
Abstract
Introduction
Head and neck cancer is the sixth most common type of cancer globally, with treatment often involving radiotherapy, which can significantly affect patients’ quality of life and lifestyle. Patient education is crucial in managing the side effects of radiotherapy and improving outcomes.
Aim
This study aims to assess the effect of implementing educational guidelines on radiotherapy side effects on the lifestyle and quality of life of patients with advanced head and neck cancer.
Method
A one-group pre- and posttest quasiexperimental design was utilized for this study, which was conducted at the radiation therapy outpatient clinic and the Clinical Oncology Department. A purposive sampling method was used to select 100 patients diagnosed with head and neck cancer who were undergoing radiotherapy. Data collection involved a structured questionnaire that captured patient characteristics, medical history, the Health-Promoting Lifestyle Profile, and the SF-36 quality of life questionnaire.
Results
There was a statistically significant improvement in both the quality of life and lifestyle of the patients after the intervention. Nearly two-thirds of patients had a low quality of life preintervention, which reduced to one-fifth postintervention (p < .05). Lifestyle improvements were also observed across all domains, with significant increases in physical activity, nutrition, and stress management.
Conclusion
The study concluded that implementing educational guidelines on radiotherapy side effects can significantly enhance the lifestyle and quality of life of patients with advanced head and neck cancer. However, the study's limitations, including the lack of a control group and reliance on self-reported data, suggest the need for further research with more robust designs.
Keywords
Introduction
Head and neck cancer (HNC) ranks as the sixth most prevalent cancer globally, with approximately 600,000 new cases and 350,000 deaths reported annually (Fernandes et al., 2020). Typically, this type of cancer is detected in its advanced stages. HNC encompasses malignancies in the mouth, larynx, oropharynx, salivary glands, and various parts of the pharynx (Hamilton et al., 2019). Patients with HNC frequently experience weight loss, muscle wasting, and functional decline both during and after treatment. These issues arise due to the tumor locations, nutritional challenges, inflammatory responses associated with the tumors, and the side effects of treatments (Senchak et al., 2019).
Head and neck cancer presents significant treatment challenges due to the need for complex surgeries, radiation, and/or chemotherapy, each of which introduces specific difficulties for patients (Fernandes et al., 2020; Machiels et al., 2020). Treatment often involves altering critical areas of the body responsible for speech, eating, and breathing. As a result, patients may experience functional issues such as dysphagia and respiratory difficulties, along with physical, psychological, and social complications (Britton et al., 2019).
Radiotherapy (RT) plays a vital role in the curative treatment of various cancers, either as a standalone therapy or in combination with chemotherapy, hormone therapy, immunotherapy, and/or surgery (De Felice et al., 2016; Mayo et al., 2022). However, there is a significant gap in the care and support provided to head and neck cancer patients during the critical period following treatment (Yan et al., 2021). Inadequate nursing care, where essential care to meet patients’ needs is omitted, has been linked to low-quality care (Deribe et al., 2021). There is a pressing need for increased professional assistance in areas such as physical care, lifestyle programs, social care, and mental health support. Effective strategies to manage treatment side effects are crucial for preserving patients’ functionality and quality of life (Kazoba & John, 2021). Despite its effectiveness, RT still causes a range of side effects that adversely affect patients’ quality of life (QoL). Fatigue is one of the most commonly reported symptoms among cancer patients undergoing RT, affecting over 65% of them (Tribius et al., 2021). Additionally, around 30% of RT patients experience a decline in psychosocial functioning (Hess & Chen, 2014).
The lifestyle and QoL of patients undergoing radiotherapy for HNC is often severely impacted by the treatment and its side effects. Poor nutritional intake, reduced physical activity, and psychological stress are common among these patients, further complicating their overall health status (Kazoba & John, 2021). Educational interventions that address lifestyle modifications, such as dietary adjustments, exercise routines, and stress management techniques, can play a significant role in improving patients’ ability to cope with the demands of their treatment. Moreover, promoting a healthier lifestyle can contribute to better treatment tolerance and recovery (Kazoba & John, 2021).
Nurses are essential in educating patients with advanced head and neck cancer about the lifestyle impacts of radiotherapy’s side effects. They deliver tailored patient education, help manage expectations, and provide support for coping with both physical and emotional challenges during and after treatment. Additionally, nurses encourage lifestyle modifications to improve treatment outcomes, closely monitor patient progress, and ensure effective communication with the healthcare team. By equipping patients with the necessary knowledge and support, nurses play a crucial role in enhancing the quality of life and overall well-being of those undergoing radiotherapy for advanced head and neck cancer (Braat et al., 2022).
