
Abstract
Background
The COVID-19 pandemic significantly impacted emergency department (ED) operations and patient care. Understanding its effects on nursing processes, triage accuracy, and wait times is pivotal for optimizing outcomes.
Objectives
This study aimed to analyze the differences in nursing processes, triage accuracy, and wait times before and during the COVID-19 pandemic.
Design
A retrospective cohort study.
Methods
The study analyzed 224 electronic medical records from a single ED, with 120 records from the pre-pandemic period (January 2019–February 2020) and 104 records from the pandemic period (March 2020–March 2021). Dependent variables included missed nursing care per validated scales, triage accuracy per Emergency Severity Index, and wait times for nursing triage and physician examination. Independent factors encompassed sociodemographic, clinical characteristics, and organization dynamics.
Results
Sociodemographic and clinical profiles were comparable between periods. Triage accuracy remained high except for older patients. Nursing triage wait times differed little, yet physician examination and urgent case waits decreased amidst the pandemic. Nursing documentation completeness, such as recording patient status and mental state, augmented during this crisis period.
Conclusion
This evaluation identified differences in triage accuracy, wait times, and documentation completeness before and during the COVID-19 pandemic period at a single institution. Patient age and clinical status influenced some metrics. Lessons from comparing precrisis benchmarks to intra-pandemic nursing performance may guide pandemic preparedness strategies. Further research is warranted to optimize emergency processes and outcomes during public health emergencies, as well as examine strategies through multicenter investigations comparing prepandemic to intra-pandemic performance to provide broader insights into challenges and inform efforts to bolster emergency care through future crises.
Introduction
The emergency department (ED) is a critical component of acute care hospitals, providing immediate and potentially life-saving care for patients who present with acute conditions or worsening chronic conditions. The ED is staffed around the clock by skilled professionals, operating 24/7 to meet the community's urgent and emergent care needs (Wang et al., 2020a). When patients arrive at the ED, they undergo an initial triage assessment to determine priority of care. Traditionally, this process begins with a nurse-conducted triage to obtain key information rapidly from the patient. During triage, the nurse evaluates the presenting complaint, collects vital signs, reviews the medical history, and assesses symptom severity. Using this initial data, the nurse then assigns an acuity level for the patient via a standardized triage scale. The triage process provides a prioritization of patients based on medical need upon arrival to the ED (Oredsson et al., 2011). Accurate and timely triage is crucial, as it directly impacts patient flow, resource allocation, wait times and clinical outcomes (Cameron et al., 2017; Weber, 2019).
Beyond the initial triage, the ED nursing role encompasses ongoing reassessments, administration of treatments, coordination of diagnostics such as labs and imaging, patient advocacy, and communication with physicians (Brosinski et al., 2017; Craig et al., 2016). Nurses play a pivotal role in monitoring for clinical deterioration, ensuring patients’ physical and emotional needs are met, and facilitating smooth transitions of care. However, ED nurses face numerous challenges in delivering optimal care due to issues such as overcrowding, staffing shortages, and limited resources that can lead to missed nursing care (Ding et al., 2019; van der Linden et al., 2016) The emergence of the COVID-19 pandemic in early 2020 significantly impacted and overwhelmed healthcare systems worldwide (Quah et al., 2020). EDs found themselves on the frontlines, managing surging patient volumes including those under investigation for COVID-19. Changes were necessitated in processes, infrastructure, availability of resources, and staffing models to minimize virus transmission while sustaining operations (Quah et al., 2020; Ross, 2020).
Review of Literature
During the COVID-19 pandemic, EDs faced unique challenges, including increased patient load and adaptations of the triage protocols to the new reality. Many acute care hospitals around the world, including Israel, established dedicated emergency facilities for COVID-19 patients with specifically trained medical teams (Quah et al., 2020; Silvagni et al., 2020; Wang et al., 2020b). While these changes were necessary to prevent the spread of the virus and alleviate public fear of contracting the virus in the ED, they placed an additional psychological burden on the already overworked nursing staff. The need to wear personal protective equipment also resulted in physical exhaustion and dehydration, and the requirement to guarantee physical isolation meant that nurses had to maintain constant vigilance regarding infection control procedures (Quah et al., 2020). Despite these difficulties, nurses embraced these challenges and demonstrated critical thinking and creativity in addressing new problems in the healthcare system (Jose et al., 2020).
