
Abstract
Introduction
Knee osteoarthritis (KOA) is one of the most common and prevalent debilitating chronic diseases across the world with various adverse effects such as pain and movement limitations which impact the health status and quality of life of the patients in the long run.
Objectives
This study aimed to investigate the effects of self-care education on pain, quality of life, and consequences of disease in patients with KOA in Southern Iran.
Methods
This is a randomized controlled clinical trial using a pretest–posttest design. Eighty patients with KOA were enrolled in this study and randomly allocated to a control and an intervention group. The data collection instruments included VAS: Visual Analog Scale, the SF-36 quality of life scale, and the Knee Injury and Osteoarthritis Outcome Score. The collected data were analyzed through SPSS v. 22, using descriptive tests, paired t-tests, independent t-tests, Chi-square, and ANOVA. A P level of <.05 was considered as the significant level.
Results
Before the self-care educational intervention, no statistically significant difference was found between the control and intervention groups in pain intensity, quality of life, and consequences of osteoarthritis. After the self-care educational intervention, the findings revealed a significant difference between the intervention group's mean ± standard deviation for pain intensity (41.25 ± 21.74), quality of life (49.87 ± 14.74), and consequences of KOA (39.06 ± 12.15), respectively (P < .05). However, in the control group, there was no significant difference.
Conclusion
Based on the results of this study, the positive effect of self-care education on patients with osteoarthritis was shown as to their pain intensity, quality of their lives, and reduction of the disease consequences. Thus, healthcare managers are recommended to apply this type of intervention for patients with osteoarthritis.
Introduction
Knee osteoarthritis (KOA) is one of the most common chronic diseases which leads to disability worldwide, imposing a substantial and increasing health burden (Wangl et al., 2020). As one of the top 10 debilitating diseases in the world, KOA causes limitations in performing daily activities in 80% of the patients (Kiadaliri et al., 2018). The prevalence of symptomatic KOA and radiographic KOA in patients over 60 years of age ranges from 10.0 to 16.0% and 35.0 to 50.0% (Cho et al., 2015; Nguyen et al., 2011; Postler et al., 2018), respectively. Approximately 250 million people have KOA worldwide, with a two-fold increased prevalence in men and a threefold increased prevalence in women in the USA over the past 20 years (Deshpande et al., 2016). In a study carried out by Dehghan et al., it was shown that the prevalence of KOA in Iran had a rising trend ranging from 11.7% in 2012 to 18.7% in 2021 (Dehghan et al., 2021). In a systematic review conducted by Conley et al. (2023) which aimed to evaluate the quality of clinical practice guidelines for interventions used to investigate osteoarthritis (OA), patient-centered care including exercise, education, and weight loss (where appropriate) was recommended. Also, a study conducted in 2023 suggested nonsteroidal anti-inflammatory drugs and surgical interventions for disabling OA which had not responded to nonsurgical care (Conley et al., 2023). The purpose of treatment in OA patients is to relieve pain and inflammation and improve or maintain mobility, function (including daily life activities), and health-related quality of life (Larmer et al., 2014). Even though various treatment modalities, from analgesics as the least intense and total knee replacement surgery as the most intense, have been applied, which treatments are the most effective ones for each patient has remained unclear (Brophy & Fillingham, 2022). Based on the American Rheumatism Association guidelines for the treatment of OA patients, patient education, weight control, exercise, assistive devices, physical therapy, and occupational therapy should be included as nonpharmacological therapies. It has been suggested that patients should be encouraged to take part in self-care programs (Charlesworth et al., 2019). According to World Health Organization, self-care encompasses the activities that individuals, families, and societies perform to promote health, prevent and control diseases, and regain health (Martínez et al., 2021).
Review of the Literature
Self-care behaviors also include the medical, behavioral, psychological, and emotional acts that individuals perform to take care of themselves. Research shows that appropriate self-care behaviors can effectively improve the communication between the healthcare experts and patients, reduce emotional stress in patients, and enhance the patients’ awareness of diseases, all of which contribute to patients’ quality of life (Hughes et al., 2020). Educating patients with OA in self-care will enable them to reach a health status at which they can not only enjoy a satisfactory personal life but also be a useful member of their society. Motivating patients to adopt appropriate self-care behaviors is a key factor in managing arthritis (Narasimhan et al., 2019). Implementing the Enabling Self-management and Coping with Arthritic Pain using Exercise, ESCAPE-pain, in community venues facilitates improved access and continuous support for individuals with chronic joint pain (Hurley et al., 2022). Also Delivering ESCAPE-pain in the community could facilitate access to effective care and on-going support to sustain the benefits of healthcare programs producing a more efficient use of health care costs and community resources (Hurley & Thompson, 2024).
