
Abstract
Introduction
Mother-to-child transmission of hepatitis B infection is one of the major routes of hepatitis B virus (HBV) infection in Africa. Amusingly, Africa is the only region yet to meet the World Health Organization's target of reducing the prevalence of HBV infection to less than 1% among children under 5 years of age by 2020. In Ghana, little has been documented about midwives’ views on the factors impacting the successful implementation of mother-to-child transmission via HBV prevention programs.
Objective
This study explored midwives’ views on the challenges associated with the prevention of mother-to-child transmission of HBV infection in the La-Nkwantanang municipality.
Methods
The study adopted an exploratory descriptive qualitative design and involved 14 midwives who were purposively recruited from a primary-level health facility in the La-Nkwantanang Municipality, Accra. Individual face-to-face interviews were conducted using an in-depth interview guide. The data were content analyzed using the six steps recommended by Braun and Clark.
Results
Three main themes, namely, health professional or midwife factors and patient and health facility factors, negatively impacted the prevention of maternal-to-child transmission program. The five subthemes identified in this study included lack of awareness, financial constraints, and unavailability of logistics and protocols. The study recognized that midwives face many challenges even though they have a strong desire to prevent vertical transmission of HBV.
Conclusion
The implementation of a mother-to-child transmission program is negatively impacted by many intrinsic, client, and health facility factors. Midwives who act as major stakeholders need to be periodically trained on the components and protocols for managing pregnant women living with HBV. The necessary logistics and management protocols need to be urgently provided. The skills and education obtained from the training will empower midwives to be knowledgeable about how to deliver quality care and provide education and support for HBV-infected pregnant women. The provision of logistics needed for the successful implementation of the program could avert delays associated with the administration of the hepatitis B birth dose vaccine and immunoglobulin to exposed newborns.
Introduction
Hepatitis B virus (HBV) infection is one of the most potentially life-threatening liver infections in the world and has a high infectivity rate and multiple modes of transmission (Trépo, Chan & Lok, 2014). Prevention of maternal-to-child transmission (PMTCT) is crucial for eliminating HBV (Matthews et al., 2023). The components of successful PMTCT for the HBV program include the universal screening of all pregnant women at the antenatal clinic; immunization of babies born to HBV-positive mothers within the first 12 hours after birth with both the hepatitis B immunoglobulin (HBIG) and hepatitis B vaccines; and administration of antiviral prophylaxis with nucleos(t)ide analogs (NAs) for high-risk mothers from 28 weeks of gestation onwards (Loarec et al., 2022; Matthews et al., 2023; WHO, 2022a, 2022b; Zhang et al., 2019). These are all part of the World Health Organization's “triple elimination initiative” to lower morbidity from syphilis, HIV, and HBV. The other components include full vaccine coverage, access to affordable diagnostics to identify HBV-infected individuals, and linkage to care and antiviral therapy (CDC, 2019; Spearman et al., 2017; WHO, 2017).
Midwives are essential key players in every PMTCT session for the HBV program. Prevention practices that include cutting across health education, screening, administering postexposure prophylaxis for HBV-exposed newborns, vaccinating newborns with the hepatitis B birth dose (HepB-BD) vaccine, and providing linkage to care are crucial for eliminating HBV (CDC, 2019; WHO, 2019b). These practices, when effectively delivered by midwives, have the potential to avert many vertically transmitted HBV infections in newborns and prevent complications associated with HBV, as well as help achieve the elimination target by 2030. Despite the implementation of many strategies and programs, including PMTCT for HBV, reports indicate that MTCT for HBV still occurs in many Sub-Saharan African countries, including Ghana (Schmit, Nayagam, Thursz & Hallett, 2021). This observation has initiated discussions from various sectors and stakeholders to identify the factors that hinder the successful implementation of the PMTCT program. In this light, we undertook a qualitative enquiry to assess the factors or challenges affecting the successful implementation of PMTCT for the HBV program from the perspectives of midwives in the La-Nkwantanang municipality.
