
Abstract
Introduction
Cardiac arrest is a serious threat to patients in intensive care units (ICUs), posing a significant risk that can lead to a patient's death if not treated promptly. The utilization of capnography to improve outcomes for patients with cardiac arrest has received substantial attention in research.
Purpose
The purpose of this study was to assess ICU nurses’ knowledge and perceptions of capnography use specifically during cardiac arrest resuscitation in South West Bank Hospitals.
Methods
A cross-sectional descriptive approach was used, employing a questionnaire for data collection. Data were collected from January 15, 2024, to March 15, 2024. The sample of the study consists of 155 nurses working in ICUs in South West Bank hospitals.
Results
The results of the study revealed that most participants
Conclusion
The study confirmed that ICU nurses had fair and poor perceptions toward capnography use during cardiac arrest resuscitation. This highlights the need for targeted education to improve bedside capnography assessment skills among ICU nurses. Recommendations for enhancing capnography training and further research were presented.
Introduction
In intensive care units (ICUs), capnography is a crucial monitoring tool that offers real-time insights into a patient's ventilation, circulation, and metabolic status. The ability to continuously monitor carbon dioxide levels in exhaled air provides invaluable data that can indicate changes in patient condition, facilitating timely interventions (Ayed et al., 2015; Salameh et al., 2018). During cardiac arrest, continuous capnography monitoring is particularly valuable for assessing the return of spontaneous circulation (ROSC) and guiding ventilation, as it provides immediate feedback on the effectiveness of chest compressions and ventilation efforts, in line with guidelines from the American Heart Association (Panchal et al., 2019).
Despite its importance, ICU nurses often report limited knowledge and confidence in using capnography effectively at the bedside. This lack of confidence may stem from insufficient training and exposure to capnography in clinical practice. Research indicates that gaps in capnography education and training may hinder ICU nurses’ ability to assess and interpret capnographic data, thereby impacting patient outcomes during cardiac arrest (Ayed, 2025; Sandroni et al., 2018; Wollner et al., 2020). The implications of these knowledge gaps are particularly significant in high-stakes situations such as cardiac arrest, where timely and accurate assessment can greatly influence patient survival and recovery. This knowledge gap highlights an urgent need to enhance bedside assessment skills to optimize patient care during cardiac emergencies.
This study aims to assess ICU nurses’ perceptions and knowledge of capnography specifically during cardiac arrest resuscitation. By identifying educational needs, the study seeks to support the development of more effective bedside assessment practices for ICU nurses in managing cardiac arrest patients. Furthermore, the findings will provide a foundation for tailored educational interventions that can enhance nurses’ proficiency in capnography, ultimately leading to improved patient outcomes.
Literature Review
Capnography's value in cardiac arrest settings is well-documented, especially for its role in detecting ROSC and verifying endotracheal tube placement. According to current guidelines, capnography monitoring during CPR enhances resuscitation quality and reduces complications related to ventilation (Panchal et al., 2019; Leturiondo et al., 2018). Although endorsed by clinical guidelines, including those from the American Heart Association, many ICU nurses lack comprehensive training on capnography use during resuscitation, which limits their ability to interpret and apply capnographic data effectively in emergency settings (Faltas Marzouk Falt et al., 2023).
Studies highlight that inadequate bedside assessment skills among ICU nurses often stem from gaps in capnography training. Issues such as poor ETCO₂ waveform interpretation and limited familiarity with equipment setup impede their ability to monitor and adjust resuscitation efforts effectively, potentially leading to suboptimal patient outcomes (Shah et al., 2022; Smith, 2021). Given the critical role of nurses in implementing capnography during emergencies, there is a need for targeted training to bridge these knowledge gaps. This study aims to fill a gap in the literature by specifically assessing ICU nurses’ knowledge and perceptions of capnography in a cardiac arrest context, offering insights that can guide the development of educational interventions to improve bedside assessment (Smerat et al., 2025).
Some researchers argue that greater emphasis on training medical personnel to use capnography for real-time patient monitoring and diagnosis of potential cardiac complications is essential (Langham et al., 2017; Long et al., 2017). Capnography education ensures that healthcare providers can accurately interpret capnography traces, which has been shown to positively influence nurses’ attitudes and perceptions regarding the tool's importance during CPR (Kerslake & Kelly, 2017).
