
Abstract
Background
Clinical judgment is declining in new graduate nurses, which affects patient safety and is therefore tested on the Next Generation NCLEX. There is limited research describing barriers and facilitators impacting nursing faculty's experiences teaching clinical judgment.
Aims
The purpose of this study was to explore barriers and facilitators affecting undergraduate nursing faculty's clinical judgment teaching methods.
Methods
Sixteen qualitative interviews were conducted with full-time nursing faculty at seven universities in the Northeast and Southeast regions of the United States.
Results
The findings revealed program, student, and faculty factors affecting clinical judgment teaching methods. Subthemes included time, class size, students’ class preparation, critical thinking, task orientation, professional development, and faculty resistance.
Conclusion
Minimizing barriers and strengthening facilitators based on participants’ practices and previous research can support more effective clinical judgment pedagogy, which has the potential to achieve Next Generation NCLEX success and potentially increase patient safety.
Keywords
Background
Nursing faculty are tasked with teaching clinical judgment to nursing students to increase patient safety (Kavanagh & Sharpnack, 2021; National Council of State Boards of Nursing [NCSBN], 2018) and ensure nursing licensure exam success (Betts et al., 2019). However, clinical judgment is challenging to teach (Monagle et al., 2018) because according to Benner et al. (2009), clinical judgment relies on pattern recognition and intuition developed over years of experience. Therefore, an assumption can be made that barriers and facilitators exist when teaching clinical judgment to nursing students.
Clinical judgment is defined by Tanner (2006) as the “interpretation or conclusion about a patient's needs, concerns, or health problems, and/or the decision to take action (or not), use or modify standard approaches, or improvise new ones as deemed appropriate by the patient's response” (p. 204). Clinical judgment is complex because it occurs within the context of each patient's situation, the patient's unique responses, and the nurse's interactions with the patient. Clinical judgment is influenced by the nurse's professional knowledge, experience, values, and the healthcare environment (Tanner, 2006).
To support patient safety, teaching nursing students to recognize a patient's deteriorating status and intervene appropriately is a priority for faculty (Manetti, 2019). However, clinical judgment is declining among new graduate nurses (Kavanagh & Szweda, 2017), with less than 10% possessing safe clinical judgment skills (Kavanagh & Sharpnack, 2021). Forty percent of new graduate nurses fail to recognize a patient's urgent problem, and 50% fail to intervene appropriately (Kavanagh & Sharpnack, 2021). A practice analysis revealed clinical judgment is an essential skill for new graduate nurses (NCSBN, 2018). As a result of these studies, the NCSBN revised the nursing licensure exam, called the Next Generation NCLEX (NGN), to evaluate clinical judgment (Dickison et al., 2019).
To support the inclusion of clinical judgment in nursing curricula, clinical judgment is a required prelicensure concept in the American Association of Colleges of Nursing's (AACN, 2021) The Essentials: Core Competencies for Professional Nursing Education. Altmiller (2023) explained how faculty can map their competency-based curriculum, which includes threading clinical judgment throughout the nursing courses. Additionally, Sirianni et al. (2020) discussed the need for faculty development when implementing competency-based education, implying a professional development need for clinical judgment pedagogy.
Review of the Literature
Ongoing deficits in clinical judgment exist among new graduate nurses and experienced nurses as evidenced by lapses in assessment, situational awareness, cue recognition, problem identification, appropriate intervention, medication safety, and communication (Callihan et al., 2023; Lavoie & Clarke, 2022; Lavoie et al., 2020). While inadequate clinical judgment in nursing remains an ongoing challenge, particularly concerning is the role of insufficient clinical judgment in patient deterioration, untimely rapid response team activation, and failure to rescue leading to adverse patient outcomes (Al-Moteri et al., 2019; Burke et al., 2022; Jensen et al., 2022; Tilley & Spencer, 2020; Treacy & Stayt, 2019). However, new graduate nurses (Willman et al., 2021) and staff nurses (Monagle et al., 2024) have specifically described the problem of inadequate clinical judgment among new graduate nurses and the need for postgraduation training (Willman et al., 2020). Inadequate clinical judgment is a safety issue, particularly in healthcare facilities that are unable to provide extensive new graduate nurse training. In one study, new graduate nurses’ clinical judgment was noted starting at 10 to 12 months post hire in reflection journals (Monagle et al., 2018). New graduate nurses need clinical judgment training past an orientation period lasting only weeks.
