
Abstract
Introduction
The intensive care unit is a distinct environment that emphasizes the importance of professional and skilled nursing practice.
Purpose
This study aims to assess the relationship between the nurse practice environment and perceived patient-centered care (PCC) among nurses in intensive care units (ICUs) in Palestinian southern West Bank hospitals.
Methods
A cross-sectional, descriptive correlational design was employed for this study. The sample composed of 150 ICUs nurses. Data were collected using scales that assessed the practice environment and PCC.
Results
The practice environment scores ranged from 2.1 to 3.2, with a mean of 2.7 (±0.3), reflecting a moderately favorable environment. The PCC competency scores ranged from a mean 1.9 to 4.1, with of 3.4 (±0.5), indicating a generally high level of competency. A positive correlation was found between the practice environment and PCC competency (r = .397, p = .001). Predictors of PCC included the practice environment (B = .836, p = .001), age (B = .027, p = .006), and educational level (B = .154, p = .015).
Conclusion
The study found a moderately favorable practice environment and a generally high level of competency in PCC among nurses. Additionally, there were significant positive correlations between the practice environment and PCC competency. Age, educational level, and the practice environment were identified as predictors of PCC.
Introduction
Advancements in disease management, research, evidence-based practice, and the integration of technology have transformed the delivery of care, creating a highly fluid nursing practice environment. This evolution has been driven by regulatory demands, financial constraints, and personnel limitations (Engle et al., 2021). Despite these advancements, the nursing practice environment remains challenging, as noted by the American Association of Colleges of Nursing. Nurses must continually adapt to this dynamic setting to provide safe, high-quality care while upholding the standards of professionalism (American Association of Colleges of Nursing, 2021).
The rapid and dramatic changes in healthcare delivery have led many nurses to express dissatisfaction, describing their practice environment as highly stressful and professionally unfulfilling (Aqtam et al., 2023). These changes often conflict with healthcare institutions’ goals of delivering high-quality care while managing costs (Nilsen et al., 2020). The evolving nature of the nursing practice environment underscores the need for a focus on PCC. The essentials of nursing care, as highlighted by Credland et al. (2021), are fundamental components required by every patient, and patient experience is a crucial indicator of high-quality care (Barbazza et al., 2021).
In the intensive care unit (ICU), patients receive intensive monitoring and therapy, often involving medications, life support, and safety devices. The ICU environment can lead to harsh treatment, loss of autonomy, and family separation, contributing to a range of postdischarge issues such as cognitive decline, anxiety, depression, posttraumatic stress disorder, muscle weakness, and impairment of daily activities (Halvorsen et al., 2022; Hiser et al., 2023). These issues can diminish the quality of life (Hiser et al., 2023). Therefore, there is a growing need to shift the focus of care in the ICU to be more patient-centered, emphasizing the patient’s needs beyond mere survival (Schwartz et al., 2022).
However, the complexity of ICU equipment and the overwhelming workload often hinder effective communication between patients and nurses, making it challenging to provide PCC (Almenyan et al., 2021; Cucolo et al., 2024). Identifying factors that facilitate or obstruct nurses in delivering effective PCC is crucial (Youn et al., 2022). Improving the working environment is essential to enhance nurses’ performance and care delivery (Parra-Giordano et al., 2022). A well-designed “nursing practice environment” is associated with excellent care and improved patient outcomes (Nascimento & Jesus, 2020).
The concept of the nursing practice environment includes the physical surroundings, team dynamics, organizational policies, and resources (Wei et al., 2018). It encompasses not only physical aspects but also managerial skills, leadership, support structures, staffing, and the interaction between nurses and physicians (Mabona et al., 2022). Key characteristics of this environment involve collaborative relationships with multidisciplinary team members and recognition within the healthcare hierarchy. As the demand for high-quality care and changes in the healthcare system and population demographics increase, there is a reciprocal need for practice environments that allow nurses to fully utilize their skills while maintaining the profession's caring nature (Malak et al., 2022). Although caring is not exclusive to nursing, it is a fundamental and valued aspect of the profession (Watson & Foster, 2003).
In 2001, patient-centeredness was introduced as one of six key aims for improving quality patient care, emphasizing the importance of communication and patient involvement in care decisions (Institute of Medicine [IOM], 2001; Pelletier & Stichler, 2014; Rangachari et al., 2011). PCC, often used interchangeably with terms like person-centered care or client-centered care, focuses on providing holistic care that respects patients’ cultural beliefs and values (Hobbs, 2009). Principles of PCC include respecting patient values and preferences, coordinating and integrating care, involving family and friends, ensuring physical comfort, and providing emotional support (Ortiz, 2018).