Literature Review
Prevalence of HBV in Africa
Reports available indicate that the WHO African region has the highest prevalence of HBV seroconversion, 2.5%, among children under 5 years of age. According to these reports, the WHO African region remains the only region that has yet to meet the WHO's global target of reducing chronic HBV incidence to less than 1% among children (Kabore et al., 2023). The MTCT is one of the major routes of acquiring HBV in Africa (WHO, 2019b). The successful implementation of PMTCT programs by midwives has the potential to avert many infections in newborns and facilitate the attainment of global elimination targets. This is because successful PMTCT programs have the potential to (a) identify pregnant women infected with HBV through routine screening, (b) offer these women antiviral drugs to lower their viral loads and (c) offer exposed infants postexposure prophylaxis for HBV as well as HepB-BD.
Despite the many benefits of PMTCT for HBV and the efforts of many countries to achieve the HBV elimination target, evidence from Senegal and many African countries suggests that new HBV infections are still being recorded in the region. For example, it was recently reported that 990,000 new HBV infections occurred in the WHO African region in 2019, an indication of existing gaps in the implementation of the PMTCT program Djaogol et al. (2019).
Awareness/ Knowledge Level of Healthcare Workers
At the healthcare worker level, studies have reported unsatisfactory knowledge of HBV and its transmission and treatment options for infected pregnant women (Adjei, Nachinab, Atibila, Ansah-Nyarko, Kyei & Fosu, 2022; Belete, Wondale, Kiros & Demissie, 2022; Freeman, Chea & Shobayo, 2023). The unsatisfactory knowledge and lack of awareness have largely been attributed to a lack of training and continuous education for healthcare personnel, who are major stakeholders in the PMTCT program (Moturi et al., 2018).
Barriers to PMTCT
Barriers operating at three different levels have been identified as having a negative impact on the implementation of the PMTCT program. Specifically, in Senegal, Djaogol et al. (2019) reported that several factors hinder healthcare providers from fully engaging in activities aimed at PMTCT of HBV. Reports available indicate that at the individual healthcare worker level, most healthcare personnel lack awareness since they have not received training on HBV infection or its treatment, especially for pregnant women. At the health facility level, the unavailability of free HBV Rapid Diagnostic Test (RDT) kits, HBIG coupled with the high cost of screening, antiviral treatment for HBV-positive mothers, and missed opportunities for vaccination for home birth deliveries have been highlighted as factors impeding the PMTCT program. Again, at the facility level, the scarcity of HBIG and the absence of national directives or programs to prevent HBV have all negatively impacted PMTCT programs (Chabrol et al., 2019; Djaogol et al., 2019; Ntsime, Makhado & Sehularo, 2022; Olakunde et al., 2023). At the client and family level, the mother's denial of her hepatitis B seropositivity, her ignorance of the effects of hepatitis B on her infant and her entire family, and her partner's lack of participation in posttest counseling have all been reported as barriers affecting PMTCT program implementation (Adjei, Suglo, Ahenkorah, MacDonald & Richter, 2023; Paul, Marie & Bechem, 2017).
Midwives in the PMTCT Program
There is enough evidence to show that midwives have the ability to intervene to reduce the vertical transmission of HBV. Many studies have shown that midwives play an essential role in preventing new infections, especially those that are vertically transmitted (Adjei et al., 2022; Opoku-Danso & Habedi, 2023). In many settings, including highly endemic regions of the world, midwives provide HBV counseling, testing support in antiviral therapy, and administration of postexposure prophylaxis to exposed newborns (CDC, 2019; WHO, 2019b). The role of the midwife extends to follow-up for HBV-infected mothers and their families as well as referrals for continuity of care. Studies have demonstrated the willingness of midwives to participate in the care of pregnant women infected with bloodborne infections, including HBV (Nkwabong, Meboulou Nguel, Kamgaing & Keddi Jippe, 2018). The effectiveness of activities and practices of midwives in averting new vertically transmitted HBV infections depends largely on the removal of individual-, client-, and health facility-level barriers that hinder the effective performance of their roles.
Research Question
What are the challenges faced by midwives who are involved in the implementation of the prevention of mother-to-child transmission of hepatitis B program in the La-Nkwantanang municipality?
Methods
Study Design
The study used a qualitative exploratory descriptive design to investigate midwives’ practices toward the PMTCT of HBV and the factors that influence these practices. The approach was deemed appropriate because it allowed participants to describe intensely the challenges associated with the PMTCT of HBV.