Review of Literature
Karvonen-Gutierrez et al. (2008) conducted a study using the Short Form-36 (SF-36) scale, where they reported mean scores of 42.3 for the physical component and 44.7 for the mental component. Both scores are below the average norms of the general population. Similarly, research by Karimi et al. (2019) found a significant decline in QoL for patients undergoing HNC treatment, particularly concerning functions and symptoms. Additionally, the study by Lee et al. (2023) concluded that the Nurse-Led Survivorship Care Program positively impacted the primary caregivers of HNC patients by reducing emotional distress, enhancing social support, improving mental and physical health, and bolstering resilience. Additionally, Elkader et al. (2022) highlighted the importance of nursing instructions in minimizing treatment-related complications such as oral mucositis and pain, as well as in improving hemoglobin levels.
Despite these efforts, 60% to 70% of individuals with HNC experience unmet needs after therapy (Hunter et al., 2020). The transition back to “regular life” can be challenging, but certain supportive interventions may help. There is a clear and pressing need to develop new educational guidelines to better address lifestyle concerns and meet the needs of HNC survivors (Nehlsen et al., 2022). So, the current study aimed to assess the impact of implementing educational guidelines on radiotherapy side effects and their influence on the lifestyle of patients with advanced head and neck cancer.
Hypothesis
Implementing educational guidelines on radiotherapy side effects may improve the lifestyle and QoL of patients with advanced HNC.
Methods
Design
A one-group pre- and posttest quasiexperimental design.
Setting
The study was conducted at the radiation therapy outpatient clinics within the Clinical Oncology Department and the Radiotherapy Unit at the Hospital.
Sample Size and Power
Using OpenEpi with a 95% confidence interval, a type 1 alpha error of 0.05, and a type 2 beta error (1-β) of 80%, the estimated sample size was determined to be 100 patients.
Respondents
The study involved 100 patients diagnosed with HNC who were undergoing radiotherapy, either alone or in combination with chemotherapy, selected using a purposive sampling method.
Inclusion Criteria
Patients diagnosed with advanced head and neck cancer Individuals undergoing radiotherapy as a primary or combined treatment Patients aged 18 years or older Patients able to provide informed consent and participate in educational sessions Individuals willing to participate throughout the study's duration
Exclusion Criteria
Patients with mental or cognitive impairments that hinder their understanding of the questionnaires or sessions Patients who had previously undergone radiotherapy for head and neck cancer Individuals not undergoing active radiotherapy during the study period Patients unwilling to participate or unable to attend scheduled educational sessions
Instruments
Part I: Characteristics of patient included age, gender, marital status, education level, and job.
Part II: Medical history included onset of cancer, type of cancer, surgical operation, type of treatment, and type of cancer cell.
Part III: Health-Promoting Lifestyle Profile . This section utilized the Health-Promoting Lifestyle Profile developed by Walker et al. (1987), which includes 52 items organized into six subscales. Each item scored through four-point Likert scale (never, sometimes, often, routinely). Higher mean scores indicate more frequent engagement in the described behaviors. For analysis, the lifestyle scores were categorized as follows: less than 50% indicated the least healthy/poor lifestyle, 50% to less than 70% was considered moderate, and 70% or more was classified as the healthiest/good lifestyle (Hansen et al., 2020).
Part IV: The SF-36 quality life questionnaire was developed by Ware and Sherbourne (1992). It consists of 36 items divided into eight domains. Each item was scored using a Likert scale ranging from 1 to 5, with higher scores on the SF-36 indicating better health-related QoL. Total QoL is categorized as low if the score is less than 50%, moderate (50% to 70%), and high if above 70% (Magiera & Pac, 2022). A mean score of less than 50 suggests a below-average health status (Ware et al., 1993) (Online supplemental material).
Validity and Reliability
The content's validity was assessed by a panel of five specialists in medical-surgical nursing, who provided feedback on the format, layout, consistency, accuracy, and relevance of the tools. A statistician then evaluated the reliability of the modified instruments using Cronbach's alpha test. The internal consistency reliability was found to be good for the lifestyle scale (α = .823) and excellent for the QoL scale (α = .913).