In 2010, The Joint Commission revised standards for PCC to enhance safety and quality, including greater involvement of patients and families. Many healthcare organizations faced challenges in meeting these revised standards and engaging patients and families (The Joint Commission, 2012). The focusing on improving hospital quality and safety, along with the pressure to reduce healthcare costs, has led organizations to seek ways to improve patient care outcomes and satisfaction (Bernstein et al., 2022; Karaca & Durna, 2019). Patient satisfaction has been recognized as an indirect measure of improved outcomes, associated with lower readmission rates and better patient adherence and self-management (Apker et al., 2018; Friganovic et al., 2020).
In the context of Palestinian healthcare, there is a significant gap in understanding how the nursing practice environment influences perceived PCC, particularly in ICUs. While international studies have explored these relationships in various healthcare settings, such as long-term care hospitals and general medical units, research specific to Palestinian healthcare environments remains limited. The literature underscores the importance of factors like staffing adequacy, leadership quality, and practice environment perceptions in shaping PCC outcomes. However, these factors may differ in impact within Palestine’s unique socio-political and resource-constrained context, where nurses encounter challenges such as staffing shortages, geopolitical tensions, and limited resources.
Conducting a study within Palestinian ICUs is essential to gaining insights into how these specific contextual factors affect nurses’ ability to deliver PCC. Such research could inform targeted interventions and policy recommendations tailored to the Palestinian healthcare setting, ultimately improving PCC in this context. Therefore, the purpose of this study was to assess the relationship between the nursing practice environment and perceived PCC among nurses in ICUs in Palestinian southern West Bank hospitals.
Literature Review
Park and Park (2018) highlighted the role of moral sensitivity and the nursing practice environment in fostering PCC among nurses in long-term care hospitals. Their findings established that these two factors are positively correlated with PCC, reinforcing the notion that ethical awareness and supportive work conditions enable nurses to provide care that prioritizes patient dignity and needs. Also, Bachnick et al. (2018) provided additional evidence by surveying a large sample of patients and registered nurses in Switzerland. They found that adequate staffing, leadership support, and resource availability were critical to achieving high levels of PCC. Conversely, the implicit rationing of nursing care—often a consequence of inadequate resources—was linked to diminished PCC, signaling a clear need for systemic improvements to nursing environments. Shin and Yeom (2021) explored the interplay between self-leadership, nursing practice environment, and PCC among oncology nurses in South Korea. Their study identified that both the practice environment and self-leadership were significant predictors of PCC, accounting for a substantial variance in its delivery. This suggests that empowering nurses through supportive environments and leadership training can significantly enhance PCC outcomes. Additionally, Kang and Lim (2019) emphasized the impact of interpersonal relationships and workload on PCC within ICUs. They found that factors like the number of patients per nurse and collegial relationships among healthcare workers significantly influenced the quality of PCC. This underscores the critical role of manageable workloads and positive interpersonal dynamics in enabling effective patient-centered practices.
Similarly, Lee and Lee (2020) linked the nursing practice environment and moral distress to PCC in long-term care settings. Their findings revealed that improvements in the practice environment and strategies to mitigate moral distress could directly enhance PCC delivery. On a larger scale, Jarrar et al. (2021) examined the mediating role of PCC between practice environment dimensions and care outcomes in Malaysian private hospitals. Their findings highlighted the interdependence between the practice environment and care quality, suggesting that fostering PCC-focused environments can lead to better patient outcomes and improved safety standards.
While these studies collectively emphasize the importance of the nursing practice environment in shaping PCC, there is a notable gap in research within low-resource and politically unstable settings like Palestine. These unique environments present additional challenges, such as staffing shortages, high patient-to-nurse ratios, and limited access to resources, which may profoundly affect the delivery of PCC. By examining the relationship between the nursing practice environment and PCC in Palestinian hospitals, this study aims to provide context-specific insights that can inform policies and interventions to improve nursing care quality.
Method
Study Design
A cross-sectional, descriptive correlational design was employed for this study. The study was conducted in ICUs of governmental and non-governmental hospitals in South West Bank hospitals in the period of January 1 to June 1, 2024.
