
Abstract
Introduction
Family members caring for a person living with dementia (PWD) can experience caregiver burden, leading to psychological distress if unmanaged. It's essential for healthcare professionals, especially nurses to identify caregivers at risk of stress and depression, triggering prompt management during their contact with caregivers of PWD. The study team developed an evidence-based caregiver burden-mastery hybrid assessment and intervention decision matrix (CHAT-MI) for caregivers of PWD and examined its feasibility of use.
Objective
To determine the feasibility and usability of implementing the CHAT-MI assessment-decision matrix tool in an outpatient setting in Singapore.
Methods
CHAT-MI was developed through earlier research, research evidence, clinical guidelines, and expert opinion. A multimethod study was conducted in a Singapore outpatient memory clinic from November 2020 to January 2021. Caregivers of PWD who attended the clinic self-administered the assessment tool to determine their burden and personal mastery levels. Clinicians used a decision matrix to guide interventions based on the assessments. Feedback was gathered from both caregivers and clinicians through surveys and semistructured interviews.
Results
Thirty-four caregivers and six clinicians participated in the study. Caregivers found the burden-mastery assessment tool relatively easy to use and understand and helpful. Clinicians found the assessment-decision matrix tool acceptable, feasible, and useful, enhancing standard care by providing insights into caregivers’ current coping capabilities. Clinicians shared that junior clinicians could benefit from CHAT-MI to better detect caregiving stress and deliver interventions. Nevertheless, more can be done to train clinicians in the understanding of the concept of mastery (i.e., perceived control over life events) to help clinicians better engage and support caregivers.
Conclusion
CHAT-MI was found to be relatively brief and can aid the outpatient clinic setting. This suggests that such an evidence-based assessment cum intervention can be considered for use in a real-world clinical setting to aid both caregivers and clinicians.
Introduction
Dementia exerts a disproportionate impact on family members, who often play an integral role in caregiving, while simultaneously juggling multiple commitments in their personal lives. In Singapore, over 95% of older adults live together with with their family caregivers and depend on them for aspects of their care (Mehta, 2005). This places an increasing burden on family caregivers to care for their aged parents, often taking on the challenging caregiving role with little or no preparation, knowledge, skills, and resources (Blum & Sherman, 2010). Caregiving for a person living with dementia (PWD) is an especially stressful experience, as the demands of care often surpass the financial, emotional, social, and personal resources of caregivers. Caregiver burden places them at greater risk of burnout, social isolation, and poor physical and mental health (Chan et al., 2018, 2019b; Lim et al., 2023; Richardson et al., 2013; Sallim et al., 2015). When one's capacity to care is depleted, this inevitably impacts the quality of care for the PWD, and in some extreme cases, it can lead to maltreatment and poor healthcare outcomes in the PWD, such as increased risk of hospitalization, institutionalization, and mortality (Lau et al., 2021; Tew et al., 2010; Yan & Kwok, 2011). The early identification of caregivers at risk of distress and depression to enable prompt intervention thus warrants immediate and urgent attention.
The Zarit Burden Interview (ZBI) is a widely used instrument to measure caregiver stress, which has been validated for use in caregivers of PWD in Singapore (Seng et al., 2010; Tu et al., 2022; Whalen & Buchholz, 2009). Beyond role strain and personal strain, the ZBI also captures a unique dimension of burden—worry about performance—salient in Asian societies with a strong obligation to “care for elders” as an expression of filial piety. This pertains to a caregiver's self-appraisal of caregiving performance and personal belief that one could be doing more and doing a better job in the caregiving role (Cheah et al., 2012; Lim et al., 2014).
In addition, it is important to assess protective factors and available resources, given their buffering effects against stress and negative outcomes (Adams et al., 2005; Chan et al., 2018; Roepke & Grant, 2011; Roepke et al., 2008). One important protective factor to consider would be the personal mastery of a caregiver—the sense of control one has over the life circumstances (Pearlin et al., 1990; Pearlin & Schooler, 1978; Skaff & Pearlin, 1992). Earlier research confirmed this, with personal mastery associated with better coping, optimism, and positive physical and mental health (Chan et al., 2018). A better understanding of caregivers’ personal mastery could hence guide clinicians on how caregivers are coping with their stressors and care demands.
Nurses play a critical part in identifying and providing education and emotional support to distressed caregivers, as they are the advocate and main point of contact between the hospital and caregivers, often engaging caregivers in dementia-related education (Chan & Glass, 2022; Chan et al., 2022). Nurses would benefit from a concise, user-friendly assessment tool to examine caregivers’ burden and capacity to cope (Alves et al., 2022; Bédard et al., 2001).