It is not easy to conclude whether self-care programs for KOA are effective or not due to the variability in the structure of previous studies; they have not been in the same line in terms of different types of arthritis, interventions, and behavior models, as well as variations in trial structures and the outcome measurements (de Rezende et al., 2016; Keefe et al., 2004). In addition, although self-care programs have been confirmed to be effective in different countries (Allen et al., 2016; Hurley et al., 2022; Norozi et al., 2020), such programs should be specific to local culture and adjusted to the ethnic group (Heuts et al., 2005). Moreover, the medical costs of treating patients with OA can make a significant dent in a nation's revenue, emphasizing the need for strategies that can diminish medical and nonmedical costs. Thus, further studies are required to clarify the effectiveness of self-care education among patients with KOA. This study aimed to evaluate the efficiency of self-care education on pain, quality of life, and consequences of disease in patients with KOA in southern Iran.
Methods
Study Design
This is a randomized controlled clinical trial conducted on an intervention and a control group, with no blinding. The participants received treatment at two teaching hospitals in the south of Iran from June to October 2021. We explained the objectives of the study to the participants and obtained their informed consent. In the present study, to determine the quality of the randomized controlled trial, we used the CONSORT (Consolidated Standards of Reporting Trials) checklist (Schulz et al., 2010). Supplementary file: CONSORT checklist.
Research Question
Is there a difference between the pretest and posttest mean scores on pain, quality of life, and consequences of OA in patients who have undergone education on self-care?
Hypotheses of the Study
There is a difference between the pretest and posttest mean scores on pain, quality of life, and consequences of OA in patients who have undergone education on self-care.
Sample Size and Study Population
In this study, we calculated the sample size based on Mirzaee et al.'s study, with a power of 80% and α = 0.05, using a formula (Mirzaee et al., 2016). The sample size was estimated at 30 subjects for each group, which was increased to 40, given the possibility of sample loss.
The Inclusion and Exclusion Criteria
The inclusion criteria were a definite diagnosis of KOA by orthopedic specialists using clinical outcomes and radiologic features of OA, as described by Kellgren and Lawrence (KL). The knee radiographs were used to originally describe the KL classification. Each radiograph was allocated a grade from 0 to 4, which correlated with increasing severity of OA, with Grade 0 indicating absence of OA and Grade 4 signifying severe OA (Kohn et al., 2016). The other inclusion criteria were willingness to participate in the study; lack of a history of surgery for OA, for example, joint replacement and joint repair; symptoms and physical signs of knee arthritis (joint pain, morning knee stiffness of 30 min or less; joint swelling; bony crepitation (fremitus); muscle weakness and impairment of movement, bone tenderness, and bone enlargement confirmed by an orthopedist, rheumatologist, and physiotherapist; lack of an intra-articular injection; lack of an acute or chronic mental disorder; and ability to perform self-care independently. The patients whose condition deteriorated during the study or those who did not intend to participate for any reason were excluded.
Randomization
Initially, the researchers invited and enrolled 107 patients with OA. The research team, including nursing professors, orthopedists, and rheumatologists, confirmed the eligibility of the participants. We excluded 27 patients who did not have the inclusion criteria; then, the remaining 80 patients were randomly allocated to an intervention (N = 40) and a control group (N = 40). For random allocation, 80 cards were placed inside an envelope box; 40 cards had the letter A and 40 the letter B written on them. The patients who met the inclusion criteria were asked to pick a card each. Those who picked A were assigned to the intervention group, and the ones who picked B were enrolled in the control group. The patients and researchers were blind to what was on the cards until they had taken them out of the box. Figure 1 presents the consort flow diagram of the participants throughout the study (Figure 1).

Flow diagram of the participant.
Intervention and Follow-up
After the research project was approved by the research department and ethics committee, the researchers obtained the contact information of the patients who met the inclusion criteria and invited them to participate in the study. The second author (ZH), then provided the patients of each ward with clear explanations about the purpose and methodology of the research. If the patients agreed to participate in the study, they were given the questionnaires. The second author (ZH), provided necessary explanations to the patients if they had difficulty understanding the questionnaire. Finally, the collected the completed questionnaires from the patients.