Setting
Palestine consists of the West Bank and Gaza Strip. West Bank is divided to three regions: north, middle, and south. The study was conducted in the ICUs of the South West Bank region of Palestine. The hospitals were Dura hospital, Alia hospital, Mahmoud Abbas hospital, Abu Al-Hasan Al-Qasem hospital, Al-Hussein hospital, Al-Mezan hospital, Al-Ahli hospital, Al-Yamameh hospital, and Bethlehem Arab Society hospital. In the South West Bank region of Palestine, ICUs consist of a total of 65 beds distributed across multiple hospitals, catering to critically ill patients with a range of medical and surgical conditions. Resource constraints, such as limited availability of medical equipment and supplies, coupled with staffing shortages, result in patient-to-nurse ratios that often exceed international recommendations. This impacts the quality and consistency of nursing care. High patient turnover further compounds these challenges, placing additional demands on ICU staff. Moreover, the geopolitical situation, marked by political instability and restricted movement, affects healthcare delivery by delaying the supply chain and limiting access to advanced medical resources.
Research Question
What is the mean score of nursing practice environment perception among nurses in ICUs in Palestinian southern West Bank hospitals?
What is the mean score of perceived PCC among nurses in ICUs in Palestinian southern West Bank hospitals?
What are the predictors of perceived PCC among nurses in ICUs in Palestinian southern West Bank hospitals?
Study Population and Sampling
The study targeted ICU nurses working in both governmental and nongovernmental hospitals. Convenience sampling was used to select participants, meaning that all nurses meeting the inclusion criteria in the chosen hospitals were invited to participate.
The sample size was calculated using the Raosoft online tool, with parameters set at a population of 194, a margin of error of 0.05, a 95% confidence interval, and a 50% response rate. Based on these parameters, the required sample size was 130. To accommodate potential attrition, the sample size was adjusted to 150.
Inclusion Criteria
The inclusion criterion was all practical and staff nurses currently working in ICUs. Nurse with more than 3 months of experience working in the ICUs and willingness to participate in the study were included in the study.
Exclusion Criteria
The study implemented specific exclusion criteria to ensure the validity and relevance of its findings. Nurses with less than 3 months of experience were excluded, as their brief tenure made it challenging to accurately assess their awareness of the practice environment and their performance in person-centered nursing, particularly during their adjustment period. Head nurses were also excluded, as their roles typically do not involve direct patient care. Additionally, nurses who were on extended leave, such as career breaks or maternity leave, were excluded to maintain consistency in the sample of actively practicing nurses. Part-time nurses and nursing students were excluded as well, to ensure that the study focused solely on full-time, experienced nursing professionals.
Instrumentation
Data collection was performed using a structured self-reported questionnaire comprising three sections: socio-demographic information, practice environment, and PCC nursing.
The first section, socio-demographic information, gathered data on variables such as age, gender, level of education, type of hospital, work experience, work shift, and perceived adequacy of staffing.
The second section assessed the practice environment through the Practice Environment Scale-Nursing Work Index (PES-NWI), developed by Lake (2002). This widely utilized instrument provides insight into nurse practice environments, identifying factors that either support or hinder nurses’ ability to deliver high-quality care (Swiger et al., 2017). Endorsed by various healthcare organizations in the United States, the PES-NWI is considered a key measure for promoting quality healthcare (Havens et al., 2012; Warshawsky & Havens, 2011). The PES-NWI consists of 31 items across five subscales, with each subscale containing between 3 and 10 items (Parker et al., 2010). Reliability, as indicated by Cronbach's alpha, ranges from 0.71 to 0.84 (Lake, 2002). The PES-NWI subscales utilize a four-point Likert scale, from 1 (strongly disagree) to 4 (strongly agree), to evaluate factors within the practice environment that contribute to high-quality nursing care. Higher scores reflect a more favorable practice environment (Swiger et al., 2017). In the current study, Cronbach’s alpha for the total scale was 0.82.
The third section utilized the PCC Competency Scale for Hospital Nurses, developed by Hwang (2015). This scale consists of 17 items divided into four subscales: (1) six items on respecting patients’ perspectives, (2) five items on promoting patient involvement in care processes, (3) three items on providing patient comfort, and (4) three items on advocating for patients. The overall Cronbach's alpha coefficient for the scale was 0.92, with subscale alphas of 0.85, 0.81, 0.84, and 0.80, respectively. The scale demonstrated strong convergent and discriminant validity through multitrait scaling analysis. A significant correlation was found between the total PCC competency scores and overall self-ratings of PCC performance (r = 0.60, p < .001), affirming the scale's validity and reliability (Hwang, 2015). The PCC Competency Scale uses a five-point Likert scale, where 1 = minimal, 2 = below average, 3 = average, 4 = good, and 5 = excellent. Competency scores are calculated based on the mean values of the competency items. In the current study, Cronbach's alpha for the overall scale was 0.88.