Study Setting
The study was conducted at Madina Polyclinic in the La Nkwantanang Municipality in the Greater-Accra region. The polyclinic was chosen as the study site because, even though it is a primary facility, it attracts many pregnant women due to its location in the commercial zone of the municipality. Compared to more than 20 birthing units or facilities within the municipality, the facility has the second highest number of antenatal registrants per year. The study was conducted in this setting because the midwives in the setting engage in practices that prevent mother-to-child transmission of HBV. In particular, the midwives in the setting are responsible for the vaccination of HepB-BD and HBIG to babies born to mothers living with HBV, unlike other settings that were reviewed.
Operational Definitions of Terms
Midwife: In this study, a midwife was a trained professional who provided antenatal, delivery, and postnatal services to women and was also involved in the activities and practices outlined for the PMTCT of HBV (ICM, 2011).
Prevention of mother-to-child transmission: PMTCT refers to interventions to prevent transmission of HBV from an HBV-positive mother to her infant during pregnancy, labor, delivery, or breastfeeding. These interventions include counseling, testing, support for antiviral therapy, initiation of postexposure prophylaxis for exposed newborns and follow-up care for women infected with HBV and their families (WHO, 2020b).
PMTCT practices among midwives: This refers to the provision of PMTCT services according to recommended guidelines and facility-level protocols in a healthcare setting.
Willingness: The level of acceptance of midwives to participate in all PMTCT programs, including service provision in the health facility, to prevent new HBV infections through vertical transmission
The HepB-BD is the initial hepatitis B vaccine given at birth to all newborns, irrespective of the HBV status of the mothers (WHO, 2019a). In countries where the HepB-BD dose is not yet a national program, HepB-BD is given at birth to newborns exposed to HBV and are at risk of vertical transmission.
Study Population and Sampling
The research population included all practicing midwives working in the Madina Polyclinic located within the La-Nkwantanang Municipality. In all, 64 midwives provided a wide range of services to pregnant women in the facility. Fourteen participants were recruited purposively to participate in the study based on their experiences, and practices and for them to give detailed accounts of their challenges with PMTCT of Hepatitis B program in the facility. The resources available could also not allow the researchers to interview all 64 midwives.
We relied on purposive sampling procedures to select the participants for the study since it is less time-consuming, and most importantly because it allows researchers to identify and recruit only information-rich cases to be part of the study (Palinkas et al., 2015). In our case, purposive sampling made it possible for us to have only midwives who have in-depth information about the phenomenon under investigation to participate in the study. The sample size of 14 was, however, determined by data saturation, which was evidenced by the absence of new codes or themes emerging after the analysis of the 14th transcript, implying that no new information would be derived if the interviews were to continue (Saunders et al., 2018).
Inclusion and Exclusion Criteria
The inclusion criterion included all registered midwives who provided consent to participate in the study. These midwives were involved in the care of pregnant women from conception to 6 weeks postpartum. In addition, these midwives had at least 1 year of work experience in the study facilities. Midwives, who were on leave during the time of the study, performed administrative duties and hence were not directly involved with patient care activities, were excluded from the study.
Data Collection Instrument
Qualitative data were gathered through individual in-depth interviews, which were conducted from February to April 2020. The interview guide was developed deliberately for this study and included sections ranging from sociodemographic information and questions on awareness of HBV. The instrument also had sections that solicited information on client-level barriers to PMTCT as well as health facility-level barriers. The interview guide was piloted with two participants at the Pentecost Hospital before the main data collection phase, and necessary adjustments were made to guarantee high-quality research (Malmqvist, Hellberg, Möllås, Rose & Shevlin, 2019).
Data Collection Technique and Procedure
Introductory letters were presented to the administrator of the selected health facility to pave the way for data collection. The facility nurse/midwife manager as well as the unit managers were informed of the nature, aim, and procedures of the study. The study was advertised on a facility notice board, and information on the nature, and procedure of the study was given to the midwives during their weekly morning meeting. Care was taken not to create any inconvenience to the midwives; as such, the midwives were given prior information about the days and times needed for data collection, and agreements were reached with them.
