
Abstract
Introduction
Migrants and refugees belong to the most marginalized groups in the world. Barriers related to the determinants of health can often preclude access to basic human rights, and have a negative impact on health. Therefore, it is essential to understand how to properly interface with people with different perceptions of health and disease and how to design programs based on available resources.
Aim
To explore the experience of socio-health workers who work in the context of a reception project in Italy related to taking care of the health needs of a migrant population in a multicultural context.
Methods
This research was a qualitative phenomenological study with an interpretive approach adhering to the Consolidated Criteria for Reporting Qualitative Research guidelines. The conversations were audio-recorded, transcribed, and read in depth. Reflexive analysis was used to analyze the data.
Results
Sixteen health and social workers were interviewed. Three main themes were extracted: (1) nature of needs and their facets; (2) interconnection between skills and in relationships; (3) struggles against shortages. The results highlight the participants’ attribution of meaning to the needs and requirements of migrants, their experience in the relationship with the team and the migrants, and the difficulties in carrying out their role.
Discussion
What the study found underscores the importance of designing interventions that consider the unique perceptions and experiences of professionals who engage with migrants in daily practice. The complex health needs, experiences, and different cultural representations of health and illness must be read and approached with a culturally competent vision.
Conclusion
The study reveals how much the strengths of taking care of migrants’ health lie in the ability to interconnect various competencies. This study gives elements for professionals and health organizations to understand the complexity of caring for the migrant population.
Keywords
Introduction
In the twenty-first century, the increasing wars, conflicts, and persecution have become one of the leading causes of migration worldwide (Lenderts et al., 2021). This phenomenon is reshaping the traditional arrangements on which living in societies was based locally and internationally (Dao et al., 2021). In the last decade alone, 100 million people have fled their homes to seek refuge within or outside their countries’ borders (United Nations, Department of Economic and Social Affairs, 2019). According to the Mid-Year Trend report, published by the U.N. Refugee Agency (2021), there was an exponential growth in migration. More than 84 million people worldwide migrate forced by violence, insecurity, and climate emergency (UNHCR, 2021).
In this context, an unprecedented influx of refugees, asylum seekers, and other migrants have been observed in Europe, where approximately 1.5 million people have arrived in Europe since 2015, more than 1 million of whom have sought asylum after fleeing countries affected by war, conflict, or economic crisis (Mammana et al., 2020). The social, economic, political, and cultural impacts generated by migration within the European continent are also reflected in Italy, which the last 20 years, shifted progressively into a “country of immigration.” At the end of 2021, Italy hosted over 165,000 refugees and asylum-seekers in reception facilities, including over 12,000 unaccompanied children. Most people of concern came from Nigeria, Pakistan, Afghanistan, Mali, Somalia, and Gambia (UNHCR, 2022). It is estimated that in 2015–2020, about half a million people arrived on Italian coasts, crossing the central Mediterranean route that connects the two shores of the Mediterranean. These events inevitably confronted Italian society with the challenge of reception and inclusion (Anci, 2017; Capello et al., 2014; SPRAR, 2016).
Review of Literature
Concerning health, migrants from the Mediterranean are often affected by physical and psychological traumas resulting from the violence they experienced during the journey (Commodore-Mensah et al., 2021; Fazel et al., 2005; Hameed et al., 2018). In addition, poverty, social isolation, armed conflict, human rights violations, stressors related to forced migration and separation from family make it very difficult to maintain an optimal health status (EpiCenter, 2013; Gümüşsoy et al., 2021; Legido-Quigley et al., 2019; WHO, 2018). What has been said is also amplified by the linguistic and cultural barriers and by the perception by migrants of a lack of consideration of their own needs, values, beliefs, and cultural practices by the host countries (Lenderts et al., 2021).
All of these aspects could complicate the process of adaptation and social integration within host countries, lead to health inequalities (Commodore-Mensah et al., 2021; Vázquez et al., 2011) and negatively impact the perceived quality of life (QoL) of migrants and refugees (D'Egidio et al., 2017; Toselli et al., 2018). In addition, the so-called “healthy migrant effect,” a form of self-selection at origin whereby only those in good health decide to migrate (Fennelly, 2007), is described in the literature. However, once they arrive in the host countries, migrants progressively see their health status depleted, as they are exposed to many risk factors related to generally poor living conditions and poor integration policy, as well as prejudice and stigma that limit access to care (Fennelly, 2007; Nizzi Grifi et al., 2020). Therefore, to protect migrant health, international and national policies should insist on the integration into social and health services, as outlined in the Sustainable Development Goals of Agenda 2030 (IOM, 2022) and by the Global Compact for Safe, Orderly and Regular Migration (2018). To build a society that includes people, valuable resources for its development become relevant. It is crucial to promote social and labor insertion, foster cultural assimilation of the other, and the inclusion of migrant groups in health services and ensure the care of a clientele bearing specific biographies, cultures, traditions, beliefs, and needs while respecting universal human rights (Commodore-Mensah et al., 2021). Based on these conditions, it is essential to examine the strengths, obstacles, and difficulties faced by professionals within reception systems, particularly in regions where migration is prevalent. These systems often handle initial rescue efforts, primary healthcare, pre-identification processes, and guidance on asylum and relocation procedures, as seen in Europe.