The study team sought to develop a toolkit to support nurses and frontline clinicians in the identification of caregivers of PWD who would be at risk of caregiver stress and a suite of potential interventions, the Caregiver burden-mastery Hybrid Assessment Tool (CHAT)—Matrix of Interventions (MI) (CHAT-MI). The first component, CHAT, aimed to assess the burden experienced by caregivers and their capacity to cope. This would be bundled with a Matrix of Interventions (MI) to guide clinicians on the appropriate steps they could take to support the caregiver appropriately.
Once developed, it was important to assess if CHAT-MI would be feasible and usable in caregiver engagement and consultations, in a busy outpatient clinic setting.
Review of the Literature
Few hospitals have standardized protocols for the pre-emptive identification of caregiver stress and the delivery of appropriate support (Chan et al., 2019a; Glajchen et al., 2005; Lim et al., 2023). This points toward the need for a brief screening tool that could combine the assessment of caregivers’ burden with their mastery level, to provide a consistent evaluation of caregivers’ stress and their ability to cope, prioritizing help for caregivers at higher risk of distress.
In addition, there is a need for a consistent recommendation of treatment and support for caregivers, independent of individual clinicians’ experience and awareness of resources available. Greater consistency in assessment and interventions could be achieved through the availability of a clinically useful tool that combines the assessment of the caregivers’ burden and mastery, with a corresponding decision matrix for intervention recommendation (Tan et al., 2020).
However, the development of such a decision matrix remains a nascent field, with most research focused on rapid caregiver stress screening alone without the combination of a mapped “menu” of interventions to guide practice (Glajchen et al., 2005; Guthrie et al., 2021; Tan et al., 2020). There is a need for a brief assessment tool that assesses caregiving burden and personal mastery, together with a matrix of interventions to guide clinicians in the identification and management of caregiver stress.
Hence, the study team sought to evaluate the feasibility and usability of the caregiver hybrid assessment tool and intervention decision matrix, CHAT-MI, within a real-world outpatient memory clinic.
Methods
Development of CHAT-MI
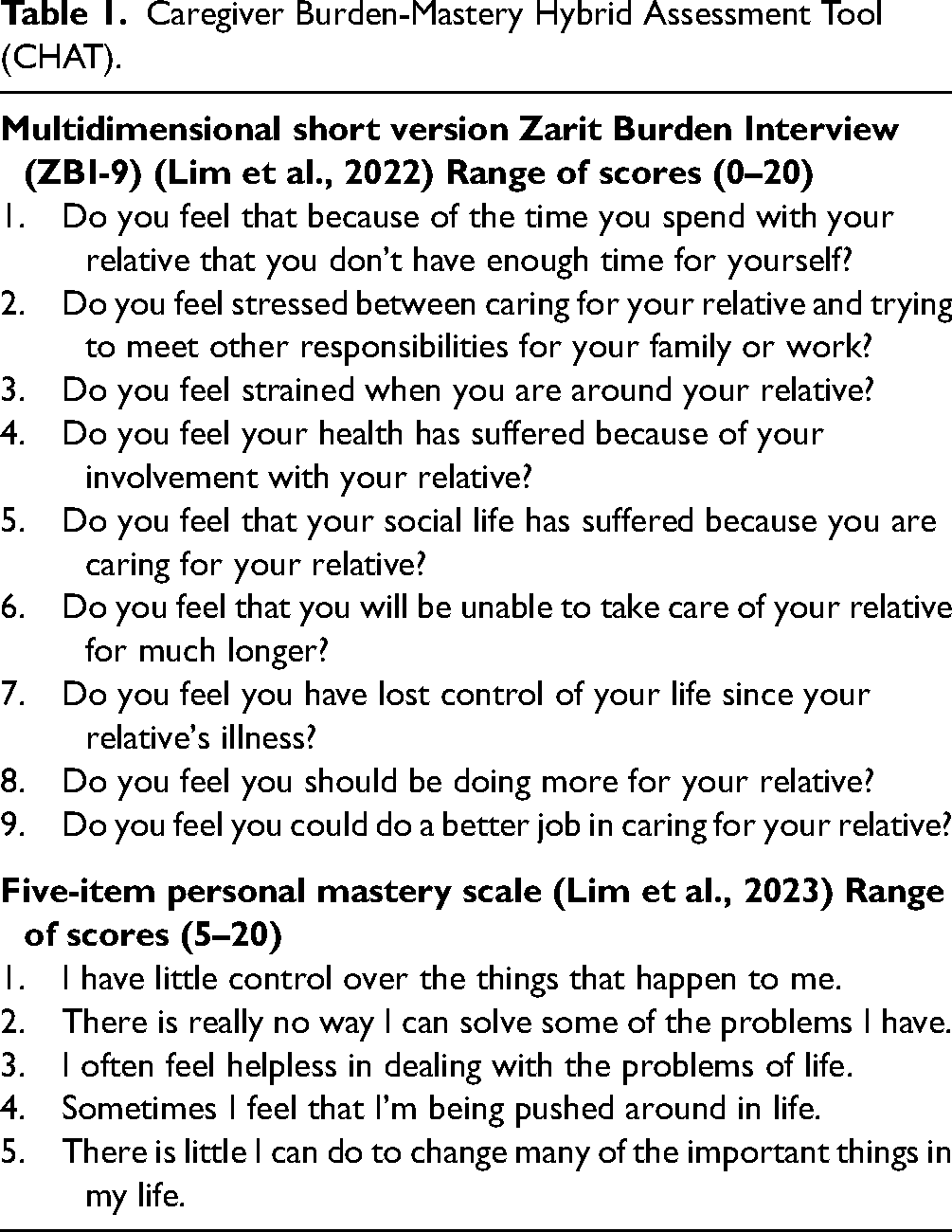
CHAT aimed to assess the burden experienced by caregivers and their capacity to cope. It was built using a combination of a short-form version of the Zarit Burden Interview (ZBI) and a short-form version of the personal mastery scale (Pearlin & Schooler, 1978; Zarit et al., 1980). The nine-item Zarit Burden Interview scale (ZBI-9) was combined with a five-item personal mastery scale. Both of these were developed and validated in caregivers of PWD in Singapore, demonstrating acceptable psychometric properties (Lim et al., 2022, 2023). Importantly, while shorter than the 22-item version of the Zarit Burden Interview scale (ZBI-22), the ZBI-9 retained the comprehensive four-factor structure dimensionality of the burden construct including that of “worry about performance” (Lim et al., 2023). The five-item mastery scale also maintains the reliability and validity of the original seven-item version (Lim et al., 2022).