The organizational changes implemented to manage the effects of the COVID-19 pandemic did not entirely prevent negative impacts on nursing care management, including cases of missed diagnoses and treatment delays for non-COVID-19 patients due to the higher workload and the need to focus on identifying COVID-19 patients.
Relationship Between Age and Outcomes
Several previous studies have found an association between patient age and factors related to ED care. A study of based on CUREd Research Database found older age was significantly correlated with longer wait times for initial assessment and treatment (Maynou et al., 2023). Delays in care for elderly patients have been linked to poorer health outcomes, such as increased risk of hospitalization and mortality (Jones et al., 2008). Research also suggests age can impact the quality of nursing care received. A lack of comprehensive assessments may lead to missed care needs among elderly patients (Gettel et al., 2022). Additionally, cognitive impairment and communication barriers associated with aging can pose challenges for nurses performing accurate triage (Dahlke et al., 2023). This highlights the importance of examining whether age influences triage accuracy, as our study proposes to analyze.
Relationship Between Wait Times and Outcomes
Prolonged wait times in the ED have been tied to negative consequences, such as leaving without being seen, complications, and lower patient satisfaction (Forero et al., 2010, 2019). Given the consequences of delays, it is prudent to evaluate whether wait times changed during the pressures of the COVID-19 pandemic compared to usual operations. Understanding potential drivers of wait time variations could point to opportunities to enhance efficiency and quality of care. To the best of our knowledge, only a few studies have examined “real life” nursing care management during the COVID-19 pandemic (Quah et al., 2020; Silvagni et al., 2020).
Specifically, the objectives are as follows:
Compare triage accuracy, mean waiting times, and completeness of nursing documentation in the ED before versus during the COVID-19 pandemic period. Determine the influence of patient characteristics (age, gender), clinical factors, and organizational elements on triage accuracy and waiting times. Identify associations between completeness of nursing assessment documentation and patient/clinical characteristics to understand populations more vulnerable to missed care elements.
Methods
Theoretical Framework
This study was grounded in systems theory, which views healthcare delivery organizations like EDs as complex adaptive systems (Clancy et al., 2008). In a systems theory framework, the ED comprises interdependent components including patient characteristics (inputs), clinical care processes (throughputs), and patient outcomes (outputs). These system elements continuously interact and adapt in response to changes in environmental factors (Williams, 2001).
Study Design
This was a retrospective cohort study utilizing electronic medical record (EMR) data collected during routine care before and during the COVID-19 pandemic period in a medium-sized academic medical center. The inclusion criteria were as follows: all patients aged 18 and above who visited the general emergency department at the hospital during the study period. The exclusion criteria were patients who bypassed the triage stage and were directly admitted to the trauma room.
Study Sample
EMR data from 120 patients seen in the prepandemic period (January 2019–February 2020) and 104 patients during the pandemic (March 2020–March 2021) were retrospectively reviewed. Data included demographic information, triage level assigned, length of stay, and vital signs recorded in the EMR. To maintain random sampling, EMR selection occurred on 10 random dates between March and May 2020 and 10 random dates in 2019. Within each date, five EMRs were randomly selected at different times between 8 am and 8 pm to avoid selection bias. EMRs of patients under 18 or those bypassing triage due to emergent conditions were excluded.
Data Collection
Dependent Variables
Missed Nursing Care. To evaluate the completeness of nursing care, two tools were utilized:
1. The Nursing Assessment Questionnaire was developed by the research team specifically for this study to evaluate the quality of nursing assessments. Key components of nursing assessments were identified based on a literature review and input from nursing experts. The items in the questionnaire addressed critical elements of patient assessment including visible injury, need for assistance, mental status, and physical condition (see Appendix 1).
The questionnaire was piloted on a sample of nursing assessments (n = 30) to establish face and content validity. Minor revisions were made based on feedback. Interrater reliability was tested on a subset of 20 assessments, demonstrating good agreement (κ = 0.80) between two independent raters.
The final Nursing Assessment Questionnaire contains 10 items, each scored 0 or 1 depending on performance or nonperformance of the assessment component. An average score out of 10 indicates the overall completeness of the nursing assessment, with higher scores reflecting more thorough documentation of important assessment findings.
2. The Nursing Care Quality and Safety Assessment Questionnaire is based on the questionnaire compiled by Kalisch and consists of the following five statements: patient identification, drug sensitivity review, vital signs assessment, reevaluation of the patient according to their condition, and whether the anamnesis refers to an existing comorbidity (Kalisch & Williams, 2009). Each statement receives a score of 1 or 0 depending on the performance or nonperformance of the statement (see Appendix 2).
