranged from 6 to 30 points, calculated by adding scores together. Individuals scoring half or more of the maximum possible score were considered to have a positive attitude towards Mpox, as defined in the operational definition.
Data Quality Control
The researchers explicitly clarified for the study participants about the purpose of the study and the data abstraction tool during data collection periods. After the data were checked for completeness, they were entered and analyzed. Pre-tests were conducted in the 5% of the study population outside study area to ensure the completeness of the data abstraction format. The respondents used for the pre-test were excluded from the final analyses. This enabled us to notice conceivable shortcomings of the methodology and data collection tool. Data collection was carried out by two well-trained fifth-year pharmacy students under the supervision of one experienced supervisor. The principal investigator and supervisor meticulously monitored the data collection process, providing critical feedback to the data collectors as needed. This entire process was coordinated by the principal investigator in collaboration with the co-authors.
Operational Definition
Data Processing and Analysis
SPSS Version 22 was used to analyze the data. The results were displayed using textual summaries, figures, and tabular presentations, while descriptive statistics such as the mean, standard error of the mean, frequency, and percentages (%) were used to describe the characteristics of the study participants. Multicollinearity was examined through the variance inflation factor (VIF), and no significant correlations among the independent variables were detected, with all VIF values being less than 1.5. Binary and multivariate logistic regression analyses were conducted to identify factors influencing participants’ knowledge and attitudes toward Mpox infection. In the binary logistic regression, predictors with a p-value < 0.25 at a 95% confidence interval (CI) were deemed potential candidates for inclusion in the multivariate regression. Subsequently, all candidate variables were adjusted in the multivariate analysis, with adjusted odds ratios (AORs) and 95% CI calculated to identify variables independently associated with knowledge and attitudes. The Hosmer–Lemeshow goodness-of-fit test was also conducted to assess the adequacy of the models, yielding p-values of 0.326 and 0.146 for the knowledge and attitude sections of the Mpox analysis, respectively. In the final multivariate model, predictors with a p-value < 0.05 were considered to have statistically significant associations.
Result
Socio-Demographic Characteristics of the Study Participants
In this study, more than half (53.3%) of respondents were males, engaged in secondary education (32.3%), employed (25.3%), and married (56.3%). One hundred and five participants reported that their primary source of information on Mpox was the internet or social media, followed by television or radio. The mean age of the respondents was 39.727 ± 11.22(SD) years. The socio-demographic characteristics and other relevant details are presented in Table 1.
Socio-Demographic Characteristics of Community Members (Residents), 2024 (n = 403).

Knowledge About Monkeypox Infection
This study showed that 33.7% of participants demonstrated good knowledge of Mpox (Figure 1). Among the surveyed residents, 39.7% correctly identified Mpox infection as a viral disorder, while 28 (59.6%) believed it was not prevalent in Western and Central Africa. Furthermore, 60.5% did not recognize that Mpox could lead to stillbirths in infected pregnant women. Similarly, 245 (60.8%) failed to identify flu-like symptoms as common clinical signs of the infection. Conversely, 38.2% of respondents were aware that Mpox can be prevented through specific preventive measures (Table 2).