Interviews were conducted by the first author, who was a registered and qualified midwife and a student in the postgraduate nursing program at the time this project was conducted. The remaining three authors, who are Ph.D. holders in nursing education and are experienced, guided the data collection process as project supervisors.
Eleven individual interviews were conducted face-to-face in the hospital's common room, while the remaining three were conducted in the comfort of the participants’ homes upon their request. All interviews were audio recorded after consent was obtained from the participants. During each interview session, the researchers’ reflections and participants’ nonverbal communication and body language were recorded in the field notes. The interviews ranged from 30 min to 1 hour, and audio recordings of the interviews were transcribed verbatim and shared with participants for member checking.
Data Analysis
The authors analyzed the data manually using the reflexive thematic analysis approach outlined by Braun and Clarke (2006). This approach consists of six steps: data familiarization and writing familiarization notes; systematic data coding; generating initial themes from coded and collated data; developing and reviewing themes; refining, defining, and naming themes; and writing the report. The field notes were read together with the transcripts during analysis, and this process assisted the authors in assigning meaning to the extracted data. The first author developed codes, subthemes, and themes from the transcripts. The remaining authors then met face-to-face to reach a consensus on the final themes and subthemes for reporting.
Data Quality Management
To ensure the trustworthiness of the study, the researcher utilized the (Lincoln & Guba, 1985) criteria for validity in qualitative research, which were credibility, transferability, dependability, and confirmability. Credibility was ensured by collecting data to saturation, audio recording all interviews, peer debriefing with other researchers who were not part of the study, and member checking with participants. To achieve transferability, the researchers ensured information on the research settings as well as a detailed description of the research participants, categorically stating the inclusion and exclusion criteria of the study participants. The confirmability and dependability of the study were maintained by describing in detail the research methodology under which the research was carried out as well as the data gathering process in detail, elaborating on what took place in the field, and prolonging the duration of data collection.
Ethical Considerations
Ethics approval was obtained from the Ghana Health Service Ethics Review Committee (GHS-ERCO48/11/19). In addition, an approval letter from the director of the la-Nkwantanang municipal assembly was sent to the administrator and Deputy Director of Nursing Services of the health facilities in the municipality for permission before potential participants were approached in the maternal health units to seek their permission for participation in the study. Agreement was reached on the date and time of the interview based on the patients’ availability.
The researcher ensured that the participants were given an information sheet to read and decide whether they would participate in the study before the data collection. Informed consent was obtained from each participant with an assurance of anonymity and confidentiality. The right to withdraw from participating in the study at any point was allowed with no consequences. Anonymity was maintained by assigning participants special pseudonyms, and confidentiality was also maintained (by ensuring that all the audio tapes, transcribed data, field notes, and documented information given by the participants were stored and encrypted). Access to the data is restricted to the research team alone.
Results
Sociodemographic Characteristics of the Study Sample
A total of 14 midwives who were all females participated in the study. Participants were aged between 29 and 50 years, and they were all Christians. All 14 participants had diploma certificates in Midwifery. Eleven of the participants were Senior Staff Midwives with work experience between 3 and 10 years, midwives were Senior Midwifery Officers with 13 to 14 years of working experience, and only one midwife was a midwifery officer with 13 years of working experience. All the participants were married except one midwife who was identified as single (Table 1).