To use CHAT, the scores of the ZBI-9 and personal mastery five-item scale were summed up separately, to better understand the caregiver's level of burden and their capacity to cope respectively. Items on the ZBI are rated on a five-point scale, ranging from 0 (never) to 4 (nearly always). The total score ranges from 0 to 36 with a higher score representing higher caregiving burden. Items on the mastery scale are rated on a four-point scale, ranging from 1 (strongly disagree) to 4 (strongly agree). The total score ranges from 5 to 20, with a higher score representing lower levels of mastery. CHAT is shown in Table 1.
Caregiver Burden-Mastery Hybrid Assessment Tool (CHAT).
MI's development was grounded in theoretical evidence, expert opinions, and current clinical practice guidelines in the hospital. The tool was designed and developed based on the following steps: (1) a review of the current evidence-based guidelines to address the caregiving burden and personal mastery and (2) the formation of a multidisciplinary team of experts to identify appropriate local resources and referral services for at-risk caregivers and to create a clinical workflow for the implementation of the tool.
From the literature review and clinicians’ experience, six domains of caregiving stressors were identified, which included the patients’ declining cognitive function, behavioral problems, poor physical functioning, financial and social stressors, caregivers’ mastery, and worry about performance. These six domains were subsequently classified into either patient-related or caregiver-related stressors for the decision matrix. Through this, six domains of caregiving stressors were identified, and appropriate interventions were mapped such as the hospital's Coaching, Advocacy, Respite, Education, Relationship, Simulation (CARERS) Program for caregivers with low mastery, designed to help improve their sense of control over their caregiving situation through problem-solving exercises (Sadavoy et al., 2021, 2022). The original matrix is shown in Figure 1.

Prototype CHAT-MI decision matrix.
With the original prototype of CHAT-MI established and deemed acceptable for testing by an expert group of clinicians, the study team sought to begin feasibility testing of CHAT-MI in the outpatient setting. The following sections detail how CHAT-MI's feasibility and usability testing was conducted.
Design
A multimethod feasibility and usability testing of the combined caregiver assessment-decision matrix tool was performed on both groups of end-users—caregivers of PWD and clinicians. The evaluation was performed through surveys and interviews.
Research Aim
The aim of the study was to gather caregivers’ and clinicians’ feedback regarding the feasibility and usefulness of the tool in providing recommendations to the caregivers according to the burden and mastery levels.
Setting
This study was conducted in the Memory Clinic, Department of Geriatric Medicine, Tan Tock Seng Hospital, Singapore, between November 2020 and January 2021. The Memory Clinic is a specialist center for the evaluation of cognitive decline, diagnosis of dementia, and management of PWD and their caregivers.
Sample
As this was a feasibility study, the study team anticipated recruiting a minimum of 20 participants. This is an acceptable sample size in pilot studies (NCSS Statistical Software, 2021; Thabane et al., 2010).