The average score ranges from 0 to 5. Validation of both questionnaires was performed by ED registered nurses working in other acute care hospitals. Minor changes were made to the wording of some items.
Triage Accuracy. This was defined as the degree of matching between the nurses’ urgency ratings and the actual waiting times for triage (Sanders & DeVon, 2016). The Emergency Severity Index (ESI) scale rates the level of urgency (P = priority) from 1 to 5 according to the professional guidelines for rating clinical urgency and the number of resources the patient will need during their stay. The ESI defines the maximal waiting time that a patient can wait for nurse triage admission: 0, 15, 30, 60, and 120 min for urgency levels 1, 2, 3, 4, and 5, respectively (Mirhaghi et al., 2015)
Waiting Times. The two time intervals measured in this study were those regularly measured in ED as part of a national measurement scheme: (1) the length of time from the patient entering the ED until being admitted by the triage nurse, and (2) the length of time from the patient's admission by the triage nurse to seeing a physician (Hinson et al., 2019).
Independent Variables
Socio-demographic variables: Age and Gender
Clinical variables: (1) The reason for the current referral to the ED: Referral reasons were grouped into the following clinical categories: cardiovascular, pulmonary, gastrointestinal, musculoskeletal, neurology, endocrinology, urology and gynecology, otorhinolaryngology and ophthalmology, poisonings, and allergies; and (B). Co-morbidities including diabetes, hypertension, or cardiovascular diseases.
Organizational variables: The type of nursing shift (morning, evening, night) when the patient was admitted to the ED and the number of patients admitted to the ED during this shift.
Patient condition: This was based on a nurse's assessment and included physical or mental disability, use of assistive devices, and mental condition (restlessness and visible injury). It is a dichotomous variable, with each of the four components attributed a value of 1 (positive answer) or 0 (negative answer) with the overall assessment ranging from 0 to 5. This variable is examined as a possible confounder.
Sample Size Calculation
The sample size was calculated using the t-test in the MedCalc software at a 5% significance level and 80% power. A minimum sample of 200 patients was obtained.
Data Analysis
Descriptive statistical analyses were performed for ranges, means, median, and standard deviations for continuous variables, while frequencies and percentages were performed for categorical variables. We then explored the association between the independent and dependent variables using correlation tests (Spearman/Pearson), t-tests for independent samples and chi-square tests for categorical variables. Lastly, several regression models were performed: Linear regression was used to examine the variables that explained the completeness of nursing care and waiting times for diagnosis and treatment, while logistic regression was used to examine variables that explained triage accuracy.
The level of significance for all statistical analysis was 5%. The data analysis was performed using the Statistical Package for Health & Welfare Science for Windows (SPSS, version 28.0, Chicago, IL, USA).
Ethical Considerations
The study protocol was approved by the Institutional Ethics Committee of the University and the Institutional Helsinki Committee at the Medical Center. All procedures were performed according to the institutional and national research committee's ethical standards and complied with national ethical standards. Patient confidentiality and privacy were strictly maintained throughout the study. Electronic medical records were de-identified prior to data collection and analysis. Each record was assigned a unique identification number to allow for linkage while de-identifying protected health information. Access to records and data was limited only to authorized researchers involved in the study.
Results
Participants’ Sociodemographic and Clinical Characteristics
The study population included 56.7% women in the pre-COVID-19 period (“before”) and 50.0% post the COVID-19 period (“after”). The mean age of the sample was 58.4 and 61.7 years, before and after, respectively. The prevalence of chronic morbidity was not statistically different between the periods. More EMRs were sampled from the morning and evening, compared with night shifts, in both time periods. The distribution of the records sampled did not change significantly between the periods (Table 1).
Description of the Study Population.