Field Work
This study was conducted over a 6-month period, from November 1, 2022, to April 30, 2023. The researcher visited the hospital three times a week to conduct patient interviews and collect data. Each interview took approximately 30 min to complete the questionnaire. The study was divided into three phases: a two-month preintervention phase, a two-month intervention phase, and a two-month postintervention phase.
In the preintervention phase, participants were interviewed to clarify the study's objectives and importance. At the beginning of the study, a structured interview questionnaire was administered to the patient sample as a pretest. Patient education was organized by dividing the participants into eight groups, with each group receiving four educational sessions over the course of 1 week.
The intervention aimed to educate patients about maintaining a healthy lifestyle, covering topics such as diet, exercise, rest and sleep, and stress management. The lifestyle guidelines were developed based on the needs and demands identified during the preintervention phase and informed by the latest relevant literature. Educational sessions utilized visual and digital written resources, and participants were provided with an informational booklet to reinforce the content.
Session 1: Introduction to Head and Neck Cancer and Radiotherapy
Objective: To introduce patients to their diagnosis and treatment, helping them understand radiotherapy and its side effects.
Content: Overview of head and neck cancer, tumor locations, and common symptoms; explanation of radiotherapy, how it works, and its role in cancer treatment, typical side effects (e.g., fatigue, dry mouth, mucositis) and what to expect during treatment, and importance of lifestyle modifications in supporting treatment outcomes.
Session 2: Coping with Side Effects and Stress Management (Duration: 90 min)
Objective: To help patients manage common side effects of radiotherapy and develop effective stress management techniques.
Content: Fatigue—strategies to conserve energy and scheduling rest breaks. Oral care: Preventing and managing mucositis (using saline rinses) and preventing infections. Skincare: Guidelines for managing radiation-induced skin irritation. Stress management: Introduction to relaxation techniques (e.g., deep breathing, progressive muscle relaxation) and mindfulness practices.
Session 3: Lifestyle Modifications—Nutrition and Physical Activity (Duration: 90 min)
Objective: To promote healthy eating and physical activity routines to support treatment outcomes and improve patients’ overall well-being.
Content: Nutrition—importance of high-protein and calorie-dense meals to prevent weight loss, hydration guidelines, and managing appetite loss. Physical activity: Recommended exercises (walking, light stretching), tips for staying active during treatment, and overcoming fatigue. Smoking and alcohol cessation: Encouraging patients to quit smoking and limit alcohol to improve treatment response and recovery.
Session 4: Creating Long-Term Health Plans and Building a Support Network
Objective: To empower patients to develop personalized health plans and establish supportive relationships with caregivers and healthcare providers.
Content: How to set realistic health goals and monitor progress. Developing a personal health plan with tailored nutrition, exercise, and rest schedules. Role of social support: Building connections with family, friends, and cancer survivor groups. Planning follow-up care and consultations with healthcare providers.
The evaluation phase is a critical step in assessing the effectiveness, success, or outcomes of an implemented approach. Two months after the intervention, a posttest was conducted to evaluate the impact of nursing management on the patients’ QoL.
Ethical Considerations
The study was granted ethical approval by the institutional review board of the Faculty of Nursing. Prior to participation, written consent was obtained from each patient. The research objective was clearly stated in writing at the beginning of the survey. Participants were informed that all collected data would remain anonymous, with no identifying information included in the questionnaire. They were also made aware that they could withdraw from the study at any time. All participant data were anonymized during collection. Each participant was assigned a unique code, and no identifying information (such as names or contact details) was linked to their responses in the dataset. Collected data were securely stored on encrypted devices and only accessible to the research team. Hard copies of any data (such as consent forms) were stored in locked cabinets within the research institution. Only authorized members of the research team had access to the data for analysis, and all team members signed confidentiality agreements.
Data Analysis
The collected data were encoded and entered into (SPSS 24) software. After completing the data entry, the information was checked for errors. The data were then analyzed using the same software, which was used to generate frequency tables with percentages. Quantitative data were described through mean and standard deviation. A dependent t-test was used to compare means of lifestyle and quality of life pre- and postintervention. A result was considered statistically significant at p ≤ .05.
Results
As shown in Table 1, this study was conducted on 100 patients. Regarding their characteristics, the mean age (±SD) was 37.1 ± 5.77 years. More than half (59%) were male. Regarding their educational level, 40% had secondary education. In terms of marital status, more than two-thirds (70%) were married, and 68% were employed.