Family Caregivers
Between November 2020 and January 2021, family caregivers of PWD visiting the Memory Clinic were recruited to use the assessment tool and receive the matrix of interventions. The inclusion criteria were caregivers who were family members of the PWD, were literate in English or Mandarin, and were able to independently complete the questionnaires in the assessment. Caregivers were excluded if their care recipients were not diagnosed with dementia or if they were not a family member of the patient.
Dementia Care Clinicians
In addition, dementia nurse clinicians and doctors who used CHAT-MI to guide their consultations were interviewed between January and February 2021. The inclusion criteria for clinicians were that they had to have administered both the assessment tool and decision matrix at least once and were permanent staff at the Memory Clinic.
Study Procedure
During a routine visit to the Memory Clinic, a dementia care nurse clinician typically interviews both the patient and caregiver to assess cognitive abilities, discuss psychosocial concerns, and administer cognitive tests for the patient. The clinician would assess the caregiver's specific stressors before providing dementia counseling for the identified areas of concern. First-time visitors are usually screened for caregiver burden using the ZBI-22, with score interpretation and subsequent actions determined based on individual clinician judgment. Given the existing workflows in place for caregiver stress screening and counseling, the integration of the CHAT-MI tool into the clinic setting was deemed to be appropriate.
For this study, the dementia care nurse clinicians assisted in the identification of eligible caregivers for participation in the study by confirming their care recipients’ diagnosis of dementia from the electronic medical records. The caregivers were then approached by a study team member to affirm their eligibility and recruited for the feasibility study after providing verbal consent.
While waiting for their consultation with the nurse clinicians, caregivers completed both the ZBI-9 and five-item personal mastery scale for their risks/needs. Items on the ZBI-9 are rated on a five-point scale, ranging from 0 (never) to 4 (nearly always). The total score ranges from 0 to 36 with a higher score representing higher caregiving burden. Items on the mastery scale are rated on a four-point scale, ranging from 1 (strongly disagree) to 4 (strongly agree). The total score ranges from 5 to 20, with a higher score representing lower levels of mastery. The tool is shown in Table 1.
During the consultation, the nurse clinicians tabulated the caregivers’ CHAT tool scores. The scores of the ZBI-9 and five-item personal mastery scale were summed up separately to better understand their level of burden and capacity to cope, respectively. Based on these scores, the nurses provided interventions using the decision matrix. A list of the interventions is described in Table 2.
Interventions Provided to Caregivers Based on the Causes.

Data Collection
After consultation, caregivers completed a feasibility questionnaire and participated in a short interview with a study team member. Caregivers were asked to rate (1) whether they understood the items on the form and (2) whether the time it took to complete the assessment was acceptable. Furthermore, if caregivers had received interventions following their assessment, four additional questions were administered: (1) if the recommendations provided would reduce their stress, (2) if the recommendations given would help in their caregiving role, (3) if the recommendations met their needs, and (4) their satisfaction with the recommendations. Responses were rated on a five-point Likert scale, from 1 (strongly disagree) to 5 (strongly agree). Using an interview guide (Table 3), the study team also interviewed the caregivers to better understand their experience and thoughts on the assessment and matrix. The interview guide asked questions on whether the patients found the questions easy to understand, and met their needs, and to clinicians, whether it had helped them in their consultations and if it could be adopted across their clinic (Table 3).
Interview Guide for Caregivers and Clinicians.

To assess the feasibility of the CHAT-MI from the point of view of clinician users and improve its incorporation into the clinic's workflow, doctors and dementia care nurse clinicians who used the tool were also engaged in a semistructured interview using an interview guide (Table 3). These clinicians provided feedback on the tool, relative to the current care they typically deliver, and suggested improvements to further refine the tool. They also completed a seven-item questionnaire (Table 4) to assess the acceptability and utility of the tool, appropriateness of the interventions, and likelihood of future adoption after the pilot study has concluded.
Questionnaire for Caregivers and Clinicians.

Note: Items 3 to 6 were calculated based on a total sample size of n = 22 indicating those with difficulties coping (mastery score ≥10).
Interviews conducted with both caregivers and clinicians were recorded manually through detailed field notes. Member checking was conducted at the end of the interview to ascertain the accuracy of the notes.
Data Analysis
Quantitative Data
A descriptive analysis was conducted on caregivers’ burden and mastery scores and their feedback forms. The study team examined the proportion of respondents’ level of agreement with the questions to better evaluate how the assessment and recommendations benefitted them.
Qualitative Data
Thematic analysis was conducted based on the following steps: data familiarization, generating codes, grouping of codes into themes, and revising and defining themes (Braun & Clarke, 2006). Two study team members independently familiarized themselves with the data gathered and used it to generate codes, coming together to propose themes. These were then reviewed by the overall study team to revise and define the themes accordingly.
