
Abstract
Keywords
Introduction
Approximately 50 million individuals worldwide are currently living with dementia (World Health Organization, 2017). Compared with the general population, older adults with dementia in hospitals experience poorer nutrition and functional ability, an increased risk of delirium, longer hospital stays, and higher risks for mortality and falls (Mukadam & Sampson, 2010; Rudolph et al., 2010; Sampson, Blanchard, Jones, Tookman, & King, 2009; Sampson et al., 2014; Zhu et al., 2015). Staff in acute care settings, however, do not provide high-quality care for older adults with dementia due to the focus on managing acute illnesses and inadequate staff training (Dewing & Dijk, 2016; Turner, Eccles, Elvish, Simpson, & Keady, 2017).
As dementia progresses, the likelihood of persons with dementia experiencing responsive behaviors increases. Responsive behaviors are defined as words, movements, or actions that persons with dementia use to have their needs known, and the term emerged from persons with dementia (Murray Alzheimer Research and Education Program, 2017). Examples of responsive behaviors include grabbing onto others, wandering, yelling, hitting, kicking, restlessness, repetitive sentences/questions, making noises, and sexually inappropriate behaviors (Alzheimer's Society of Canada, 2017; Draper, Finkel, & Tune, 2015). We chose to use the term responsive behaviors compared with other well-known terms such as Behavioural and Psychological Symptoms of Dementia (BPSD) as responsive behaviors are more reflective of the constructivist paradigm underlying Thorne's (2016) interpretive descriptive approach used in this study. Responsive behaviors acknowledge the multiple layers that exist underneath a behavior and the various behaviors that can be used by persons with dementia to respond to a situation or environment. Responsive behaviors have been identified by persons with dementia as the preferred term and is widely adopted (Dupuis, Wiersma, & Loiselle, 2012). This term also reflects person-centered language, and this type of language is one of the recommendations of the Alzheimer's Society of Canada (2012) to maintain the dignity of persons with dementia. The term BPSD appears to be more in keeping with a clinical diagnostic language or a medicalized term. The terms challenging and aggressive behaviors have negative connotations and suggest that a problem is caused by an individual (Alzheimer's Society of Canada, 2012).
Approximately 70% to 90% of persons with dementia will be affected by responsive behaviors over the course of their disease (Freeman & Joska, 2012). When older adults with dementia receive care in hospital, 75% of this population will experience responsive behaviors at least once (Sampson et al., 2014). The hospital environment may trigger responsive behaviors among older adults with dementia (Sampson et al., 2014) and lead to feelings of distress, insecurity, anxiety, and fear (Baille, Cox, & Merritt, 2012; Hynninen, Saarnio, & Elo, 2016). Hospitalization heightens the sensitivity of clients with dementia to responsive behaviors due to being in an environment with numerous triggers (e.g., noise and poor lighting) and receiving care from staff who have limited knowledge of their preferences (Schindel Martin et al., 2016).
Responsive behaviors are symptoms of dementia that are perceived by health-care professionals to be one of the most difficult aspects of dementia care to address in acute care settings. With the growing number of older adults with dementia in acute care settings, health-care professionals are not able to meet the needs of this population due to a lack of understanding of dementia and ability to address responsive behaviors (Turner et al., 2017). Nurses may be the most impacted by responsive behaviors in acute care settings as they spend more time in providing direct care than other health-care professionals (Westbrook, Duffield, Li, & Creswick, 2011). Nurses are expected to excel in providing dementia care despite inadequate staffing and few educational training opportunities (Coffey et al., 2014). Due to lack of skills and knowledge in caring for clients with responsive behaviors of dementia, nurses report being hit, bitten, or physically injured (Marx et al., 2014). Nurses perceive that almost 50% of negative physical and verbal experiences occur during the delivery of care for clients with dementia in hospitals (Speroni, Fitch, Dawson, Dugan, & Atherton, 2014). Experiencing responsive behaviors in the workplace affects job satisfaction, leads to burnout, and causes nurses to contemplate changing professions (Public Services Health and Safety Association, 2007).
There are a number of educational programs for health-care professionals to help them better support individuals with responsive behaviors such as Montessori/DementiAbility (DementiAbility Enterprises, 2016), Gentle Persuasive Approaches (GPA; Schindel Martin et al., 2016), and P.I.E.C.E.S. education (Behavioural Supports Ontario [BSO] Education and Training Committee, 2012). P.I.E.C.E.S. is a 2-day educational workshop for health-care professionals delivering care for persons with complex mental health behaviors such as responsive behaviors of dementia (Hamilton, Harris, Le Clair, & Collins, 2010). P.I.E.C.E.S. constitutes an acronym that considers the following factors as instrumental in the quality of life of older adults: Physical, Intellectual, Emotional, Capacities, Environment, and Social (McAiney et al., 2007).