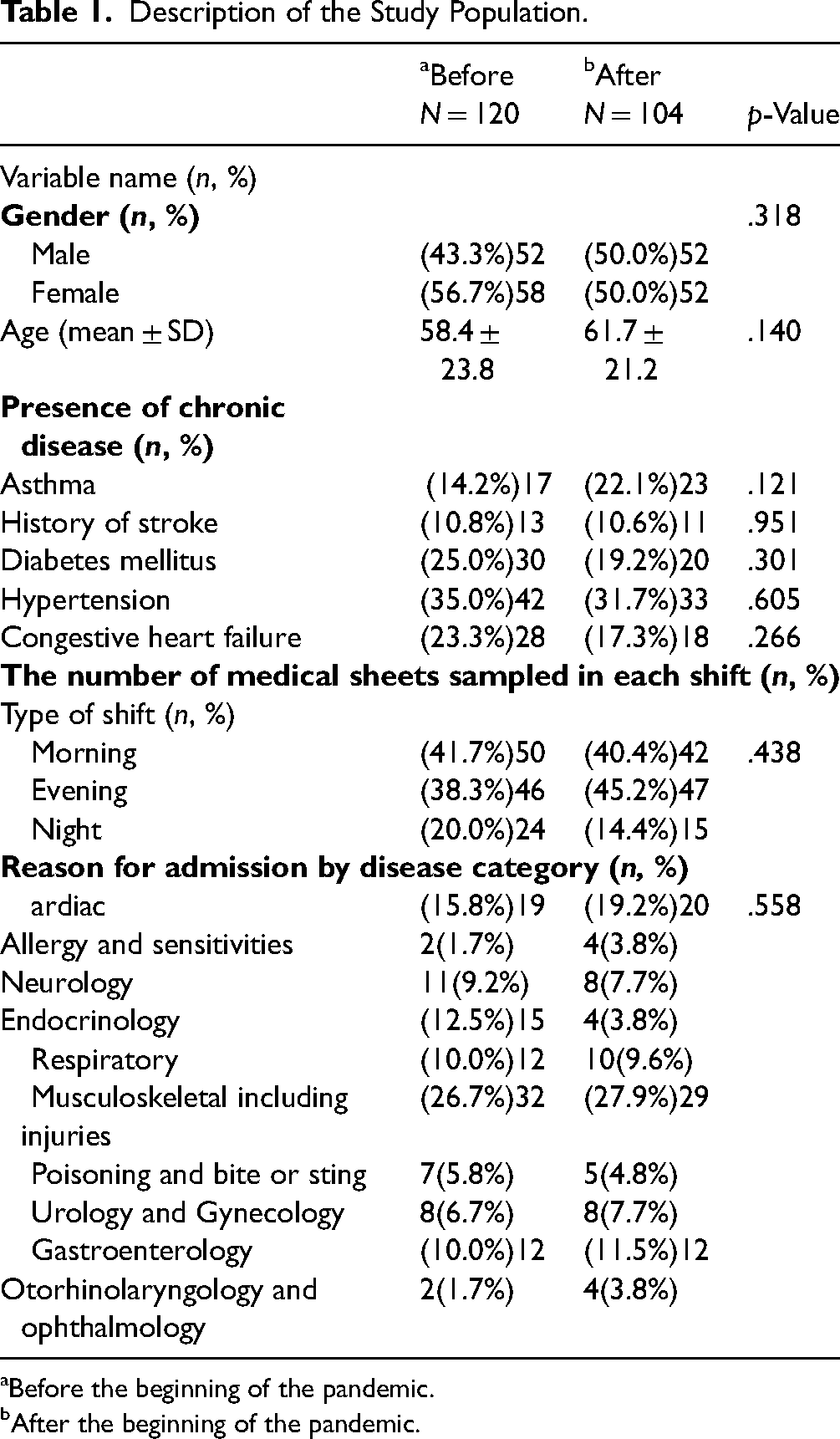
Before the beginning of the pandemic.
After the beginning of the pandemic.
The mean ESI urgency score was 2.9 and 3.1 (on a scale of 1–5) before and after the pandemic began, respectively. The most common urgency level was P3, with slightly more than half of the records reviewed in both study periods. P1 and P5 were the least common urgency scores in the study sample. The period did not have a statistically significant effect on the score distribution (Table 2).
Triage Accuracy, Before and After Covid-19.

Table 2 presents the proportions of ED patients assigned each Emergency Severity Index (ESI) triage level during the pre-pandemic and pandemic study periods. The ESI is a 5-level scale used to categorize patients based on acuity and resource needs. “P1” signifies the proportion of patients assigned ESI level 1, “P2” the proportion assigned level 2, and so on up to “P5” representing the proportion assigned ESI level 5.