The patients in the intervention group attended four education sessions. The intervention consisted of a 5-session educational program (10 hours a week). The review of educational research was used in the preparation of educational content validity that was verified by seven orthopedic specialists and rheumatologists who were also faculty members and three nursing professors. In the first session, the participants were informed about KOA and the associated symptoms and complications. In the present study, the experiences and expertise of different groups, including orthopedic specialists, physiotherapy and occupational therapists, dieticians, as well as experienced nursing professors (first author [ZJ] and corresponding author [MB]), who are an associate professors of nursing), were used in the development and implementation of the educational program. In other words, interdisciplinary training was used to improve the efficiency of the training program. The content of the training program included knowledge about OA, symptoms of the disease, treatment of the disease, the aggravating factors of the disease, drug therapy and important points about how to take the drugs, adherence to physical exercises and sports to improve the function of the joints, and the importance of follow up of the treatment.
At the end of each session, the participants’ queries were answered, and their learning was assessed through questions and answers and discussions. The patients were provided with a checklist and asked to perform the prescribed stretching exercises every day and frequently practice the correct position of sitting and standing. The researchers emphasized that they should adhere to the exercises. Through phone follow-ups, we provided the participants with counseling, and their queries were answered. The patients in the control group did not undergo any intervention and were only provided with a pamphlet on arthritis care and treatment, food regimen, physical activities, exercising, lifestyle improvement, and the common and uncommon symptoms of arthritis and how to manage them. The questionnaires were filled out by both groups before and two months after the last educational session. The content of the training program is shown in Table 1.
The Content of the Training Program.

Outcome
In this study, three issues were investigated. The main outcome was quality of life, and the secondary outcomes were pain and consequences of disease in patients with KOA.
The Data Collection Tools
The self-reported questionnaire comprised three parts (a) The Visual Analog Scale (VAS), (b) The SF-36 quality of life scale, and (c) KOOS (Knee injury and Osteoarthritis Outcome Score).
Visual Analog Scale
Visual Analog Scale is a simple and popular scale for assessing pain intensity. The pain measurement visual scale is a 100-mm ruler. In the scale, the left end indicates “no pain” (0 points) and the right end shows “the worst pain possible” (100 points). Visual Analog Scale pain scores of 30 mm or less indicate mild pain, scores of 70 mm or more show severe pain, and those from 31 mm to 69 mm denote moderate pain. The test–retest method was used to determine the reliability of the scale, yielding a Cronbach's alpha of 0.79 (Weigl & Forstner, 2021).
The SF-36 Quality of Life Scale
This quality-of-life scale consists of 36 items and 8 domains: physical functioning, functional disorders due to physical health problems, functional disorders due to emotional health problems, energy and fatigue, emotional well-being, social functioning, pain, and general health. The items are scored from 0 to 100, with higher scores showing a better quality of life in that domain (Ware & Sherbourne, 1992). In a study, Motamed et al. in Iran (2001) tested the reliability of the scale, showing that Cronbach's alpha of the Persian version of the scale was estimated at 0.87 (Motamed et al., 2002).
Knee Injury and Osteoarthritis Outcome Score
Knee Injury and Osteoarthritis Outcome Score, which was developed by Roos and Lohmander (2003), is a 42-item patient-centered questionnaire. It assesses the outcomes of KOA. It contains five patient-related factors: pain (9 items), symptoms (7 items), activities of daily living (17 items), sports (5 items), and quality of life (4 items). The items are scored using a 5-point Likert scale, ranging from 0 to 4. For each subscale, the respondents’ total score is subtracted from 100 and then divided by 4 and multiplied by 100. The obtained percentage shows the respondents’ score for each section. The lower the scores, the more serious the issue (Roos & Lohmander, 2003). Salavati et al. in a study conducted in Iran verified the reliability of the scale using Cronbach's alpha (0.89) (Salavati et al., 2008).
Ethical Considerations
Written informed consent was obtained from the subjects before they participated in the study. The present study was conducted based on the principles of the revised version of the Declaration of Helsinki, which is a statement of ethical principles that directs physicians and other participants in medical research involving human subjects. The participants were assured about the anonymity and confidentiality of their information. Moreover, the study was approved by the Institutional Research Ethics Committee of Bushehr University of Medical Sciences, Bushehr, Iran (Ethical code: (IR.BPUMS.REC.1396.82), as well as a registration code (IRCT2017100218117N2) from the Iranian Registry of Clinical Trials (IRCT).