Results
Thirty-five caregivers were recruited for the feasibility study of CHAT-MI, but one caregiver was unable to complete the feasibility study as she declined to receive intervention through the matrix and was excluded from the analysis. Six clinicians (three geriatricians and three dementia care nurse clinicians) were recruited to give feedback on CHAT-MI.
Assessment Component of CHAT-MI
Thirty (88.2%) caregivers found it easy to understand the items on the screening component of CHAT-MI, while four caregivers (11.8%) found some items difficult to comprehend. This includes ZBI items assessing caregivers’ worry about performance, such as “Do you feel you should be doing more for your relative?” and “Do you feel you could do a better job in caring for your relative?”. A summary of the responses to each item in the questionnaire is shown in Table 4.
The CHAT-MI's assessment component provided caregivers an opportunity to check in on their personal well-being and reflect on their unmet caregiving needs and stressors, providing them the opportunity to raise these issues with their clinician during consultation: (The) questionnaires helped me to reflect and introspect on areas where I need more support, and (think about) whether I’ve overlooked my own wellbeing. (CG5) It's useful to give a quick snapshot of how the caregiver is doing, which is easier for doctors, especially when we have a busy clinic. The checklist is more practical and easier for doctors to see what intervention was administered, rather than checking C-doc [electronic medical records]. (HCP4)
Furthermore, CHAT-MI's assessment component provided ancillary information on caregivers which might not have been picked up in the busy clinical setting. This was useful in detecting high burden among caregivers to whom clinicians had initially thought were coping adequately: It would be good because you are able to identify high burden scores in a case [caregiver] that you don’t expect. (HCP6) The tool is able to pick up that she [caregiver] is stressed, and the nurse gave suggestions for (referrals to) [caregiver-centric programs] or [mindfulness programs]. (HCP5)
While most clinicians expressed positive attitudes toward the importance of evaluating caregiving burden and mastery, one clinician expressed hesitation in using CHAT-MI to achieve this purpose. Given that mastery was a relatively new construct that was recently introduced to clinicians, they were not fully confident in using the scale and interpreting the scores, highlighting the necessity for more in-depth training: I’m unsure about how to use the mastery tool because it's my first time. I’m not very confident in using the scale as a healthcare professional. I need someone to teach me how to use it, especially with the interpretation of scores and suggesting interventions based on the scale. (I’m) scared that I will apply and interpret it wrongly, and (worry about) whether I gave the right intervention. (HCP3)
Decision Matrix Component of CHAT-MI
Based on their CHAT-MI assessment scores, 22 of the 34 caregivers (65%) were assessed to have difficulty coping. This was defined by a mastery score of ≥10. The caregivers were subsequently provided interventions according to the decision matrix. Most caregivers felt that the recommendations provided would help to reduce caregiving stress (86.3%), assist them in fulfilling their caregiving roles (95.5%), and meet their needs (81.8%). In addition, caregivers were generally satisfied with their recommendations (95.5%).
Caregivers valued the approach of clinicians applying the decision matrix to guide their interactions and consultation. One caregiver (CG31) shared that the “question-and-answer” discussion on the interventions following the assessment sessions helped. This was echoed by another caregiver (CG4), who commented that “The (combined experience of) assessment and counseling should be provided” for all caregivers.
Clinician feedback on the decision matrix of CHAT-MI was positive, with all except one of the clinicians (83.3%) agreeing on the feasibility of the recommendations, that they would help reduce stress and can be administered within an acceptable amount of time. Disagreement between the clinicians was present in only two statements—whether CHAT-MI added value to their approach in recommending care (16.7% disagreement) and whether the time taken to complete CHAT-MI was acceptable (16.7% disagreement). A summary of the responses to each questionnaire item is shown in Table 4.
