
Abstract
Introduction
Despite the fact that cognitive behavioral therapy is regarded as a superior pain relief method and an alternative to drug therapy, little is known about its scope of application and determinant factors. As a result, the study sought to assess nurses’ knowledge and practicing level of cognitive behavioral pain relief methods in public hospitals in eastern Ethiopia.
Objective
To assess the knowledge and practicing level of cognitive behavioral pain relief among nurses working in public hospitals of eastern Ethiopia.
Methods
A cross-sectional study was conducted among randomly selected 390 nurses. The data were collected using a self-administered questionnaire. The data were entered into Epi-data 3.1 and exported to SPSS 22 for analysis. Bivariate and multivariate logistic regression models were used to identify factors associated with cognitive behavioral therapy.
Result
In this study, more than half (54.1%) of the respondents had good cognitive behavioral methods practicing levels. Nearly two-thirds (58.8%) of the participants had adequate knowledge about pain relief methods. Having adequate knowledge (adjusted odds ratio [AOR] 2.664; 95% confidence interval [CI]: 1.75, 4.7), having training (AOR 1.7; 95% CI: 1.03, 3.01), and positive attitude (AOR 4.02; 95% CI: 4.5, 12.4) were significantly associated with cognitive behavioral therapy.
Conclusion
In this study, more than half of nurses had good cognitive behavioral methods practicing levels. Having a positive attitude, being knowledgeable, and having training were determinant factors in the practice of cognitive behavioral therapy. Continuing education and training should be considered for nurses to enhance their cognitive behavioral therapy practice.
Introduction
Pain is defined as an unpleasant sensory and emotional experience associated with tissue damage (IASP 2012). It can be either acute or chronic. Acute pain, such as postoperative pain, vanishes as the body heals. Chronic pain is pain that lasts for an extended period and includes both cancer-related and nonmalignant pain, such as arthritis, low-back pain, and peripheral neuropathy (Wells et al., 2008).
According to estimates of chronic pain prevalence, chronic pain affects 10% of the world's population, or approximately 60 million people. Opioid analgesics are widely diverted and misused, and their widespread use has resulted in a national epidemic of opioid overdose deaths and addiction. Pharmaceutical opioids were responsible for more than a third (37%) of the 44,000 drug-overdose deaths reported in 2013. Simultaneously, there has been an increase in the rate of opioid addiction, which affected approximately 2.5 million adults in 2014 (NSDUH, 2014).
In contrast to opioids, other pain relief methods, such as cognitive behavioral methods, were ignored (WHO, 2007). Cognitive behavioral therapy (CBT) is a type of psychotherapy that assists people in identifying and developing skills to change negative thoughts and behaviors. Several studies have found that CBT can help with pain and other problems. It is an effective method for maintaining emotional distress and behavioral problems such as depression, anxiety, stress, and chronic pain (Aggarwal, et al., 2011, Astin, et al., 2002, Butler, et al., 2006; Lim et al., 2018). Evidence also indicated that CBT alleviates pain and distress by modifying physical sensations, catastrophic thinking, and maladaptive behaviors (Wetherell et al., 2011, Hofmann et al., 2012, Ehde et al., 2014, Lim et al. 2018).
Inadequate pain management can result in negative physical and psychological outcomes for the individual, patients, and their families (Wells et al., 2008). Even though nurses play an important role in pain management, their knowledge and attitude toward pain management were very low. Because the absence of pain is a basic human right, nurses must be equipped with the necessary information to effectively manage pain (Manwere et al., 2015).
In Ethiopia, inadequate cooperation of physicians (77.55%), multiple responsibilities of nurses (74.0%), and an insufficient number of nurses per patient ratio (72.8%) were the main barriers to the practice of pain management (Zeleke et al., 2021). Other evidence also showed that lack of motivation including salary, role confusion, and lack of continuing training were the identified barriers that hinder pain management (Rahel & Getachew 2014). Due to those challenges, pain relief managements were not fully practiced in Ethiopia. Evidence showed that only 40.1% of the professionals used nonpharmacological labor pain management including CBT (Abebayehu et al., 2016). Furthermore, another study done in Ethiopia showed that 26% of the nurses fully practiced pain relief methods (Zeleke et al., 2021).