According to Leininger's Transcultural Nursing Model (Leininger, 2002), nurses are responsible for guiding migrants through their settlement process. This model stresses an anthropological approach to healthcare, which involves understanding and respecting the cultural beliefs and lifestyles of individuals and groups. The main goal is to provide care that is culturally congruent, aligning with the patients’ cultural values, beliefs, and practices. Nurses must consider the entire cultural context of the patient, requiring deep cultural sensitivity and effective communication across linguistic and cultural differences. They need to identify and respect patients’ cultural practices, adapting their care methods accordingly (McFarland & Wehbe-Alamah, 2019).
This anthropological perspective also promotes the inclusion and integration of migrants into the host community, facilitating their adaptation and improving overall health outcomes. With a comprehensive understanding of people's needs and addressing health concerns of various kinds, nurses serve as intermediaries between professionals and the population under examination (Commodore-Mensah et al., 2021). To respond to the needs of migrants, refugees, and asylum seekers, many European countries united by hosting high migratory flows have adopted a specific system of reception and integration implemented by local authorities. Various services are implemented as part of the organized reception and the support of projects composed of multidisciplinary teams, including healthcare workers (European Union Agency for Asylum, 2022; Mancini et al., 2019; Priebe et al., 2011). The aim is to guarantee protection and material, health, social, and psychological reception thanks to individual paths of socioeconomic insertion and integration into the community (Reception and Integration System, 2022). These territorial projects provide for implementing social accompaniment activities aimed at knowledge of the territory and adequate access to local services, including social and healthcare. Specialized projects for the reception are also implemented to support people with specific vulnerabilities such as disabilities or health problems (physical and mental), unaccompanied minors, victims of torture, single-parent households, and single pregnant women (Reception and Integration System, 2022).
Moreover, specific projects are implemented in Italy to enhance Italy's inland areas, i.e., those geographic contexts mainly characterized by a low number of residents and a shortage of health services. An emblematic example is Camini, a small Italian country located on the Ionian Sea coast in the Calabria region of Southern Italy. It represents an example of integration between native and immigrant populations (Bianco et al., 2016; Reception and Integration System, 2022).
Although several studies have analyzed the complexity of immigration (Albers et al., 2021; Lebano et al., 2020; Segal, 2019), only a few studies in Europe, particularly in Italy, have explored professionals’ views regarding strengths and barriers in the care of a migrant population (Driel, 2020; Mancini et al., 2019; Priebe et al., 2011; Viola et al., 2018). However, to the best of the author’s knowledge, no studies have analyzed the experience of social and health workers in a shelter rooted in the local area, in a situation of close coexistence between migrants, the native population and the workers themselves. Understanding how to properly interface with people with different needs and perceptions of self, body, health and disease, and how to design programs to take care of the health of “migrants,” is fundamental to overcoming the emergency logic with which it has been faced to date. Migration can represent an opportunity for the growth and development of the health supply that is notably lacking in these areas. The complexity of reception systems also raises questions about the most effective ways to take care of the needs of migrants and the challenges and resources needed to ensure a higher level of health and provide culturally congruent care aimed at inclusion and integration. The setting up of a structured and systematic modality of reception, health promotion, and integration allows to work to achieve the highest possible level of health for all individuals in the area, whether they are migrants or natives. Knowing the experiences of professionals working in the field of welcoming migrants can therefore help to highlight that which has already been done in this direction and be able to promote an improvement in the entire healthcare process.
The study aimed to explore the experience of social and health professionals working within a reception project in Italy concerning taking care of the health needs of a migrant population.
Methods
Design
This research was a qualitative phenomenological study with an interpretive approach adhering to the Consolidated Criteria for Reporting Qualitative Research guidelines (Tong et al., 2007).
Interpretative phenomenological analysis (IPA) focuses on the in-depth meaning of the participants’ experiences (Smith et al., 2009). On the one hand, it adopts an idiographic approach because of the individual case investigation. On the other, it uses an interpretive one, following the principles of hermeneutics (Welch, 1999). Finally, the phenomenological perspective is used to get knowledge from phenomena, free from theoretical presuppositions that assign meanings to experience a priori (Larkin & Thompson, 2012). Researchers run into the personal representations of the experience of people immersed in a linguistic, relational, cultural, and physical world, taking part in intersubjective meaning-making, where one cannot avoid interpretation but must reflect on one's role in producing such interpretations (Smith et al., 2009).
The Consolidated criteria for qualitative research standards for reporting were followed in writing the research report (Tong et al., 2007).
Research Question
The following research questions were addressed in this study:
What are the experiences and perspectives of social and health workers regarding the health needs of migrants? What are the perceived strengths and barriers in addressing the health needs of migrants within a reception project in Italy?
Sample
A propositional criterion was used for sampling (Polit & Beck, 2014). Health and social workers working in the migrant reception project in Camini (RC) were recruited.
Inclusion/Exclusion Criteria
Since the standard length of participation in a reception project for each migrant is six months, participants recruited were social and health workers working on the migrant reception project with at least six months of work experience. This minimum period was chosen to include professionals who have experienced at least an entire project with a migrant. A shorter work experience in the project probably would not have been sufficient to understand the health needs of migrants and possible health interventions to implement.