Themes and Subthemes
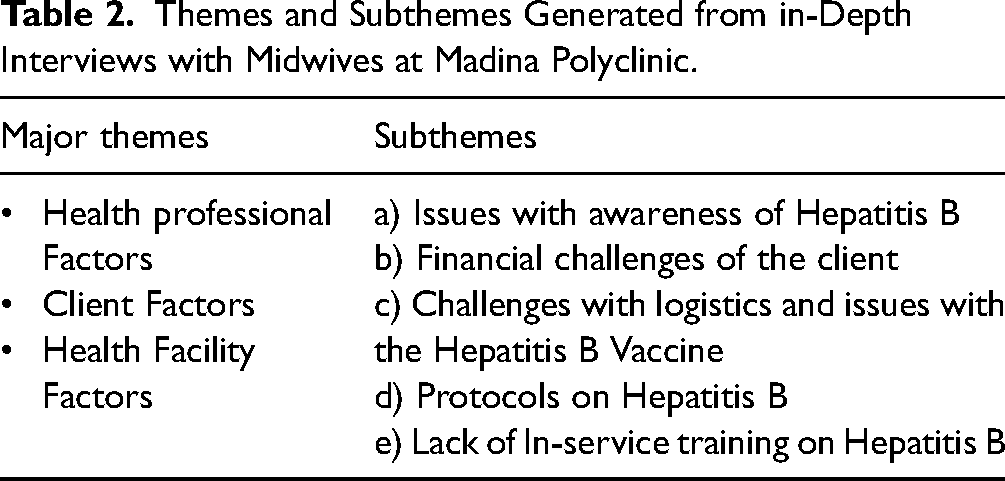
Three major themes, namely, health professional factors, client factors, and health facility factors emerged from the study. Five corresponding subthemes were also identified. These include knowledge of HBV, financial challenges of clients, availability of logistics, protocols on HBV, and, ultimately, in-service training on HBV. Table 2 presents a summary of the themes and subthemes.
Sociodemographic Characteristics of the Study Sample at Madina Polyclinic (n = 14).

Themes and Subthemes Generated from in-Depth Interviews with Midwives at Madina Polyclinic.
Theme 1: Health professional factors affecting the successful implementation of prevention via PMTCT for the HBV program.
The participants in this study reported several factors that impeded the successful implementation of the PMTCT program. These factors, according to the participants, are inherent and affect midwives’ ability to provide adequate care to pregnant women under the PMTCT for the HBV program. The study identified the HBV knowledge of midwives as a factor that can affect the successful implementation of the program.
Issues with Awareness of HBV
Participants expressed various levels of knowledge about HBV, which also included some misconceptions about the causes and mode of transmission.
Hepatitis B I think, in my own opinion, is a viral infection that can be acquired through body fluids, yeah that is the simple thing I can say about hepatitis B. Yes, you can get it through body fluids, you can get it through saliva and urine; what I am not too sure about is sweat, but I have not had the time to check whether sweat can transmit hepatitis B or not, am not very sure.
In contrast, P3 had this to say about the causes of hepatitis B:
Okay, I know hepatitis B is an infection and it also affects the kidney. Yeah, and it doesn’t make it function well that is what I know. I know that when you take in too much of NSAIDS like paracetamol you take them rough, rough and you do not take in too much fluids to urinate so that the kidney will be free you can contract it, that is what I know.
Concerning the knowledge of the HBV vaccine and whether it was safe and effective participants shared their various views. Most of the participants believed the vaccine was safe and effective, while few had contrary views to show that other alternatives, such as being careful and educating clients, can prevent HBV infection.
Thus far, we all think that if you are vaccinated, you are protected that is the mentality we have now. I don’t think it is safe as such, but all we can do is take our infection prevention seriously by screening all our clients, promoting education about hepatitis B, and letting our clients know more about hepatitis B and how to take care of themselves. Well, the vaccine will help us, but what if you did not get it at the right time? I do not think is 100% safe. Therefore, I think if we can educate the clients and take good care of ourselves, I think it is better than the vaccine.
Furthermore, concerning the knowledge of treatment options available for pregnant hepatitis B mothers, the majority of the participants were unaware of the availability of treatment for pregnant women infected with HBV and that treatment during pregnancy is possible.
No, I don’t know of any treatment options
Participants had diverse views concerning whether hepatitis B was curable. Most of the participants thought it was not curable, while a few of them had diverse views.
No, it is not curable I know it is managed. You will be on drugs that are not curable. I learnt they can only be managed with some lifestyle changes. They are not supposed to eat certain foods such as fats, and they have to eat vegetables and fruits just to keep the disease from progressing to the next stage or something.
I think it can be curable because a sister's daughter had it. She tested positive after she started taking some drugs, but I had forgotten her name. She was taking it every day for a year she then tested, and she was negative; she waited for six months, she tested negative again, and she went for the vaccination.
Theme 2. Client factors affecting the successful implementation of PMTCT for the HBV program.