Cognitive behavioral therapy must be encouraged as part of a comprehensive pain management strategy. Because it is multipurpose, the dosage of analgesic drugs required can be reduced, reducing side effects and lowering health care costs by reducing doctor visits and reliance on expensive medications (Ali et al., 2013; Burns et al., 2020). Studies have emphasized the importance of nonpharmacological pain management techniques such as CBT (George & Kumar, 2013). Furthermore, another piece of evidence also emphasized that since CBT is effective in alleviating pain, depression, and anxiety, and improving quality of life, it should be practiced (Castro et al., 2012; Elyasi et al., 2021; Getu et al., 2021).
Even if nurses had an imperative and critical role in the care of people living with pain throughout their life span and had a role in providing services that strongly influence the effectiveness of pain management including nurse-led CBT (Brown 2013), there is a practice gap in CBT in public hospitals of eastern Ethiopia. Furthermore, as far as the knowledge of the authors is concerned there is no study done on CBT pain management in the eastern parts of Ethiopia. Therefore, this study aimed at assessing nurses’ knowledge and practicing a level of cognitive behavioral pain relief methods in public hospitals in eastern Ethiopia. The finding of this study will have a crucial input for policymakers in setting different strategies for enhancing CBT use as a pain relief method.
Literature Review
The practicing level of nurses toward CBT is varying from place to place. A study done in the USA showed that the practice of CBT was 12.7% (Beissner et al., 2009). A similar study done in Saud Arabia also showed that 65% of nurses practiced one of the CBT (Ali et al., 2013). Regarding studies done in Ethiopia, a study done in Debre Tabor showed that 26% of nurses practiced nonpharmacologic pain management including CBT (Zeleke et al., 2021).
The knowledge level of nurses toward pain management including CBT also varies from one place to another place. A study done in Ethiopia showed that 54.2% of nurses had adequate knowledge regarding pain management (Tekletsadik et al., 2021). A similar study also showed that 51.2% of nurses had adequate knowledge regarding pain management (Jira et al., 2020). Furthermore, studies done in Gondar and Addis Ababa, Ethiopia also showed that 66.9% and 64.9% of nurses had adequate knowledge regarding pain management (Liyew et al., 2020, Wondimagegn et al., 2021).
Even though those studies are done in every corner of the globe, there is still a gap in the practice of pain management. This study aimed at assessing nurses’ knowledge and practicing a level of cognitive behavioral pain relief methods in public hospitals in eastern Ethiopia. The finding of this study will serve as a base for future researchers and it can also serve as an input for policymakers in setting different strategies for enhancing CBT use as a pain relief method.
Methods
Design
A cross-sectional study was conducted in public hospitals in the Harari region, and Dire Dawa city administration, Eastern Ethiopia, from February 1–28, 2018 Harari Region is one of Ethiopia's nine regional states. In the region, there are two military hospitals, two public hospitals, two private hospitals, eight health centers (four urban and four rural), 19 health posts, and 10 private clinics. Among them, HFSUH and JH provide multidimensional aspects of care to patients who need highly qualified/specialized health care services (Harari regional health bureau). HFSUH is a teaching hospital of Haramaya University with a total number of 161 beds and has medical, surgical, gynecology, pediatrics, and psychiatric wards. Regarding the number of health care professionals, there are 168 nurses, 21 midwifery nurses, 2 emergency and critical care nurses, 33 GP, 16 specialists, and 34 pharmacists. Pain management training was given to the nurses from different departments (Human resources of HFSUH). Jugol Hospital is a regional referral hospital of the Harari National Regional state with 95 beds and medical, surgical, and gynecology wards and with a total number of 87 nurses and 23 midwifery nurses (Human resources of Jugol hospital).