Inadequate clinical judgment and safety concerns have brought calls for teaching and evaluating clinical judgment in nursing students and new graduate nurses (Bussard et al., 2024; Monagle et al., 2018; Nielsen et al., 2016). However, although clinical judgment teaching strategies such as case studies, simulation, questioning, concept maps, feedback, reflection, coaching (Nielsen et al., 2023), and in-class simulation (Klenke-Borgmann et al., 2021) have been described, insufficient research supports their effectiveness particularly on long-term transfer of learning (Calcagni et al., 2023; Gonzalez & Nielsen, 2023; Lavoie et al., 2019; Lee et al., 2020), prompting a need for more research-supported pedagogy (Cantrell et al., 2021; Poledna et al., 2022; Thirsk et al., 2022).
Due to ongoing challenges with inadequate clinical judgment, a question that must be raised is what barriers and facilitators faculty may face teaching clinical judgment. Although prior research was conducted on students’ and faculty's barriers and facilitators teaching critical thinking and clinical reasoning (van Wyngaarden et al., 2019; Wong & Kowitlawakul, 2020), no prior research was found revealing nursing faculty's experiences teaching clinical judgment.
Purpose
The purpose of this study was to explore barriers and facilitators experienced while prelicensure faculty were teaching clinical judgment. Exploring these factors could assist faculty in minimizing barriers and maximizing facilitators to improve clinical judgment teaching effectiveness. The findings were part of a larger study exploring faculty's clinical judgment teaching methods (Kerns, 2023). Barriers and facilitators emerged as an unexpected finding due to a broad, open-ended statement used as the first interview question.
Methods
Research Question
What are the barriers and facilitators nursing faculty experience when teaching clinical judgment to prelicensure nursing students?
Study Design
The study used the pragmatic qualitative research method (Merriam & Tisdell, 2016; Savin-Baden & Major, 2013) to address the research question. This method is appropriate when a practical practice problem in nursing education needs data to inform the research question. The pragmatic method uses an exploratory approach, in this study individual interviews, to collect data; an inductive coding process to analyze the data; and a descriptive, explanatory style to report the findings. Preexisting literature is then used to suggest a solution for that problem.
Study Setting
Seven universities in the Northeast and Southeast regions of the United States were selected based on their broad range of university classifications and because faculty website directories were readily accessible. Potential participants at these sites were sent a recruitment letter via email.
Study Population
The inclusion criteria were intentionally broad based on the assumption at the start of the study that barriers and facilitators might be affected by many factors particularly when teaching a relatively new, complex topic such as clinical judgment. Therefore, the inclusion criteria in this exploratory study were full-time or part-time faculty with a master's or doctorate regardless of years’ teaching experience. There were no exclusion criteria.
Data Collection
Participants were individually interviewed once via password-protected Internet-based video conference for a range of 50 min to 1 h and 40 min with an average of 1 hour each, for a grand total of 20 h. The first interview question indicated in Table 1 was intentionally broad for two reasons. First, when the study began it was unknown whether faculty were teaching clinical judgment since the NGN exam administration had not started, although the participants were informed the study was on clinical judgment. Second, starting with a broad statement avoided the possibility of obtaining biased data (Josselson, 2013). The researcher did not want to prompt the participants to say what they thought the researcher wanted to hear. As a result, participants shared the barriers and facilitators they experienced while teaching clinical judgment either after the first interview question or intermittently throughout the interview. After the initial interview question, the researcher focused the interview. Because this study was part of a larger study, the interview questions presented in Table 1 pertain to the findings of barriers and facilitators to teaching clinical judgment. Data collection took place from August 2022 through December 2022. Data saturation occurred at 16 participants when redundancy was noted during the interviews.
Semi-Structured Interview Protocol.

Data Analysis
Interviews were transcribed verbatim. Data were then manually coded by comparing the findings from each participant within each transcript and by comparing those findings with other participants’ transcripts, a process called constant comparison (Corbin & Strauss, 2015). Transcripts were coded using three steps. First, holistic coding (Saldaña, 2021) was used, where a participant's discussion about a barrier or facilitator was separated into a large section to aid analysis. Second, in vivo coding (Saldaña, 2021) was used, where quotations were extracted from the section as examples. Third, thematic coding (Saldaña, 2021) was used, where the participant's quotations were categorized by similarity under types of barriers and facilitators.