Ethical Considerations
Permission to conduct the study and ethical approval were obtained from the Ethical Committee of Palestine Ahliya University. Prior to data collection, a support letter was secured from the selected hospitals. Rapport was established with participants, who were informed of their voluntary participation. To ensure privacy, data collection was conducted in a comfortable, private setting. Participants were assured that their personal information would be protected and securely managed by the researcher, with confidentiality maintained throughout the study.
Data Collection Procedure
After obtaining ethical approval, meetings were arranged with head nurses in each unit at the selected hospitals to explain the study’s purpose, request a list of eligible nurses, and gain access to the ICUs. Participants were then asked to sign an informed consent form and complete the questionnaire. Each participant was provided with an envelope to place the completed questionnaire and given time at their convenience to fill it out. To ensure no questionnaires were lost, the researcher was present while the respondents completed them, collecting the completed questionnaires at the end of each working day. The principal investigators were responsible for distributing and collecting the questionnaires, which were administered and completed face-to-face in English. Additionally, participants were encouraged to ask for clarification if they encountered any language-related difficulties, ensuring they fully understood the content of the questionnaires.
Data Analysis
SPSS software version 23.0 was employed for data entry and analysis. Each questionnaire was reviewed for completeness before analysis. Descriptive statistics, including frequency, proportion, mean, and standard deviation, were used to summarize the data, with results presented in tables and bar charts. Statistical significance was determined at a p value of <.05. To analyze the correlation between the practice environment and PCC of ICU nurses, Pearson's correlation coefficient was calculated. Additionally, multiple linear regression analysis was conducted to assess the predictors of PCC.
Results
Participants’ Characteristics
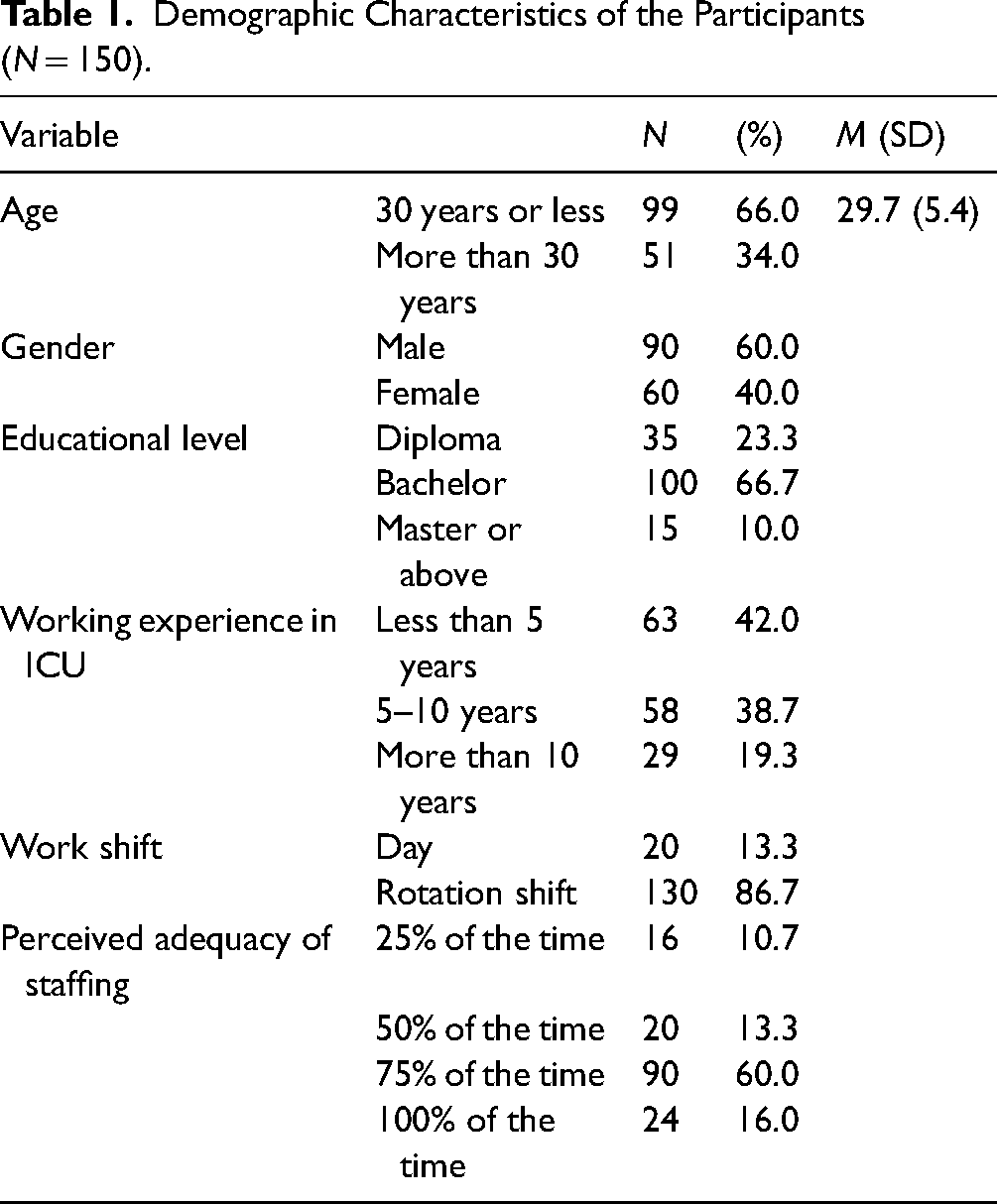