Dire Dawa City Administration is one of Ethiopia's two federal city administrations, the other being Addis Ababa. It is located in the eastern part of the country, 515 km from the capital city. Dilchora is a Dire Dawa City Administration referral hospital with 149 nurses, 21 midwifery nurses, and medical, surgical, gynecology, pediatrics, and psychiatric wards (Dire Dawa health bureau, Human Resources of Dilchora hospital).
Sabian primary hospital is another hospital of Dire Dawa city administration, with a total number of 48 nurses and 12 midwifery nurses (Human resources of Sabian primary hospital).
Research Questions
What is the knowledge and practicing level of nurses toward CBT in public hospitals of eastern Ethiopia?
What are the factors significantly associated with practicing level of nurses toward in public hospitals of eastern Ethiopia?
Sample
The sample size was calculated by using a single population proportion formula as follows. n = (Zα/2)2p (1-p)/d2, n = the minimum sample size required, p = estimated proportion of nonpharmacologic pain relief methods Zα/2 = the value of standard score at 95% confidence interval (1.96); with the following assumptions: Confidence level at 95% = 1.96; Margin of error (d) = 0.05 and nonresponse rate = 10% is considered to get appropriate sample size with available resource and proportion of nonpharmacologic pain relief methods = 40% (Abebayehu et al., 2016). The sample size was calculated as (Z∝/2) 2* P(1-q) /d2 = (1.96)2 * 0.4* 0.6/ (0.05)2 = 368 by adding nonresponse rate (10%), the final sample size was 405.
There are two public hospitals in the Harari region namely Hiwot Fana specialized university hospital (HFSUH) and Jugol hospital and two public hospitals Dire Dawa city administration namely Dilchora referral hospital and Sabian primary hospital. In this study area, there were 531 nurses (HFSUH = 191 nurses, JGH = 110 nurses, DRH = 170 nurses, SPH = 60 nurses). From those, 405 study samples were taken by proportional allocation for each hospital (HFSUH = 146 nurses, JGH = 84 nurses, DRH = 130 nurses, SPH = 45 nurses). The individual participant was selected by simple random sampling for the self-administered questionnaire and for the observation the participants were randomly selected among those nurses providing inpatient and emergency service for patients having pain (HFSUH = 14 nurses, JGH = 9 nurses, DRH = 13 nurses, SPH = 4 nurses).
Inclusion and Exclusion Criteria
All nurses working in public hospitals in the Harari region and Dire Dawa city administration were the study population. All nurses have been working for the last six months before the data collection period were included in the study, while those nurses who were on leave during the data collection period were excluded from this study.
Data Collection Methods and Procedure
Structured self-administered questionnaires were used to collect data from nurses. The questionnaires contain five sections which were developed by reviewing previous articles (Bicek 2004, Ali et al., 2013, Rahel & Getachew, 2014, Sitotaw & Zeleke, 2014). It includes the sociodemographic characteristics of the respondent, related to age, sex, religion, educational level, and years of experience of nurses; knowledge level of the respondent; attitude of the respondent; and nonpharmacological pain management including CBT. Four diploma nurses’ data collectors and two BSc nurses’ supervisors were recruited for the data collection, and training for data collectors and supervisors was given.
Measurement
Practicing level of CBT is measured using Likert-scale questions that include encouraging the patient to think about pleasant/positive matters when he/she feels pain, try to focus a patient's thoughts/attention away from pain, encourage the patient to relax different parts of his/her body to alleviate the sensation of pain, teach the patient the correct breathing technique, and encourage the patient by rewarding he/she verbally (Ali et al., 2013). The response levels of all the items were five (not at all, very seldom, sometimes, nearly always, and always) which were coded as not at all = 1, very seldom = 2, sometimes = 3, nearly always = 4, always = 5, and the total score ranges from 6 to 30 and the mean score was 18.5. A practice was considered good practice if the respondent scored mean and above for practice-related questions (Rahel & Getachew, 2014).