Statistical Analysis
SPSS version 22 was used to analyze the collected data. The results of the Shapiro–Wilk test indicated that the variables in both groups were normally distributed. A paired t-test was used to find out the difference in the means of the variables both before and after the intervention in the groups. An independent t-test was used to determine the difference in the mean of the variables both before and after the intervention between the groups. We also used analysis of covariance (ANCOVA) to determine whether there are any significant differences between the two groups. P < .05 were considered statistically significant for all tests.
Results
In this study, 57 out of 80 patients (71.25%) were women and 23(28.75%) were men. Their mean age was 39.41 ± 4.36 years, and the mean duration of their illness was 6.78 ± 4.13 years. No significant difference was found in demographic variables among the intervention and control groups (Table 2). Table 3 displays the comparison of the mean scores of VAS (pain intensity) in intervention and control group participants at the pre- and posttest stages within and between the groups. This shows the effect of intervention on the level of pain. Analysis of covariance was used after statistical control of the pretest effect and found that self-care education in patients with KOA had a significant effect on the dependent variable (pain) (P < .05). Table 4 compares the mean QOL scores of the intervention and control groups at pre- and posttest stages within and between groups, which shows the effect of intervention on QOL level. The ANCOVA test used after statistical control of the pretest effect showed that self-care education in patients with KOA had a significant effect on the dependent variable (QOL) (P < .05). Table 5 shows the comparison of the mean scores of disease consequences in patients with KOA between the intervention and control groups at pre- and posttest stages within and between groups, which shows the effect of intervention on consequences of disease. The ANCOVA test used after statistical control of the pretest effect showed that self-care education in patients with KOA had a significant effect on the dependent variable (consequences of disease) (P < .05).
Demographic Characteristics of the Studied Subjects.

*Independent sample t test.
**Chi square test.
Mean and Standard Deviation of Visual Analog Scale Score (Pain Intensity) of Intervention and Control Group in Pre- and Posttest Stages and Between the Two Groups.

*Paired sample t-test.
**Independent sample t-test.
***Analysis of covariance (ANCOVA).
Mean and Standard Deviation of Quality of Life Score of Intervention and Control Group in Pre- and Posttest Stages and Between the Two Groups.

*Paired sample t-test.
**Independent sample t-test.
***Analysis of Covariance (ANCOVA).
Mean and Standard Deviation of Consequences of Disease Score of Intervention and Control Group in Pre- and Posttest Stages and Between the Two Groups.