During the interview, clinicians shared how they combined the results from the screening component with the matrix of interventions to better individualize their engagement with the caregiver. Through this, they were able to better address caregivers’ needs and concerns, highlighting a greater shift toward the provision of caregiver-centric care: I will probe deeper when their burden scores (reported in the screening component) are high. (HCP3) (CHAT-MI) guides clinician to dig more [probe] when they score high on mastery and burden… Having (CHAT-MI) will guide the consultation process, and nurses will know how to intervene [provide recommendations for caregivers]. The consultation is more structured and systematic compared to before. (HCP1) When scores (on the screening component of CHAT-MI) show that the caregiver is experiencing stress, the doctors will know that they must portion time and check in with the caregiver on how the caregivers are doing. (HCP5) I’ve not gone through the CARERS program, I’m unsure what it consists of. I will need to be sure that this program will be suitable for this category of NOK [next-of-kin]. For instance, CARERS’ problem-solving techniques program can be very different from what the nurses and caregivers have in mind—they can refer to different problems. (HCP3)
Another challenge to the effective implementation of CHAT-MI was competing issues within a time-limited consultation. Without a firm understanding of the value behind assessing mastery and its recommended interventions, some clinicians may wish to spend more clinical time addressing PWD-related stressors (e.g., behavioral and psychological symptoms of dementia), leading to a low adoption rate of the tool: I didn’t really use the tool. I don’t have time to talk about mastery, especially for reassessment cases, because there are other problems, such as (the patient's) behavioural issues to talk about. (HCP2)
The CHAT-MI tool was found to be valuable in complementing and enhancing standard care consultations by providing additional information regarding caregivers’ current coping capabilities. The assessment tool provided a platform for caregivers to reflect on their caregiving concerns which can be highlighted during the clinical consultation; similarly, the snapshot of identified issues and interventions alerted clinicians to caregiver issues that may otherwise be missed and facilitated appropriate individualized interventions.
Using these findings, the study team continued making refinements to the decision matrix. The team recognized the importance of immediate engagement with caregivers who were found to have low mastery, reinforcing counseling. This led to the introduction of nurse-led interventions, to “reinforce counseling” and “encourage the caregiver to seek family/social/spiritual support.” The finalized framework is shown in Figure 2. A table summarizing the changes done is shown in Table 5.
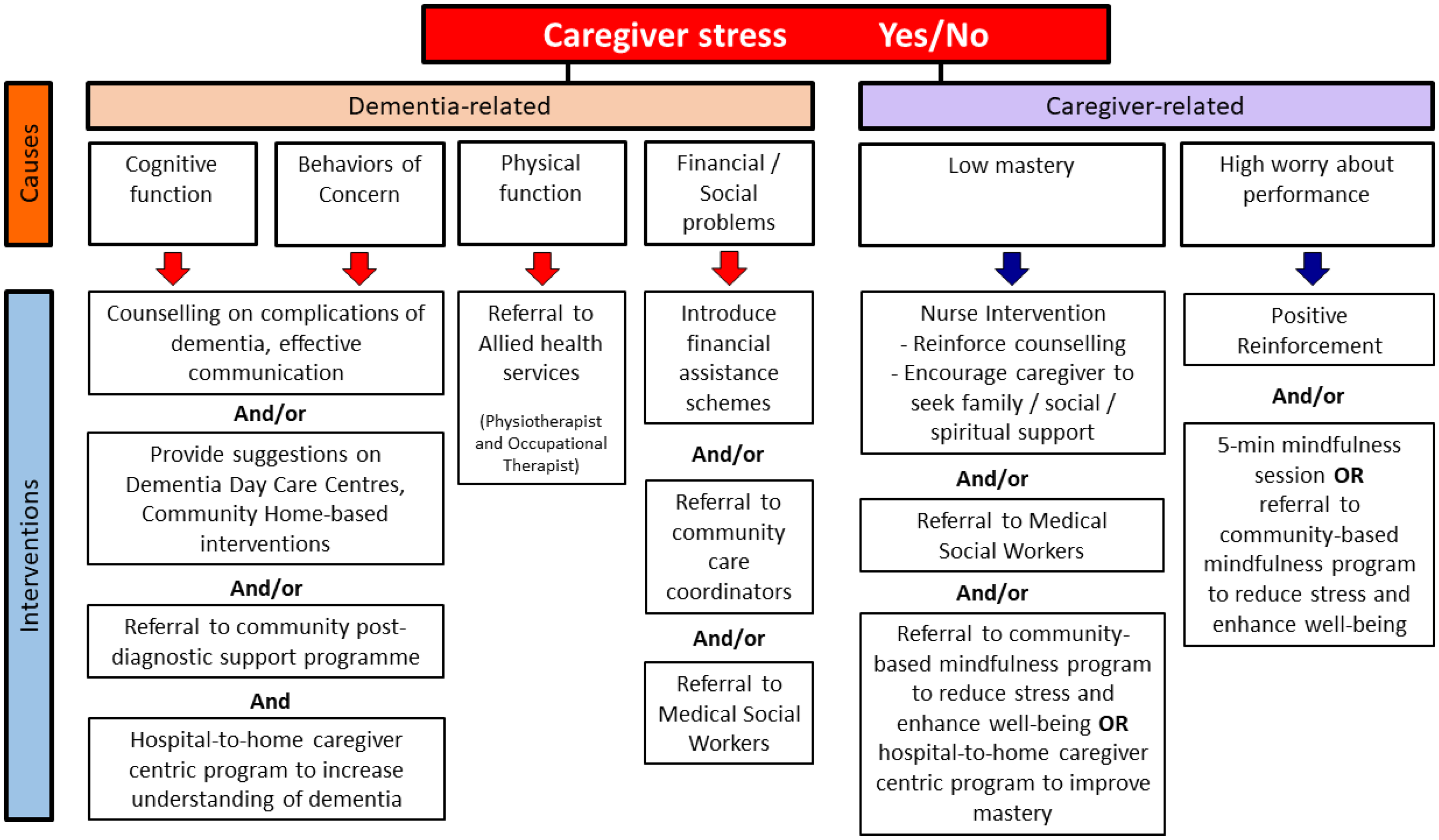
Finalized CHAT-MI decision matrix.