Knowledge of Nurses: It was measured using 8 “yes/no” questions, the total scores were computed and the mean score was calculated. Adequate knowledge: those who scored mean and above on knowledge items (Remla et al., 2017).
Positive attitude: Respondents who scored mean and above for attitude-related questions (Rahel & Getachew, 2014).
Workload: If one ICU-trained nurse provides nursing care services for more than two beds in ICU and if one nurse provides for more than six patients in inpatient service other than ICU and emergency per shift is considered as work overload (Ethiopia standard, 2012).
Patient instability: Those patients with clinical presentation either of, altered level of consciousness, systolic BP < 90 mmHg, shortness of breath, pulse rate > 120 bpm, pulmonary edema, and poor skin sign (Obispo, 2007).
Data Quality Control
A pretest was conducted on 10% of the sample at Haramaya hospital to check the reliability of the instrument in which the Cronbach's alpha was 0.75, to estimate the time needed to collect data, and to modify the questionnaire accordingly. The training was given to data collectors and supervisors for one day on data collection tools. A brief introductory orientation was given to the study participants by data collectors about the purposes of the study. Data double entry was done to make comparisons between two data clerks, and some difference was resolved.
Ethical Approval
Ethical approval was obtained from the Institutional Health Research Ethics Review Committee of Haramaya University, College of Health and Medical Sciences. Support letters from the College of Health and Medical Sciences were submitted to the selected Hospitals where the study was conducted. After getting all permission letters from the responsible body, and informed voluntary, written, consent was signed by study participants. Confidentiality was maintained by using codes instead of the participant's name. Participants were also informed that they have full right to refuse participation or withdraw at any time from the research.
Statistical Analysis
The collected data were checked for completeness and cleaned before entry into a computer. Then the questionnaire was coded and data were entered into Epi data version 3.1 by two data clerks who were recruited. Then the data were exported to SPSS version 22 for further data cleaning and analysis. Frequency was run to check for any missing values and checked accordingly. for analysis of the outcome variable, practicing level of CBT, the value above the mean was coded as “1” and below the mean was coded as “0.” The independent variables, knowledge level of the respondent value mean and above was coded as “1” and below the mean was coded as “0,” the attitude of the respondent the value mean and above was coded as “1” and below the mean was coded as “0.” To know whether there is an association between the outcome variable and each independent variable, bivariate and multivariate regression analysis was used at a p-value of .05. Variables that yield a p-value of <.25 in bivariate analysis were considered to be a candidate for multivariable logistic regression analysis to control all possible confounders and to detect true predictors of nurses’ practicing a level of CBT.
The model goodness-of-fit was tested by the Omnibus test and Hosmer–Lemeshow statistical test. The model was a good fit since it is found to be insignificant for Hosmer–Lemeshow statistic (p = .632) and significant for Omnibus tests (p = .001) The multicollinearity test was carried out to observe the linear relationships between independent variables using VIF and standard error. The finding indicated that there was no multicollinearity (VIF of >12 and standard error > 2.7). The direction and strength of statistical association were measured by the odds ratio with 95% confidence interval (CI). The adjusted odds ratio (AOR) along with 95% CI was estimated to identify factors for practicing a level of CBT by using multivariate analysis in the binary logistic regression. In this study, p-value <.05 was considered to declare a result as a statistically significant association.
Results
Sample Characteristics
A total of 390 study participants were involved in this study making the response rate 96.3%. Among the respondents, 204 (52.3%) were female. Nearly two-thirds of 257(65.9%) nurses were in the age group between 20 and 29 years. More than half 246 (63.1%) of nurses had working experience of five and below years. Regarding ward distribution of the respondents, 145 (37.2%) were working in the medical and surgical wards (Table 1).