One hundred and fifty out of 194 questionnaires (77.3% response rate) were completed and returned by the nurses. The majority of participants are 30 years old or younger 99 (66.0%), with an average age of 29.7 years (SD = 5.4). Gender distribution shows that 90 (60.0%) are male. Educational levels vary, with the majority holding a bachelor's degree 100 (66.7%). In terms of working experience in ICU, 63 (42.0%) have less than 5 years of experience. The majority of participants 130 (86.7%) work rotation shifts. Regarding perceived adequacy of staffing, 90 (60.0%) feel staffing is adequate 75% of the time. This perception likely stems from their experiences with workload distribution, availability of support staff, and alignment between patient acuity and staffing levels. Perceived adequacy significantly impacts the practice environment, influencing nurses’ capacity to adhere to evidence-based practices, manage clinical priorities, and ensure patient safety (Table 1).
Demographic Characteristics of the Participants (N = 150).
The overall practice environment score ranges from 2.1 to 3.2, with a mean of 2.7 ± 0.3, indicating a moderately favorable environment for the participants. Nurse Participation in hospital affairs has a mean of 2.7 ± 0.3, indicating moderate involvement. The nursing foundations for quality of care score a mean of 2.8 ± 0.3, reflecting a high foundation. Nurse manager ability, leadership, and support of nurses have a mean of 2.8 ± 0.4, showing high managerial support. Staffing and resource adequacy score lower with a mean of 2.7 ± 0.4, highlighting moderate adequacy. Collegial nurse-physician relations have a relatively higher mean of 2.8 ± 0.5, indicating good interprofessional relationships, as seen in Table 2.
Description of Practice Environment Among the Participants.

The total PCC competency score ranges from 1.9 to 4.1, with a mean of 3.4 ± 0.5, indicating a generally high level of competency. Regarding subscales of patient-centered scale, both promoting patient involvement in care process scores and advocating for patients scores have the highest with a mean of 3.5 ± 0.6, reflecting a strong emphasis on engaging patients in their care and a strong dedication to patient advocacy. However, the lowest subscale was respecting patients’ perspectives that has a mean score of 3.3 ± 0.6. Overall, these results suggest that participants generally exhibit high competency in various aspects of PCC, as seen in Table 3.
Description of Patient-Centered Care Among the Participants.

The total practice environment is positively correlated with all aspects of PCC, particularly with respecting patients’ perspectives (r = .396, p = .001) and the overall PCC competency (r = .397, p = .001), highlighting the integral role of a supportive practice environment in fostering PCC, as seen in Table 4.
Relationship Between Practice Environment and Patient-Centered Care Among the Participants.

*Significant at the 0.05 level.