The study identified several other factors that are not within the midwives’ control but rather are directly related to the clients and have an effect on the midwives’ practices regarding PMTCT for HBV. According to the participants, the financial situation of pregnant women and their families can greatly affect the implementation of the PMTCT strategy.
Financial Challenges of Clients
Several participants mentioned that most of their clients are not able to perform their financial obligations regarding purchasing the hepatitis B vaccine and immunoglobulin for their newborns. Some other participants further added that the cost of hepatitis B screening is also a source of financial challenge for some clients.
Okay, the number one challenge will be an economic challenge because immunoglobulin is very expensive; I once had a mother who couldn’t even get the money for the immunoglobulin, which was approximately 500 Cedis so the baby was just given the vaccine and I don’t know how one can work.
Theme 3. Health facility factors affecting the successful implementation of PMTCT for the HBV program
Challenges with Logistics and Issues with the Hepatitis B Vaccine
Almost all the participants expressed that they had challenges with the availability of RDT kits for HBV to screen pregnant women for hepatitis B during antenatal booking visits and for other pregnant women who reported late during the antenatal period. The participants admitted that some pregnant women never had the opportunity to be screened for HBV during pregnancy and that they delivered without knowing their HBV status only because the facility did not have RDT kits for screening their clients.
The test on the first visit, regarding HIV, is free, and immediately after you come for the first visit, we test you for free because we have the logistics with us. We have the test kits, but as for Hep B, we don’t even know how to check its number one; we don’t even have the test kits number two, and then the client pays for it number three. Therefore, a client who cannot pay for it may not be screened until he or she can pay.
Sometimes there is a shortage of logistics at the facility which means the hepatitis B testing kits because some time ago, for some months, we did not have test kits. For people who came to do the test, hepatitis B was not done for them; unfortunately, you get a late attendant someone who comes in her 36 to 37th weeks, and the test was not done. She will deliver, and she won’t know her hepatitis B status.
Most of the participants had issues concerning the availability of the HBV vaccine, which is used as a HepB-BD for exposed newborns. Most participants further expressed frustrations with the arrangement of the vaccines for clients since the vaccines are not stocked in the facility. According to the participants, the unavailability of the vaccines in the facility results in delays in the administration of the vaccines to newborns, which can lead to frustrating mothers breastfeeding their newborns before the HBV birth dose is administered.
Where I am working, the HBV vaccines are not readily available in the labour ward; we call those who sell them, and most of the time, they are not available to deliver the vaccines to you at night when the baby is born during the night shift; sometimes on weekends, they are not on duty with us, and you have to call and call. Sometimes you would not even get them during the weekend, and with this, the baby would be crying due to hunger disturbing the mother; sometimes some mothers give up, and then they breastfeed the babies.
Unavailability of Protocols for PMTCT
Regarding protocols for hepatitis B, most of the participants stated that they had not seen clear written guidelines or protocols on the management of pregnant women infected with HBV. We need to see a protocol or how we go about it, and even before we give the vaccine, we need some protocol from ANC up to delivery as well as discharge. There should be a protocol for us to go through before making every child receive the vaccine. These few ones that we know are just on screening, and if the mother is positive, you vaccinate the child that is all that we know. If there are other things involved, we do not know if all babies can take the vaccine, if a baby whose mother is G6PD reactive, or if a baby who is G6PD reactive can also take it. We do not know if there are any contraindications for the vaccine. Additionally, we do not know about any treatment available for mothers who have HBV, unlike for HIV-positive mothers, so we need protocols and guidelines disseminated via workshops and training sessions to guide us.
Lack of In-Service Training on the PMTCT of HBV
The participants expressed that they had never attended any form of training on HBV or its management during pregnancy. According to the participants, the lack of training and adequate information contributed to the low level of awareness and unsatisfactory level of knowledge about HBV disease and its management.
No! no, because I have not previously received any workshop on Hepatitis B, so I do not have enough knowledge on it; it is just what I have heard and read that I do not have enough knowledge.
We need training and a workshop on hepatitis B as a midwife because we must know what to do and what treatment aspects should be used, especially because we do not have any protocol or guidelines or any written protocol that guides what to do when handling pregnant women infected with hepatitis B virus.