Trustworthiness was established using the four methods of credibility, applicability, dependability, and neutrality (Morse, 2015). First, to support credibility, maximum variance sampling was achieved by recruiting participants with diverse backgrounds which included years nursing; clinical specialty; degree; university type; courses taught; didactic, simulation, or clinical; teaching experience; race; and gender. A second, experienced qualitative researcher reviewed the transcripts, coding, and data analysis. The reviewer's analysis concurred with the authors. Member checking was used, and no participants requested changes to their transcripts. The interviewing techniques of summary and clarification were used to test the researcher's emerging interpretations. Journaling was used throughout the study for reflexivity. A rich, thick description was generated through 600 pages of transcripts and extensive use of in vivo codes. Second, to support applicability, site and participant data are provided in Table 2 (Merriam & Tisdell, 2016).
Site and Participant Characteristics.
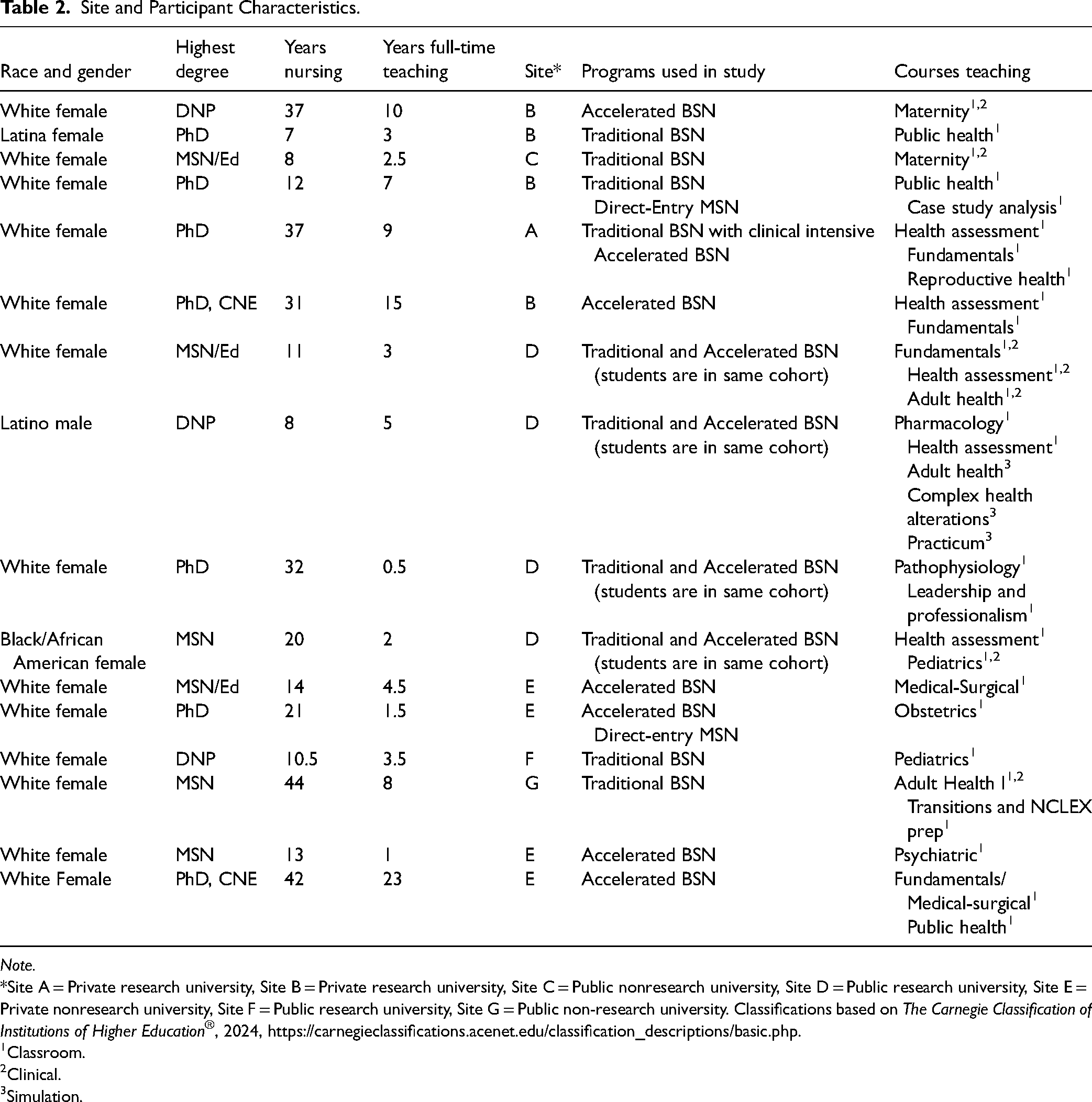
Note.