**Significant at the 0.01 level.
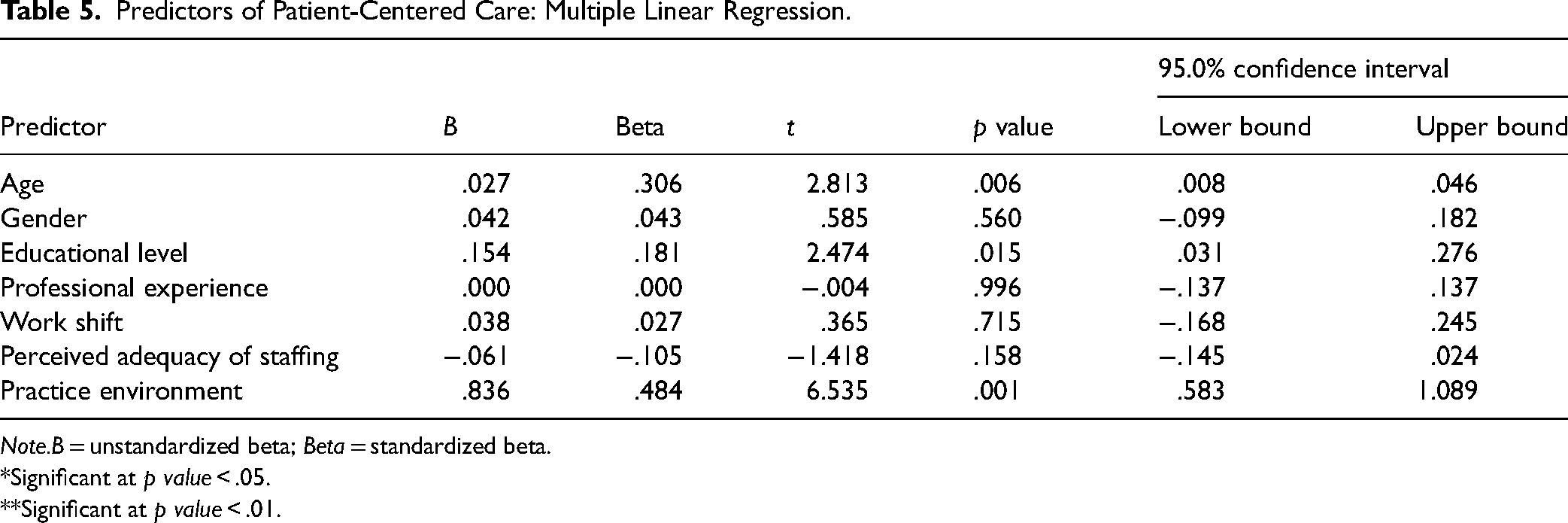
A multivariable regression analysis was utilized to identify the PCC predictors among nurses in ICUs. As shown in Tables 4 and5, the independent variables (age, gender, educational level, professional experience, work shift, perceived adequacy of staffing, and practice environment) were entered into the model of predictors. The overall model was statistically significant (p ≤ .001, R = 0.530, R2 = 0.281, adjusted R2 = 0.245). This stated that 28.1% of the variance in PCC was clarified by the whole model.
The findings showed that age, educational level, and practice environment had a significant impact on PCC. The practice environment has the strongest positive effect (B = .836, p = .001), emphasizing its critical role in enhancing PCC. Age is a significant predictor, with a positive effect (B = .027, p = .006), indicating that older participants tend to report higher levels of PCC. Educational level also shows a positive and significant effect (B = .154, p = .015), suggesting that educational level is associated with better PCC, as seen in Table 5.
Predictors of Patient-Centered Care: Multiple Linear Regression.
Note.B = unstandardized beta; Beta = standardized beta.
*Significant at p value < .05.
**Significant at p value < .01.
Discussion
The current study revealed that the mean practice environment indicates moderate score. In the context of Arab and Palestinian healthcare settings, these findings are particularly relevant as they emphasize the need for continuous improvements in hospital affairs and managerial support to enhance care quality.
This result aligns with previous studies that highlight the importance of a supportive practice environment in promoting quality care among nurses (Asseeri & El Seesy, 2019; Ibrahim et al., 2019). Ibrahim et al. (2019) indicated that majority of the nurses (79%) had a moderate level of professional nursing practice environment in their study to assess the effect of a professional nursing practice environment and psychological empowerment on nurses’ readiness for change. Also, Asseeri and El Seesy (2019) reported that nurse's practice environment was favorable at King Abdul-Aziz University Hospital. Additionally, Saad et al. (2021) reported that the majority of staff nurses (84.0%) have moderate practice environment at Benha University Hospital in critical care units. However, this result was high than a study conducted by Dordunoo et al. (2021) which reported a mean practice environment score of 2.54 ± 0.34.