Some studies have explored the experiences of health-care professionals with responsive behaviors; however, these studies generalize the experience of all providers without considering the unique role that nurses play in delivering care for older adults with responsive behaviors (Houghton, Murphy, Brooker, & Casey, 2016; Hynninen, Saarnio, & Isola, 2014). Previous studies have explored the experiences of providers caring for persons with dementia in specific acute care settings (e.g., surgical settings, emergency departments, and psychogeriatric units; Cunningham & McWilliam, 2006; Edvardsson & Nordvall, 2008; Hynninen et al., 2014), but none have focused specifically on acute medical units (i.e., general internal medicine). Some studies were focused on general hospital settings and did not differentiate their findings based on type of units (Digby, Lee, & Williams, 2016; Houghton et al., 2016; Moonga & Likupe, 2016; Turner et al., 2017). It is important to recognize the uniqueness of acute medical units as these areas provide services to a large clientele of persons with dementia (Sampson et al., 2009, 2014).
Little is also known about the Canadian nursing experiences in delivering care for older adults with dementia experiencing responsive behaviors in acute care settings although many nurses are caring for this population. Canadian nurses were caring for about 90,000 older adults with dementia in hospital in 2016, and about 38% of older adults with dementia were hospitalized on more than one occasion (Canadian Institute for Health Information, 2018a). Canada is a unique population with a large amount of ethnic and cultural diversity, and this is an important consideration for nurses when implementing holistic dementia care. Canada is renowned for universal health-care and has been found to be one of the highest spenders on health from a global perspective where spending has now reached $200 billion annually (Canadian Institute for Health Information, 2018b). Health-care spending has been aimed toward dementia care through the recent passing of the National Strategy for Alzheimer's Disease and Other Dementias Act (2017), but little is known about whether Canadian nurses feel that they are being supported in care delivery for older adults with dementia in hospital.
The present study aims to address the gaps in research by providing a Canadian perspective on nursing experiences in the delivery of care for older adults with dementia experiencing responsive behaviors in acute care settings. This understanding is important because it has potential to guide nursing practice and education in effectively addressing responsive behaviors in hospital settings. The research questions of this study were as follows: (a) What are the nursing experiences of care delivery for older adults living with dementia who express responsive behaviors in acute medical settings, and (b) what are the recommendations of nurses to improve dementia care in acute care settings?
Method
Study Design
The design that was used in this study was Thorne's (2016) interpretive description approach as it is suitable for exploring clinical practice issues and realities. In the study, the clinical practice issue consists of nursing care delivery for older adults with dementia experiencing responsive behaviors on acute medical units. Interpretive description (Thorne, Kirkham, & Macdonald-Emes, 1997) has been widely applied by various disciplines. Interpretive description is appropriate for examining multidimensional clinical phenomena (Thorne, 2016).
Setting
The setting for the study was four acute medical settings (i.e., three clinical teaching units and a cardiology unit) in an urban teaching hospital in Southern Ontario, Canada. Approximately 130 acute medical beds are located within this hospital.
Sampling
Participants consisted of registered nurses, registered practical nurses, and allied health professionals (e.g., occupational therapists, a social worker, a physiotherapist, and P.I.E.C.E.S. educators). Although the main purpose of the study was to focus on nurses' experiences in delivering care for older adults with responsive behaviors of dementia, we sampled a small number of allied health professionals (n = 5) so that their experiences could complement the understanding of nurses' experiences. We sought to understand the diverse experiences of allied health professionals in delivering care and their recommendations for improving dementia care.
Purposive sampling was used including criterion, maximum variation, and theoretical sampling (Creswell, 2013). Nurse participants met the following criteria: (a) hold the professional designation of registered nurse or registered practical nurse, (b) work in an acute medical setting, and (c) have cared for at least one older adult with dementia experiencing responsive behaviors in an acute medical setting within the past 2 years. Allied health professionals met the following criteria: (a) experience in either caring for or interacting with older adults with dementia experiencing responsive behaviors in acute medical settings, (b) currently collaborating with nurses in delivering dementia care or supporting the practice of providers by delivering P.I.E.C.E.S. education, and (c) have received P.I.E.C.E.S. education. We intentionally sought P.I.E.C.E.S.-trained health-care professionals to explore their perspectives of P.I.E.C.E.S. education, and the results are reported in another article (Yous, Ploeg, Kaasalainen, & Martin, 2019). Maximum variation sampling (Patton, 1990) was used to locate participants with varied work experience, education levels, and dementia care preparation. Theoretical sampling was used following data collection and analysis of the initial phase of the study as patterns and themes emerged (Thorne et al., 1997; Thorne, 2016). The gap in understanding that led us to further sampling was the need to understand nursing experiences based on varied years of experiences.
Recruitment
To recruit participants for this study, we requested that a BSO leader send an introductory e-mail invitation to all eligible participants. BSO is an organization that provides specialized services for persons living with complex mental health disorders including responsive behaviors of dementia (BSO, 2017). Nursing managers shared information about the study during their nursing rounds. The primary author provided brief in-person introductions for nurses on acute medical units and posted recruitment posters in the staff rooms and at nursing stations. An incentive was offered to all participants (i.e., $25 gift card).
Data Collection
Sample Interview Questions.