The influence of nurses’ training and work-related factors on patient outcomes is well-documented. Improved tools, practices, and hospital environments have led to better health indicators for patients (Batran et al., 2025; Darocha et al., 2017). Factors such as the availability of capnography tools, the personnel's perception of the technique, and the skills necessary to interpret capnographic waveforms have been identified as influential in ICU settings (Darocha et al., 2017; Jaffe, 2017). These findings highlight the need for comprehensive training programs and standardized practices that support effective use of capnography in critical care.
The consequences of failing to utilize advanced tools like capnography can be severe, including increased mortality. Studies note that only about 20% of patients receiving CPR survive, with survival rates outside the hospital dropping to as low as 10% (Pantazopoulos et al., 2015). Effective use of capnography during resuscitation could be instrumental in improving these outcomes. Ensuring that ICU nurses have the technical skills to use capnography during CPR is essential for patient safety and resuscitation success. The lack of proper training on capnography underscores the need for well-developed programs that can significantly improve patient outcomes (Wright, 2017).
Saunders et al. (2017) explored the relationship between training and nurses’ effective use of capnography in clinical settings. Although their study was not focused on resuscitation, they found that training improved nurses’ competency with capnography, reduced the need for ventilation support, and enhanced patient care. This highlights the importance of education in improving outcomes, as well as the need for training programs that address capnography use specifically during CPR.
Challenges remain in the effective use of capnography during CPR. For instance, Aramendi et al. (2017) found that chest compressions during resuscitation can distort capnogram readings, impairing ventilation sensor accuracy. Their study suggests that understanding the limitations and proper application of capnography during CPR is critical for ICU nurses, reinforcing the need for comprehensive training.
Given the evidence, practice guidelines should incorporate more education and training initiatives for capnography in emergency settings, particularly for ICU nurses. Studies emphasize that further care and training are necessary for using capnography during resuscitation, due to waveform distortions caused by chest compressions. Leturiondo et al. (2018) noted that over 70% of capnograms were affected by CPR efforts, recommending a CPR-specific algorithm to reduce distortion. Capnography's primary functions during resuscitation include verifying correct chest compressions, diagnosing ROSC, and predicting patient outcomes, emphasizing the need for ICU nurses to be proficient in capnography interpretation to prevent adverse events.
Methods
Design
A cross-sectional descriptive approach was used among nurses working in the ICUs in South West Bank hospitals.
Research Questions
What is the knowledge level of capnography use during resuscitation among ICU nurses in South West Bank hospitals?
What is the perception level of capnography use during resuscitation among ICU nurses in South West Bank hospitals?
Study Population and Sampling
The study focused on ICU nurses employed in both governmental and non-governmental hospitals. Participants were selected through convenience sampling, meaning that all nurses who met the inclusion criteria in the selected hospitals were invited to participate.
The sample size was determined using the Raosoft online calculator, with a population size of 194, a margin of error of 0.05, a 95% confidence level, and a 50% response rate. The calculation indicated that a sample size of 130 was needed. To account for potential dropouts, the sample size was increased to 155.
Inclusion Criteria
The inclusion criteria were all practical and staff nurses currently working in ICUs, with at least 1 year of ICU experience and willingness to participate in the study.
Exclusion Criteria
The study implemented specific exclusion criteria to ensure the validity and relevance of its findings. Nurses with less than 1 year of experience were excluded. Additionally, nurses on extended leave, such as career breaks or maternity leave, were excluded to maintain consistency in the sample of actively practicing nurses. Part-time nurses and nursing students were also excluded to ensure that the study focused solely on full-time, experienced nursing professionals.
Research Instrument
Data were collected from participants using a self-administered questionnaire. The demographic and professional characteristics of the participants included age, gender, qualifications, years of experience, years worked in ICUs, length of experience with capnography, experience with capnography on intubated patients in ICUs, and any experience with capnography outside these ICUs.