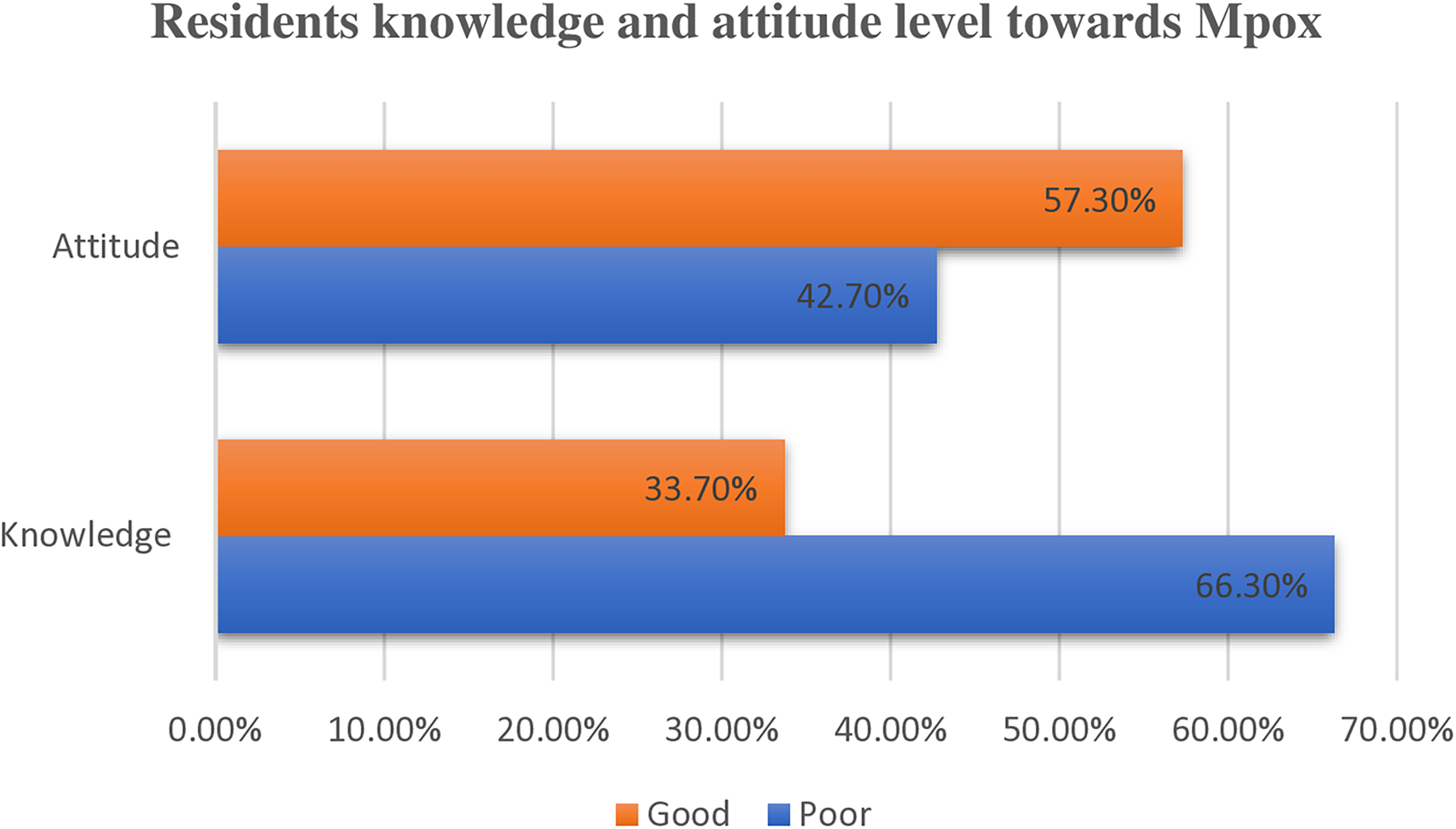
Overall Knowledge and Attitude Towards Monkeypox Among Residents 2024 (n = 403).
Resident's Response to Knowledge Questions About Mpox, 2024 (n = 403).