Level of Triage Accuracy
It is defined as the degree of matching between the nurse's urgency rating and the actual waiting time for triage
Factors Affecting Nurses’ Accuracy in Performing Triage
The following parameters were examined: period (before and after the beginning of the pandemic), gender, age, and time from the patient's entry into the ED until triage initiation. The analysis showed that age was the only variable that has a statistically significant effect on nurses’ triage accuracy. A negative correlation was demonstrated between patient age and triage accuracy, that is, the younger the patient, the higher the accuracy in triage (OR = 0.950, p = .033) (Table 3).
Factors Contributing to the Nurses’ Accuracy in Triage, Using Logistic Regression.

Table 3 presents the results of a logistic regression analysis examining factors contributing to nurses’ triage accuracy.
Period: 1 = before the COVID-19 pandemic; Gender: 1: Male; 2: Female; Age and Time to triage were entered into the model as continuous variables.
S.E. = Standard error of the B coefficients; df = Degrees of freedom for each Wald statistic.
Waiting Times in the ED
The mean waiting time for nurse triage, as measured from admission to the ED to the initiation of triage, was measured almost unchanged between the two study periods: 5.94 and 6.02 min, before and after the pandemic began, respectively; p = .46 (not shown). However, a statistically significant 10 min shorter mean waiting time from triage to the initiation of physician's examination was found during the COVID-19 period compared to the period before the pandemic: 49.75 and 39.96 min, respectively; p = .03 (not shown).
Waiting Times According to the Urgency Score Given During Triage
Waiting times for nurse triage, at level P5, that is, among the least urgent patients, were extended by 5.2 min (relative difference 0f 39%) during the pandemic, compared with the prepandemic period. For patients defined as most urgent, that is, levels P1 and P2, waiting times were somewhat shortened. Waiting times for physician examination were extended by 55% (relative difference) in the most urgent (P1) cases, while the waiting times for urgency levels of P2, P4, and P5 were significantly shortened (p = .034) (Figure 1).
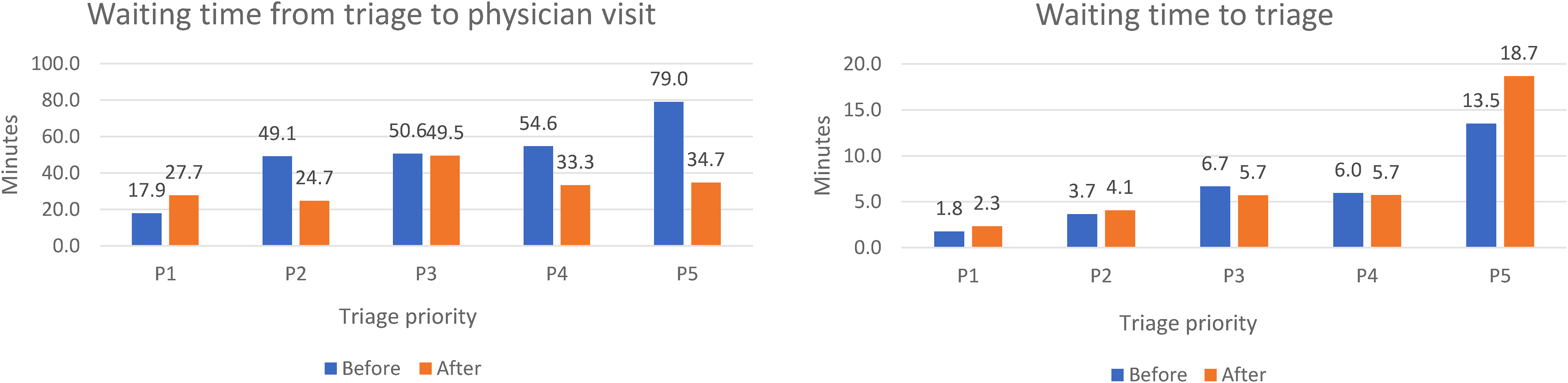
Waiting times in the ED (in minutes) according to the urgency score given during triage, before and after the pandemic began (n = 224).
Completeness of Nursing Care
Documentation of patients’ conditions requiring nursing assistance and patients’ mental status was significantly more frequent in the “after” compared to the “before” period. The mean score in the nursing assessment questionnaire was significantly higher in the “after” compared to the “before” period (3.78 and 3.33, respectively; Figure 2).

Completeness of nurse assessment, by period.