The Nurses’ Knowledge about Capnography Test (NKCT) was used to collect data on the nurses’ capnography knowledge. Kiekkas et al. (2016) created this tool, which includes 30 correct and incorrect (dichotomous scale) assertions regarding capnography. “The components are divided into four main groups: capnography function principles, ETCO₂ pressure conditions, capnography waveform conditions, and guidelines for capnography use.”
Knowledge scores were converted into percentage scores by dividing respondents’ results by the potential maximum scores and multiplying by 100. The total score of each result was calculated using Bloom's cutoff point (Bloom, 1956). The degree of knowledge was categorized into three levels based on the aggregate scores: low-level knowledge (less than 60%), moderate-level knowledge (60–79%), and high-level knowledge (80–100%). The NKCT's reliability has previously been assessed. Kiekkas et al. (2016) reported internal consistency and item analysis to determine the instrument's reliability.
The Nurses’ Perceptions of Capnography Use Scale was developed by the researcher after a rigorous review of relevant literature. The scale comprises 13 items rated on a five-point Likert scale (from strongly disagree to strongly agree), designed to capture various dimensions of nurses’ perceptions, including perceived benefits, challenges, and confidence in using capnography during resuscitation. To ensure content validity, five experienced clinical and academic nursing professionals reviewed each item, providing feedback to refine clarity and relevance. The perception scores were converted into percentage scores by dividing the respondents’ results by the potential maximum scores and multiplying by 100. The degree of perception was categorized into three levels based on the aggregate scores: poor level perception (less than 60%), fair level perception (60–79%), and good level perception (80–100%).
Instruments validity was confirmed by five experienced clinical and academic nursing professionals who reviewed the questionnaire. Reliability was established through a pilot test with 30 nurses, yielding a Kuder-Richardson 20 coefficient of 0.82 for NKCT and a Cronbach's alpha of 0.84 for perceptions of capnography use, reflecting high internal consistency.
In the main study, the Kuder-Richardson 20 coefficient for nurses’ knowledge of capnography increased to 0.84, and Cronbach's alpha for perceptions of capnography use rose to 0.88, indicating an acceptable level of internal consistency reliability.
Ethical Considerations
Ethical approval and permission to conduct the study were granted by the Ethical Committee of Palestine Ahliya University and the participating hospitals. Informed consent was obtained from all participants before they completed the questionnaire. Participants were informed that their involvement was voluntary and that they could withdraw from the study at any time.
Data Collection Procedure
Data collection took place over a 2-month period, from January 15, 2024, to March 15, 2024. During this time, ICU nurses who met the inclusion criteria were invited to participate by completing a self-administered questionnaire on their knowledge and perceptions of capnography use during cardiac arrest.
After receiving ethical approval, meetings were scheduled with head nurses in each unit at the selected hospitals to explain the study's purpose and request a list of eligible nurses. Participants were then asked to sign an informed consent form and complete the questionnaire. Each participant was provided an envelope to submit the completed questionnaire and was allowed to complete it at their convenience. To prevent any loss of questionnaires, the researcher was present while respondents completed them. The principal investigators handled the distribution and collection of the questionnaires, which were administered and completed face-to-face in English.
Data Analysis
Data entry and analysis were conducted using SPSS software version 26.0. Before analysis, each questionnaire was reviewed for completeness. Descriptive statistics, including frequency, proportion, mean, and standard deviation, were used to summarize the data. Statistical significance was set at p < 0.05. Pearson correlation, independent t-tests, and ANOVA were used to compare the mean scores of capnography knowledge with demographic and professional characteristics.
Results
Participants’ Characteristics
The findings revealed that the mean age of the participants was 31.4 ± 6.9 years, ranging between 22 and 54 years. More than half of the participants, 90 (58.1%), were male, and 107 (69.0%) were staff nurses. The mean of the participants’ total experience was 7.4 ± 5.8 years, with an average of 2.4 ± 2.7 years of experience specifically with capnography. More than half, 92 (59.4%), reported that they had used capnography on intubated patients. Additionally, 56 (36.1%) had experience with capnography outside of the ICUs. Table 1 provides detailed demographic and professional characteristics of the 155 ICU nurses surveyed, including years of experience, exposure to capnography, and experience with intubated patients.