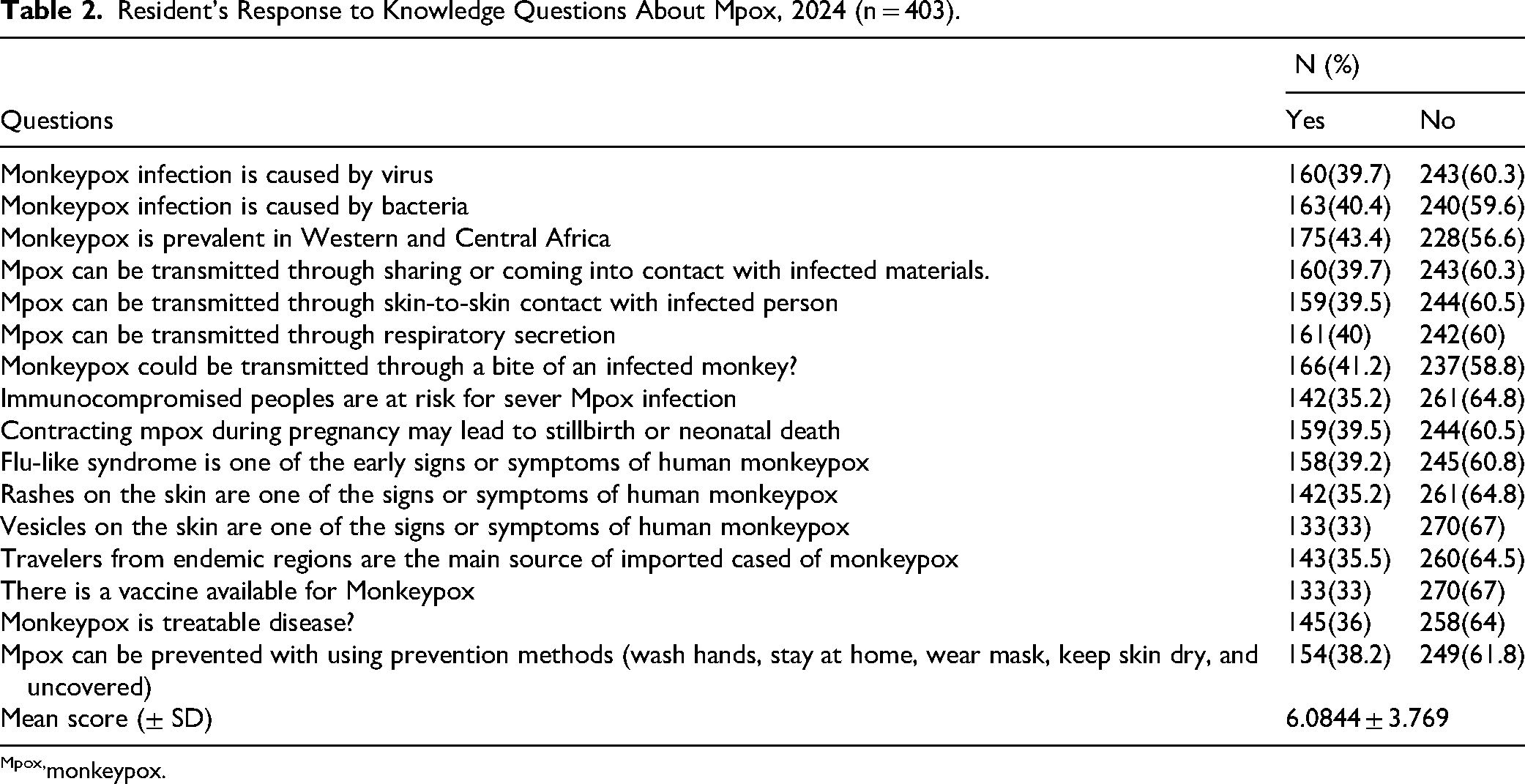
monkeypox.
Factors Associated with Knowledge Toward Monkeypox
In this study, binary and multivariate logistic regressions were computed to examine the association between independent variables and knowledge towards Mpox. The bivariate regression analysis indicated that sex, level of education, age, occupation, marital status, and source of information were statistically associated with knowledge of mpox (p< 0.25). Upon further adjustment of these variables using multivariate logistic regression analysis, sex, age, educational level, and source of information showed a significant association with knowledge (p < 0.05). This study demonstrated that male participants were more likely to possess good knowledge than their female counterparts (AOR = 0.56, 95% CI: 0.349–0.903, p = 0.017). Similarly, the odds of having good knowledge on Mpox infection were 1.151 times higher in married participants (AOR = 1.151, 95% CI = 0.357, 3.758, p = 0.029) compared to single participants (Table 3).