In both periods, patient identification, documentation of sensitivities, and documentation of vital signs were performed in 100% of the record-reviewed cases. Reassessment of patients’ conditions was slightly but insignificantly higher “before” compared with “after”, while documentation of background comorbidities was slightly higher “before”, compared with “after” (Figure 2). Comorbidities were documented in 95.8 and 94.8%, “before” and “after”, respectively (not shown). The mean score for the safety and quality questionnaire was slightly insignificantly higher “after” compared with “before”; 4.76 and 4.73, respectively.
Discussion
The study revealed that accurate ED triage was recorded in most of the cases both before and during the pandemic. Moreover, waiting times for nurse triage did not change during the pandemic compared to the prepandemic period. These findings suggest that the triage teams continued to perform efficiently and accurately even during the pandemic, with no significant impairments in triage accuracy or waiting times.
Among several variables examined, age was the only factor that influenced triage accuracy. Specifically, we found that older patients exhibited lower triage accuracy. These findings are consistent with a previous Israeli study that showed a negative correlation between patient age and nursing attention to patients, as well as between patient age and triage accuracy(Saban et al., 2021). These findings may be understood by the findings of a qualitative study conducted among nurses in medical wards in Iran; it found that factors like “age-unfriendly structure,” “inefficient care,” and “frailty of older adults” could increase the risk of missed nursing care among elderly patients. The authors suggested that high care needs, communication problems, and nursing care complexity contributed to missed nursing care (Rezaei-Shahsavarloo et al., 2021). The complexity of underlying diseases and diagnoses in older patients may also contribute to incorrect diagnoses and a decrease in treatment quality (Saif-Ur-Rahman et al., 2021). Additionally, most nursing and medical staff lack specialized training in treating geriatric patients, which can result in increased difficulty in treating older patients (Moloney et al., 2022). These factors collectively highlight the need for improved training and care practices when treating older patients (Van Wicklin, 2019). Moreover, a considerable proportion (57% to 86%) of ED physicians believe that elderly patients tend to require more time and resources from the staff than nonelderly patients, including clinical management challenges such as communication problems which may result in delayed treatment and adverse consequences. Consequently, medical staff may avoid tending to elderly patients in a timely manner which can exacerbate the problem (Ayalon & Tesch-Römer, 2018).
The current study found very short average waiting times from ED admission to nurse triage (approximately 6 min both before and during the pandemic). These times were both shorter than the national target (15 min) and the national average of all 27 acute care hospitals (8 min in 2021). The fact that these times did not lengthen during the COVID-19 pandemic may have been due to the hospital administration’s decision to flexibly assign staff where they were most needed during the peaks of the health crisis. For example, by diverting staff from considerably reduced elective hospital diagnostic and curative procedures and surgeries, to the ED and other wards that functioned under increased workload. Indeed, during the first wave of the COVID-19 pandemic, guidelines recommended postponing or scaling back all surgeries that were not considered urgent or time-sensitive (Wang et al., 2020b). A study in the New York City area found that the cessation of elective surgeries resulted in a 40% decrease in hospital admissions, which led to decreased overall volume of patients visiting EDs but those who did visit the ED were often sicker and required more intensive care (Richardson et al., 2020). Fear of contracting COVID-19 and public health messaging encouraging people to avoid seeking medical care for minor health concerns may have further contributed to a significant decrease in ED visits in the USA. Indeed, hospitals had to adapt their operations to prioritize COVID-19 patients and those with life-threatening conditions, resulting in longer wait times for patients who visited ED for nonurgent conditions. The pandemic also highlighted the importance of telemedicine in healthcare, which could be a game-changer for emergency care in the future (Saran et al., 2020).
Several studies and reports noted that the pandemic led to decreased ED visits for non-COVID-19 related conditions, possibly due to patient concerns about contracting the virus or a perception that healthcare resources should be reserved for COVID-19 patients (Martínsánchez et al., 2020). Indeed, at the national level, visits to the ED for all but obstetric reasons, considerably decreased during the first and second peaks of the pandemic with a maximal decrease in April, May, and October 2020, compared with the average volume in the parallel months in 2017–2019. The volume of admissions due to injuries, including motor vehicle accidents, also decreased considerably.
The current study found that during the COVID-19 pandemic, the waiting times for nurse triage in the least urgent cases was extended by 39%, while those for the more urgent cases were somewhat shortened. This might stem from the focus of nursing staff on more complicated and/or urgent patients. Accordingly, the direction of resources and staff towards care for the more urgent patients came at the expense of the less urgent population.