Data Collection
Data were collected in April 2021 in Camini, a rural center in Southern Italy, at a location agreed upon by the participants. After identifying possible participants for the study, they were contacted individually by the host project leaders to agree on the date and time of the interview. Previously, the participants had had no contact with the researchers.
Following the chosen methodology, each researcher involved in the study performed bracketing before the data collection (Creswell, 1994), writing ideas, preconceptions, and beliefs about the phenomenon under investigation. This first step is crucial because researchers’ preconceived notions could influence data analysis in studies using a phenomenological interpretive approach (Tufford & Newman, 2012). By performing this “reflective technique” before data collection and analysis, researchers can take more outstanding care to avoid introducing preconceptions that could negatively influence the research. Data were collected using a semi-structured face-to-face interview (Smith, 2017). This type of interview was chosen because it was particularly informative, allowing the researcher to create a logical progression for the topics covered. However, the interviewee's responses determine how the interviews are directed (Whiting, 2008). In addition, the semi-structured interview guide provides a clear set of instructions for interviewers and, at the same time, can provide reliable and comparable qualitative data. The questions asked in the interviews are shown in Table 1.
Interviews’ Guide.

During the interviews, the researchers maintained an empathetic attitude, expressing warmth and reassurance, to facilitate the participants’ narration of their experiences (Simeone et al., 2018). Field notes were written, which are useful for recording personal reflections, notes related to the setting, and nonverbal language used by the interviewees. According to Corbin and Strauss (1998), interviews were conducted without interruption until participants stated that they had nothing more to add or until new information emerged. Data saturation (Polit & Beck, 2014) was reached after 16 interviews.
A socio-demographic questionnaire, explicitly created for this project, was used to gather information on the characteristics of the participants.
Ethical Considerations
The procedures applied in this study followed the principles outlined in the Declaration of Helsinki. Approval was obtained from the Ethics Committee of the University of Rome Tor Vergata (protocol registration number 160.21). The purpose of the study was explained to each participant, and written informed consent was acquired to ensure anonymity, confidentiality, and data protection. All participants were assured they could withdraw from the study at any time. Each interview was assigned a sequential alphanumeric code, with no possibility of identifying participants.
Data Analysis
The interviews were audio-recorded and then transcribed in full. Interviews, data analysis, and the verification of results were conducted in the local native language of the study participants (Italian). The interviews and field notes were read and re-read in depth by two interviewers (PA and SS) independently, initially proceeding to annotate descriptive, linguistic, and conceptual elements that emerged from the text (Smith et al., 2009).
Next, emergent themes were identified, organized in a table to implement a comparison (clustering of themes), and finally grouped within superordinate themes. Each superordinate theme was linked to the underlying themes, which, in turn, were related to the participants’ original quotes (Smith et al., 2009). Table 2 illuminates the data analysis.
The Stages of Interpretative Phenomenological Analysis According to Smith et al. (2009).

A consensus validation was performed between the two researchers, experts in phenomenological analysis, and already co-authors of several qualitative studies. No discrepancies or disagreements were revealed. Finally, the identified themes were exemplified with a descriptive narrative and illustrated with quotes from the participants.
The criteria of credibility, transferability, and reliability described by Lincoln and Guba (1986) were considered to ensure the study's methodological rigor. Member checking was performed (Sandelowski, 2000). The findings were shared with participants, who were asked to confirm the emerging themes and share any additional information. At this point, translation was performed to compile the research report. The processes of translating and back-translating the in-text citations to enhance the themes were carried out according to the World Health Organisation (2016) methodology and focused on conceptual content rather than literal equivalents. The purpose of the translation was to look for the conceptual equivalent of a word or phrase and not a word-for-word translation. Thus, it was ensured that the original meaning of the data obtained was respected.