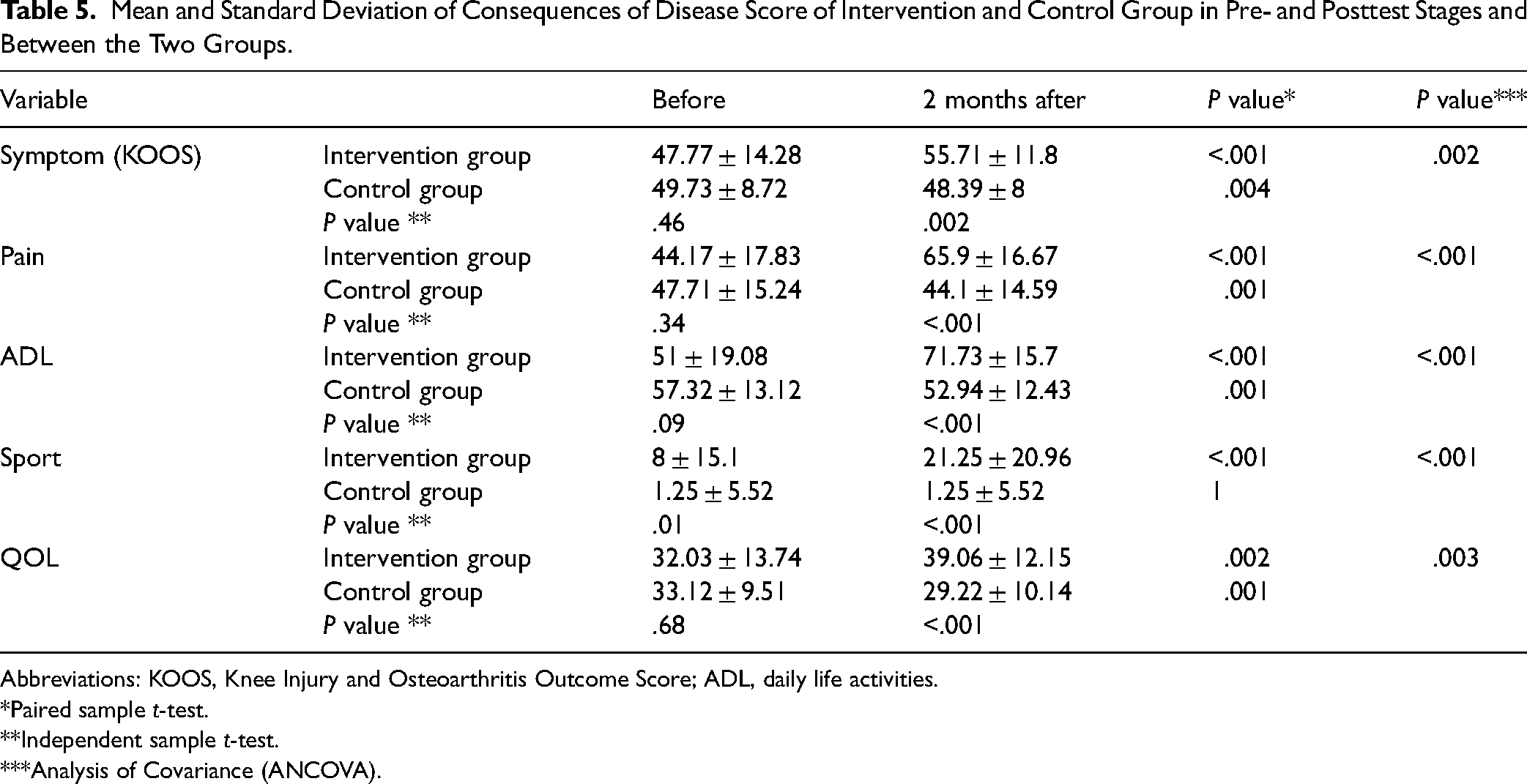
Abbreviations: KOOS, Knee Injury and Osteoarthritis Outcome Score; ADL, daily life activities.
*Paired sample t-test.
**Independent sample t-test.
***Analysis of Covariance (ANCOVA).
Discussion
The present study aimed to investigate the effects of self-care education on the pain, quality of life, and consequences of disease in patients with KOA in the south of Iran. A comparison between the patients’ mean scores of pain in the intervention and control groups as measured before and two months after the intervention revealed a significant decrease in the pain mean score in the intervention group as the secondary outcome after the intervention, whereas the change in the control group was not shown to be significant. This finding demonstrates that education in self-care can significantly reduce the patients’ pain mean score as the secondary outcome. In the same line with our results, the findings of a study carried out by Boonti et al. (2020) showed that the use of a self-care intervention resulted in a significant reduction in pain in patients with knee arthritis (Boonti et al., 2020). Moreover, in a study carried out by Ganji et al. (2018), the self-management plan implemented for patients with knee arthritis proved to be effective in alleviating the participants’ pain (Ganji et al., 2018), which is in the same line with the findings of the present study.
According to a study by Khachian et al. (2020), education in self-management can improve the health status of patients suffering from knee arthritis. Following a proper food regimen, using pain reduction techniques, and exercising can improve the adverse effects of knee arthritis (Khachian et al., 2020). These results are in the same line with those of the present study since both studies revealed the positive impact of self-care education on the health status and functioning of the patients. Thus, educational interventions that empower patients with knee arthritis in self-care are effective in their treatment and rehabilitation and should be employed as part of their treatment plans.
In the present study, a significant difference was revealed between the pre- and posttest scores of the intervention group as to improvement of the quality-of-life mean score as the main outcome of patients with KOA. In their study, Kaya and Bilik (2022) concluded that education and counseling contributed to the patients’ self-care and quality of life after knee replacement surgery (Kaya & Bilik, 2022), which is in the same line with the findings of the present study; the results of both studies highlight the role of patient education in improving the quality of life in KOA patients. Likewise, a study by Holm et al. (2020) reported that the performance of daily activities and physiotherapy in the form of a self-care plan enhanced the quality of life of patients with knee arthritis (Holm et al., 2020).