Summary of Changes Made to the Interventions in Figure 1.

Discussion
This article describes the feasibility and usability testing of the combined burden-mastery hybrid assessment tool with a decision matrix to support caregivers of PWD, incorporating it into the clinical workflow of an outpatient setting.
Clinicians generally displayed positive attitudes toward the assessment tool and decision matrix, perceiving them to be practical, acceptable, and feasible to implement. The assessment-decision matrix tool was also valuable in complementing and enhancing the standard care consultations by providing additional information regarding caregivers’ current coping capabilities. This provided greater ease for clinicians in detecting caregiving stress and delivering appropriate individualized interventions.
The CHAT assessment tool was valued by caregivers as it “opened the door” for caregivers to self-check on how they were coping and provided an opportunity for engagement and dialogue with clinicians to discuss the stress they faced. This was a similar benefit shared by cancer caregivers on the usage of CancerSupportSource-Caregiver, a distress screening for cancer caregivers designed in a similar vein (Shaffer et al., 2019) to the CHAT assessment tool. This reflects the value of a short-form self-administered caregiver stress assessment tool in the clinical setting, allowing the detection of caregiver distress to segue into much-valued interaction and intervention with clinicians.
While short-form caregiver burden assessment tools are currently available, they often are not integrated or interfaced with an intervention matrix, to guide clinicians on possible courses of action when they detect a stressed caregiver (Alves et al., 2022; Bédard et al., 2001). In addition, the assessment tools available require validation for local contexts (Chan et al., 2019a; Lim et al., 2023). The combined short-form assessment tool and intervention matrix offers a validated easy-to-administer caregiver assessment tool and a suite of potential interventions to guide clinicians on the subsequent best course of action.
This study also highlighted potential barriers to the use of such tools amongst clinicians, in a time-limited consultation. For instance, clinicians raised concern about assessing caregivers’ mastery level and recommending interventions, citing their lack of understanding of the construct. This might be attributed to the lack of familiarity and comfort level with the global nature of the mastery construct, which pertains to the sense of control one has over the life circumstances (Pearlin et al., 1990; Pearlin & Schooler, 1978; Skaff & Pearlin, 1992). Such a global concept is less familiar to clinicians as compared to more specific stressors and solutions typically addressed in consultations, such as behavioral regulation and managing sleep disturbance (Bryden 2002; Griffiths et al., 2021).
However, improving caregivers’ behavioral management skills and other practical skills contributes toward helping caregivers feel they are better “in control” and hence raise their mastery levels. This was a trait expressed by many thriving caregivers of PWD interviewed in the team's earlier research (Chan et al., 2019b). The protective effect of such mastery was demonstrated in the team's earlier research as well, protecting against depressive symptoms in caregivers. (Chan et al., 2018). Hence, while more can be done to train clinicians in the concept of mastery to help in their engagement and support of caregivers, the body of evidence supports providing caregivers with practical knowledge and skills to care for the PWD to enhance their sense of control and hence mastery as a protective mechanism against caregiver burden and depressive symptoms. In this regard, the construct of mastery aligns well with the assessment and decision matrix components of CHAT-MI.
Many caregivers seek help and utilize support services only when they are experiencing significant distress, which usually occurs much later in the disease trajectory when their care recipients have greater care needs (Lim et al., 2012). Unfortunately, the delay in seeking and receiving help may render interventions less effective in alleviating the caregiving burden, as the intensity of their caregiving needs may have far exceeded the potential of the intervention to help (Markle-Reid & Browne, 2001), resulting in the placement of older adults in long-term care facilities due to caregiver distress. Thus, it is paramount to address caregiving stress through systematic assessment for early risk detection, allowing the prompt identification of at-risk caregivers. Guided by the intervention matrix, caregivers can subsequently be recommended early intervention and resources promptly. By adopting a preventive approach, caregivers can receive appropriate services earlier, enabling them to provide sustainable caregiving without placing their physical and mental well-being at stake.