*Site A = Private research university, Site B = Private research university, Site C = Public nonresearch university, Site D = Public research university, Site E = Private nonresearch university, Site F = Public research university, Site G = Public non-research university. Classifications based on The Carnegie Classification of Institutions of Higher Education®, 2024, https://carnegieclassifications.acenet.edu/classification_descriptions/basic.php.
Classroom.
Clinical.
Simulation.
Third, the dependability of the study was maintained using analytic memos throughout the interviewing, coding, and data analysis processes to monitor for researcher bias and decision-making. Bias was minimized through the extensive use of in vivo codes (Creswell & Creswell, 2022). Fourth, to support neutrality all data were analyzed which revealed diverse participant experiences (Marshall et al., 2022).
Ethical Considerations
Institutional Review Board approval was obtained from the parent institution and each participant site. Informed consent forms were signed by voluntary participants who responded to the recruitment letter email. Participant and site confidentiality and anonymity were maintained.
Results
Study Sites
Two sites were private research universities, one site was a private nonresearch university, two were public research universities, and two were public nonresearch universities. Programs included five traditional Bachelor of Science in Nursing (BSN), one traditional BSN with a clinical intensive, four accelerated BSN, and two direct-entry Master of Science in Nursing (MSN). Four sites had more than one program type. Courses faculty taught included all core BSN courses: Health Assessment, Pathophysiology, Fundamentals, Medical/Surgical, Maternity, Pediatrics, Psychiatric, Public Health, Leadership, and an NCLEX preparation course.
Study Participants
A convenience sample of 16 full-time participants who taught classroom, simulation, and clinical courses were selected based on participants’ voluntary responses to the emailed recruitment letter. Participants had 0.5 to 23 years’ teaching experience and 7 to 44 years’ nursing experience. Participants represented nursing degrees earned from MSN, Doctor of Nursing Practice (DNP), and PhD programs. Two participants, both with a PhD, were Certified Nurse Educators. See Table 2.
Themes 1 and 2: Barriers and Facilitators
Two themes, barriers and facilitators, affected participants’ clinical judgment pedagogy. In many situations the facilitators were the faculty's method to alleviate barriers. Therefore, barriers and facilitators are addressed together under the program, student, and faculty subthemes. However, some barriers seemed insurmountable by participants although they were addressed in the literature (see Table 3).
Summary of Findings.
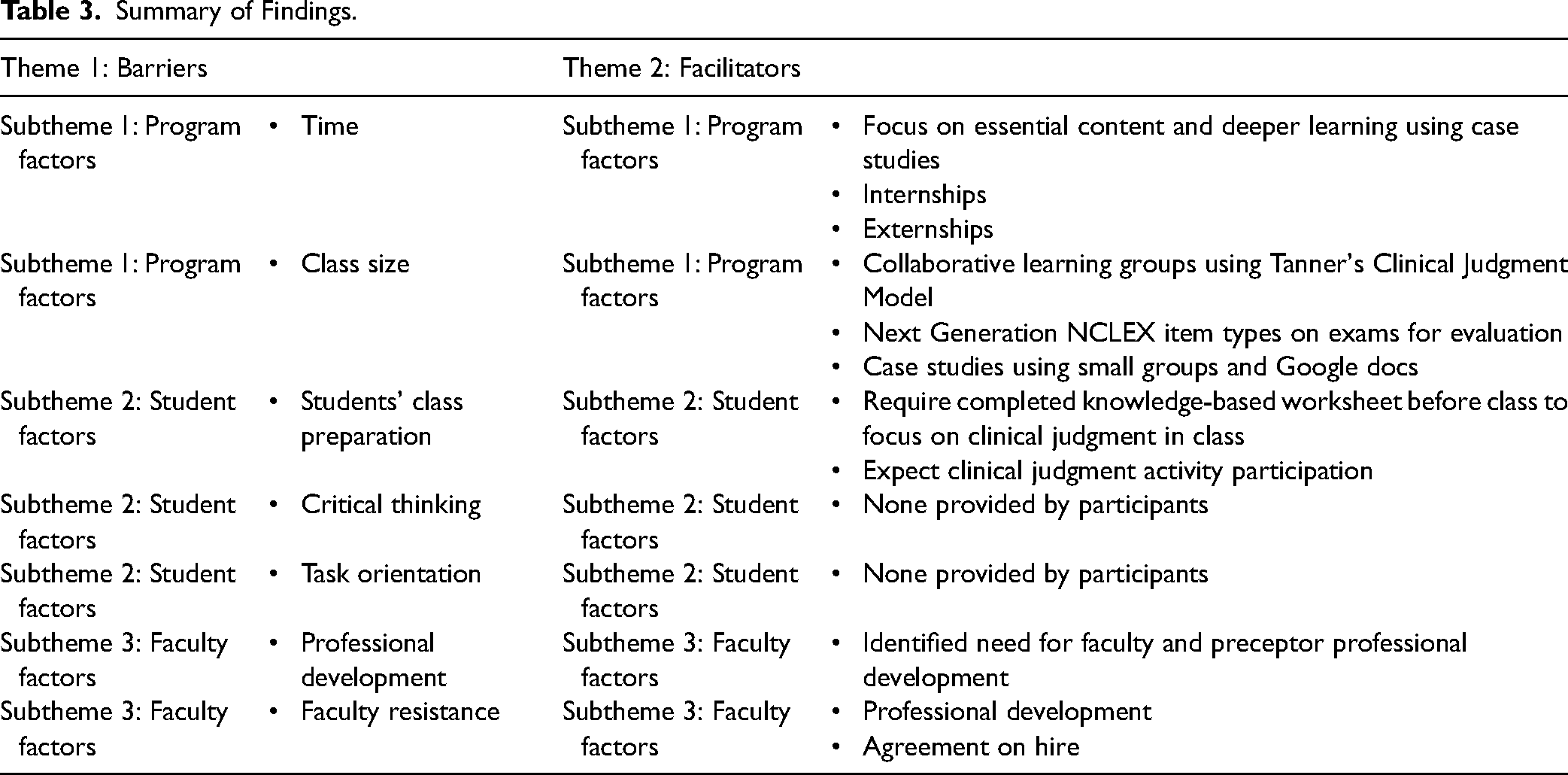
Subtheme 1: Program Factors