Sociodemographic Characteristics of Nurses Working in Public Hospitals of the Harari Region and Dire Dawa City Administration, Eastern Ethiopia, 2018 (n = 390).

Catholic, Waqefeta, Adventist
Divorced, widowed.
Knowledge of Nurses About Pain Relief Methods
Among study participants, 324 (83.1%) of them knew that asking the patient to suggest ways to relieve his/her pain increases the patient's ability to manage pain. Three hundred eighteen (81.5%) of them knew that providing a suitable room temperature and good air conditioning can alleviate pain, and 313 (80.3%) of them knew that including family members in the pain management regimen increase patients’ ability to manage pain. More than half 228 (58.8%) of the participants had adequate knowledge about pain relief methods, and 162 (41.5%) of them had inadequate knowledge (Table 2).
Knowledge About Pain Relief Methods Among Nurses Working in Public Hospitals of Eastern Ethiopia, 2018 (n = 390).

The Attitude of Nurses Toward Pain Management Methods
In this study, 51 (13.1%) of nurses strongly agreed that pain relief therapies should be given to sick people, while 68 (17.4%) of nurses strongly disagreed that pain relief therapies should be given to sick people. About 185 (47.4%) of nurses agreed on their willingness to encourage patients to think about pleasant and positive matters when he/she feels pain while 184 (47.2%) agreed on their willingness to provide information on an issue related to nonpharmacological pain management methods to sick people. Furthermore, 182 (46.7%) of nurses agreed on nonpharmacological therapy should be given to sick people.
In this study, 21.3% of nurses strongly agreed on carefully preparing the patient for the procedure by informing him/her about what will be done can increase patients’ ability to manage pain. Additionally, 67 (17.2%) of nurses strongly agreed on encouraging the patient to relax different parts of his/her body can alleviate the sensation of pain.
More than half of the 390 participants, 233 (59.7%), had a positive attitude toward nonpharmacological pain management practice, while the remaining 157 (40.3%) had a negative attitude (Table 3).
Attitude on Pain Management Methods Among Nurses Working in Public Hospitals of Eastern Ethiopia, 2018.

NB: Strongly disagree (SD), Disagree (DA), No comment (NC), Agree (AG), strongly agree (SA). Frequency (percent).
Health Care System and Patient-Related Factors
Among the study's participants, 201 (51.5%) nurses reported receiving pain relief training. More than half 256 (65.6%) of nurses reported the presence of pain management guidelines. This study finds that 253 (64.9%) nurses had a workload. The majority of nurses, 284 (72.8%), provide pain management for stable patients, and 213 (54.6%) report that patients are willing to use nonpharmacological pain management methods such as CBT.