Characteristics of Studied Patients (n = 100).

Table 2 presents the medical history of the studied patients. The onset of cancer was ≤12 months for 41% of the patients. Less than two-thirds (61%) had no history of surgical operations. Additionally, 20% had sinonasal cancer, and more than one-third (40%) underwent surgery combined with radiation as treatment.
Medical History of Studied Patients (n = 100).

Table 3 presents the QoL scores of patients before and after the implementation of educational guidelines. The results reveal statistically significant improvements across all measured domains after intervention, including physical functioning, role physical, bodily pain, general health, vitality, social functioning, role emotional, and mental health (p < .05 for all). The overall QoL score also showed a significant increase after the intervention. These findings indicate that the educational guidelines had a positive impact on enhancing the QoL for patients with advanced head and neck cancer undergoing radiotherapy.
Quality Life of Studied Patients Pre- and Postintervention (n = 100).

Table 4 displays the lifestyle scores of patients before and after the educational intervention. The data show significant improvements in all lifestyle domains, including responsibility for health, physical activity, nutrition, spiritual growth, interpersonal relations, and stress management (p < .05 for all). The total lifestyle score increased substantially after the intervention, suggesting that the educational guidelines effectively promoted healthier lifestyle behaviors among the patients, contributing to their overall well-being during radiotherapy treatment.
Lifestyle of Studied Patients Pre- and Postintervention (n = 100).