Time was a barrier particularly in accelerated BSN programs with shortened semester and program lengths because teaching and learning clinical judgment takes time. One participant who taught in an accelerated BSN program for second degree students who had work experience explained, “I am very clear with my students that this is a year they need to set aside to study and it is almost impossible to work while they are in the program. Due to decreased class time, I focus only on essential content and try to go deeper into case studies. Most clinicals are medical-surgical rather than specialty areas.” One program either required or encouraged a nurse externship and internship while the students were in school, thereby relying on healthcare experience outside of class and clinical to help develop clinical judgment. Study participants’ feedback regarding how helpful these additional experiences were in building clinical judgment was not equally enthusiastic, however. One participant explained she was unable to determine whether the externship or other factors, such as some students’ being “exceptional,” made the difference.
Class size consisting of nearly 150 students in some traditional BSN programs made teaching and evaluating clinical judgment challenging. Several participants explained the barriers they faced and ways to facilitate learning clinical judgment. The first participant broke students into collaborative learning groups of six students each and asked students to help each another understand the four cognitive processes of clinical judgment using Tanner's Clinical Judgment Model as a guide during an unfolding case study (Tanner, 2006). A second participant had students answer case studies with embedded questions and open text responses on Google docs projected on the projector screen so all students could see and share their answers.
Evaluating clinical judgment in a large class was also a concern. Due to grading load concerns, some participants stated they were unable to grade essay-like responses from homework. One participant's concern was how to evaluate clinical judgment in class because she did not want to merely rely on exams. She used a class polling system because it was fast and gave her an overall picture of student responses, but not every student answered the polls. Also, polls were limited to using multiple choice, select all that apply, one-word answer, or short phrase. In contrast, another participant explained she evaluated clinical judgment mainly on exams due to her large class size. Some faculty were uncertain how they could adequately evaluate clinical judgment in clinical, although others felt confident doing so by coaching and questioning students individually.
Subtheme 2: Student Factors
Participants shared their experiences of students’ class preparation and their subsequent ability to teach clinical judgment. Two participants who taught clinical judgment using small group activities, one using case studies and another using activities developed by Caputi (2022), stated their students came prepared for class because they realized they had to be prepared to participate meaningfully in the activities. Although she sometimes had shy students, one participant’s philosophy was that her students needed to work through their shyness as part of socialization into the nursing role. Three participants explained how their students did not read the textbook before class, but one participant stated she overcame this barrier by requiring a completed knowledge-based worksheet for homework points before class.