The variability in findings across different studies can be attributed to several factors, including differences in the healthcare settings, the specific populations studied, and the methodologies used. For example, the studies by Asseeri and El Seesy (2019) and Ibrahim et al. (2019) were conducted in university hospital settings, which may have more resources and structured support systems compared to other healthcare environments. These supportive conditions can lead to more favorable perceptions of the practice environment among nurses. On the other hand, Dordunoo et al. (2021) reported lower practice environment scores, which could be due to differences in the institutional policies, availability of resources, or cultural factors within their study setting. These discrepancies underscore the importance of context in assessing the professional nursing practice environment and suggest that while some settings may excel in providing supportive environments, others may face challenges that require targeted interventions to improve nurse satisfaction and care quality.
Also, the current study revealed that the mean perceived PCC score was generally high. The current study's finding of a high mean perceived PCC score among nurses in ICU aligns with broader trends observed in Arab and Palestinian healthcare contexts. In these regions, there is a strong cultural emphasis on family and community, which can translate into a more holistic and patient-centered approach in healthcare settings (Alkhaibari et al., 2023). This cultural backdrop may contribute to higher levels of perceived PCC as nurses are often more attuned to the needs and preferences of their patients, striving to provide care that respects and integrates these cultural values. Furthermore, ongoing efforts to improve healthcare quality and patient outcomes in many Arab countries, including investments in training and resources for ICU staff, could also enhance the delivery of PCC. In Palestine, despite facing numerous challenges such as political instability and resource limitations, healthcare professionals often exhibit a strong commitment to patient care, driven by a deep sense of community solidarity and resilience. This commitment may foster higher perceptions of PCC among nurses working in ICUs, where the stakes are particularly high and the need for compassionate, individualized care is paramount.
This result was consistent with Shin and Yeom’s (2021) study which indicated that the average score for PCC among oncology nurses was 3.74 ± 0.42, which is somewhat higher than those (i.e., 3.52∼3.70) reported in previous studies about ICU nurses (Kang & Lim, 2019; Kang & Shin 2019). This alignment may be due to the intense training and heightened awareness of patient needs required in both oncology and ICU settings. However, the current study result was high than Pakdaman et al.’s (2019) study which found that the mean score of PCC was 2.34 ± 0.58 from nurses’ point of view. The markedly lower score suggests significant contextual differences, possibly due to disparities in healthcare infrastructure, cultural factors, or the specific challenges faced in their study settings. These discrepancies highlight the influence of varying institutional environments, resource allocation, and cultural attitudes on the delivery and perception of PCC among nurses.
The current study revealed that there is a positive correlation between the total practice environment and all aspects of PCC, particularly respecting patients’ perspectives and overall PCC competency, which highlight the integral role of a supportive practice environment. In the Arab and Palestinian context, fostering a supportive practice environment could significantly enhance PCC, which is critical for improving patient satisfaction and outcomes. These findings are consistent with previous research indicating that a positive practice environment enhances PCC practices (Shin & Yeom, 2021). Previous studies have demonstrated an association between nurse practice environments and improved patient outcomes (Klaus et al., 2012; Membrillo-Pillpe et al., 2023). Also, a study by Carthon et al. (2020) examined practice environments associated with PCC using a cross-sectional survey design of nurse practitioners (NPs) across four states in the United States. The results showed that practice environments classified as good (23.6%) were significantly more involved in PCC, particularly in integrating patients’ preferences. In contrast, environments classified as bad (76.3%) were not involved in PCC. Additionally, the study found that practice environments supported with adequate resources were more likely to promote the provision of PCC. However, unlike the current study, Carthon et al. (2020) conducted their research among NPs rather than bedside nurses. This distinction is important because NPs often have different roles, responsibilities, and levels of autonomy compared to bedside nurses, which can influence their perceptions and implementation of PCC. The focus on NPs in their study may account for differences in findings related to practice environments and PCC practices.
The current study found that age, educational level, and the practice environment significantly affect PCC. In Palestinian healthcare settings, enhancing the practice environment through improved management practices and resource allocation could lead to notable advancements in care quality. These findings align with previous qualitative research highlighting the importance of workload, organizational leadership, support, motivation, and practice environment in delivering PCC (Moore et al., 2017; Nkrumah & Abekah-Nkrumah, 2019). Additionally, the study revealed that while nurses’ background characteristics generally do not impact PCC, age and education level do. Older nurses tend to demonstrate greater empathy, effective communication, responsiveness to patients’ perspectives, and collaborative decision-making. Previous evidence supports that older nurses are also more adept at involving patients as active participants in their care plans (Malfait et al., 2017).