The multiple linear regression model (Table 5) analyzes the impact of several predictors on quality of life (QoL). Significant predictors include age (B = −0.224, p = .014*), history of surgical operation (B = −0.252, p = .003**), and stage of the tumor (Stage IV) (B = −0.465, p = .002**), suggesting that older age, previous surgeries, and advanced tumor stages negatively affect QoL. Other variables, such as work status, number of months from diagnosis, and treatment during the study (chemoradiation), do not significantly impact QoL, with p-values above 0.05. The ANOVA results indicate that the overall model is statistically significant (F = 7.942, p = .001), with an R-value of 0.56 suggesting a moderate correlation between the predictors and QoL. The R² value of 0.31 reveals that 31% of the variability in QoL can be explained by the model, leaving room for additional factors not captured in this analysis.
Multiple Linear Regression Model.

Dependent variable: quality of life.
Predictors: (constant) age, work (job), number of months from diagnosis, history of surgical operation (yes), treatment during the study (chemoradiation), stage of tumor (Stage IV).
Figure 1 shows that two-thirds of the studied patients (65%) had a low QoL before the intervention, while about one-fifth (20%) had a low QoL after the intervention.
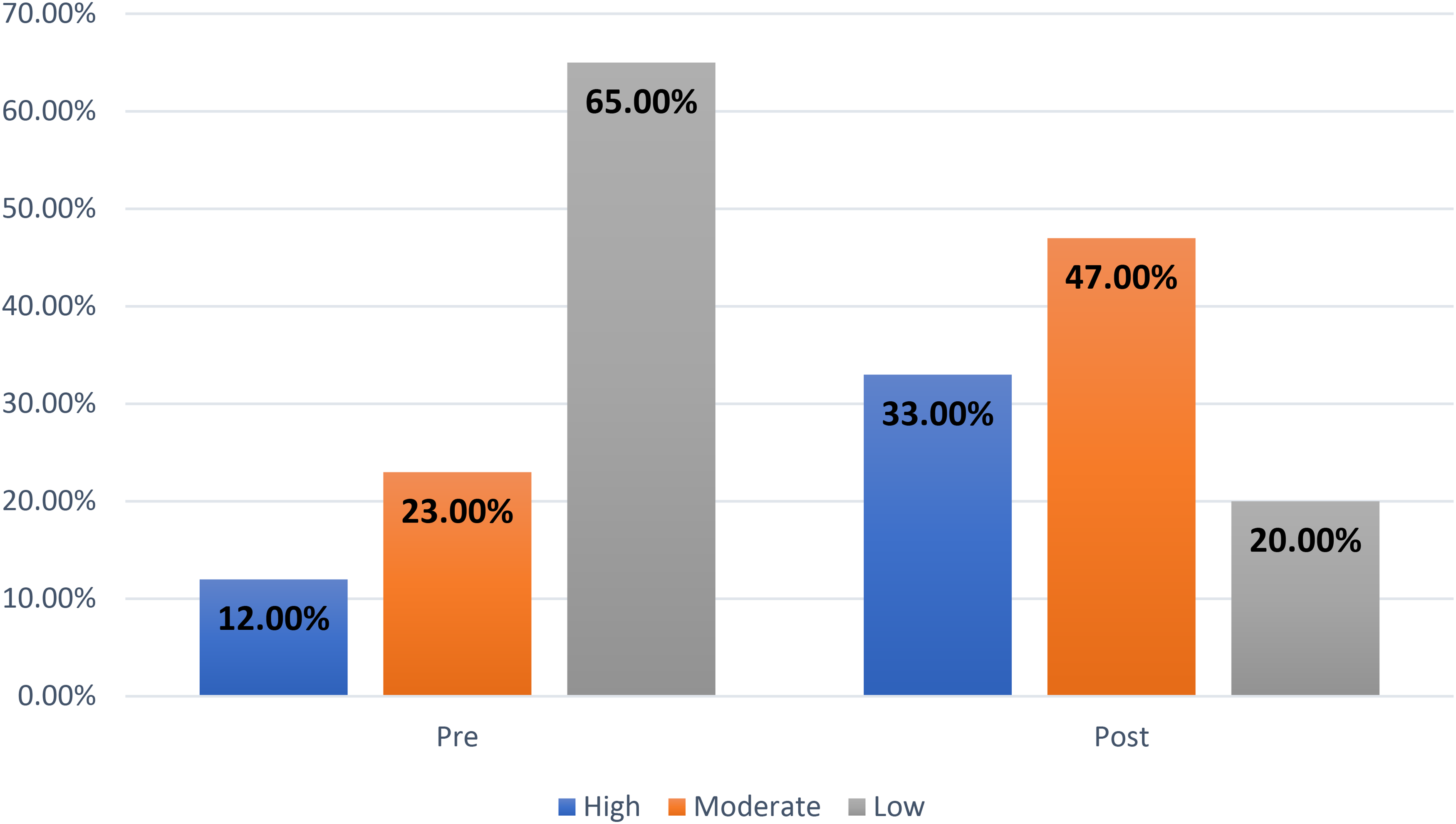
Total quality life of studied patients pre- and postintervention (n = 100).
Figure 2 presents the total lifestyle before and after the intervention. More than half of the studied patients (56%) had a poor lifestyle before the intervention, while about one-fifth (19%) had a poor lifestyle after the intervention.
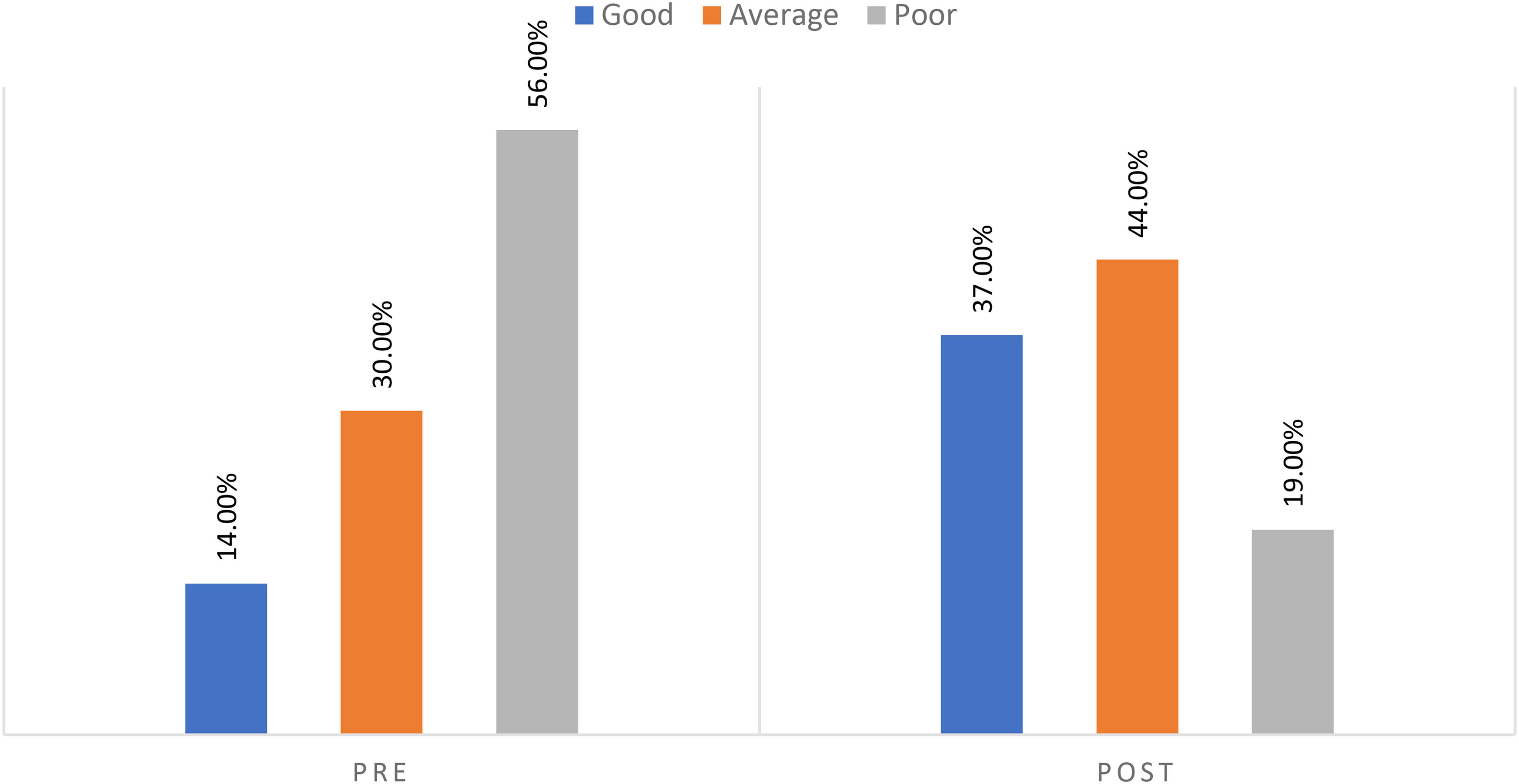
Total lifestyle of studied patients pre- and postintervention (n = 100).