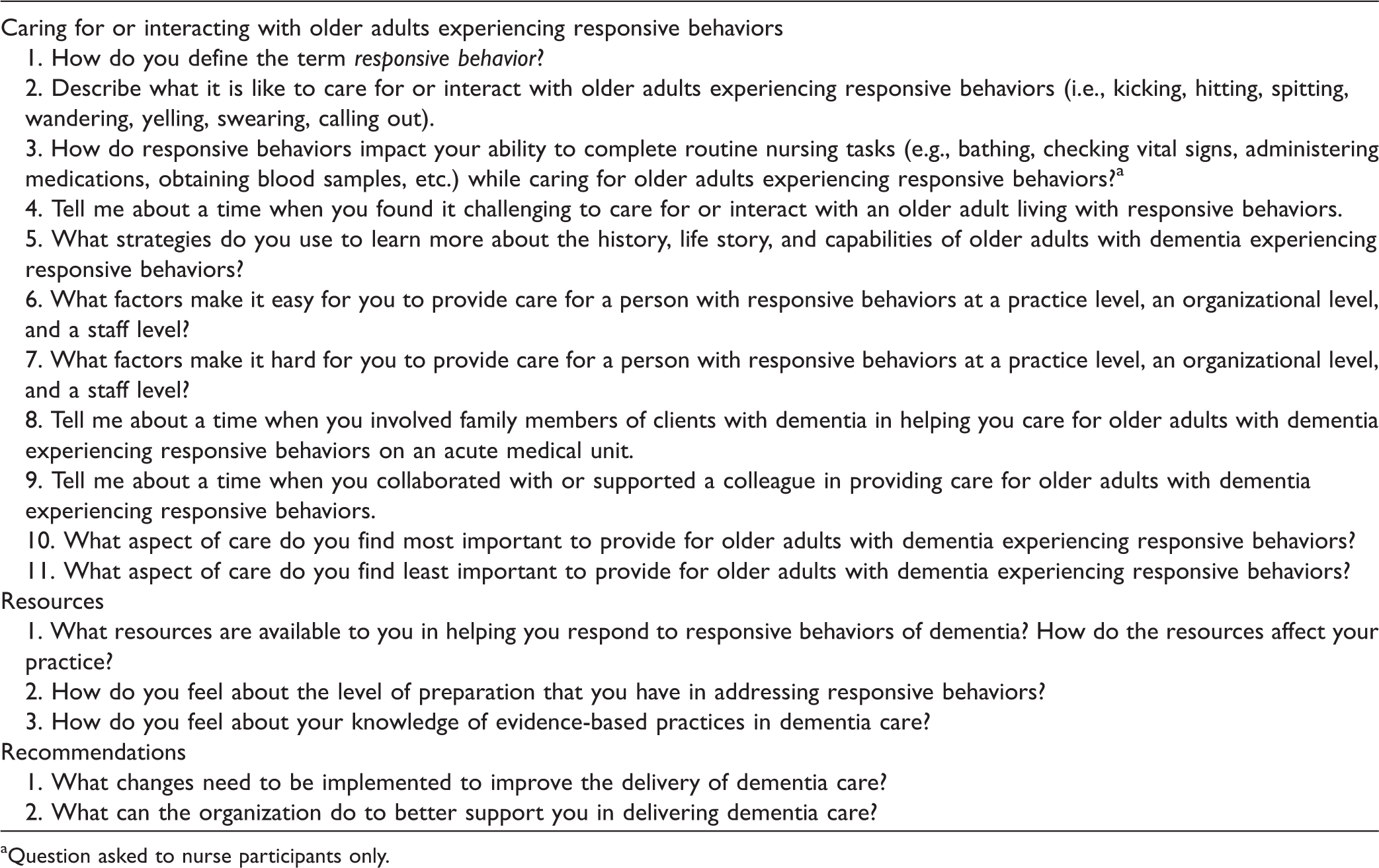
Question asked to nurse participants only.
Data Analysis
Thematic analysis was used in this study as it was consistent with Thorne's (2016) design, and it identifies themes and patterns within data by focusing on the research question (Braun & Clarke, 2006). Experiential thematic analysis, a form of thematic analysis, focuses on the viewpoints of participants and their experiences (Braun & Clarke, 2013). We used experiential thematic analysis as an interpretive framework guiding the creation of codes and themes as it was consistent with interpretive description (Thorne, 2016). It involves a process of interpreting data to name themes (Braun, Clarke, & Terry, 2014). The actual words of the participants are recognized as narrative data that support the naming of themes through interpretation. Data obtained from the nurses were analyzed separately from data obtained from allied health professionals. Data analysis was conducted independently by all members of the research team (M. Y., J. P., S. K., L. S. M.). A coding tree was developed by M. Y. and J. P. and then refined by all members through consensus discussion. We followed the six phases of thematic analysis: (a) becoming familiar with the data, (b) performing coding, (c) seeking themes, (d) reviewing themes, (e) creating a definition for themes and naming them, and (f) developing a written report (Braun & Clarke, 2006). Consensus regarding inclusion and naming of themes was reached through open team discussions during monthly meetings that occurred over 4 months. Dedoose, a computer software program, was used to help organize themes (SocioCultural Research Consultants, 2018).