Results
Sample Characteristics
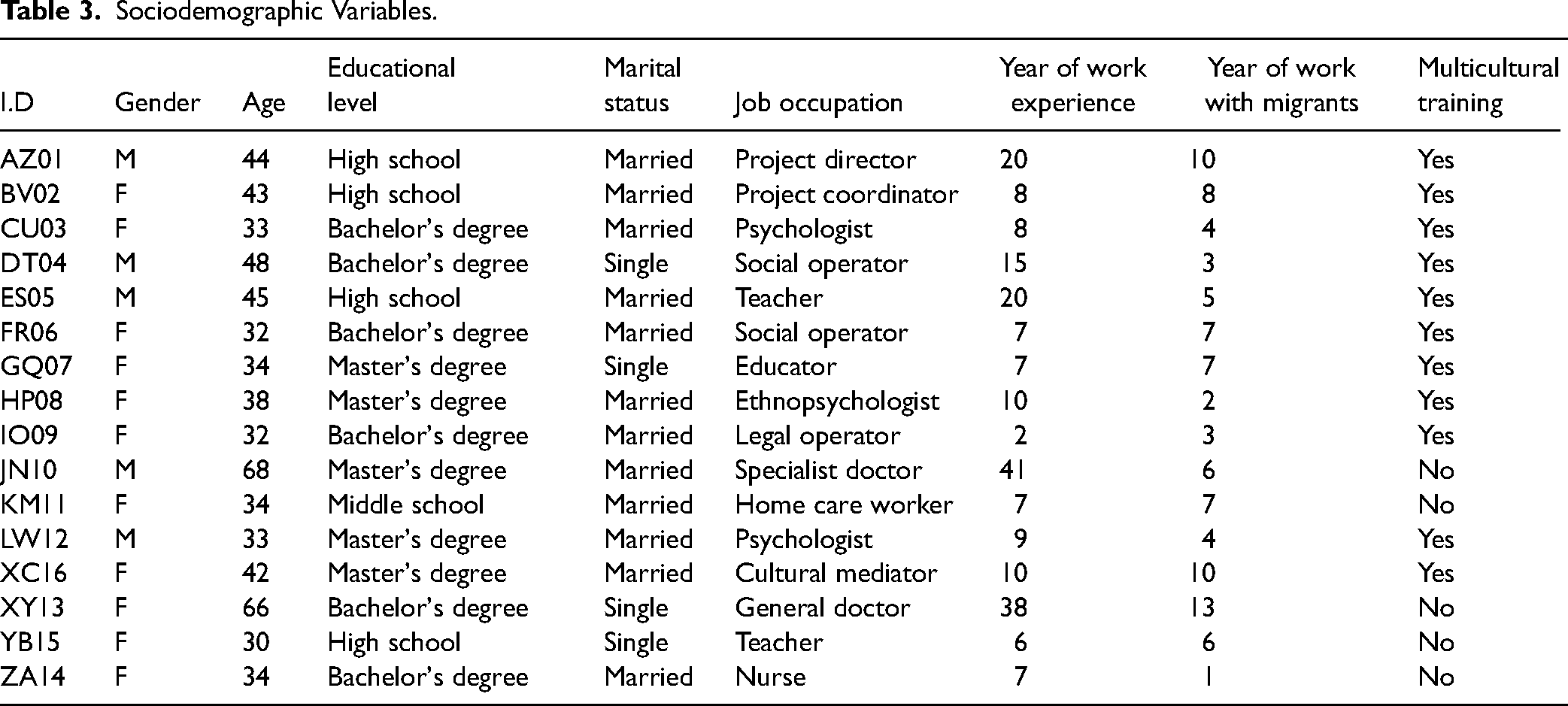
The sample comprised 16 people working on a welcoming project, with a prevalence of male gender (68%) and an average age of 41 years (SD 11.5). In total, 37.5% were healthcare professionals, 37.5% were social workers, and 25% were people involved in community management. Concerning education level, most participants had a higher education level than high school. At least 12 people (75%) attended a specific course in the multicultural field. The sample worked in Camini for an average of 6 years (SD 7). The main sociodemographic results are reported in Table 3.
Sociodemographic Variables.
Data analysis identified three main themes: (1) nature of needs and their facets; (2) interconnection between skills and in the relationship; and (3) struggle against shortage. Each theme encompasses different subthemes, summarized in Table 4.
Summary of Themes and Subthemes.

Nature of Needs and Their Facets
This theme includes the participants’ attribution of meaning to the needs and necessities of migrants. The interviewees’ experience is rich in references to how these needs are expressed and their different facets. First, what in the community represents the “status” of migrants emerges. Although they do not speak the same language, it seems that the operators can perceive the primary needs expressed.
The migrant population, although coming from different life experiences and cultural references, is united by the same needs, which manifest themselves as the very consequence of “being a migrant.”
In this sense, practitioners describe a commonality of needs, rather than a differentiation based on each person's peculiar context of origin, as reported by participants: They arrive at a place where they symbolically need to be welcomed, embraced, protected and helped for everything, starting from the foundation to start living again. They express so many complex needs in so many different ways, sometimes openly, sometimes we have to understand the needs they fail to bring out. (GQ07) As soon as they arrive, there is the problem of language, but we are now able to understand what they need immediately, because the migrant needs the same thing, regardless of where he or she arrives. (BV02) They come here with the same needs, and we try to help them. (CU03)
The interviewees highlight the discrepancy between the needs reported by migrants and those identified as priorities by the operators. A participant says in this regard: The most noticeable thing at the beginning is that they come with needs and requests that we want to welcome, but, at the same time, these needs don't fit with the goals of the project; it's as if we have different priorities. (XC16)
Among the needs reported, for migrants, it was essential to return to the land of origin; stakeholders, instead, recognized inclusion in the new country as a crucial aspect aimed at promoting integration between the different cultures, as described by a nurse: They always want to return to their homes … to their roots, and we struggle because our goal is to integrate them into our community (…). It is crucial to understand the boarding line between my point of view as a practitioner and that culture, which must be maintained. The integration between the two cultures is the real challenge. (GQ07)
The strength of the operators in the reception project is the tension toward the autonomy and independence of migrants. Integration and job placement are achieved through interventions aimed at making them autonomous and independent in society, defined by the interviewees as an intrinsic value of each job placement project. At the same time, the operators maintain the recognition of the particular identity of each one. The words of this participant confirm this: “This identity is powerful from a psychological point of view. It gives them the possibility of being recognised as people with personal values, and it is something that leads people to love the community” (HP08).