This figure illustrates the distribution of patients across the four TNM stages. The data show a steady increase in the number of patients from Stage I to Stage III, peaking at 35 patients in Stage III. A slight decline is observed at Stage IV, with 30 patients; see Figure 3. Also, the bar chart shows the distribution of patients receiving different types of chemotherapy. The highest number of patients (10) was treated with paclitaxel, followed closely by combination therapy with seven patients. Carboplatin and cisplatin were administered to eight and five patients, respectively; see Figure 4.
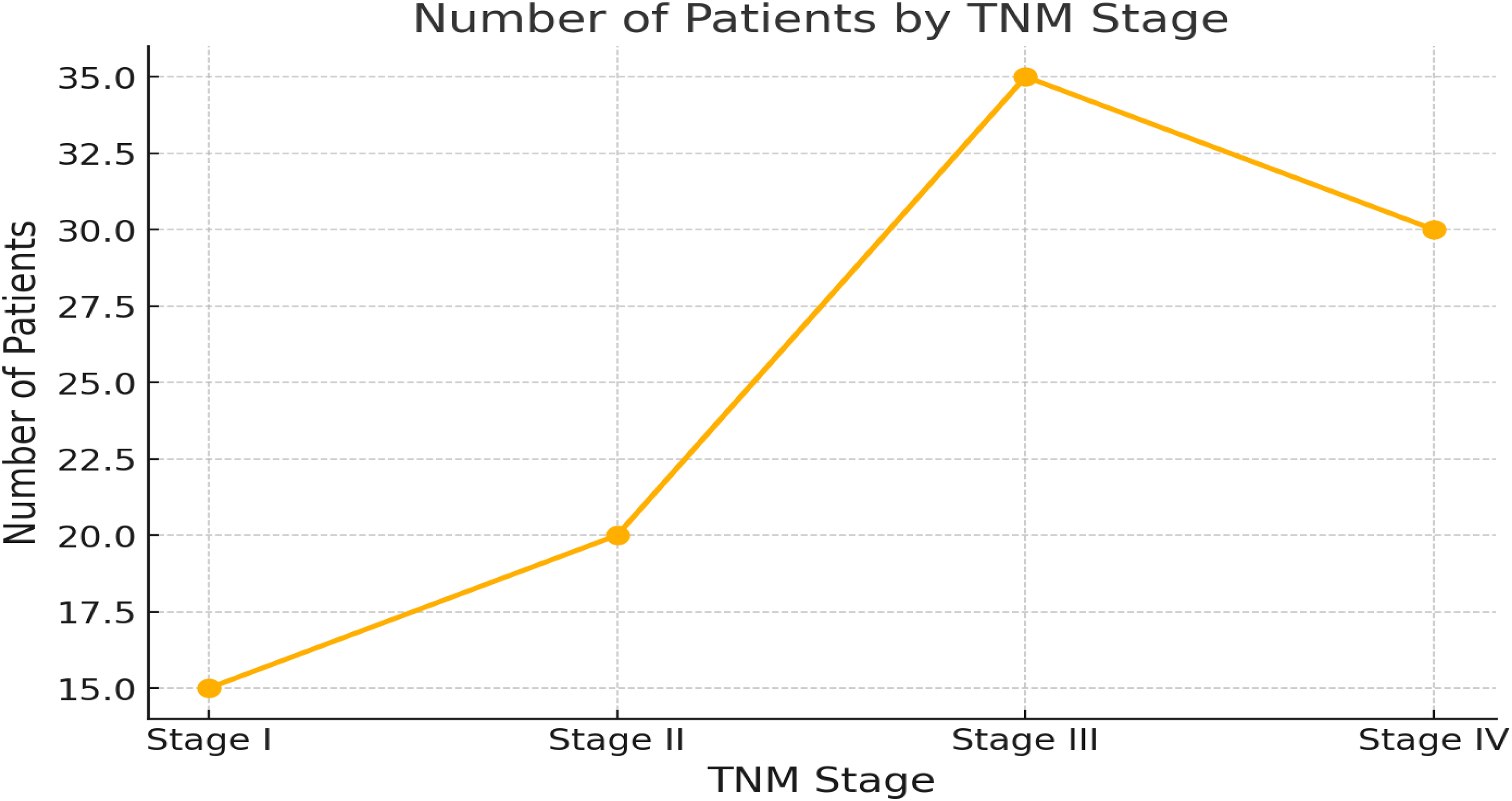
Distribution of patients by TNM stages.

Distribution of patients by type of chemotherapy.
Discussion
Radiation oncology remains one of the most misunderstood cancer treatment methods. Many patients are less familiar with radiation compared to chemotherapy or surgery and often struggle to grasp the more complex aspects of treatment. Therefore, patient education is crucial in this field, as it enhances knowledge and understanding and can potentially influence treatment-related behaviors (Brook, 2020). This study aimed to assess the impact of implementing educational guidelines on QoL and lifestyle among patients with advanced HNC.
According to the medical history of the patients, over one-third had been diagnosed with cancer within the last 12 months. Less than two-thirds had no history of surgical operations. Additionally, one-fifth was diagnosed with sinonasal cancer, and more than one-third underwent a combination of surgery and radiation as treatment. These findings differ from those reported by Bonomo et al. (2020), who found that the most common primary site for