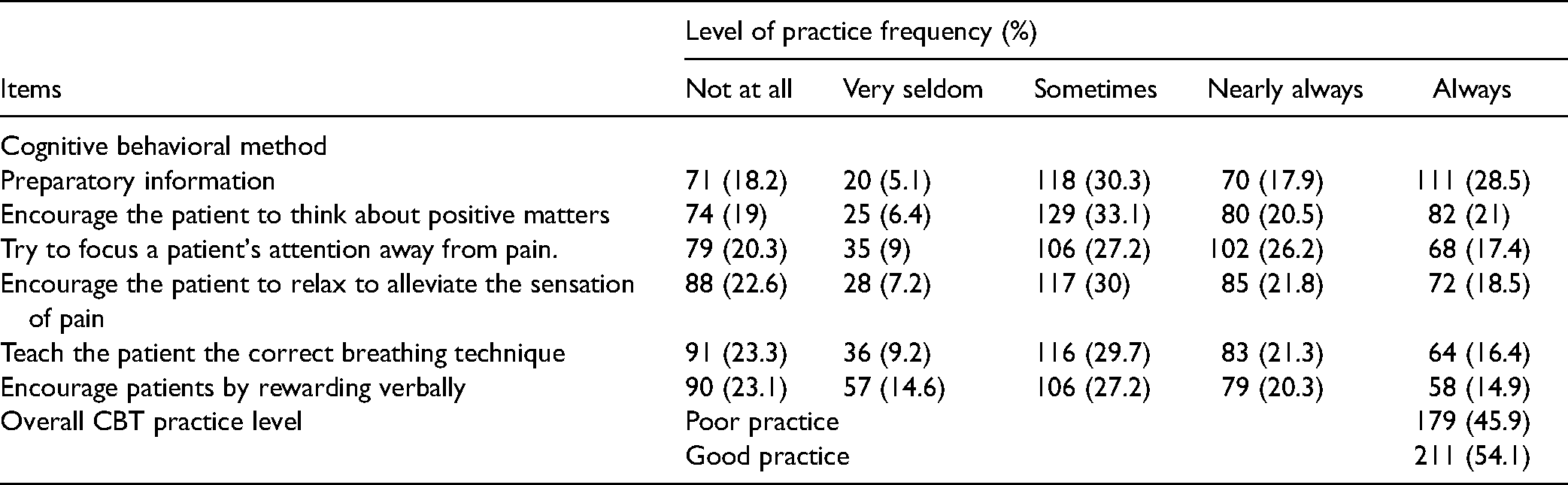
Practicing Level of CBT Methods
About 111 (28.5%) of nurses provide the patient the preparatory information and 82 (21%) of nurses encouraged the patient to think about pleasant/positive things when the patient is in pain. Out of 390 participants, 211 (54.1%) had good cognitive behavioral methods practice, with a mean value of 18.6 (7.36SD) and a minimum and a maximum score of 6 and 30, respectively (Table 4).
Cognitive Behavioral Method Practice of Nurses Working in Public Hospitals of Eastern Ethiopia, 2018.
Factors Associated with CBT Practice of Nurses
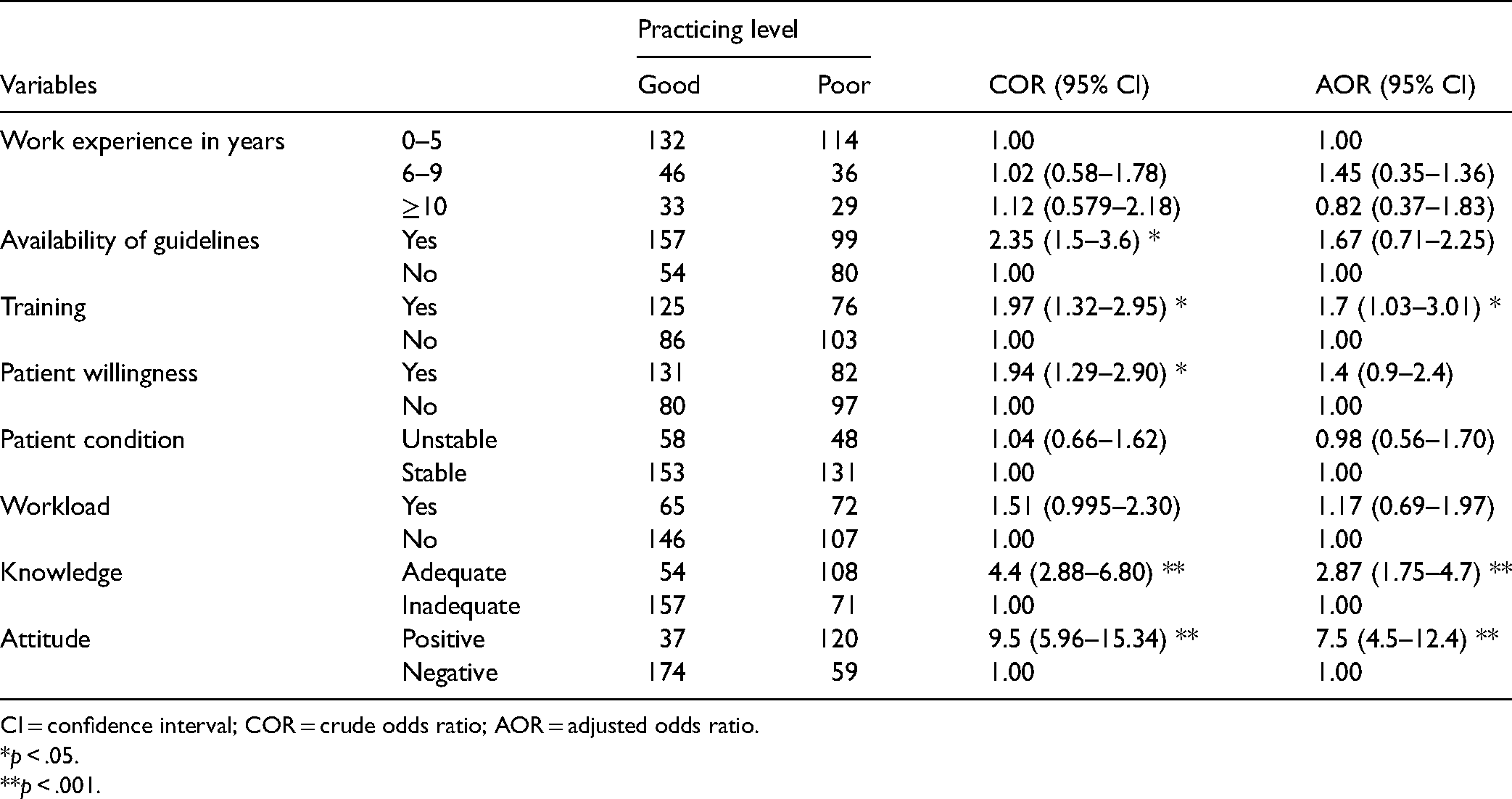
In bivariate analysis, the availability of guidelines had training, patients’ willingness, nurses’ attitude, and knowledge was significantly associated with CBT practicing level. But, in the multivariable logistic regression, nurses who had training, nurses’ attitude, and knowledge were significantly associated with CBT practicing level.
The odds of good practice of CBT were 2.87 times higher among nurses with adequate knowledge of pain relief methods than those nurses with inadequate knowledge (AOR 2.664; 95% CI: 1.75, 4.7). Nurses who received pain relief training were 1.7 times more likely than their counterparts to use CBT pain management (AOR 1.7; 95% CI: 1.03, 3.01). The likelihood of good CBT practice was 7.5 times greater among nurses with a positive attitude than among nurses with a negative attitude (AOR 4.02; 95% CI: 4.5, 12.4) (Table 5).
Factors Associated with CBT Practice Among Nurses Working in Public Hospitals of Eastern Ethiopia, 2018.
CI = confidence interval; COR = crude odds ratio; AOR = adjusted odds ratio.
*p < .05.
**p < .001.
Discussion
Cognitive behavioral pain relief methods are recognized as the best nonpharmacologic pain relief method. However, it is not practiced well in the study area. Thus, the study aimed at assessing nurses’ knowledge and practicing level of cognitive behavioral pain relief methods in public hospitals of eastern Ethiopia. Nurses who had a positive attitude toward nonpharmacological pain management including CBT, nurses who had adequate knowledge of nonpharmacological pain management including CBT, and nurses who had training were significantly associated with outcome variables.