Multivariable Logistic Regression Analysis on Factors Associated with Knowledge Towards Mpox among Residents, 2024 (n = 403).

AOR, adjusted odds ratio; CI, confidence interval; Mpox, monkeypox.
Attitudes Towards Monkeypox Infection
The study showed that 57.3% (95% CI: 52.6–62%) of the study participants had a positive attitude towards Mpox infection (Figure 1). A portion of participants (17.4%) strongly agreed that the Mpox outbreak is a major public health concern, and 17.9% expressed a strong willingness to receive the vaccine. However, 99 participants (24.6%) strongly disagreed with awareness campaigns in Ethiopia (Figure 2).
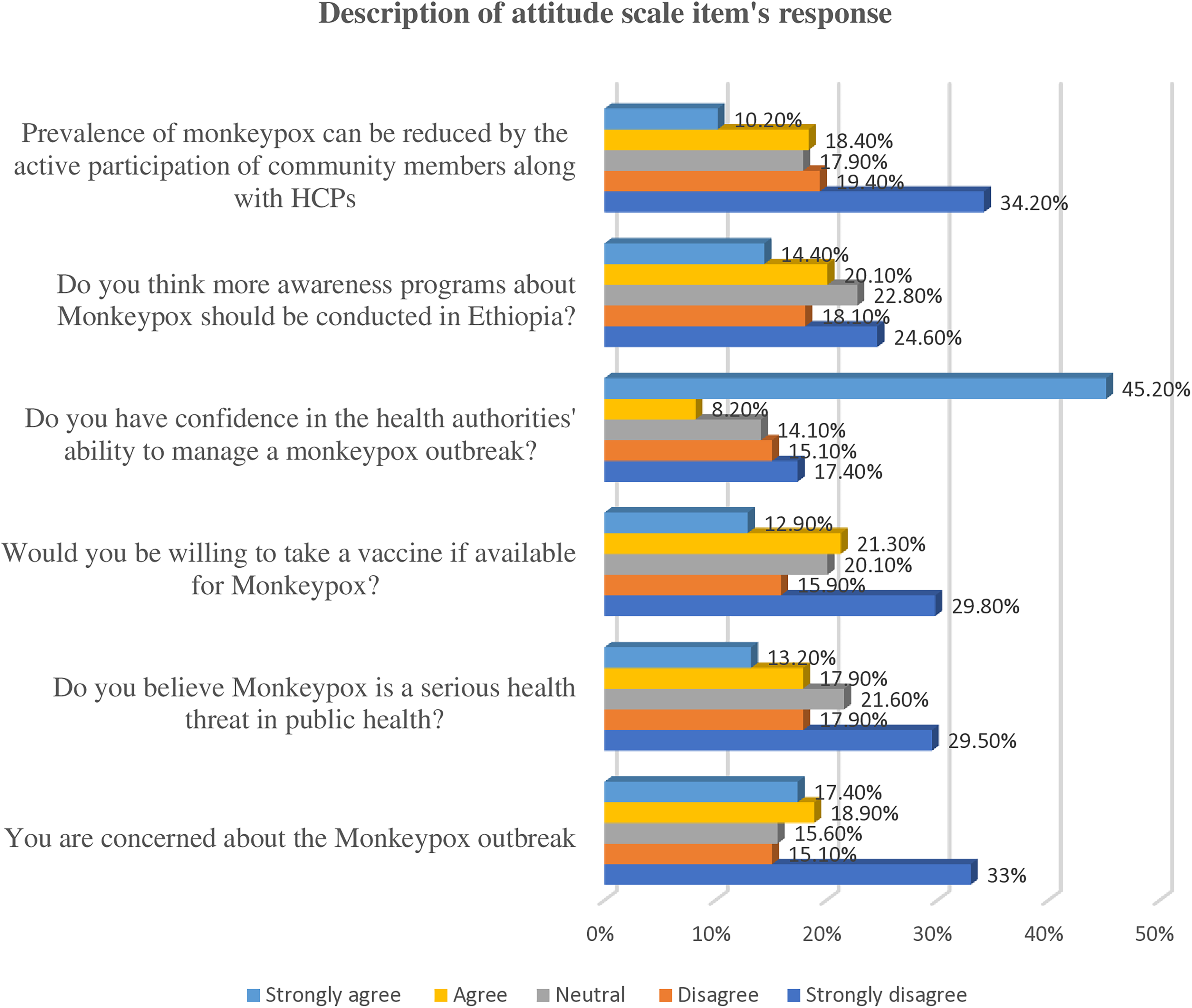
Description of Respondent's Attitude Scale Items Towards Mpox Among Residents, 2024 (n = 403).