head and neck carcinoma was the oral cavity (33.7%), followed by the oropharynx (23.5%) and nasopharynx (17.8%). However, the results are consistent with the study by López-Jornet et al. (2012), which showed that more than two-thirds of patients had squamous cell carcinoma, with about one-quarter receiving both surgery and radiation as treatment. Additionally, Rani (2021), who conducted a quantitative, nonexperimental, descriptive study on 30 cancer patients, found that most of the studied patients had not undergone surgical operations.
Additionally, nearly two-thirds of the studied patients had a low QoL before the intervention, while about one-fifth had a low QoL after intervention. The implementation of educational guidelines on radiotherapy side effects significantly improved the quality of life among these patients, as indicated by a p-value of <.05*. These results may be attributed to the effectiveness of the training program, which was designed by the researcher based on the patients’ needs prior to the intervention. Zhang et al. (2022) reported that patients with lung cancer undergoing radiotherapy or chemotherapy experienced better treatment compliance, self-efficacy, lung function, and QoL with evidence-based nursing interventions. Similarly, Nguyen et al. (2018) found that psychological nursing care helped cancer patients undergoing chemotherapy manage anxiety and depression, leading to improved sleep quality. Saeed (2018) also stated that educational training about radiation therapy could enhance patient satisfaction and QoL. However, Fernandes et al. (2020) found that an educational video did not significantly affect patients’ depression, anxiety, or QoL, though all patients expressed high satisfaction with the video.
