
Abstract
Introduction
The increased prevalence of patients with heart failure urges the need to examine the current evidence on educational interventions conducted to foster self-care behaviors, thus, guiding best practices and identifying existing gaps in advance patient- centered care. This integrative review, guided by the Middle-Range Theory of Self-Care, aimed to synthesize the current evidence regarding the impact of educational programs on self-care behaviors among patients with heart failure.
Methods
An integrative review was conducted in accordance with the Joanna Briggs Institute (JBI) methodology. Seven electronic databases (PubMed, CINAHL, Scopus, Web of Science, PsycINFO, EMBASE, and the Cochrane Library) were searched for studies published between 2009 and 2025. Eligibility criteria were applied using the Population, Concept, Context framework. Data extraction, quality appraisal utilizing JBI critical appraisal tools, and thematic synthesis were executed systematically.
Results
Thirty-four studies that met specific criteria were included in the final analysis. The studies found that educational programs demonstrated a positive influence on self-care behaviors and quality of life among patients with heart failure, leading to reductions in hospital admissions and mortality rates. Nurse-led and technology-assisted interventions, such as telenursing and mobile-based education, further enhanced patient engagement in self-care practices.
Conclusion
Structured educational programs are crucial for improving self-care behaviors in patients with heart failure and need to be integrated into the routine clinical practice. Future research that investigates the long-term effects of these interventions on patient outcomes is recommended.
Introduction
Heart failure (HF), a complex syndrome resulting from structural or functional abnormalities of the heart, leads to insufficient cardiac output for the body's needs (Schwinger, 2021). This escalating global health issue is estimated to affect 64.34 million people, accounting for approximately 8% of the world's population (Savarese et al., 2022). HF imposes a substantial economic burden; it costs approximately $346 billion annually worldwide (Bergamasco et al., 2022). The prevalence of HF is projected to increase to 9.81 per 1,000 people by 2030, driven by an aging global population, lifestyle changes, and, in some regions, limited access to preventive care (Liu et al., 2024).
Beyond its physical manifestations, HF significantly diminishes patients’ quality of life (QoL). Recurring symptoms such as breathlessness, fatigue, and swelling restrict daily activities and increase reliance on healthcare services (Johansson et al., 2021). This chronic condition is strongly linked to high mortality rates, frequent hospital readmissions, and a poor QoL (Savarese et al., 2022). Physical symptoms are often compounded by psychological issues, including depression and anxiety, which can hinder overall health outcomes and self-care practices (Al-Sutari & Abdalrahim, 2024; Chernoff et al., 2022). HF also negatively impacts social connections, reduces physical activity, and impairs self-management (Salahodinkolah et al., 2020). Furthermore, the financial burden of medication costs, frequent medical visits, and lost productivity can further worsen patients’ overall well-being (Kitko et al., 2020).
HF is an increasing health concern, partly due to insufficient patient education (Saifan et al., 2024). Addressing this issue requires a multidimensional approach that actively involves patients in managing their disease to optimize outcomes. This approach, known as self-care (Sedlar et al., 2021). Self-care maintenance specifically involves preventing complications and preserving psychological well-being (Jaarsma et al., 2021), while self-care management focuses on addressing symptoms as they emerge (Martínez et al., 2021).
Effective HF management hinges on robust self-care practices, which include strict medication adherence, vigilant symptom monitoring, dietary modifications, and regular physical activity (Jaarsma et al., 2021; Niriayo et al., 2024). However, several factors often impede patients’ ability to engage in self-care, such as cognitive decline, low health literacy, and insufficient social support (Niriayo et al., 2024). Therefore, patient education is crucial for effective HF management (Dizdarevic-Hudic et al., 2025). Leading health organizations, including the ESC, HFSA, and ACCF/AHA, all underscore the importance of individualized education centered on self-care (Puspitawati & Widani, 2024). Planned, structured, and patient-centered educational programs have consistently demonstrated improvements in self-care practices among HF patients (Okazaki et al., 2024).