Finally, it is important to note that students’ food insecurity, transportation and housing needs, family and friend problems, health, and job factors were either never seen previously in the participants’ teaching careers or were not seen to such a great degree. Students’ anxiety, decreased resilience, and learning disabilities, which all affected mental health, had also escalated. One participant stated these created barriers for faculty presumably because learning deeper thinking skills requires more focus and concentration, which is difficult or impossible for students to sustain when facing these challenges. One site started a food pantry for students.
Critical thinking varied in skill level and therefore served as a facilitator or a barrier. Two participants viewed second-degree students’ critical thinking skills learned from their prior degree and work experience as a facilitator. By way of contrast, two participants stated critical thinking was lacking in traditional and accelerated BSN students which served as a barrier. One participant explained it was more challenging for second-degree students to learn clinical judgment because the students believed they already knew how to think like a nurse. She remarked that other disciplines such as natural scientists and journalists did not think like nurses. To her, what made nurses’ thinking distinctive was that they must multitask, constantly sift through information to determine what is and is not important very quickly at a rate that is much higher than most other professions, and appropriately intervene very quickly during 12-h shifts. Finally, traditional and accelerated BSN students expressed to one participant the difficulty they faced becoming nurses because they memorized in their prerequisite courses but had to learn a new way of thinking in nursing courses.
Two participants discussed how their students were task-oriented, focusing on procedures and technology in clinical rather than clinical judgment. In one situation, students were so focused on using technology they did not notice a patient's developing complication. In other situations, students did not realize that physical assessment, determining stability, and patient education were important.
Sub-theme 3: Faculty Factors
Additional professional development in clinical judgment definitions in many participants was needed. When the first interview statement was used, seven out of 16 participants responded by using the term critical thinking, were unable to define the difference between critical thinking and clinical judgment when asked by the researcher for clarification later in the interview, or stated the terms meant the same thing. The lack of understanding regarding what constitutes clinical judgment affected teaching methods. For example, one participant explained how she learned to focus on the critical thinking behind psychomotor skills while earning her master’s degree in nursing education. However, this participant sometimes referred to how she taught clinical judgment but was describing knowledge-based content, such as hormonal action.
Additional professional development in clinical judgment pedagogy was also needed. An explanation for this may be seen in how participants learned to teach clinical judgment. One participant provided workshops to full-time and clinical faculty on how to teach clinical judgment using Tanner's Clinical Judgment Model (Tanner, 2006), but one newer faculty struggled with incorporating clinical judgment pedagogy and expressed doubt as to whether incorporating Tanner's model would be effective. Other participants learned from mentors, imitated the way they were taught in nursing school, or by being preceptors. One participant relied on a vendor's podcasts. One participant stated a factor she believed affected pedagogy is many faculty do not have any education training, whether it is an education degree, new faculty development, or experience with clinical judgment research and the literature. Indeed, two participants stated they adjusted their teaching based on student feedback and “trial and error.” Participants who took education classes stated they found them helpful to learn general teaching methods, but they learned how to teach critical thinking instead of clinical judgment. Finally, some participants needed professional development in how to teach specific cognitive processes of clinical judgment, such as identifying and prioritizing a patient's problem, or evaluating outcomes with limited clinical time.
Preceptors also lacked professional development in clinical judgment teaching methods. Because of burnout and staff shortages, seasoned staff nurses with clinical judgment allowed a student to observe but they did not have the energy to teach them. A participant explained their hospital was staffed with half traveler nurses, who were unable to take students, and half new graduate nurses with only one year of experience. Because new graduate nurses lacked clinical judgment (Benner et al., 2009; Kavanagh & Sharpnack, 2021), they were unable to teach this to students.
Participants described their clinical nursing experience as a barrier and facilitator to teaching clinical judgment. Almost half the participants were nurse practitioners, which served as a barrier if the participant expected students to learn advanced practice skills. In two of these participants, the influence of their advanced practice was seen when describing the importance of teaching students how to perform a health history and assessment and differentiating between disease nuances when making a medical diagnosis. One participant expressed a concern about nurse practitioners teaching without an education background, and that her PhD had a nurse education emphasis which changed the way she taught clinical. Finally, the barriers expert clinicians experienced in learning how to teach was evident when one participant stated she taught based on “just being a nurse” from clinical experience. She described how she had to stop and think through the steps of how to teach clinical judgment because they were intuitive to her.
Pedagogical Reasoning
Some participants explained the reasoning behind their clinical judgment pedagogy. First, there was resistance to the NGN in one participant, serving as a barrier. She explained she did not think the NGN should affect her teaching methods. She stated she was not teaching to an exam; she was teaching course content.