Rigor and Trustworthiness
For interpretive description, the criteria to achieve credibility consist of “epistemological integrity, representative credibility, analytic logic, and interpretive authority” (Thorne, 2016, p. 96). To reflect epistemological integrity, we ensured that our line of reasoning was aligned with the research purpose, study design, and assumptions about knowledge. We maintained an epistemological position using transparency and made notes in a reflexive journal to ensure that our assumptions did not influence the interpretation of results. For representative credibility, we used triangulation of two data sources to expand knowledge generated through different worldviews (Thorne, 2016). We included data from allied health professionals to support the claims made by nurses and to offer an alternative perspective on caring for older adults with dementia. Allied health professionals were included in the study because they work closely with nurses and could provide valuable insight regarding collaborating with nurses. They also provide an insider perspective on how they perceive nurses to deliver dementia care in hospital.
Credibility was maintained in this study by using purposive sampling to seek information-rich participants and reaching data saturation. In terms of analytic logic, we ensured that for the study process, the description of our research methods was detailed and sound (Thorne, 2016). A thorough review of the current literature was conducted prior to developing the research protocol to ensure that this study was supported by recent evidence and reflected the current gaps in the literature. In considering interpretive authority, we displayed honesty in findings and took into consideration past experiences (Thorne, 2016).
Ethical Considerations
Ethics approval was received from the Hamilton Integrated Research Ethics Board (HiREB #4101). All participants provided written informed consent prior to the interviews, and participation was voluntary. Participants were provided with the option to refuse to answer any questions and withdraw from the study at any time without facing any consequences.
Findings
Demographic Characteristics
Demographic Characteristics of Participants (N = 15).

Themes
Themes and Subthemes of Nurses' Experiences.

Nurses' Experiences in Addressing Responsive Behaviors of Dementia
Delivering Care Is a Complex Experience
Navigating through different perspectives
Nurses reported navigating through and incorporating different perspectives when delivering care for persons with dementia including perspectives of family members of older adults with dementia and allied health professionals. To avoid conflicts, nurses often negotiated care priorities with families of persons with responsive behaviors. … there is one particular family that came in and did not like the way we were managing the patient… . They're finding fault with everything we do yet, we were doing amazing with this patient … you have to look at every side… . So you try and listen, you try and negotiate … (N04)
Providing care can be challenging
Nurses perceived that being able to deliver nursing care for older adults living with responsive behaviors is challenging. Almost half of the nurses felt that performing invasive treatments and assessments for persons with dementia took more effort, time, and skill than for other clients. Nurses recognized that clients with dementia may not be able to understand the benefit of such tasks and refused care; however, nurses still initiated intravenous therapy and obtained vital signs as these were seen as necessary. One nurse reported distress for a client when obtaining a blood pressure reading: … putting a blood pressure cuff on their arm … that tightens, can escalate their behaviours. They think we're doing that to them, it's uncomfortable… . They get stressed out, their blood pressure gets elevated, their reading may not be accurate… . So in that aspect of basic nursing care, it is difficult. (N02)
Embarking on an emotional journey
Nurses experienced one emotion after another, and sometimes emotions were experienced simultaneously such as anger and vulnerability. The most common emotions expressed by nurses were frustration, anger, fear, and sadness. A nurse describing an experience in being met with responsive behaviors of a physical nature stated: You try to control your emotions or your anger. You just gotta realize that these are patients and they don't know what they're doing sometimes… . There's anger … you kind of like feel sometimes helpless at the same time because you can't do anything. (N10)
When met with physical forms of responsive behaviors, nurses stated that they were upset because they felt that “nothing is being done” (N01) on the part of the organization to address and prevent these occurrences. When nurses witnessed clients experiencing responsive behavior of a physical nature and unintentionally harming others, this brought about feelings of sadness through empathy. “I don't think they walk around thinking ‘oh, I am gonna beat them up’. I think there's something that's initiating that and it's very sad” (N06).
Nurses experienced frustration in not being able to consistently meet the needs of clients with dementia: “ … you get a little frustrated too because it's a medicine floor. It's very busy” (N03). Allied health professionals similarly experienced frustration in delivering care for older adults with responsive behaviors. “It's the calling out, it's the crying and repetitive questions that I find harder to handle personally” (AHP02).
Using Pharmacological Strategies
Using chemical restraints in desperate situations
Nurses reported using chemical restraints as a last-resort solution and in times of desperation when they felt that they had exhausted nonpharmacological approaches. Nurses reported using chemical restraints when de-escalation was ineffective and clients had signs of distress: “ … a patient is getting aggressive, it's a language barrier, they're kicking, they're screaming, they're biting and the only form before physical restraints … it's usually prn Haldol [antipsychotic] or something chemical … ” (N02). Feeling desperate also meant that nurses felt they had no other choice but to administer a chemical restraint as they were falling behind on their nursing duties.