Many studies have reported that self-care models and plans are effective in increasing the quality of life of patients with knee arthritis; however, a study by Gurt et al. (2018) found the impact of a self-care plan on the patients’ quality of life was insignificant; this is not consistent with the findings of the present study. The discrepancy can be attributed to the fact that Gurt's intervention focused on physical activities, while the present educational program addressed other aspects of the patients’ lives including their nutrition and medication as well. Inasmuch as quality of life is a multidimensional concept, a one-dimensional intervention is not likely to affect it in a significant way (Gurt et al., 2018).
One of the reasons for the effectiveness of the training program in the current study is face-to-face training and patient-centered training (The Andragogy Approach). Employing andragogy in patient education enables healthcare providers to gain a better understanding of their clients’ educational needs and develop individualized patient-centered education.
Limitations: The current study was carried out in the south of Iran, and the findings may not be generalizable to other countries. The study was conducted on a small sample and in several centers in southern Iran with a different culture than in other parts of Iran and the world, so the results cannot be conclusive. However, similar healthcare facilities will benefit from our findings. It is suggested that similar studies should be conducted in other countries. The severity of the OA of those in the study in relation to the general population with OA, it was not investigated and was not part of the objectives of the study. It is suggested to be investigated in future studies.
Strengths: The strengths of the current study include conducting the study as a randomized clinical trial, using clinical guidelines (osteoarthritis-care-and-management-in-adults-cg177.pdf), and using an occupational therapist, physiotherapy specialist, nursing professor, and orthopedic specialist (Education Using Team-based Learning Method) in the training program.
Implication in Clinical Education
The findings of this study confirmed the existing evidence claiming the effectiveness of educational interventions based on self-care in the improvement, quality of life, and consequences of KOA in patients. Given the educational role of nurses and their significant impact on self-care behaviors of patients with chronic diseases, including OA, and the improvement observed in the self-care scores of the intervention group in this study, this educational approach can serve as an accessible and effective intervention in health centers and medical facilities. It is also recommended that further research should be conducted on the long-term effects of education based on this self-care model on OA patients. As well as self-care education implemented as a community-based program enhances accessibility for individuals in need, reducing logistical and financial strains on healthcare systems, while empowering individuals to lead better lives. This approach would be highly valued by millions of people grappling with joint pain.
Conclusion
This study also confirmed the active role of nurses as members of community-based care service teams, not only in the hospital but also in the community and even in the home environment, in reducing pain and improving the quality of life in KOA patients. Furthermore, the results highlight the need for attention to the role and special position of nurses in the presentation community-based services, especially in existing health network in the south of Iran, which emphasizes the need for equality and justice in health. The findings of the present study revealed that educating patients with OA of the knee to practice self-care was effective in reducing the intensity of their pain, improving the quality of their lives, and alleviating the consequences of their disease. Since self-care interventions are designed to promote the patients’ capabilities and independence by involving them in their caring process, the application of self-care models is a practical approach to providing holistic care based on scientific evidence to patients with knee arthritis.
Supplemental Material
sj-doc-1-son-10.1177_23779608241260822 - Supplemental material for Self-Care Education on the Pain, Quality of Life, and Consequences of Disease in Patients with Knee Osteoarthritis
Supplemental material, sj-doc-1-son-10.1177_23779608241260822 for Self-Care Education on the Pain, Quality of Life, and Consequences of Disease in Patients with Knee Osteoarthritis by Zeinab Jokar, PhD, Zahra Hosseinabadi, MS, Sanaz Rustaee, MS, and Mostafa Bijani, PhD in SAGE Open Nursing
Footnotes
Acknowledgments
The authors thank the patients participating in the study.
Author Contribution
MB and ZJ was involved in the conception and organization of the study. SR, ZH, and ZJ were involved in the execution and data collection of the study; MB and ZJ participated in statistical analysis design and/or execution. All authors contributed to the preparation, critical review, and all of them approved the final manuscript.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Written informed consent was obtained from the subjects before they participated in the study. The present study was conducted based on the principles of the revised version of the Declaration of Helsinki, which is a statement of ethical principles that directs physicians and other participants in medical research involving human subjects. The participants were assured about the anonymity and confidentiality of their information. Moreover, the study was approved by the Institutional Research Ethics Committee of Bushehr University of Medical Sciences, Bushehr, Iran (Ethical code: (IR.BPUMS.REC.1396.82), as well as a registration code (IRCT2017100218117N2) from the Iranian Registry of Clinical Trials (IRCT).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.