Demographic and Professional Characteristics of ICU Nurses.

ICU=intensive care unit.
Knowledge and Perception of Capnography
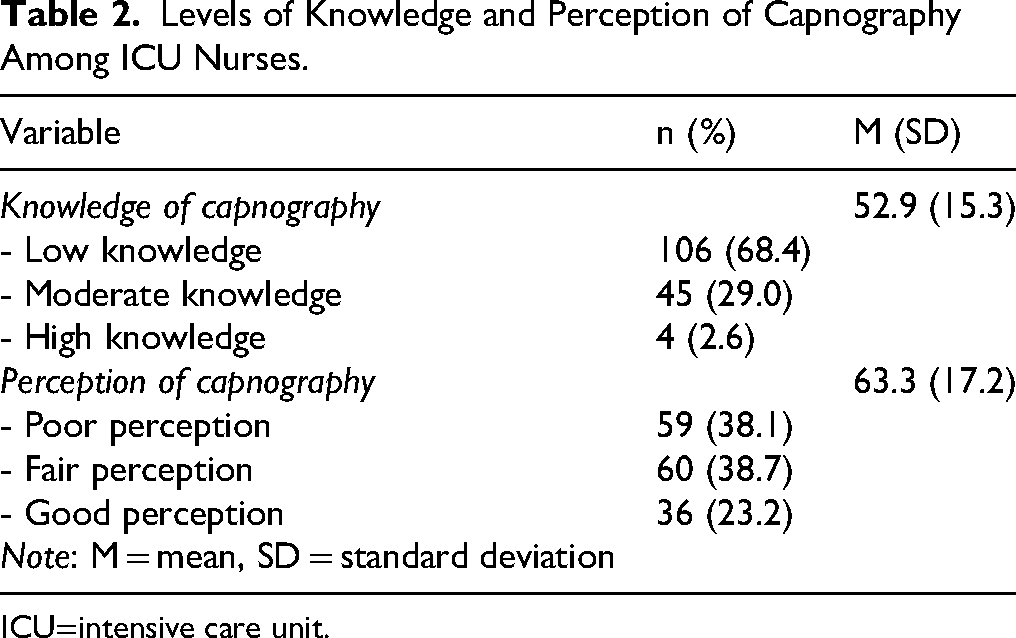
A majority, 106 (68.4%), demonstrated low knowledge in capnography. Forty-five (29.0%) exhibited a moderate level of knowledge, while only 4 (2.6%) showed a high level of knowledge. The analysis revealed that the mean perception score of capnography use was 63.3 ± 17.2. Additionally, perception levels varied among the nurses: 59 (38.1%) of respondents expressed a poor perception, 60 (38.7%) reported a fair perception, and 36 (23.2%) held a good perception of capnography usage, as presented in Table 2.
Levels of Knowledge and Perception of Capnography Among ICU Nurses.
ICU=intensive care unit.
Correlation Between Knowledge of Capnography and Demographic and Professional Characteristics
The results of the Pearson correlation test showed no significant relationships between knowledge of capnography and selected demographic or professional characteristics of the participants (p > 0.05), as displayed in Table 3.
Correlation Between Knowledge of Capnography and Nurses’ Demographic and Professional Characteristics.

ICU=intensive care unit.
Differences in Knowledge of Capnography Based on Demographic and Professional Characteristics
Independent t-tests and ANOVA were conducted to compare the mean scores of capnography knowledge across different demographic and professional characteristics. The analysis revealed that there were no significant differences in knowledge of capnography use based on demographic and professional characteristics (p > 0.05), as detailed in Table 4.
Differences in Knowledge of Capnography Based on Demographic and Professional Characteristics.

ICU=intensive care unit.