The current study's finding of a significant 20% decrease in waiting times to see a physician cannot be explained by a decreased patient volume since this volume remained constant before and during the pandemic. However, conversely to the waiting times for triage, the waiting times until a physician's examination were significantly longer for the most urgent cases and shorter for the less urgent cases. A possible explanation for this is that when a critically ill patient arrived at the ED, the medical team began taking care of him/her before opening the computerized medical sheet and thus created a falsely extended measured time. Another reason for delaying the opening of the computerized and extending the time before a physician's examination for urgent patients was the required use by staff of personal protective equipment (PPE), including removing it, and cleaning and disinfecting it after exposure to a suspected or confirmed corona patient (Aloweni et al., 2022). Indeed, a previous study found that the process of removing PPE took an average of 4.9 min, which may have contributed to longer turnaround times for patient care. Nevertheless, in our study overall waiting times for nurse triage were not extended and those for physician examination were shortened during the COVID-19 period, compared with the pre-COVID-19 period. These observed outcomes can be attributed to the effective implementation and swift adaptation of appropriate work processes by the triage nurses, tailored to the exigencies of the pandemic. Furthermore, it is plausible to surmise that the hospital management demonstrated administrative proficiency by efficiently managing resources and adapting their staff's deployment during the crisis (Tomas et al., 2015).
The current study's finding that for the least urgent patients there was a significant shortening of the waiting times for a physician's examination during the pandemic may be due to the medical staff being uncertain regarding the volume of patients that would be admitted to the ED. Therefore work processes were efficient, aiming to rapidly discharge nonurgent patients, continue their care in the community, and maintain staff capacity for the care of more critically-ill patients (Tyrrell et al., 2021). This is contrary to a previous study's findings which have found that patients with complex medical issues usually require more intensive treatment in the ED and those with less complex medical requirements may wait longer for a physician's examination. Longer waiting times are correlated with decreased care quality and overcrowding in the ED (Ataman & Sarıyer, 2021)
A study conducted in a US trauma center found that accurate triage that managed to classify patients according to condition severity allowed physicians to prevent the consequences of long waiting times (Sabry et al., 2023). It is therefore possible that in the current study, the fact that triage accuracy was not compromised during the pandemic, contributed to keep waiting times at a prepandemic level.
The current study found that the completeness of nursing care, measuring both nursing evaluation performance and care quality and safety, did not change significantly during the COVID-19 pandemic. This is in contrast to some previous studies, which found that the pandemic had a negative impact on nursing care in certain contexts. For example, a cross-sectional study conducted in a university hospital in Stockholm, Sweden, found that during the pandemic, basic nursing care was often overlooked in the intensive care unit (Falk et al., 2022). Another study conducted in the same hospital's cardiology department found that the quality and safety of nursing care were significantly worse during the first wave of the pandemic compared to before the outbreak (Nymark et al., 2022). Similarly, a study conducted in a hospital in Iran found that the completeness of nursing care deteriorated during the pandemic due to administrative and organizational factors, such as a lack of personnel and inadequate medical equipment (Dehghan-Nayeri et al., 2015). Conversely, a study of hospital nurses in the Philippines found a low rate of inadequate nursing care during the pandemic, especially in terms of patient monitoring However, the size of the hospital and the safety culture within it were found to be associated with inadequate nursing care. Therefore, larger hospitals experienced more missed care while better safety cultures were associated with less missed care (Labrague et al., 2022).
The current study demonstrated that nursing care management was not affected or even improved during the pandemic compared with the prepandemic period. It is possible that these findings were explained by an efficient response by the hospital (like many other acute care hospitals in Israel), such as the diversion of medical and nursing staff from less urgent facilities to the ED and to dedicated COVID-19 medical wards, and the opening of a designated COVID-19 ED, with guidelines to postpone or scale back all diversion of confirmed and suspected patients directly there, thus alleviating the pressure on the general (non-COVID-19) ED. Future research may help to identify the specific factors that contribute to improved nursing care during pandemics and other crises, as well as strategies for addressing the challenges that could arise.