Administrating chemical restraints as a proactive approach
Some nurses reported administering chemical restraints for persons with dementia with known responsive behaviors before these behaviors were exhibited. Being proactive in this sense was perceived as a way to prevent client harm to themselves and others. Nurses would ask physicians if they could order medications for clients with responsive behaviors if they felt that clients had a routine of exhibiting responsive behaviors at a certain time: … usually if I think somebody should have something[medication] to help them settle like at 3 pm, I'll go to the doctor or geriatrician and say “you know what … he gets agitated, can we get something you know prior to knowing that it's coming?” (N01)
Using Low Investment Nonpharmacological Strategies
Nurses used simplistic forms of nonpharmacological approaches to deliver care for persons with dementia including involving different individuals (e.g., one-on-one providers, families, and specialty teams) and person-centered strategies. These strategies required low investment in terms of resources and time.
Involving allied health professionals and specialty teams
Collaborating with and including a variety of allied health professionals in the care of persons with dementia were perceived to be beneficial by all nurses. Specialty teams such as those composed of geriatricians and BSO clinicians were perceived as valuable resources to provide dementia care recommendations. Involving allied health professionals promoted sharing of information about the client and care planning: … as a nurse we take the broad way but the other healthcare providers like PT [physiotherapist], OT [occupational therapist], they share a different way about the patient and when we talk about the patient, we can see the big picture and then plan for the patient. (N09)
Involving families
Nurses recognized the need to involve families in the care of persons with dementia because they have the most knowledge about the person and serve as a source of familiarity. All of the nurses reported involving families in the care of persons with dementia experiencing responsive behaviors throughout their stay on acute medical units: “ … talking to their family or friends is the easiest thing and the most useful resource because they tend to be the ones that know the patient the most” (N05). Allied health professionals similarly recognized the value of collaborating with families to understand the life story of clients with dementia. In cases where they are not able to share or be a good historian for themselves, you look to … the closest person to them. It could be a family member, it could be a friend but you search for things that are from their distant past, things that will resonate with them, proper names, routines, things that will … make their heart sing and music is an example of that. (AHP05)
Using person-centered approaches
Nurses incorporated simplistic forms of person-centered approaches to understand the reality of persons with dementia, learn more about them, and respect their preferences. Nurse felt that it was important to individualize care for this population. Nurses implemented person-centered care approaches based on the “routines” (N01) of persons with dementia and provided them with their favorite activities: “what they love to watch, like shows [on television]” (N10). Some nurses reported using some type of a person-centered approach to help them care for older adults experiencing responsive behaviors such as creating a calming and familiar atmosphere through music: “I love playing music for patients. I think that music always brings out memories whether good or bad and in most cases they are good. So if there's a certain type of music that they like in the past … ” (N02). Some of the approaches used by nurses did not require that the nurse remain with the client. For example, nurses offered a newspaper to clients with dementia so that they may read it alone at a table.
Nurses' Experiences in Delivering Dementia Care
Facing Barriers in Dementia Care
Limited time and a focus on acute needs
Nurses reported that having enough time to provide client care was a significant barrier on acute medical units. Some nurses felt that delivering care for persons with dementia was time-consuming. Nurses felt that they spent more time with persons with dementia than other clients when de-escalating situations where responsive behaviors occur. Acute priorities were perceived as most important, and dementia care was given little priority when faced with urgent issues: “Due to acuity in patients, it's priority over chronic. So when we have a code going on or an MI [myocardial infarction], that takes precedence. And then the patients with dementia unfortunately become lower on the priority scale … ” (N02).
Allied health professionals also felt that nurses are often preoccupied with attending to acute care issues leading to lack of attention for clients with responsive behaviors. … a lot of the nurses are involved with patients who have acute medical needs and often times they're busy with these patients who are acutely ill. And in the meantime, something is happening with these patients with the responsive behaviors because there is nobody to supervise or assist them … (AHP01)
A fast-paced environment and push for discharges
Nurses perceived acute medical settings to be highly active and busy areas of the hospital making it challenging to provide dementia care: “ … it's hard because it's a fast-paced place … people are coming and going to tests all day … more people in the room… . The porter's there, the nurse's there … it's an active environment so it's even harder” (N07). Nurses and allied health professionals also felt that the focus on expediting discharges in these settings led to challenges in care delivery for persons with dementia: “I would say because there's such a large focus on discharge and trying to discharge people quickly and move them through the system that I think that is one of the biggest challenges [in providing dementia care]” (AHP03).
Inadequate staffing and heavy workload
Most nurses felt that care provided for persons with dementia was sometimes compromised due to lack of available staff on acute medical units: “We cannot look after these patients the way they should be looked after based on that we don't have the staff to do it” (N04). Nurses perceived that inadequate staffing and heavy workload affected their ability to interact, build a therapeutic relationship, and provide comfort for clients with dementia. Nurses felt that their organization did not provide them with enough staffing support to care for clients with dementia experiencing responsive behaviors in terms of personal support workers (PSW) and nurses.