Second, there was evidence of confusion regarding teaching clinical judgment and the nursing process, serving as a barrier. Some participants expressed confusion regarding whether they should still teach the nursing process in addition to clinical judgment. One participant's students learned the nursing process during the beginning of their first nursing course and then learned clinical judgment based on Tanner's Clinical Judgment Model (Tanner, 2006) throughout the remainder of the program. If the nursing process was mentioned in a later course, students became confused and stated they did not know what the professor was talking about. Therefore, the participant decided to no longer discuss the nursing process in her later class.
Another participant found that teaching clinical judgment using the Caputi Clinical Judgment Framework (Caputi, 2022) was a facilitator and solved the nursing process dilemma. For example, the participant shared how her students found that noticing a patient's declining status was challenging. She used Caputi's competency of comparing and contrasting data. By comparing their patient's current and past breathing patterns, students learned to notice breathing that was erratic and shallow. Caputi's clinical judgment competencies gave students guidance in how to think more deeply by teaching them to assess accurately, systematically, and comprehensively; note inconsistencies; and ask if they needed to gather additional information before analyzing the data to determine the patient's problem. Finally, when students interpreted their findings, they determined how to prioritize and manage the patient's care. However, this participant faced faculty resistance in her program. Although new faculty were required to teach using Caputi's framework, despite professional development the participants with teaching experience at that site did not use it.
Discussion
Findings were at times mixed and contradictory, which is not unusual in qualitative research (Merriam & Tisdell, 2016). Open-ended questions were used in the interview protocol to prevent participants from saying what they thought the researcher wanted to hear (Josselson, 2013). This generated a rich, thick description with unexpected findings. In some cases, diversity in findings was due to the variations in programs, students, and faculty. For example, although the study incorporated six accelerated BSN and direct-entry MSN programs, some of these students were integrated into a traditional BSN program, so participants discussed them as traditional BSN students. A second group of accelerated BSN students were more advanced due to a prior degree, work experience, a high degree of motivation, focused study effort, the ability to not have to work while in school, selective admission, and a program orientation outlining high expectations. A third group of accelerated BSN programs had no attendance policy and did not require students to buy and read the textbook because the faculty believed students should make this decision. These participants struggled more to help students learn clinical judgment and found that students who did not attend, engage in class, or read their textbooks failed the class.
Participants described strengths and deficits in students’ critical thinking, a concern because critical thinking is increasingly needed in the complex healthcare environment (Jessee, 2021; Van Damme, 2022). A recent higher education study of nonnursing and nursing students (n = 50,000) revealed only 47% of college graduates had desirable critical thinking skills, while 23% lacked critical thinking skills (Zahner et al., 2022). Concept maps (Bilik et al., 2020; Hidayati et al., 2020; Wu & Wu, 2020) and Socratic questioning (Makhene, 2019) increase critical thinking and increase learning motivation (Sari et al., 2021), a problem associated with task-orientation and inadequate class preparation.
Findings of faculty confusion and resistance indicate a need for professional development in clinical judgment pedagogy. Expert clinical practice does not automatically translate into expert pedagogical practice (Crider, 2022). While the median years of nursing experience was 17, the median years of teaching was only four. New faculty are novice educators and lack pedagogical content knowledge (Crider, 2022), which is pedagogical expertise combined with content expertise. Pedagogical content knowledge in this study's context includes an understanding of clinical judgment cognitive processes, pedagogy, and evaluation. Also, while an education degree or formal coursework in education is recommended for nursing faculty (McNelis et al., 2019), professional development and a change in teaching practices to teach clinical judgment are essential regardless of experience (Garner & Bedford, 2021; Patterson & Forneris, 2023). Teaching by trial and error, adjusting pedagogy based solely on student feedback, or absent formal faculty development in clinical judgment teaching methods do not support evidence-based pedagogy.
Some of the participants’ confusion may lie in a paucity of research findings on how to best teach clinical judgment. A separate finding of this study was a wide diversity in teaching methods within sites and between sites (Kerns, 2023). Faculty used three different clinical judgment models, no conceptual model, or solely the nursing process to teach, a similar finding supported in a separate national survey by Jessee et al. (2023). Nursing education has many clinical reasoning and clinical judgment conceptual models developed through years of research with no consensus on how clinical judgment should best be taught.