Recent scholarly work consistently underscores the pivotal role of self-care in enhancing outcomes for individuals with HF. For instance, Stahlman et al. (2023) demonstrated that an in-person educational class for HF patients significantly improved patient confidence and self-management ability, leading to a notable reduction in emergency department visits and hospital admissions, with readmissions dropping from 96% to 35% in the 90 days following the class. Also, studies demonstrated a clear association between heightened self-care confidence and reduction in hospitalizations and mortality rates, improvement of medication adherence and symptom monitoring across diverse patient cohorts (Jaarsma et al., 2021; Dessie et al. (2021). A randomized controlled trial (RCT) by Vellone et al. (2022) further revealed that integrating nurse-led education with telemonitoring substantially enhanced self-care behaviors and decreased emergency department visits. Furthermore, a scoping review by Madujibeya et al. (2022) indicated that Health interventions hold promise for improving self-care and knowledge, despite inconsistencies in engagement metrics. Collectively, these studies underscore that multimodal, technology-supported educational strategies particularly those delivered by nurses and augmented via mobile platforms effectively enhance self-care behaviors, reduce hospitalizations, and boost confidence among HF patients. This robust evidence reinforces the rationale for this review's focus on synthesizing the impacts of educational programs on self-care, QoL, and clinical outcomes in HF. Thus, the review involved a wide range of years (2009–2025) to capture the most recent and relevant studies reflecting contemporary practices and developments in this field, thereby allowing us to critically evaluate the impact of educational programs and the diversity of strategies used.
Despite the established importance of patients’ education, gaps remain concerning the optimal content, delivery methods, and sustainability of educational programs designed to enhance self-care among HF patients. This is particularly true given emerging technologies and diverse healthcare settings. Seminal work by Barbara Riegel and Ercole Vellone on the Middle-Range Theory of Self-Care of Chronic Illness underscores the multidimensional nature of self-care. This theory posits that self-care involves both maintaining health through prevention and symptom monitoring (self-care maintenance) and responding appropriately to symptoms when they occur (self-care management) (Riegel et al., 2022; Vellone et al., 2019).
Given the increasing prevalence of HF and the critical role of education in supporting self-care behaviors, there is a clear need to synthesize current evidence on educational interventions. This synthesis can help in guiding best practices and inform the development of future programs.
Therefore, this integrative review aims to synthesize existing research on the impact of educational programs on self-care behaviors among patients with HF. Thus, this helps identify effective strategies and existing gaps to advance patient-centered care in HF management.
Methods
Design
An integrative review approach was used. The use of integrative review allows broad and flexible exploration of emerging topics such as self-care behavior of patients with HF, opposing the systematic review which mostly narrow and rigid design (Cronin & George, 2023). The review was conducted in accordance with the Joanna Briggs Institute (JBI) methodology for systematic and integrative reviews (Aromataris et al., 2024). This framework guided the study process in appraising the quality of the studies and systematically synthesizing the evidence.
Search Strategy
A robust search strategy, developed in consultation with the JBI Manual for Evidence Synthesis (Aromataris et al., 2024), was executed to identify relevant literature. A comprehensive search was performed from February to June 2025 across seven major electronic databases: PubMed, CINAHL, Scopus, Web of Science, PsycINFO, EMBASE, and the Cochrane Library. To ensure a thorough search, a combination of keywords and subject headings was used, including terms such as “heart failure,” “educational programs,” “self-care behaviors,” “patient education,” and “hospital readmission.” This approach allowed for the capture of a wide array of interventions aimed at improving self-care practices. Additionally, to minimize the risk of missing relevant studies, the reference lists of all included articles were manually screened for any other articles that met the review's inclusion criteria.
Inclusion/Exclusion Criteria
To identify relevant studies, seven electronic databases were thoroughly searched, focusing specifically on primary research that examined how educational programs influence self-care behaviors in patients with HF. Any study reporting findings on the impact of educational interventions—whether structured, semi-structured, or technology-assisted—on any aspect of self-care was included. This encompassed outcomes such as patients’ adherence to medications, symptom monitoring, dietary management, and engagement in physical activity. To minimize selection bias and ensure accuracy, two independent reviewers screened and extracted all data.