Discussion
To ensure accurate assessment of ICU nurses’ knowledge and perceptions of capnography, this study employed the “Nurses’ Perceptions of Capnography Scale,” a tool specifically adapted for critical care settings. Instrument validity was confirmed by five experienced clinical and academic nursing professionals who reviewed the questionnaire for content relevance and clarity. Reliability was established through a pilot test with 30 nurses, yielding a Cronbach's alpha of 0.84 for the perception scale, reflecting high internal consistency. In the main study, the internal consistency of the scale improved further, with a Cronbach's alpha of 0.88. The scale included items measuring confidence in interpreting ETCO₂ waveforms, understanding capnographic readings during resuscitation, and perceived clinical utility of capnography. Example items included: “I feel confident interpreting ETCO₂ waveforms during cardiac arrest” and “Capnographic changes help me assess the effectiveness of chest compressions.” This tailored and psychometrically sound instrument ensured that the findings accurately reflect the specific competencies required for effective capnography use in ICU resuscitation scenarios.
Nurses’ understanding of clinical devices for monitoring, assessing, and treating cardiac patients is essential for delivering high-quality patient care and ensuring organizational effectiveness (Cook & Harrop-Griffiths, 2019). End-tidal CO₂ (ETCO₂) level measurement, as a non-invasive technique, is strongly recommended by the American Heart Association (AHA) and Advanced Cardiovascular Life Support (ACLS) guidelines for assessing the effectiveness of resuscitation efforts during cardiac arrest (Lui et al., 2016). The study findings highlight that 68.4% of ICU nurses exhibit low knowledge levels regarding capnography, with only 23.2% reporting a high perception of their ability to use capnography effectively for resuscitation. These gaps were observed to persist irrespective of years of nursing experience, underscoring the need for targeted educational interventions.
In comparison with prior research, these findings align with studies such as those by Lin et al. (2017), De Oliveira and Moreira (2015), and Pantazopoulos et al. (2015), which also revealed limited capnography knowledge among healthcare professionals. These studies highlight that a lack of capnography training may impair nurses’ abilities to make accurate clinical judgments, especially in high-stakes resuscitation scenarios. In high-resource settings such as the United States, the United Kingdom, and parts of South Africa, capnography is a standard component of ICU protocols and resuscitation guidelines, with structured training programs routinely provided to both nurses and paramedics. Notably, studies such as Wylie et al. (2019) found that paramedics in South Africa demonstrated significantly higher levels of capnography knowledge and confidence, likely reflecting better access to formal training and hands-on practice. In contrast, this study revealed that ICU nurses in the South West Bank had limited knowledge and perception of capnography use, despite their frontline role in resuscitation efforts. These disparities highlight the pressing need for localized educational initiatives and the integration of capnography training into critical care curricula. Bridging this global gap through context-sensitive interventions could enhance the standardization of care, improve patient outcomes, and align ICU nursing practice in the South West Bank with international best practices.
The findings also emphasize specific deficits in critical capnography skills, such as ETCO₂ waveform interpretation and real-time capnographic monitoring during resuscitation. Without these skills, nurses may miss crucial changes in patient status, which could impede effective CPR and elevate the risk of adverse patient outcomes, including mortality. Targeted training initiatives that focus on these areas could significantly enhance nurses’ abilities to detect early indicators of ROSC, thereby improving CPR outcomes.
This study further revealed that there were no significant differences between nurses’ capnography knowledge and demographic or professional characteristics, such as years of experience or job position. This suggests a systemic gap in knowledge across all levels of ICU nursing staff, reinforcing the need for comprehensive, institution-wide educational reforms. Simulation-based training programs tailored to ICU scenarios could be particularly effective, especially in settings where capnography is not routinely used. Such programs would offer nurses practical, hands-on opportunities to build familiarity and competence with capnography in a controlled environment, leading to better patient outcomes and enhanced clinical confidence.
Additionally, the study's results indicate that nurses’ perceptions of capnography use were generally fair or poor, consistent with findings from Clark et al. (2018), who reported that the perceived safety impact of capnography was moderate among nursing staff. This suggests that improving nurses’ knowledge and practical skills with capnography could positively influence their perceptions of its utility, as greater understanding often correlates with increased confidence in clinical applications. Enhancing perception through education may foster a more favorable view of capnography as an essential tool in patient care, motivating nurses to integrate it more readily into resuscitation protocols.