Factors Associated with Attitude Toward Monkeypox
In the binary logistic regression analysis, sex, education, occupation, and age were found to be statistically associated with attitudes towards Mpox (p < 0.25). After adjusting these variables using multivariate regression, sex, age, and occupation remained significant predictors of residents’ attitudes towards Mpox. Hence, the odds of having positive attitude towards Mpox were 2.226 times higher in respondents aged50 years old and above compared to those ≤29 years old (AOR = 2.226, 95% CI = 1.017–4.872, p = 0.045). In same vein, jobseekers were found to be 2.461 times more likely to have a positive attitude toward Mpox than housemaids (AOR = 2.461, 95% CI = 0.897–6.754, p = 0.008) Table 4.
Multivariable Logistic Regression Analysis on Factors Associated with Attitude Towards Mpox among Residents, 2024 (n = 403).

AOR, adjusted odds ratio; CI, confidence interval; Mpox, monkeypox.
Discussion
Though no confirmed Mpox infections have been reported in Ethiopia, the country is vulnerable to the disease due to poor hygiene practices, low socioeconomic status, and people's tendency to live with animals. Additionally, Ethiopia is a major tourist destination, and limited access to healthcare exacerbates the spread of such zoonotic diseases (Alemu et al., 2023). Therefore, early assessments of community's knowledge and attitudes are vital in Ethiopia because the healthcare workforce density remains low to effectively combat such viral infections, and healthcare access is insufficient (Haileamlak, 2018). As the first community-based study of its kind in Ethiopia, the findings provide valuable insights that could address existing gaps and inform targeted interventions for potential Mpox outbreaks.
The present study demonstrated that 33.7% of community members had good knowledge of Mpox. The result concurred with the findings among HCPs in Lebanon (30.7%), Pakistan (34.4%), Indonesia (32.5%), and community members in Pakistan (34.4%) (Arayici et al., 2025; Harapan et al., 2020; Jamil et al., 2023; Malaeb et al., 2023). However, our finding notably higher than studies conducted in Nigeria which reported 22.5% of HCPs exhibited good knowledge about Mpox (Orok et al., 2024). Conversely, our finding was lower than those reported in Vietnam and Saudi Arabia (Alshahrani, Algethami, et al. 2022; Nguyen et al., 2024). These discrepancies may be attributed to differences in educational qualifications, access to information, and study populations. Many previous studies focused on HCPs, who are likely to have more up-to-date health information. The present study, however, targeted the general public, who may primarily rely on information disseminated through social media. This was supported by the fact that the majority (26.1%) of participants reported learning about Mpox through the internet or social media. The cut-off of points for the knowledge and study area could be the additional factors contributed to these knowledge variations.