Serological tests are performed for babies born to HBV-positive mothers after the completion of the HBV vaccination series or at least a month after the last hepatitis B dose, as documented by experts (Schillie et al., 2018; Woodring, Pastore, Brink, Ishikawa, Takashima & Tohme, 2019). Therefore, midwives need to refer pregnant women with a positive prognosis to specialists so that they can be evaluated for possible treatment. Otherwise, many more pregnant women who are eligible for treatment may not be treated, leading to an increased viral load and risk of HBV transmission to the foetus. The HBV status of HBV-exposed infants must be evaluated after HBV vaccination.
Discussion
This study sought to explore the factors affecting the successful implementation of the PMTCT program from the perspective of midwives. The participants in this study reported the presence of several intrinsic, client, and health facility factors that have negative effects on their efforts to prevent mother-to-child transmission of HBV.
In this study, some participants had misconceptions about the mode of transmission and treatment options available for pregnant women with HBV. These findings agree with other studies that reported unsatisfactory knowledge of HBV among healthcare personnel (Adjei et al., 2022; Belete et al., 2022; Chen et al., 2018; Freeman, Chea & Shobayo, 2023). Specifically, some of the participants believed that sweat was a medium for the transmission of HBV, contrary to what was reported by Schillie et al. (2018). The majority of the midwives in this study were not aware that pregnant women infected with HBV could be treated with NAs such as entecavir and tenofovir alafenamide based on their viral load during pregnancy, as recommended by the WHO (WHO, 2020a, 2022b). These findings are similar to previous reports demonstrating a lack of knowledge and awareness of treatment modalities for pregnant women infected with HBV (Djaogol et al., 2019). Moreover, there are available treatment options for pregnant HBV patients, and these preparations are effective at reducing the viral load and preventing the vertical transmission of HBV(Chen et al., 2022; Lee, Bang & Lee, 2021; WHO, 2020a, 2022b). The lack of knowledge on treatment demonstrated by participants in this study has implications for the care and treatment of women infected with HBV and, most importantly, the link between testing and treatment. Although midwives in Ghana may not be able to prescribe drugs for HBV-positive mothers who may need treatment, knowledge of the available treatment options will allow midwives to act as advocates for pregnant women who need linkage to care and support them in adhering to their treatment regimen.
Most of the midwives in the study were aware of the HBV vaccination and had confidence in the safety and efficacy of the vaccine for PMTCT. However, the financial challenges of their clients have served as major obstacles to the timely and effective use of the HBV vaccine and HBIG as postexposure prophylaxis measures to prevent disease transmission to newborns. According to the midwives, most mothers cannot afford HepB-BD or immunoglobulin. This is because, in Ghana, HepB-BD is not integrated into the expanded immunization program, as is the case in other countries and as recommended by the WHO (Awuku & Yeboah-Afihene, 2018; Moturi et al., 2018; WHO, 2022a). Hence, Ghanaian mothers with HBV-exposed newborns must make arrangements to purchase the HBV vaccine for use as postexposure prophylaxis. Furthermore, some pregnant women are unable to afford the fee for HBV screening even though it has been subsidized under the National Health Insurance Scheme. These challenges may prevent pregnant women from being screened for HBV and their exposed newborns from receiving appropriate postexposure prophylaxis. These findings agree with previous studies, which revealed that the high cost of hepatitis B screening and vaccination is detrimental to HBV prevention strategies (Adjei et al., 2023; Djaogol et al., 2019; Olakunde et al., 2023; Paul, Marie & Bechem, 2017). The high cost of HBV testing and vaccination with HepB-BD may negatively impact the successful implementation of the PMTCT program in the facility.
Participants in the present study further reported difficulties obtaining access to the HBV vaccine and immunoglobulin. This is because, in Ghana, HBIG and monovalent HBV vaccines are not stocked in all health facilities (Senoo-Dogbey et al., 2023). The HepB-BD and HBIG are acquired through middlemen who may not be reached or may not be able to deliver the vaccine on time when needed. These issues can affect the successful implementation of the PMTCT program. These findings agree with reports that indicate that the unavailability of vaccines, limited vaccination hours, lack of institutional mechanisms available to deliver vaccines at birth, vaccine stockouts, and high cost of vaccines hinder the PMTCT program (Adjei et al., 2023; Gera et al., 2019). The difficulties in obtaining HepB-BD and HBIG may affect the timely administration of the vaccine to HBV-exposed newborns, and this defeats the overall goal of the PMTCT program.