Currently, capnography training for ICU nurses in the study setting is limited in both frequency and scope. Most training, when available, is informal or integrated briefly within broader resuscitation or advanced life support courses, with minimal emphasis on advanced competencies such as ETCO₂ waveform interpretation or its use in monitoring the effectiveness of chest compressions. Furthermore, participation in such training sessions is inconsistent, with only a small proportion of nurses reporting prior exposure. This limited access to comprehensive, structured training highlights a critical gap in current educational efforts. Therefore, future initiatives should not only expand the reach of capnography education to include nurses from various units and hospitals but also enhance the depth of training by incorporating hands-on sessions, simulation-based learning, and practical case scenarios
In summary, this study underscores the essential role of capnography in enhancing CPR effectiveness and suggests that improved training in its use could bridge current knowledge gaps. The absence of significant differences across experience levels points to a pervasive need for education that spans all ranks within ICU nursing staff. Targeted, hands-on training in capnography, coupled with ongoing assessment and feedback, could help mitigate knowledge deficits, thereby advancing patient care quality and aligning with globally recognized standards in critical care.
The participating ICUs primarily serve critically ill patients with high rates of mechanical ventilation and intubation, yet capnography equipment is inconsistently available and not routinely used during resuscitation. This limited accessibility likely contributes to the observed knowledge gaps, as nurses have fewer opportunities to engage with capnography in real-world clinical scenarios. Moreover, the lack of standardized protocols or institutional guidelines for capnography use may reduce its perceived importance among ICU staff. Infrequent exposure to capnography, particularly in emergency situations such as cardiac arrest, diminishes the likelihood that nurses will develop confidence or competence in interpreting ETCO₂ readings and waveform data. These contextual limitations underscore the need not only for educational interventions but also for policy changes that prioritize capnography integration into routine ICU monitoring and resuscitation protocols.
Conclusion
The findings from this study emphasize the need for enhanced educational initiatives around capnography use in ICUs, particularly as knowledge deficits were observed across all levels of experience. Addressing these gaps through comprehensive training can improve ICU nurses’ ability to monitor and interpret capnographic data effectively, which is essential for optimal patient outcomes during cardiac arrest. This study underscores the importance of bedside assessment skills and supports a call for targeted training in this critical area of patient monitoring.
The study further revealed that most ICU nurses demonstrated fair to poor perceptions of capnography's role in resuscitation, consistent with their limited knowledge. However, understanding the current training practices within hospitals would be beneficial for developing targeted educational strategies. For example, some hospitals may only provide brief orientation sessions on capnography for new ICU nurses, focusing on basic equipment handling rather than advanced topics like ETCO₂ waveform interpretation. Including a review of current training content and practices would help identify specific gaps and better inform the design of comprehensive educational interventions.
Strengths and Limitations
This study is the first to investigate nurses’ knowledge of capnography use in hospitals in the South West Bank, providing valuable insights for healthcare personnel and administrators. However, the study has limitations. The use of self-administered questionnaires could introduce reporting bias due to participants’ interpretations or their desire to present themselves favorably. Additionally, the cross-sectional design does not allow for identifying cause-and-effect relationships.
Recommendations
Future research should include a broader range of participants, incorporating nurses from different units and locations. Organizing structured training sessions on capnography and developing guidelines for its use in resuscitation would help standardize practices and improve capnography utilization. Based on the identified knowledge and perception gaps, future research should focus on evaluating the effectiveness of targeted, simulation-based training programs on capnography use among ICU nurses. Such interventional studies could assess changes in knowledge, skill acquisition, and confidence before and after training, offering measurable evidence of educational impact. Additionally, longitudinal research could explore whether improved capnography competency translates into better clinical decision-making and patient outcomes during resuscitation events. Investigating the integration of capnography education into nursing curricula or continuous professional development programs could also provide valuable insights into sustainable capacity-building strategies.
Footnotes
Acknowledgements
The author would like to express their thanks to the nurses who participated in the study.
Ethics Approval and Consent to Participate
Ethical approval for this study was obtained from Palestine Ahliya University (CAMS/CCNA/7/124). Written informed consent was obtained from all subjects before the study.
Consent for Publication
I affirm that this work is original and has not been published elsewhere, except as noted in the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Use of AI Software
I affirm that the integrity and originality of this work are entirely my own and are not influenced by any AI technology.