However, a consciously unexpressed need would seem to emerge, namely that of learning the host country's language, as this social worker describes: “In one case, there was a literacy problem, which paradoxically was a great asset because the lack of literacy denied a person access to an educational path from a work perspective. It is as if they also did not want to eradicate their identity through the difficulty of learning our language” (DT04). Literacy is thus a pathway that is often hindered by the migrants’ lack of motivation to study the host language and by their tendency toward welfarism rather than the acquisition of independence. The words of the interviewees confirm that the limit of the project lies in the risk of responding to the immediate needs of the beneficiaries and of not being able to promote their autonomy: They often do not work hard enough to learn the language, which leads to an obstacle in hiring a job. If they cannot interact with their partner or employer (…), we often lull ourselves a bit on our laurels. (GQ07) A deficit of these projects I see (…) is a defect of origin. The paternalism that is “we do everything for you” means that when they come into the project, they go into a muffled reality, depending on the beneficiary agency. (ES05)
Migrants report different needs to operators, but unexpressed needs, not perceived by migrants, are often common. They usually view mental health as embodied in corporeal forms and emerge when help is requested, generating an experience of helplessness, as reflected in the words of these study participants: “We often find psychosomatic disorders which in reality may conceal a psychic discomfort” (CU03)."I am often confronted with no real request for help, and no real manifestation of distress; this I regret, I don't know what to do to help them” (FR06).
Interconnection Between Skills and in the Relationship
The second theme explores the experience of health and social workers in dealing with the team and migrants. The interviews show that the success of taking care of migrants’ needs depends mainly on the ability to create connections between professionals and with the migrants regarding skills and mutual understanding. Sharing the peculiarity of living in the same territory in which migrants are welcomed, the work of professionals is directed toward the needs of individuals but oriented toward creating a multicultural community, of which they are part. In the latter aspect, therefore, migrants are not passive users but become active participants in constructing a community that involves both those who are welcomed and those who receive.
Two participants describe this reciprocity: I feel the need for openness, for confrontation, to welcome through listening to the colleague and the migrant the best way to help them, but also to help themselves along a path that a whole community, just as a community, not as individuals, but as a collection of individuals who are walking the path of mutual help. (DT04) We put our skills to work for them, and they restore our confidence and tell us how we can best work for them and how we can live together. (HP08)
The real strength of a group working with migrants is its members’ cohesion and interdependence, important aspects which are felt by the study participants. Teamwork skills are based on relationships, listening to each other, and the ability to interconnect, which is the self-representation that emerges most from the interviewees’ experience. Indeed, the participants speak of moldable skills that are not rigidly defined; the complexity of migrants’ needs and the immediacy with which they demand response require mutual adaptation, elasticity, and the ability to respond by uniting different perspectives and points of view, as expressed below: “The union, because we are a truly united team which works in tune, means that we listen to each other and that every day we do more and more in a continuous union. One person without the other doesn't make sense in this project. We are connected” (YB15). “What can't be achieved by someone, another does. Sometimes you can't say ‘this is up to me,’ because the needs they bring to us are about nuanced skills, for which each person can participate in taking charge in a continuous mutual listening” (XC16). The sub-theme “empathic understanding” mainly originates from the condition of migration that social workers share with the migrant population. From the interviewees’ words emerged a deep meaning of “being a migrant,” given by the experience of those who left their country to seek better living conditions in a new land. It represents a condition they share because, personally or referring to close affections, they have experienced migration from the particularly resource-poor South Italy to Northern Regions or other nations. What one interviewee states is emblematic in this sense: “I have been a migrant. Or rather, I come from reality, as I told you before, that my class had 35 pupils in elementary schools in the post-war period. Of these, 33 have now migrated far away” (JN10). Sharing this experience is a privileged condition because it allows the operators to understand the needs, expectations, and desires of the migrants they encounter in their work. A healthcare worker tells us about this: Also, because of our ancestors or we passed this experience. In my opinion, you should not burden a person who comes from another place, but you have to integrate him and make him feel like a person from the community. Because we know what it's like to live in a land other than ours, maybe we can help them better. (CU03)
Struggle Against Shortage
This theme summarizes the central experience of fatigue in social and health workers. It was caused by the multiple deficiencies that the territorial context in which they are placed manifests, the time limits of the reception project, and elements that often lead to the inability to provide the most effective response to the health needs of the migrant population. It is a significant dilemma experienced by the caregivers because they are in charge of care but at the same time are aware that they do not possess all of the resources to be able to do this to the best of their ability. The struggle is a constant in their caregiving. It is experienced with frustration but at the same time with acceptance, as they grew up in this poor context that led them to struggle to receive care, economic support, and job opportunities for themselves.