This study found that 54.1% (95% CI: 48.5–59.2) of the respondent had a good CBT practice level. This result is lower than the study done in Saud Arabia 65% (Ali et al., 2013). The possible explanation may be linked to the fact that high patient flow in public hospitals. It also could be due to the difference in the level of knowledge and attitude of nurses toward pain relief methods. The finding of this study implied that low practicing level of CBT compared with other studies. And there need to enhance nurses’ practice of CBT by formulating different strategies including increasing knowledge levels and improving the attitude of nurses toward pain. Evidence indicated that CBT is cost-effective in treating chronic pain and needs to increase its practice (Lamb et al., 2010). This finding is also higher than a study done in the USA with the practice of CBT was 12.7% (Beissner et al., 2009). A possible explanation may be the difference in sample size and socioeconomic status of the countries.
The finding from this study shows that 58.8% (95% CI: 53.8–63.9) of the nurses had adequate knowledge about pain relief methods. This finding is higher than the study done in the Amhara region 54.2% (Tekletsadik et al., 2021) and the Benishangul Gumuz region 51.2% (Jira et al., 2020). One possible explanation is that the current study has a larger sample size than those studies. The other possible explanation is related to study settings; this study was conducted in multicenter hospitals, whereas the others were conducted in single institutions. The other possibility is that study participants’ sociodemographic characteristics differ. This indicated that concerned bodies should work on strategies such as short-term and long-term training that increase the knowledge level of the nurses which inversely increases the practice of CBT.
This study found that nurses who had a positive attitude toward nonpharmacological pain management including CBT were more likely to practice CBT than nurses with a negative attitude about it. This may be due to the reasons that as nurses develop a positive attitude; they tend to be more likely to practice CBT. This is supported by a study done in Malaysia (Alzghoul et al. 2016), and the Tigray region, North Ethiopia (Ermias et al., 2017). This finding reviled that improving the attitude of nurses can have a significant improvement in the practice of CBT.
According to the findings of this study, nurses with adequate knowledge of nonpharmacological pain management, including CBT, were three times more likely to use it than nurses with inadequate knowledge. This is consistent with the findings of a study conducted at Al Mansoura University, which found a positive relationship between nursing staff knowledge and the practice of nonpharmacological methods (Ali et al., 2013). This could be because good knowledge boosts nurses’ confidence and readiness to perform their routine tasks.
According to this study, nurses who received training were 1.9 times more likely to use CBT than nurses who did not. One possible explanation is that those who had received training had sufficient knowledge and skill to provide CBT. This is supported by various studies (Coker, E., et al., 2010, He, H.-G., et al., 2010, Rantala, M., et al., 2012, Zeleke et al., 2021) that found that one of the nurses’ barriers to providing CBT and other nonpharmacologic pain relief techniques was a lack of training.
Strength and Limitation of the Study
The use of higher sample was the strength of this study. The questionnaire was prone to social desirability bias; because no one wants to expose one inability. The study was done with a cross-sectional study design, so it has an effect of temporal ambiguity.
Implication for Practice
The finding of this study implied that it is important to increase the practice of CBT among nurses by improving their knowledge and attitude. This has implications for clinical practice in improving the practicing level of nurses and helping patients to control their pain.
Conclusion
The study revealed that more than half of nurses had a good practice level of the CBT pain management method. Having a positive attitude, being knowledgeable, and having training were significantly associated with the nurses’ practicing level of CBT. Enhancing educational opportunities and facilitating short-term and long-term training could avert the poor practicing level of CBT.
Footnotes
Acknowledgments
The authors would like to extend our deepest thanks to Haramaya University, College of Health and Medical Science staff for providing their constructive support.
Author Contributions
HK conceived the idea, reviewed data, drafting, and editing of the manuscript. KT, AE, AD, and NA work on proposal writing, project administration, methodology, data analysis, and result writing. AE, TG, NA, SH, ADW, and AD contributed to data management, data review, and data analysis. KT, HK, SH, ADW, and AE contributed to reviewing the result, manuscript preparation, and revision of the manuscript. Finally, all authors read and approved the final version of the manuscript to be published and agreed on all aspects of this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.