Strengths of the Study
This study represents the first of its kind conducted in Palestine. By employing a comprehensive set of variables to analyze both the practice environment and PCC, the study offers a thorough understanding of the factors influencing care quality. This extensive approach allows for an in-depth examination of various dimensions of the practice environment and their effects on PCC.
The use of multiple statistical methods, including correlation and regression analyses, enhances the robustness of the findings. These rigorous statistical techniques are instrumental in identifying significant predictors and elucidating the relationships between different variables. Furthermore, the study's focus on Palestinian healthcare settings provides context-specific insights that are essential for addressing the unique challenges in these regions. This contextual emphasis aids in designing targeted interventions and policies to improve healthcare outcomes within these specific settings.
Limitations of the Study
The study has limitations such as the use of convenience sampling and the geographic constraints of the research setting.
Recommendations
While a substantial body of research on PCC exists, focusing primarily on quality, safety, and patient satisfaction, there are several areas where further investigation is needed. Future research should involve larger sample sizes across multiple healthcare organizations and utilize diverse data collection methods to enhance the robustness of the findings. Additionally, examining variables such as working experience and educational background can provide further validation of results.
The use of self-report measures to assess nurses’ perceptions of PCC may introduce bias, highlighting the need for future studies to incorporate more objective data collection methods. As PCC remains a foundational pillar of high-quality care, ongoing research should aim to address and mitigate barriers that nurses face in delivering PCC. This will ultimately benefit patients, nurses, and healthcare organizations.
Furthermore, future studies could explore the comparison between patients’ perceptions of PCC and those of nurses. Incorporating feedback from both patients and nurses will provide a more comprehensive understanding of care quality and enhance the development of effective interventions.
Conclusion
This study provides valuable insights into the practice environment and its relationship with PCC among nurses in ICU settings. The findings underscore the importance of a supportive practice environment in enhancing various aspects of PCC. The PCC is considered essential to achieving high-quality care.
The moderately favorable practice environment, characterized by strong nursing foundations for quality of care and high managerial support, highlights the strengths within the current healthcare settings. However, the study also reveals areas needing improvement, particularly in staffing and resource adequacy, to further enhance PCC. Also, the current study indicated that perception of PCC was generally high level of competency among nurses.
The significant positive correlations between the practice environment and all aspects of PCC, especially respecting patients’ perspectives and overall competency, emphasize the integral role of a supportive work environment. Also, the current study revealed that age, educational level, and the practice environment significantly influence the level of PCC provided.
Supplemental Material
sj-docx-1-son-10.1177_23779608251321365 - Supplemental material for The Relationship Between the Nurse Practice Environment and Perceived Patient-Centered Care in Intensive Care Units: Nursing Perspective
Supplemental material, sj-docx-1-son-10.1177_23779608251321365 for The Relationship Between the Nurse Practice Environment and Perceived Patient-Centered Care in Intensive Care Units: Nursing Perspective by Musab Bardhia, Ahmad Batran, Ahmad Ayed, Moath Abu Ejheisheh, Bahaa Alassoud and Ibraheem Abu-Siam in SAGE Open Nursing
Supplemental Material
sj-docx-2-son-10.1177_23779608251321365 - Supplemental material for The Relationship Between the Nurse Practice Environment and Perceived Patient-Centered Care in Intensive Care Units: Nursing Perspective
Supplemental material, sj-docx-2-son-10.1177_23779608251321365 for The Relationship Between the Nurse Practice Environment and Perceived Patient-Centered Care in Intensive Care Units: Nursing Perspective by Musab Bardhia, Ahmad Batran, Ahmad Ayed, Moath Abu Ejheisheh, Bahaa Alassoud and Ibraheem Abu-Siam in SAGE Open Nursing
Footnotes
Acknowledgments
The authors would like to express their thanks to the nurses who participated in the study
Consent for Publication
The authors affirm that this work is original and has not been published elsewhere, except as noted in the manuscript.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
Ethical approval for this study was obtained from Palestine Ahliya University (CAMS/CCNA/27/524). Written informed consent was obtained from all subjects before the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this paper is available online.
Use of AI Software
The authors affirm that the integrity and originality of this work are entirely their own and are not influenced by any AI technology.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.