Two participants say: Referring to deficiencies, I say that many times they can be determined, in my opinion as I said before, by deficiencies concerning services, access to services in the territory (…). What happens is that now we have been cornered. In essence, we have extended this stay of some beneficiaries even though the project should be concluded, but they still need. (BV02) We too are “health migrants,” we too know what it is like to struggle to get a job, and that is why we used to struggle to emerge, and now we are doing it for them as well. (AZ01)
Participants speak of a daily “struggle” to assert health and social rights in a scenario of territorial scarcity. According to an empathetic vision consistent with the interconnection theme, this situation unites the migrants as much as the operators, who feel alone acting as intermediaries and accompanying the project beneficiaries in the weak services network, as told by two health workers In Calabria, we work in a poor territory, not only from an economic point of view but also because of the lack of services and territorial network. We often have to face difficulties alone, when problems should be shared with a complex system of taking charge, instead. (LV12). Calabria, a land of love and lack. For them but also us. That's why we try to be a liaison in the network because we know what it means not to have services. (AZ01)
Finally, a feeling of anger and helplessness for the absence of taking care of migrants by the area's social-health services, due to cultural prejudices ingrained in the system, prevails.
A participant tells: Seeking an alliance with public facilities that in the case of migrant patients refuse to take them in, we had great refusals despite going with mediators (…) So much anger! (HP08)
The other element that social workers struggle against is time. Reception projects are temporary and, given the complexity of the health needs and integration needs of individual migrants and their families, time is not sufficient to achieve the project's goals. Literacy, job placement, autonomy and economic independence require resources that are unlikely to be deployed in a limited period, especially in the socio-environmental scenario in which the project is embedded.
The words of these interviewees are significant in this sense: “Especially for the vulnerable cases, it is almost impossible to get job placement, so we have to prolong the situation, but now you just can't go back, now they have to get out of the project, and we are trying to find solutions” (BV02). "Time is not enough, mainly because of the difficulties we have in helping them find a home, because of prejudice, but even in other regions of Italy we struggle, even the time to care for them is long” (XY13).
Discussion
This study explored the experience of social and health professionals working in an Italian reception project about taking care of the health needs of a migrant population. Analysis of the interviews identified three themes: (1) nature of needs and their facets; (2) interconnection between skills and in the relationships; and (3) struggles against shortages.
In the first theme, the facet of needs is represented first and foremost by the priority given by migrants and caregivers throughout the reception process. The latter's perception sometimes seems to move in different directions. For migrants, it is crucial to maintain their identity roots with the hope of returning to their original country. It is a human condition that is described in the literature as an element that can hinder adequate settlement (Nicolais et al., 2021) and lead to resistance to language learning, which turns out to be the first intervention to facilitate the achievement of autonomy and independence in the host country, as reported by study participants. Language barriers and cultural norms are interrelated elements that result in barriers to settlement and access to care (Mammana et al., 2020; Manuti et al., 2010; Mladovsky, 2007; Naing et al., 2020; Priebe et al., 2011; Serre-Delcor et al., 2021). The tendency toward welfare described by the interviewees seems to be a consequence of the difficulty of attachment to a place that is typical of settlement approaches (Albers et al., 2021).
In contrast, studies report that the host society may unconsciously exclude migrants if there is no possibility of providing consistent forms of livelihood (e.g., with low-skilled job offers or low-paid occupations) (Galabuzi, 2004; Mancini et al., 2019; Van Loenen et al., 2018). This “social exclusion” approach can delay or even prevent the integration of migrants into the host society (Mancini et al., 2019). The other aspect already mentioned and described by the participants in the study concerns the cultural differences that underlie a different perception of priority in the needs expressed by migrants and detected by the professionals. The literature reviewed agrees that professionals experience the difficulty related to the perception of an “immeasurable” distance between the cultural and traumatic experiences experienced by migrants and the help and support that can be provided to them (Bischoff et al., 2009; Mammana et al., 2020; Mancini et al., 2019; Serre-Delcor et al., 2021). The real challenge, then, of a reception project is to maintain the identity of the migrant, recognizing cultural roots as the value elements on which to base interventions of caregiving and treatment.
According to Betancourt et al. (2003), cultural competence in healthcare involves different elements. First, to understand the importance of cultural influences on people's health beliefs and behaviors, second to consider how these factors influence the healthcare delivery system at different levels and, finally, to design interventions that take these issues into account to ensure quality care. As stated by Leininger (2002), providing adequate training in intercultural competence is indeed the strategic level for transforming the “foreigner” into a person who feels part of a community. They recognize it as their own and emphasize the crucial role of culturally competent nurses in leading the paradigm shift in reception and caretaking. Not only that but considering the needs of migrants with a cross-cultural perspective also means being able to go beyond the most superficial manifestations of those needs. Indeed, the study shows that there are often unexpressed needs or needs that manifest themselves in bodily forms. In general, the literature agrees that psychological distress is more common among asylum seekers and refugees compared to other types of immigration (Lindert et al., 2009; WHO, 2018) and that in response to psychosocial stress, somatoform disorders often occur (Giammusso et al., 2018; Lanzara et al., 2019; Manuti et al., 2013). In this regard, psychosocial characteristics (ethnicity, culture, religion, exposure to traumatic events, causes of migration, and other individual elements) influence the perception of one's needs and altered psychological health status, as well as help-seeking behavior (Lanzara et al., 2019; Satinsky et al., 2019). Although there is a high incidence of mental health-related problems among immigrants, they show lower rates of utilization of mental health services than natives (Giammusso et al., 2018; Satinsky et al., 2019), an assumption confirmed by the experiences reported by interviewees.