This study identified key disparities in Mpox knowledge based on independent variables such as sex, age, educational level, and source of information. Participants aged 30–39 demonstrated good Mpox knowledge, consistent with studies in Turkey, Egypt, and Jordan, which found higher health literacy rates in this age group (AlBalas et al., 2024; Amer et al., 2024; Arayici et al., 2025). Furthermore, recent research at Debre Tabor University showed that younger participants also possessed good Mpox knowledge (Kiros et al., 2025). This suggests that participants in this study, a substantial number of whom were young, benefited from age-targeted interventional training. A surprising finding was that males demonstrated better mpox knowledge than females, concurred with study reported in Turkey (Arayici et al., 2025). This difference may stem from cultural beliefs or varying levels of involvement in public health topics. While documented gender-based differences in public health knowledge exist, health campaigns should prioritize and empower women through targeted health education initiatives (Molla et al., 2023). In Ethiopia, traditional gender roles often confine women to domestic responsibilities, limiting their access to public health training and potentially contributing to lower levels of Mpox understanding (Kifetew, 2006). In addition, women are commonly viewed as caregivers, homemakers, and nurturers, with less emphasis on formal education or leadership roles in many communities in Ethiopia (BONSA, 2018). This likely impacted the women's knowledge of Mpox in this study. Similarly, educational qualification also significantly affected the knowledge status of the respondents. Individuals with college or higher education demonstrated better Mpox knowledge compared to those who were illiterate or had completed only primary or secondary education. The finding is consistent with studies conducted in Lebanon and Nigeria (Malaeb et al., 2023; Orok et al., 2024). This result was not surprising, as respondents with higher educational attainment may have been more engaged in various research projects, training sessions, and conferences or lectures, especially those focused on Mpox. To update the knowledge of the rest of the population, collaborative efforts are essential. The government, health professionals, and other stakeholders should direct their attention to the general public to facilitate early prevention, screening, and the application of Mpox control measures. This approach could also help reduce the patient burden in regions with limited healthcare access, such as Ethiopia.
The source of information was identified as another factor affecting respondents’ knowledge, in line with the finding in Turkey (Arayici et al., 2025). Respondents who obtained information about Mpox via TV/radio had higher odds of having better knowledge. The results showed that TV and radio were the most common sources of information in the communities, surpassed only by the internet and social media. Therefore, it is recommended that any concerned organization disseminate health and related information through these credible channels. This finding highlights the predominant influence of digital sources of information compared to traditional methods like formal education. This could be due to the widespread access to TV/radio and limited interaction with health professionals in low socioeconomic countries.
This study showed that, 57.3% (95% CI: 52.6–62%) had a positive attitude toward Mpox, a finding that aligns closely with a study conducted in Ethiopia (Aynalem et al., 2024), where 62% reported a positive attitude. On the other hand, the findings of this study were lower than those reported in studies conducted among physicians in Bangladesh, (Hasan et al., 2023), Ohio, and USA (Bates & Grijalva, 2022). This difference is likely because physicians are often at the forefront of access to up-to-date information. However, despite this generally positive perspective, fewer than half expressed concern about a potential Mpox outbreak or considered it a serious public health threat. The study underscores the need for increased public awareness, as most respondents indicated the importance of such efforts. This is further supported by the fact that only 12.9% of participants strongly agreed to receive a vaccine to mitigate the spread of this re-emerging disease.
Different factors affect residents’ attitudes toward Mpox. In this study, multivariate regression analysis demonstrated that factors such as sex, age, and occupation are positively associated with attitudes consistent with the research conducted among nurses in Bangladesh (Rony et al., 2023). Specifically, individuals aged 30 and above were found to have a more positive attitude toward Mpox compared to its counterparts. This suggests that as people age, they tend to develop higher levels of critical thinking, gain more experience, and become more open-minded and receptive to new information. Likewise, subjects engaged in various occupations were more likely to have positive attitudes compared to those working as housemaids. This could indicate a greater interest in combating disease progression, as some participants supposed to participate actively collaborating with HCPs. Although men were about 1.3 times more likely to exhibit a positive attitude, the reasons for this are not entirely clear. The present finding concurred with study in Nigeria (Orok et al., 2024). Further research is needed to explore the underlying factors behind this difference. Sociocultural beliefs in Ethiopia may influence attitudes of women, as they are often not as empowered as men. Additionally, information access, community engagement, and health literacy might have effect on attitudinal disparities in this study.