The main research question for this literature review was developed using the Population, Concept, Context framework, a model well-suited for synthesizing diverse evidence. The framework was defined as follows: the Population includes adults with HF; the Concept centers on educational programs and their impact on self-care behaviors; and the Context is any healthcare setting or community. Based on this structure, the research question was: “What is the impact of educational programs on self-care behaviors and health outcomes among adults diagnosed with HF across various healthcare settings?”
The inclusion criteria for the selection of studies were: (1) Original empirical research; (2) were published in the English language between 2009 and 2025; (3) involved adult patients diagnosed with HF; and (4) examined the effects of educational programs on self-care behaviors or related health outcomes. The timeframe of 2009–2025 was selected to capture the modern era of HF management and the evolution of contemporary self-care educational interventions (Heidenreich et al., 2022). This period ensures a robust sample size for analysis while reflecting practices aligned with current clinical standards. To maintain methodological rigor and ensure the inclusion of high-quality, validated evidence, gray literature (including dissertations) was excluded, along with reviews, editorials, and commentaries.
Selection of the Studies
For this integrative review, the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guidelines was followed (Parums, 2021). This helped in ensuring transparency of the review and made the process easily reproducible (Page et al., 2021). Ultimately, this comprehensive approach allowed us to thoroughly evaluate the existing evidence to determine the effectiveness of educational programs in improving self-care behaviors among individuals living with HF. The final protocol was formally registered on July 9, 2025, with the Open Science Framework (OSF), and you can find it under the registration https://doi.org/10.17605/OSF.IO/UTGWJ
Quality Appraisal Process
The JBI Critical Appraisal Checklists for QuasiExperimental and Qualitative Studies were applied to evaluate study rigor and identify potential bias (Aromataris et al., 2024). Each article received an overall methodological quality score, which was verified by a second independent reviewer to ensure consistency. Discrepancies were discussed and resolved, strengthening the reliability and transparency of the appraisal process.
Data Extraction and Synthesis
Two independent reviewers meticulously extracted data from all eligible studies. They utilized a predeveloped, standardized forms to ensure consistency and minimize any potential extraction bias. The information extracted included key study characteristics such as the author(s), publication year, country, study design, sample size, and settings. Details were recorded about the type and content of the educational program, the intervention's duration, and the follow-up period. Furthermore, documentation of the measurement tools and any reported changes in self-care outcomes after the intervention were critically reported. Any discrepancies that arose between the two reviewers were resolved through discussion until consensus reached.
For this integrative literature review, a thematic analysis approach was adopted for data synthesis. Studies were grouped and summarized based on their intervention type and their measured outcomes. This allow effectively capture both variations and consistencies across the different studies. This synthesis facilitated a qualitative comparison of the effectiveness of various educational interventions, while allowing diversity in the reviewed studies populations and intervention modalities used (whether face-to-face, group-based, or technology-assisted). Also, transparently, the clinical heterogeneity found across the studies were reported (Page et al., 2021) to ensures the credibility and reliability of the findings, ultimately providing a clear understanding of the current evidence regarding the effect of educational programs on self-care behaviors among patients with HF.
Ethical Consideration
There are no human participants in this article and informed consent is not required.
Results
The initial search efforts yielded a total of 470 studies where the specified search terms appeared in either the title or abstract. After diligently removing duplicate entries found across the various databases we searched, 200 studies were excluded. The remaining studies then underwent a thorough title and abstract screening to assess their relevance to the population of interest and to confirm their focus on educational programs targeting self-care behaviors among patients with HF. During this critical stage, 236 studies were excluded because they either didn't meet the inclusion criteria or lacked alignment with the core themes of the study. This rigorous process ultimately resulted in 34 studies being identified as eligible for full-text screening and subsequent inclusion in this integrative review. For a visual representation of how studies were identified, screened, excluded, and finally included in this review, please refer Figure 1.