The answer to the complexity of migrants’ health needs lies in channeling different skills capable of ascertaining expressed and unexpressed needs to provide culturally congruent responses (De Melo et al., 2014). The second theme that emerged from the analysis emphasizes the interconnectedness among the members of the socio-health team of a receiving facility. Participants in the study report the experience of a multidisciplinary approach as a guide to caregiving action. They provide that health is a construct composed of interconnected bio-physiological, psychological, and social dimensions that require an overall view rather than an analytical approach focused on the individual domains (Dahlgren & Whitehead, 1991). Indeed, the flexibility of skills and organization is described as a strength in a migrant intake service (Bottura & Mancini, 2018; Priebe et al., 2011), as is the ability to ground care interventions by placing the relationship with the individual migrant and different cultural groups at the center. According to the literature, migrants experience a sense of attachment to the hosting place and responsiveness to their needs when they are in contexts in which they engage in new positive relationships and feel welcomed expectations and difficulties (Harmsen et al., 2005; Priebe et al., 2011). The scenario is one in which health is seen as the ability to carry out the tasks of daily life without resorting to the dependence on others (Godlee, 2011; Huber et al., 2011). In the study conducted, interconnectedness among group members and with migrants was concreted thanks to the development of empathic skills. Empathy is the main attribute of welcoming and caring for migrants. It is manifested in the study participants with the particular characteristics of the concept itself: the ability to understand the feelings and experience of being a migrant and communicate participation and understanding (Gümüşsoy et al., 2021; Kunyk & Olson, 2001; Morse et al., 2006; Wiseman, 1996).
The third central theme was summarized as “struggle against shortage.” Responding to migrants’ health needs faces structural, spatial, and time constraints. Much literature on the topic confirms that even in countries with public and universalistic healthcare systems, migrants face significant barriers to accessing health services due to bureaucratic, administrative, and organizational factors (Institute of Medicine, 2003; Mammana et al., 2020; Mavratza et al., 2021; Salami et al., 2018; Serre-Delcor et al., 2021). There is evidence of a lack of cultural competence in health services or the ineffectiveness of interventions aimed at overcoming these barriers and building immigrant-friendly services focused on migrant health needs and geared toward ensuring equity and appropriate care, both at the time of initial reception and in the long term (Mammana et al., 2020; Serre-Delcor et al., 2021). As reported by interviewees, the fragmentation of services and the lack of a continuous and coordinated intake network seem to be the leading cause of delays in diagnosis and treatment and disparities in outcomes (Mancini et al., 2019). The peculiar context of the study, however, revealed a substantial similarity with what is experienced by native citizens. As literature confirmed, they would experience a similar level of healthcare utilization and the same critical access to care produced in similar contexts in southern Italy (Bianco et al., 2016; Manuti et al., 2010; Manuti et al., 2013). Indeed, these are economically poor territories, lacking health facilities that are capable of responding to citizens’ care needs and often forcing them to migrate to other regions of the country to access services. In addition, migrants have to deal with stigma and discrimination that is still very much present, as narrated by study participants, which further limits access to care (Gil-Salmerón et al., 2021; Mak et al., 2021; WHO, 2018).
Strengths and Limitations
This study emphasizes the significance of comprehending the cultural influences of migrants on their health beliefs and behaviors. As highlighted by Iqbal et al. (2022), collaboration and empathy between professionals are key to addressing the diverse needs of migrant populations. By recognizing structural barriers and systemic challenges, such as language barriers and structural constraints, this study contributes to the ongoing debate on equity and access to healthcare for migrants.
This study also presents some limitations. First, the research was conducted exclusively within a single European nation. This aspect potentially limits the broad applicability of the findings due to the acknowledged importance of contextual analysis in assessing healthcare needs. It would be advantageous to include comparable settings to improve the understanding and adaptability of care models for broader implementation.
Second, the identification and recruitment of available participants, selected by project coordinators, may have influenced the perspectives and responses of those involved in the study.
Lastly, although not formally classified as a limitation, qualitative insights are inevitably influenced by preconceptions and biases. Given the distinct cultural environment of the data collection setting, which differed significantly from that of the researchers, there is an increased risk of interpretational bias, despite efforts to mitigate it through bracketing prior to data collection.
Additionally, it is worth noting the underrepresentation of nursing professionals in this study, with only one nurse participating.
Implication for Nursing Practice
The present study offers numerous implications for nursing clinical practice, providing fundamental elements for healthcare professionals and organizations to understand the complexity of caring for migrant populations. This recognition is crucial for developing effective and culturally sensitive care strategies, thus enhancing the quality of care.
Regarding needs understanding and intercultural training, there emerges a necessity for widespread intercultural education integrated into every educational context of society, not limited solely to the socio-healthcare field. Nurses must acquire advanced cultural competencies to recognize and address the often unexpressed needs of migrants. This training should encompass knowledge of migrants’ cultural backgrounds to better understand their perspectives and experiences, as well as intercultural communication techniques to overcome linguistic and cultural barriers, thereby enhancing the effectiveness of interactions between nurses and migrant patients.