Understimulation for older adults with dementia
Some nurses and an allied health professional reported understimulation in acute medical environments as impacting the care and well-being for clients with dementia. This understimulation may lead to responsive behaviors and decline in the functional status of clients. Nurses felt that clients with dementia lack stimulation in terms of activities and interactions with family members, potentially leading to confusion. I think they're very bored. I think they're just sitting in their rooms looking at the four walls. Some of them can't walk … sometimes they don't have family members. I think just sitting there bored, you're gonna get even more confused too. (N01)
Encountering Facilitators in Dementia Care
Shared care practices and strong interprofessional collaboration
Nurses felt that care provided for persons with dementia should be a collaborative effort among nurses and allied health professionals. Having an interdisciplinary team accessible to nurses and strong interprofessional collaboration was perceived as beneficial for persons with dementia in holistically meeting their needs. Half of the nurses in this study felt that acute medical units already shared a naturally strong sense of interprofessional collaboration. Most nurses believed that when providers help care for clients with dementia, care delivery was much easier. … these patients belonging to everyone … I've never nursed him before but, having seen him in action and sitting there and kind of taking over when the going gets rough for the other nurse. We all help him and it's much easier for me to deal with him … (N04)
Good continuity of care
Having continuity of care ensured that persons with dementia were being cared for by familiar nurses who recognized their routines and encouraged communication of their routines to other providers. Continuity of care was also perceived as helpful for staff as this encouraged consistent consideration of the person's preferences, needs, and routines on the part of providers: I think it [continuity] helps a lot … they're used to my familiar face whereas if it's a new nurse and a stranger and doesn't know what works for them or their routine … they might tend to listen more to me because I had them for a week and they're more familiar with me. (N01)
Holding team meetings
Team meetings (i.e., huddles and behavioral rounds) were perceived by some nurses to be facilitators in ensuring that information and approaches in caring for persons with dementia were communicated to nurses and allied health professionals. Behavioral rounds consisted of meetings implemented in acute medical units that focused exclusively on discussing plans of care for clients with dementia experiencing responsive behaviors. Nurses reported that behavioral rounds encouraged sharing of suggestions for care for persons with dementia within the team: “ … of course the behavioural rounds might help more because we have more time to look at the patient in detail and then sharing … if you work cooperatively with other co-workers then of course it helps” (N09).
Most allied health professionals also reported that team meetings were beneficial in implementing dementia care in acute medical units. They expressed that interdisciplinary team meetings were most beneficial to “see whether the plan needed any changes” (AHP01) during the hospital stay of clients with dementia experiencing responsive behaviors.
Recommendations to Improve Care Delivery
Recommendations to Improve Care Delivery for Persons With Dementia.

Note. BSO = Behavioural Supports Ontario.
Ensuring Adequate Staffing on Acute Medical Units
To improve dementia care, nurses recommended that units are adequately staffed with nurses and PSW who are trained in dementia care: “Add additional staffing, educated staffing. I think that's probably the biggest one” (N06). Nurses perceived that care for clients with dementia was time-consuming, and some nurses therefore recommended more staff to help care for them: I think the more dementia patients that we have, the more staff that we should have. Instead of having five patients on days, you have two with dementia, you know, you should have an extra nurse too… . So, I just have four patients and two with dementia … (N01)
Increasing Support From BSO
Nurses and some allied health professionals recommended increased services and support from BSO on acute medical units to serve as a dementia care resource when caring for persons with responsive behaviors: “ … because the demographic has changed, having them [BSO] more frequently on the floor might be more helpful … ” (N08). BSO clinicians were seen as responsible for conducting comprehensive assessments of clients with responsive behaviors and provide a plan for staff to follow. Nurses also recommended that BSO should be involved in orientating new nurses to the hospital to support them in their care for clients with responsive behaviors: “ … having them [BSO] involved in hospital orientation would be a great resource … it doesn't have to be a full-day, just half a day, a couple hours to explain the approach of how to deal with patients … ” (N02).