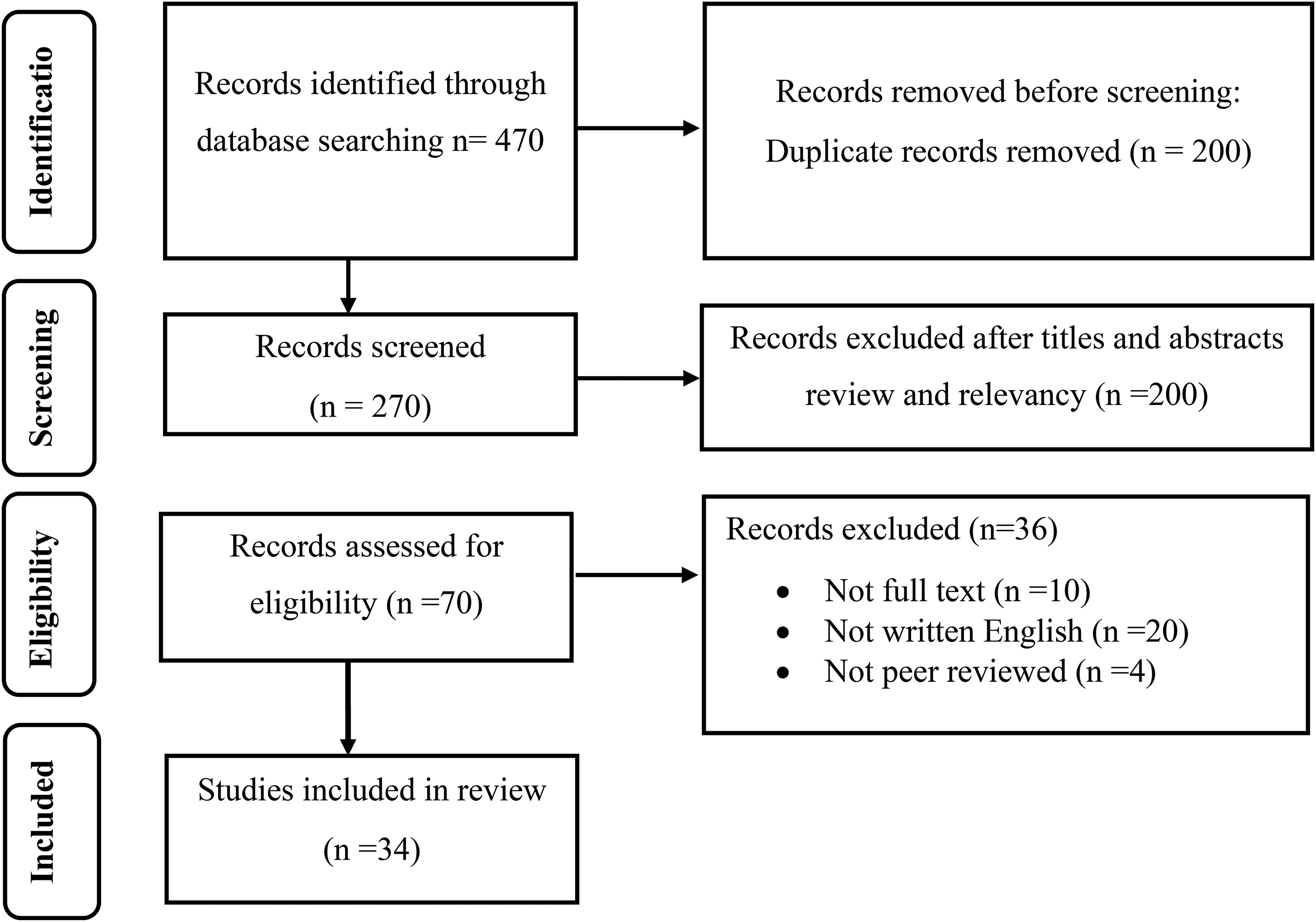
Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) Flow Diagram.
Characteristics of the Studies
A total of 34 studies were included in this integrative review. The main characteristics of the studies are summarized in detail in Table 1. These studies represented diverse geographic locations, including Lebanon, China, the United States, Iran, Colombia, Suadi Arabia, Tiwan, Vietnam, Australia, Japan, Jordan, Ethiopia and Spain (Table 1). The study designs encompassed RCTs, quasiexperimental studies, and observational studies. The studies were also conducted in a diverse range of settings, from outpatient HF clinics and community health centers to hospital-based cardiac units. Sample sizes across these studies ranged from as few as 45 participants to as many as 600. Most studies focused on adult patients diagnosed with HF, typically aged between 50 and 79 years.