Limitations
This study has several limitations. First, the study was conducted in one medical center which might limit the external generalizability of the findings. Second, various nursing procedures may have been overestimated, including the quality of care provided, due to nurses subjectively perceiving their actions as more favorable than they actually were, which may have been compounded by workload overload or insufficient prioritization of documentation. Conversely, where nurses delivered comprehensive care that was not adequately documented in the records, the evaluation of nursing care completeness may have been underestimated. A potential limitation is that the sample included a higher proportion of medical records from daytime emergency department visits compared to nighttime visits in both study periods. Though visits from all shifts were included, having more daytime than nighttime records could influence the comparisons if patient characteristics or presentations differ between day and night patients. Lastly, our study only examined records from the initial surge period of the COVID-19 pandemic and does not assess any potential longer-term impacts on ED nursing care processes or patient outcomes after the acute phase. The pandemic is still ongoing and its longer-term effects on ED operations, nursing workload, patient flow, and clinical outcomes remain unknown. Future research with data collected further out from the peak of the pandemic would be needed to explore any enduring changes. Additionally, our findings may have limited generalizability to EDs with different structures, staffing models, or patient populations.
Implications for Emergency Nursing
This study provides valuable insights for optimizing emergency nursing care and departmental operations during public health crises. By comparing key metrics before and during the COVID-19 pandemic, several implications for nursing practice emerge. The findings illustrate nurses’ critical role in rapidly adapting workflows to changing demands while maintaining aspects of standardized care, such as high triage accuracy. Reducing wait times for higher acuity patients demonstrates adaptability in prioritizing urgent needs amid constraints. These successes underscore the importance of standardized assessments and flexible innovation even under pressure. However, opportunities for strengthening specific documentation elements were also identified, such as incorporating additional assessments of mental status or comorbidities to enhance comprehensive care. Understanding factors enabling nursing flexibility, like virtual consultations or team-based triage, can further inform strategic planning. Most importantly, standardized practices, open communication, and willingness to transform models of care delivery were paramount in sustaining quality nursing support amid adversity. The lessons from this experience provide a roadmap for developing workforce capabilities through policies, education and optimized identified process areas to strengthen preparedness for future crises.
For emergency nurses, the overarching message is that standardized foundational skills paired with innovative adaptability are vital when navigating high-stakes environments with constrained resources. Applying these lessons has potential to not only improve patient outcomes but also boost nursing satisfaction in crisis conditions.
Conclusions
The results of this study may be useful as a platform for formulating recommendations for ED nursing staff management during future health crises. Future research could build upon these findings by evaluating the long-term effectiveness of such recommended strategies during health crises. Additionally, exploring the experiences and perspectives of the nursing staff could provide valuable insights for further enhancing ED operations and support mechanisms during challenging times. Ultimately, a comprehensive understanding of the impact of health crises on nursing staff and the implementation of evidence-based recommendations can contribute to the delivery of high-quality care and improved patient outcomes in emergency settings.
Supplemental Material
sj-docx-1-son-10.1177_23779608241274766 - Supplemental material for Comparing Emergency Nursing Measures Before and During COVID-19: A Retrospective Study of Assessment, Triage, and Workflow
Supplemental material, sj-docx-1-son-10.1177_23779608241274766 for Comparing Emergency Nursing Measures Before and During COVID-19: A Retrospective Study of Assessment, Triage, and Workflow by Nofar Misan, Rachel Wilf-Miron and Mor Saban in SAGE Open Nursing
Supplemental Material
sj-docx-2-son-10.1177_23779608241274766 - Supplemental material for Comparing Emergency Nursing Measures Before and During COVID-19: A Retrospective Study of Assessment, Triage, and Workflow
Supplemental material, sj-docx-2-son-10.1177_23779608241274766 for Comparing Emergency Nursing Measures Before and During COVID-19: A Retrospective Study of Assessment, Triage, and Workflow by Nofar Misan, Rachel Wilf-Miron and Mor Saban in SAGE Open Nursing
Footnotes
Author Contributions
NM conceptualized and designed the study, collected data, contributed to writing the first draft, and revised the manuscript and prepared some of the figures. MS conceptualized the study, performed analyses, prepared figures, provided insights on data interpretation, contributed to writing the first draft, and revised the manuscript. RWM conceptualized the study, provided insights on data interpretation, and reviewed and revised the manuscript for important intellectual content. All authors approved the final manuscript and agree to be accountable for all aspects of the work.
Availability of Data and Materials
The analyzed data will be made available to requesting researchers upon a reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement
The study protocol was approved by the Institutional Ethics Committee of the University (approval number: 1-0004699) and the Institutional Helsinki Committee at the Medical Center (confirmation number: 0067-21-LND). Informed consent was obtained from all the participants and/or their legal guardians.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.