Providing More Educational Reinforcements
Lack of regular training opportunities was perceived by nurses to impact their ability to effectively care for clients with responsive behaviors. Ongoing reinforcement was perceived as necessary to support nurses in caring for older adults with responsive behaviors. None of the nurses or allied health professionals reported opportunities provided by their organization to annually review learning from educational programs in dementia care. Most of the staff reported receiving GPA education (Schindel Martin et al., 2016) several years ago and had not received any further education or review of GPA since then. Some of the nurses recommended that P.I.E.C.E.S. education be provided for providers throughout their organization: I think providing us with more training even. P.I.E.C.E.S. I've never taken it before but, I've heard of it. Even providing training like that would be very helpful and in terms of providing more resources or personnel with knowledge or a lot more information on how to care for dementia patients for us would be very helpful. (N05) I find we don't really have in-services… . I've gotten emails about like presentations but, these are an hour and a half, two hours presentations. They're not great for nurses on the unit … if they could provide like half an hour to 45 minutes of something that we could go to on our lunch, that might be helpful. (N08)
Implementing More Family and Team Meetings
Nurses discussed the need for more family and team meetings to discuss plans of care for persons with responsive behaviors and to ensure that nurses' voices are heard at these meetings. These were perceived as ways to communicate information about clients with responsive behaviors to other providers and to enhance shared practices: I see quite a few patients on my unit with responsive behaviours and I feel like … maybe as part of our meeting or huddle, it would be good to let's say make everybody aware of which patients are the ones that are actively exhibiting responsive behaviours so everyone can kind of … look out for these patients… . Generally, our meetings don't really focus on that. (N05) … it would be beneficial for us to be included in those discussions [team meetings] … we hear their [family members'] perspectives and the doctors often miss family members … we could provide insight into how the family's feeling. Are they feeling stressed out, burned-out? Are they willing to go back home with extra support? … . I think nurses could provide that perspective. (N08)
Creating a Safe Unit
Nurses in this study recommended that the organization create an acute care unit that includes trained staff and appropriate resources for dementia care. Nurses recommended that these units be locked for the safety of clients and that they accommodate persons with responsive behaviors by providing them with more space to walk freely on the unit: “More locked units. More units that patients are able to wander. I find that all they want to do is just walk. They just want to walk, they just want to touch, they just want to explore” (N02). Nurses emphasized the need to have adequate staffing and specially trained care providers on such units: … ideally, they should have a specific unit, maybe a specific acute care unit for patients that have these types of behaviours and staff it accordingly so that the right type of trained people are on those units … wouldn't that be lovely? (N06) See we get these patients who are like physically responsive or responsive behaviours with physical aggression but, we don't get that like in acute mental health where they have that badge and they just press it and then it will just alarm all the security to come. We don't have that. Like we have to basically yell help! (N10)
Discussion
The key findings of this study were as follows: (a) Care delivery is a complex experience with multiple challenges for nurses due to navigating through different perspectives and feeling various emotions, (b) nurses perceived a lack of action on the part of their organization to prevent and address responsive behaviors of a physical nature, (c) nurses used pharmacological approaches in their care in times of desperation, and (d) nurses used low-investment nonpharmacological approaches to respect the preferences of and learn more about clients.
Comparison With the Existing Literature
Providing nursing care and treatment for clients with responsive behaviors was perceived as challenging, and this is consistent with other studies (Digby et al., 2016; Houghton et al., 2016; Moonga & Likupe, 2016). Monthaisong (2018) similarly found that caring for persons with dementia is complex as nurses work under pressure, and they face challenges perhaps due to lack of dementia care knowledge. Nurses in the current study found themselves in an ethical dilemma in providing necessary treatments while clients with dementia were clearly in a state of refusal or distress. Nurses face ethical dilemmas as they often meet uncertainty in making difficult decisions for clients with dementia despite their resistance to care (Eriksson & Saveman, 2002; Moonga & Likupe, 2016).
Nilsson, Rasmussen, and Edvardsson (2013) found that feelings of anger and fear among nurses were related to caring for clients with dementia experiencing confusion or resistance to care; however, nurses in the current study typically had feelings of anger when met with responsive behaviors of a physical nature. A new finding of the current study was that not only were nurses upset when they were hurt, but they were also upset with their organization due to lack of action after such incidents and few strategies put in place to prevent responsive behaviors of a physical nature from occurring. Previous studies discussed the need for nurses to meet the emotional needs of clients with dementia (Baille et al., 2012; Cowdell, 2010); however, the current study reveals that nurses also need support from their peers and management to regulate their own emotions in dementia care.
Nurses in this current study were found to rely on chemical restraints in times of desperation due to limited resources in acute medical settings and when they wanted to prevent responsive behaviors from occurring. Hynninen et al. (2014) found that nurses and physicians perceived that chemical and physical restraints increase the personal safety of clients by preventing falls and helped to overcome resistance to medical treatment. Current clinical recommendations suggest administering chemical restraints only for severe symptoms of BPSD related to high risk for safety and severe agitation and not for other behaviors such as wandering (Conn, Gibson, & McCabe, 2014; Registered Nurses' Association of Ontario, 2016). When chemical restraints are used improperly among older adults, there is an increased risk for delirium, excessive sedation, and harmful interactions with other medications (Conn et al., 2014; Inouye, Westendorp, & Saczynski, 2014).
Nurses in the current study involved other individuals to make care delivery easier for persons with dementia. Nurses relied on the expertise of specialty teams and knowledge received from family members regarding their loved ones in providing dementia care. Involving families in the care of persons with dementia in acute care settings is valuable in helping staff recognize possible triggers for responsive behaviors and provide comfort for these clients by decreasing anxiety (Digby et al., 2016; Houghton et al., 2016).