Regarding the lifestyle changes among the studied patients before and after the intervention, there was a statistically significant improvement in physical activity (T = 4.028, p < .05*), as well as in all other lifestyle factors measured. The educational intervention positively impacted the patients’ lifestyles. These findings align with Arnos et al. (2020), who reported significant improvements across all lifestyle domains following the implementation of a guideline for cancer patients undergoing chemotherapy. Similarly, Nady et al. (2018) found that a planned teaching program had a positive effect on the lifestyle of patients with gynecologic cancer. Additionally, Harby et al. (2019) observed that a nursing education program led to significant improvements in the knowledge and management of acute radiotherapy side effects among lung cancer patients.
Limitation of the Study
The study utilized a one-group pre- and posttest design without a control group for comparison. This lack of a control group makes it difficult to determine whether the observed changes in lifestyle and QoL were solely due to the intervention or if other external factors played a role. Additionally, the study had a limited follow-up period and relied on self-reported data, which could introduce biases and inaccuracies.
The two-month postintervention period may not fully capture the long-term lifestyle and QoL changes. Future studies with longer follow-up periods are recommended to provide a more comprehensive evaluation of the sustainability of educational interventions.
Conclusion
Participants reported improvements in lifestyle and QoL across multiple domains after implementing educational guidelines on radiotherapy side effects; however, these findings should be interpreted with caution due to the lack of a control group for comparison. The findings suggest that tailored patient education, based on individual needs and delivered through a structured program, can effectively address the challenges faced by these patients during and after treatment.
However, the study's design limitations, including the absence of a control group, the reliance on self-reported data, and the limited follow-up period, highlight the need for further research. Future studies should incorporate control groups and longer follow-up periods and consider varying educational needs based on the timing of radiotherapy to better understand the full impact of such interventions.
Implications for Nursing Education and Practice
This study underscores the critical role of nursing education in enhancing QoL and lifestyle management for patients undergoing radiotherapy for advanced HNC. For nursing education, the findings highlight the importance of incorporating comprehensive training on patient-centered educational interventions, particularly those addressing the side effects of radiotherapy. Nursing curricula should emphasize the development of skills necessary to assess patient needs, deliver tailored educational programs, and evaluate their effectiveness.
In clinical practice, nurses should prioritize ongoing patient education as a standard component of cancer care, focusing on individualized strategies to manage the physical, emotional, and social challenges associated with radiotherapy. Additionally, the study suggests that nurses play a pivotal role in providing consistent follow-up care to reinforce lifestyle modifications and support long-term well-being. Integrating these educational guidelines into routine practice can lead to improved patient outcomes, satisfaction, and overall QoL.
Supplemental Material
sj-docx-1-son-10.1177_23779608251317809 - Supplemental material for Impact of Educational Guidelines on Radiotherapy Side Effects and Lifestyle in Patients With Advanced Head and Neck Cancer
Supplemental material, sj-docx-1-son-10.1177_23779608251317809 for Impact of Educational Guidelines on Radiotherapy Side Effects and Lifestyle in Patients With Advanced Head and Neck Cancer by Gehan Abd Elfattah Atia Elasrag, Maha Suwailem S Alshammari, Marwa Mohamed Ahmed Ouda, Rasha Abdulhalim Alqadi, Ahmed Hendy, Abdelaziz Hendy and Salwa Abd El Gawad Sallam in SAGE Open Nursing
Footnotes
Author Contributions
G.E. and M.A.: conceptualization; M.O, R.A, and S.S.: resources; M.O, R.A, and S.S.: data curation; A.H. and A.H.: formal analysis; G.E. and M.A.: supervision; M.O, R.A, and S.S.: funding acquisition; A.H. and A.H.: validation; A.H. and A.H.: statistical analysis; M.O, R.A, and S.S.: visualization; A.M.A. and B.A.: methodology; G.E. and M.A.: writing—original draft; all authors: project administration, writing—review and editing.
Data Availability
All data needed are available in the article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Considerations
The study was granted ethical approval by the institutional review board of the Faculty of Nursing at Menoufia University (IRB approval number 940, 18/1/2023). Prior to participation, written consent was obtained from each patient. The research objective was clearly stated in writing at the beginning of the survey. Participants were informed that all collected data would remain anonymous, with no identifying information included in the questionnaire. They were also made aware that they could withdraw from the study at any time.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.