The study further revealed that the unavailability of logistics poses a great challenge to the successful implementation of the PMTCT program. According to the participants, the unavailability, frequent shortages, or stockouts of HBV RDTs for screening are major challenges. Midwives admitted needing RDTs at the antenatal clinic and labor wards, especially for the screening of non-attendants who reported only when they were in labor. This challenge may result in pregnant women not being tested, thereby increasing the risk of vertical transmission of HBV. These challenges were also documented by studies in southwestern Uganda (Mugisha et al., 2019) and rural Fatick in Senegal (Djaogol et al., 2019), where there were problems with diagnostic resources that affected the screening and treatment of pregnant women infected with HBV.
Participants in this study reported the unavailability of written protocols in their facilities regarding PMTCT for HBV. This, according to the participants, affects their practice. One major study performed in Africa reported the absence of standard clinical guidelines for standardizing HepB-BD implementation and HBV management in health facilities (Moturi et al., 2018).
The current study revealed that midwives did not receive in-service training on PMTCT for HBV. The participants in this study attributed the inadequate knowledge of treatment for pregnant women infected with HBV to the lack of continuous professional development on PMTCT. According to the participants, the little knowledge they have about is what they read on the internet. These findings are in line with the findings of studies from African countries suggesting that a lack of training opportunities for HCWs on HBV is a major challenge (Moturi et al., 2018; Olakunde et al., 2023). The implication is that midwives may not be updated with current trends in the prevention, care, and management of pregnant women with hepatitis B, and this has negative effects on the entire PMTCT for the HBV program.
Strength and Limitations
One strength of this study was the use of a qualitative design, which allowed for unstructured individual interviews. This method allowed for open responses, leading to rich data on the real-world experiences of midwives who are critical stakeholders in the PMTCT program. This study's limitation lies in the fact that the study was limited to midwives and did not include other categories of healthcare providers, which made the findings of the study one-sided.
Implications for Nursing and Midwifery Practice
In addition to self-motivation and commitment to providing care and support to pregnant women infected with HBV, midwives need periodic training and continuous professional education to update their knowledge on HBV transmission mechanisms and treatment options available for pregnant women infected with HBV. Midwives in all levels of care, especially in resource-constrained settings, need to be fully resourced with RDT kits to be used to screen all women during the antenatal period and even during labor. The availability of HBIG in facilities will reduce missed opportunities and delays in providing postexposure prophylaxis to HBV-exposed newborns. The implementation of the HBV birth dose vaccine policy and its integration into the expanded immunization program is urgently needed to relieve mothers’ financial burdens associated with arrangements for birth dose vaccines for their exposed newborns.
Conclusion
The study revealed that midwives face many challenges, and these challenges negatively impact the successful implementation of PMTCT for the HBV program. The inherent factors of midwives, such as unsatisfactory knowledge of treatment options for pregnant women with HBV, have been identified as major challenges. Other factors outside the control of the midwife were identified, including client factors, issues with logistics, unavailability of protocols, and, most importantly, lack of training for midwives. All these issues need to be urgently addressed to facilitate the effective implementation of the PMTCT program. In highly endemic HBV settings where MTCT accounts for many new infections among children under 5 years of age, the World Health Organization's target of reducing the prevalence of HBV infection to less than 1% among children under 5 years of age will not be achieved if these challenges are allowed to triumph.
Footnotes
Acknowledgements
We acknowledge the midwives who participated in the study.
Author Contribution Statement
AAM the conceptualization of the study. The manuscript writing was done by AAM, FN, CAA, and VSD. All the authors read the final manuscript.
Data Availability Statement
Data for this study would be available upon reasonable request from the principal investigator.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Consent to Participate
Ethics approval was obtained from the Ghana Health Service Ethics review committee (GHS-ERCO48/11/19). Informed consent was obtained from each participant with an assurance of anonymity and confidentiality.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.