Dementia care was perceived by nurses as consuming additional resources such as time and staff when these resources were already scarce in acute medical units. Other studies have also found that inadequate staffing and heavy workload in hospital led to poor quality of care for clients living with dementia (Byers & France, 2008; Hynninen et al., 2016). Nurses in the current study also felt that acute medical environments did not provide enough stimulation for older adults with dementia in terms of therapeutic activities and human interaction. Similarly, Edvardsson and Nordvall (2008) found that poor engagement and a strong emphasis on routine nursing tasks led to clients with dementia reporting feelings of boredom on psychogeriatric units.
Nurses in the current study typically used simple forms of person-centered approaches to care for clients with dementia such as talking or walking with them, playing music, and offering reading materials. Some of these approaches require little investment on the part of nurses in terms of resources and time. Some nonpharmacological approaches can also be implemented without the nurse having to remain present with the client such as when playing music or offering a newspaper. Because person-centered approaches requiring low investment are being used by nurses in acute medical settings, it is important for staff and organizations to consider whether current practices preserve the selfhood of persons with dementia. Post (2013) advocates for the continual preservation of the personal identity of persons who are forgetful by focusing on aspects that still have meaning for them such as creativity, emotions, music, spirituality, and tactile sensations. Regardless of the person-centered approach implemented, nurses should consider whether they are targeting similar aspects that consider the uniqueness of individuals.
Delirium was seldom discussed by nurses in the study as a contributor to responsive behaviors; however, delirium superimposed on dementia affects 22% to 89% of older adults in hospital and in the community (Fick, Agostini, & Inouye, 2002). Older adults with dementia who acquire delirium while in hospital experience poor outcomes such as higher mortality rate, longer hospital stays, and poor function upon discharge (Chen, Saczynski, & Inouye, 2014; Fick, Steis, Waller, & Inouye, 2013). Nurses in the current study often associated responsive behaviors to a diagnosis of dementia rather than delirium, and they administered chemical restraints even before responsive behaviors occurred in persons with dementia. Administering medications to address responsive behaviors may only worsen responsive behaviors or mask the presence of delirium among older adults with dementia (Fick et al., 2002). Nursing practice and educational efforts have been put in place to help nurses recognize delirium and delirium superimposed on dementia. Some educational programs (e.g., GPA and P.I.E.C.E.S.) educate staff on delirium, and tools such as the Confusion Assessment Method are used in hospitals to help staff detect delirium (Inouye et al., 1990). These efforts, however, are often aimed at exploring delirium and dementia in isolation rather than exploring their combined impact on responsive behaviors.
A new contribution made by this study is that strong interprofessional collaboration can help to address the challenges faced with providing care for clients with dementia. Having an accessible and diverse health-care team on site made it easier for nurses to care for clients with dementia and ensured that the social needs of clients were met. Having strong cohesion within the interdisciplinary team ensures care is being shared for clients with dementia and that staff are learning from one another based on individual experiences (Chater & Hughes, 2013).
Strengths and Limitations
Strengths of this study were the inclusion of both nurses and allied health professionals to better understand the experiences of nurses in providing care for older adults living with responsive behaviors. By including multiple data sources as suggested by Thorne (2016), credibility and validity were further enhanced (Lincoln & Guba, 1985). A strong analytical approach was used to develop themes and subthemes through experiential thematic analysis using Braun and Clarke's (2006) six phases of data analysis.
The limitations of the study were the inclusion of a small number of participants (n = 15). Most of the participants in the study were female; however, this is reflective of the trends in the nursing workforce as more than 90% of nurses working in Ontario are female (Canadian Institute for Health Information, 2012). The study also included acute medical units within one large urban teaching hospital in Ontario, Canada, and it may be difficult to transfer findings to other locations or clinical settings. Only P.I.E.C.E.S.-educated allied health professionals were included in the study, which could have contributed to a potential bias in responses due to the influence of dementia care education. Most of the participants in the study had received dementia care educational training within the past 5 years with all but one participant having received GPA education, and 9 out of 15 participants received P.I.E.C.E.S. education. Participants' responses suggest that they recognized responsive behaviors, and responses may be reflective of their educational preparation in dementia care.
Conclusion
This study provided an in-depth exploration of the nursing experience in delivering care for older adults experiencing responsive behaviors of dementia within acute medical units. The study revealed that delivering care for this population is complex and often confounded by numerous acute care barriers (e.g., limited time, heavy workload, lack of staff, and focus on acute care priorities). Practice implications are that there is a need for improved support on the part of the organization in terms of preventing and addressing responsive behaviors by ensuring adequate staff on acute medical units (i.e., nurses, PSW, and Bartimaeus workers), offering educational opportunities in dementia care, and promoting strong interprofessional collaboration. Organizations should ensure that guidelines in using nonpharmacological approaches are accessible to staff delivering care for older adults living with responsive behaviors of dementia throughout the hospital. Consistent with the suggestion by Moonga and Likupe (2016), this current study also reveals that more research is needed to explore ethical dilemmas faced in providing care for clients with dementia experiencing responsive behaviors to understand how nurses make difficult decisions in acute care.
Footnotes
Acknowledgments
The authors would like to thank all participants for their time, the director of nursing and nursing managers at the study site as well as the coordinators and clinicians at BSO.