The research underscores the importance of a multidisciplinary and culturally sensitive approach in designing evidence-based interventions for newly arrived migrants. Nurses must closely collaborate with other healthcare professionals, social workers, cultural mediators, and community organizations to develop patient-centered, coordinated, and integrated interventions, ensuring that different aspects of care (medical, psychological, social) are well-coordinated.
Expanding cultural competencies into organizational contexts can streamline administrative processes that often hinder migrant well-being. Nurses, as part of the healthcare system, can improve policies and administrative procedures to make them sensitive to migrant needs and promote an inclusive environment that fosters a sense of belonging among migrants, crucial for strengthening coping mechanisms and improving health and integration outcomes.
Analyzing the strengths and weaknesses of reception systems in rural areas and developing applicable solutions for similar contexts can lead to the creation of transferable reception models. Nurses can participate in the design and implementation of these models, ensuring that migrants’ healthcare needs are adequately addressed, and contribute to the formation of local support networks to optimize resources and counteract depopulation trends.
To comprehensively address these challenges, promoting intervention programs involving professionals, managers, administrators, and policymakers is necessary. Nurses must actively participate in these programs, bringing their expertise and firsthand knowledge of migrant patient needs, and develop qualities such as desire, commitment, empathy, and dedication to mitigate the critical shortage of support and resources affecting population health.
The presence of only one interviewed nurse highlights the need to introduce advanced practice nurses capable of addressing the needs of culturally diverse populations. These professionals can bridge the gap with local services, improving continuity and effectiveness of community-based care, and ensure more effective assistance by working closely with host and care communities to implement appropriate interventions.
Finally, to achieve meaningful outcomes, it would be desirable to continue research by exploring migrants’ perspectives regarding perceived health needs and correlating health status with interventions implemented by host and care communities.
Conclusion
In conclusion, one can say that study's results have provided multiple insights to guide the intake and care of a migrant population. The complex health needs, experiences, and different cultural representations of health and illness must be read and approached with a culturally competent vision. At the same time, this is embedded in a system that is capable of providing organizational structures and a network of coordinated interventions that effectively support taking care of the problems and needs of migrants themselves. What the study found also underscores the importance of designing interventions that consider the unique perceptions and experiences of professionals who engage with migrants in daily practice. The study reveals how much the strengths of taking care of migrants’ health lie in the ability to interconnect various competencies. This finding confirms, even further, the need to develop the advocacy function of nurses in the context of migration and to recognize that clinical nurses, researchers, and educators are critical to the provision of health services to migrants, as they can act as collectors and guarantors of their health rights. Nurse-led models of intake and care could also help to avoid or reduce disparities in access to care and produce culturally congruent outcomes.
Supplemental Material
sj-docx-1-son-10.1177_23779608241274234 - Supplemental material for The Experience of Staff Working in Migrants’ Reception Project: Phenomenological Study in a Multicultural Context
Supplemental material, sj-docx-1-son-10.1177_23779608241274234 for The Experience of Staff Working in Migrants’ Reception Project: Phenomenological Study in a Multicultural Context by Paola Arcadi, Mariachiara Figura, Ercole Vellone, Silvio Simeone, Loredana Piervisani, Gianluca Pucciarelli and Rosaria Alvaro in SAGE Open Nursing
Supplemental Material
sj-docx-2-son-10.1177_23779608241274234 - Supplemental material for The Experience of Staff Working in Migrants’ Reception Project: Phenomenological Study in a Multicultural Context
Supplemental material, sj-docx-2-son-10.1177_23779608241274234 for The Experience of Staff Working in Migrants’ Reception Project: Phenomenological Study in a Multicultural Context by Paola Arcadi, Mariachiara Figura, Ercole Vellone, Silvio Simeone, Loredana Piervisani, Gianluca Pucciarelli and Rosaria Alvaro in SAGE Open Nursing
Footnotes
Acknowledgments
The authors are grateful for the support of the Social Housing Cooperative Junji Mundu; and the whole town administration of the municipality of Camini. The authors would like to thank the people who participated in this study.
Author Contributions
Study design: PA, MF, EV, SS, GP, and RA. Data collection: PA, MF, EV, SS, GP, and RA. Data analysis: PA, MF, SS, GP, and LP. Study supervision: EV, SS, GP, and RA. Manuscript writing: PA, MF, SS, and GP. Critical revisions for important intellectual content: PA, MF, EV, and RA.
Use of AI Software
AI software was not used to write this article.
Availability of Data and Materials
The data and materials that support the findings of this study are available from the corresponding author upon reasonable request.
Consent for Publication
All authors who contributed to the study consent to publication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Consent to Participate
The Ethics Committee of the University of Tor Vergata approved this study on July 7, 2021 (protocol registration number 160.21). To protect privacy, all respondents signed an Informed Consent Form according to the responsibilities provided by the rules of good clinical practice and in full compliance with current legislation on personal data protection. Ethical norms and guidelines for the research project have been respected, and confidentiality was guaranteed. All participants gave consent to the processing of data for research purposes.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Center of Excellence for Nursing Scholarship, Rome, Italy.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.