Strengths and Limitations
The present study aimed to investigate public knowledge and attitudes towards Mpox. As the first of its kind in Ethiopia to assess public knowledge and attitude about Mpox, it identified a significant gap and has implications for policymakers to implement targeted interventions. For future researchers, the findings of this study provide insights and encourage further in-depth research. Nevertheless, this study has certain shortcomings. Its cross-sectional design limits the ability to assess cause-and-effect relationships. Other limitations include the non-representative nature of the small sample size, the reliance on face-to-face interview which may have tendencies toward social desirability bias, interviewer dependency of the respondents and its single-center nature, potentially limiting the generalizability. The temporal nature of the study is also considered a basic limitation. Therefore, future researchers should address these limitations and control for confounders to achieve better outcomes.
Conclusion
This study revealed that the overall knowledge about Mpox among residents was suboptimal, emphasizing the need for targeted and equitable public health interventions. Factors such as sex, age, educational level, occupation, and marital status were found to affect the knowledge and attitudes of participants. It is encouraging that more than half of the respondents showed a positive attitude. However, certain limitations in respondents’ perceptions were identified, highlighting the need to bridge the gap in awareness and public perception of Mpox. Ensuring public awareness and updating the public's attitude levels can help effectively prevent and control the disease, ultimately reducing the disease burden if it occurs. This could be achieved by facilitating outreach public health programs, especially for uneducated people, and disseminating Mpox-related information using mainstream media in collaboration with healthcare providers and other responsible stakeholders.
Supplemental Material
sj-doc-1-son-10.1177_23779608251352392 - Supplemental material for Assessment of Knowledge, Attitude, and Associated Factors towards Monkeypox Infection among residents at Bahir Dar city, Northwest Ethiopia, 2024. Community based cross-sectional study
Supplemental material, sj-doc-1-son-10.1177_23779608251352392 for Assessment of Knowledge, Attitude, and Associated Factors towards Monkeypox Infection among residents at Bahir Dar city, Northwest Ethiopia, 2024. Community based cross-sectional study by Habtamu Semagne Ayele, Assefa Kebad Mengesha, Gebremariam Wulie Geremew, Abriham Adane Lakew, Tekletsadik Tekleslassie Alemayehu, Demis Getachew and Alemante Tafese Beyna in SAGE Open Nursing
Supplemental Material
sj-docx-2-son-10.1177_23779608251352392 - Supplemental material for Assessment of Knowledge, Attitude, and Associated Factors towards Monkeypox Infection among residents at Bahir Dar city, Northwest Ethiopia, 2024. Community based cross-sectional study
Supplemental material, sj-docx-2-son-10.1177_23779608251352392 for Assessment of Knowledge, Attitude, and Associated Factors towards Monkeypox Infection among residents at Bahir Dar city, Northwest Ethiopia, 2024. Community based cross-sectional study by Habtamu Semagne Ayele, Assefa Kebad Mengesha, Gebremariam Wulie Geremew, Abriham Adane Lakew, Tekletsadik Tekleslassie Alemayehu, Demis Getachew and Alemante Tafese Beyna in SAGE Open Nursing
Footnotes
Abbreviations
Acknowledgement
We would like to acknowledge the study participants for their involvement in this research. We also extend our thanks and appreciation to two fifth-year pharmacy students for their valuable contribution to data collection
Ethical Consideration
The ethical clearance was obtained from the College of Medicine and Health Sciences Research Ethics Review Committee at University of Gondar (Ref # UoG CMHS 112/16). Respondents were informed about the objectives of the study, and data were collected only after obtaining written informed consent from each participant.
Author Contributions
All authors made substantial contributions to the work reported. They participated in the study's conception, methodology development, data collection tool design, data acquisition, analysis, and interpretation. All authors were involved in drafting the original manuscript, revising subsequent drafts, and approving the final version for publication. Furthermore, they are all accountable for ensuring that any questions pertaining to the accuracy or integrity of any aspect of this work are appropriately addressed.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The corresponding author is assigned to provide the raw data upon request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.