Preceptors and clinical faculty also need professional development (McPherson & Candela, 2019). Due to the nursing shortage with associated heavy workloads, larger proportion of new graduate nurses, and nurse burnout, the need for clinical judgment education is even greater (Enyan et al., 2021). An additional problem is that not all experienced nurses possess clinical judgment (Callihan et al., 2023; Kavanagh & Sharpnack, 2021). Two ways to teach clinical judgment to students and new graduate nurses are Tanner's four cognitive processes of clinical judgment in the Clinical Judgment Model, consisting of noticing, interpreting, responding, and reflecting (Tanner, 2006), which can be used as a guide for teaching clinical judgment, or Caputi's 23 competencies in the Clinical Judgment Framework, which explain how to teach the components of the cognitive processes of clinical judgment in a detailed manner (Caputi, 2022).
Another finding of this study was how faculty defined clinical judgment, which revealed diverse terminology use, definitions, and inadequate knowledge, likely indicating confusion over the multiple definitions found in the literature and a need for faculty development (Kerns, 2023). The NGN (Dickison et al., 2019) and clinical judgment concept in the AACN's The Essentials: Core Competencies for Professional Nursing Education (2021) are relatively new, again indicating the need for faculty development (Nielsen et al., 2023).
Professional development is also needed on the difference between critical thinking and clinical judgment. There are many definitions of critical thinking (Von Colln-Appling & Giuliano, 2017), clinical judgment (El Hussein et al., 2022; Manetti, 2019), clinical reasoning (Manetti, 2019), and clinical decision-making (Muntean, 2012). If faculty are unclear about the cognitive processes involved in clinical judgment, based on this study's findings they are less likely to teach clinical judgment effectively.
Participants expressed concerns about how to teach the nursing process and clinical judgment. The Caputi Clinical Judgment Framework (Caputi, 2022) aligns the nursing process, Tanner Clinical Judgment Model (Tanner, 2006), and the NCSBN Clinical Judgment Measurement Model on which the NGN is based (Dickison et al., 2019). However, Caputi describes 23 competencies which break clinical judgment into manageable components using teaching-learning activities to develop clinical judgment as students progress throughout nursing school. Since the framework is relatively new, robust research is needed using the Caputi Clinical Judgment Framework.
Evaluating clinical judgment is challenging. There is currently no measurement tool to evaluate clinical judgment other than the Lasater Clinical Judgment Rubric (Lasater, 2007), which although valid and reliable (Adamson et al., 2012; Rogers & Franklin, 2023; Victor-Chmil & Larew, 2013), is dependent upon interrater reliability, creating subjectivity and inconsistency concerns (Lee, 2021). The Lasater rubric has been used successfully in simulation, clinical, and new graduate nurses, however (Bertozzi et al., 2022; Manetti, 2018; Monagle et al., 2018). NGN test items (Betts et al., 2019) can be used since traditional test items, such as multiple choice, inadequately evaluate clinical judgment (Dickison et al., 2019). However, instead of using NGN items as evaluation methods in class, participants relied mainly on polling software, alternative item format questions, or discussion questions to evaluate clinical judgment in class. Further research is needed to develop a valid and reliable clinical judgment measurement tool.
Strengths and Limitations
A strength of the study is it explored details of clinical judgment pedagogical barriers and facilitators with associated recommendations from participants and the literature. A limitation of the study is lack of generalizability; all sites were universities. A second limitation is the study was not correlational or predictive; the extent to which the factors affected faculty's clinical judgment teaching methods or students’ learning clinical judgment was not quantitatively measured.
Implications for Practice
It is important for faculty to recognize the program, student, and faculty barriers and facilitators for clinical judgment pedagogy in their program. Second, administrators should find ways to mitigate barriers and means to maintain or strengthen facilitators to support faculty and students in teaching and learning clinical judgment. Third, professional development is essential along with faculty consensus and consistency in teaching clinical judgment throughout the curriculum. Further research is needed on the effects of university-based professional development on faculty's clinical judgment teaching methods.
Conclusion
While program, student, and faculty factors affected faculty's teaching clinical judgment, some of these factors were severe enough to serve as barriers. However, some factors served as facilitators. Several recommendations were given to support clinical judgment pedagogy in the context of these influencing factors. Mitigating barriers and strengthening facilitators can support faculty in teaching clinical judgment.
Footnotes
Availability of Data and Materials
Inquiries to access data and other research-related materials may be submitted for consideration to the corresponding author.
Consent for Publication
The authors consent to open access publication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
Institutional Review Board (IRB) approval was obtained from the parent institution, who declared the study exempt, and from each participating site where faculty were interviewed. Each voluntary participant signed an Informed Consent Form before being interviewed.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Study Approval Number
This study was approved as IRB Protocol #22-03-5467 by the parent institution.