Strengths and Limitations
One of the strengths is the use of a multimethod strategy of evaluation, using both quantitative surveys and semistructured interviews to elicit feedback from the caregivers and the clinicians. Another strength is that this study provides an important lens for practice-based development and field-testing of a new clinical assessment tool and appropriate interventions. The systematic approach to the development of both the assessment tool and intervention matrix, followed by the implementation and its evaluation of feasibility, demonstrates how an evidence-based intervention can be fielded and evaluated in real-world clinical settings.
Despite its merits, several limitations ought to be considered. For instance, the decision matrix was not adopted across all clinicians during their consultations. While the decision matrix adopted a holistic approach and included new caregiver support services from the hospital, unfamiliarity with these new interventions in the matrix would require a more detailed sharing of these interventions and their benefits, for greater buy-in from the clinicians. These limitations may have affected the study findings. Additionally, the decision matrix appears to be more useful for junior clinicians compared to the expert clinicians.
Future Studies
While the sample size of 30 might be adequate for a feasibility study, a larger sample size would be required to evaluate the potential effectiveness of CHAT-MI in a wider setting. Future studies could focus greater attention on removing these barriers to adoption and a wide-scale rollout of CHAT-MI to enable the successful implementation of the tool in other settings. Future studies may also wish to gather more insights on which group of clinicians and the settings, that will benefit most from the use of a tool such as CHAT-MI.
Implications for Practice
Insights drawn from this study can be useful for policymakers, hospital leaders, and social service agencies which serve as frequent touchpoints for caregivers of PWDs. The early identification of at-risk caregivers and matching of interventions will ensure the proper allocation of assistance to the caregivers promptly, leading to better outcomes for caregivers and PWDs. Given that the tool can be self-administered, can be incorporated into existing care, and requires relatively acceptable time to complete, CHAT-MI can be scaled to other specialist clinics and care settings in the community. In particular, the assessment tool and decision matrix may be useful in primary care settings, where general practitioners often report poor knowledge of the resources available for PWDs and their caregivers and exhibit low confidence in the optimal management of their needs (Devi et al., 2018). This assessment tool and decision matrix may serve as the critical first step toward enhancing the knowledge and confidence of general practitioners, potentially boosting the presently low referral rates to social services and underutilization of community resources (Aminzadeh et al., 2012; Fortinsky et al., 2009; Hinton et al., 2007).
While this was tested in the outpatient settings with clinicians including nurse specialists in caring for PWD, the user-friendliness of the matrix shows its potential to be applied in other settings where nurses have frequent contact with caregivers, such as in the inpatient or teleconsultation setting. This was reflected when a further shortened version of the assessment tool and decision matrix was found to be useful in the telephonic consultation of caregivers, allowing the telephonic team to quickly identify caregivers at risk of stress and offer customized support as required (Chan & Glass, 2022; Chan et al., 2022).
Conclusion
Caregiving can be a long and arduous journey, placing caregivers at heightened risk of stress and caregiving burden. This can be addressed through the early detection of caregiver burden, assessment of their coping capabilities through assessing their mastery level, and subsequent providing them with appropriate interventions through an intervention matrix. CHAT-MI, a combined assessment and decision matrix tool that we developed, was found to be relatively brief and easy to administer, demonstrating its practicality and usability in an outpatient memory clinic.
Footnotes
Acknowledgments
The authors would like to thank the staff of the Memory Clinic for supporting the identification of eligible caregivers, dementia care nurse clinicians Ms. Philomena Anthony and Ms. Ong Poh Ling for their expert insights and suggestions for the improvement of CHAT-MI, and our caregiver participants who volunteered to pilot CHAT-MI during their clinic consultation. We would like to thank Mr. Melvin Lim Zhi-XIang for his help in designing the original iteration of CHAT-MI.
Author Contributions
All authors meet authorship criteria and are in agreement with the content of the manuscript.
EYC, WSL, NA, ZO, JPL, and SLA conceptualized CHAT-MI and its delivery in the outpatient clinic setting. EYC supervised the overall study. EYC and ZO designed the study questionnaire and interview questions. ZO was responsible for data collection. EYC, ZO, and GFGJ analyzed the data and interpreted its findings. ZO, GFGJ, and EYC drafted the final manuscript. All authors gave critical inputs to the manuscript and all authors gave the approval of the manuscript version for publication.
Ethical Considerations
The study was approved by the Institutional Review Board at the National Healthcare Group (Ref No: 2018/00804). Verbal consent was sought from caregivers to participate in the testing of the CHAT-MI tool. Verbal consent was sought from eligible clinicians to interview them and seek their thoughts and perceptions on CHAT-MI.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the Ng Teng Fong Healthcare Innovation Program (NTF_JUN2018_I_C1_C_02): Care Redesign for Caregivers—Patients with Dementia: Project CHAT-MI: Caregiver mastery-burden Hybrid Assessment Tool—Matrix of Interventions.