Literature Review Matrix.

Note. HF = heart failure; RCT = randomized controlled trial; QoL = quality of life.
The educational interventions were quite varied, including structured face-to-face sessions, group-based education, home visits, and even technology-assisted programs delivered via telephone, video conferencing, or mobile applications. The duration of these interventions also differed, ranging from single-session education to programs that extended over six months, with follow-up periods ranging from immediate post-intervention assessments to evaluations conducted 12 months later.
Across all the studies, the educational programs generally covered key areas such as medication adherence, symptom monitoring, dietary modifications, physical activity, fluid management, and the early recognition of exacerbation symptoms. It's worth noting that several studies also incorporated individualized goal-setting and involved caregivers to further enhance self-care practices. This diversity in both intervention delivery methods and follow-up durations allowed us to conduct a truly comprehensive evaluation of how educational programs impact self-care behaviors among patients with HF.
Quality Appraisal of the Review
The analysis and synthesis were guided by the JBI methodology to integrate current evidence regarding the impact of educational interventions on medication adherence, symptom monitoring, dietary management, physical activity, and hospital readmission. Across the reviewed studies, structured educational programs—whether delivered individually, in groups, or via technology—were significantly associated with improved self-care behaviors and enhanced patient self-efficacy. Furthermore, several studies identified a reduction in hospital readmissions and improvements in QoL. These findings highlight the critical role of integrating educational programs into routine HF care to optimize clinical outcomes.
Methodological Quality Methodological quality was assessed using the JBI Critical Appraisal Checklists for QuasiExperimental and RCTs (Barker et al., 2024). Two reviewers independently evaluated each study, with a third reviewer resolving discrepancies. The assessment prioritized study design appropriateness, inclusion clarity, outcome reliability, confounding management, and follow-up completeness. Based on these criteria, nine studies were classified as high quality, 22 as moderate quality, and three as low quality.
Most included studies strengthened internal validity by clearly reporting randomization or systematic allocation. However, common limitations included the lack of allocation concealment, which introduces potential selection bias, and inconsistent blinding of outcome assessors. This lack of blinding may have influenced subjective self-care ratings. Additionally, while technology-assisted interventions generally exhibited lower risks of bias due to standardized protocols, smaller quasiexperimental studies frequently carried a moderate risk of bias, often stemming from nonrandomized designs and incomplete reporting of attrition. Despite these limitations, the high-quality RCTs included in this review provide robust evidence supporting the efficacy of educational interventions.
The Results Themes
Theme1: Effect of Educational Programs on Patients’ QoL
Most studies reported positive effects of educational programs on the QoL of patients with HF. For instance, two RCTs conducted in Iran demonstrated significant QoL improvements in intervention groups of 35 and 45 participants, respectively (Akbari et al., 2019; Khezerlou et al., 2025). Similarly, a US-based study involving a home-based program with memory enhancement components showed improved QoL specifically among younger patients with HF (Clark et al., 2015).
“Nonetheless, not all studies demonstrated sustained improvements. Some studies reported that improvements in QoL were maintained for only a few months after the intervention, followed by a significant decline in outcomes later in time (Al Shamsi & Chehade, 2019; Tung et al., 2013). The authors attributed this regression to the cessation of the intervention and the lack of continuous follow-up, noting that the withdrawal of professional support led to a gradual decrease in adherence to self-care behaviors.”
Theme2: Effect on Enhancing Patients’ Self-Care Management
Although the included studies span a 15-year period (2009–2024), the analysis reveals a consistent pattern regarding the effectiveness of educational interventions. Studies published during the earlier phase of this timeframe for example, Shojafard et al. (2009) were retained in the synthesis as they represent foundational evidence in the development of self-care interventions for HF. Crucially, these early findings established the efficacy of fundamental self-care principles that continue to inform contemporary practice trends and are supported by more recent data.
Across the reviewed literature, educational interventions consistently enhanced self-care behaviors. Reflecting the evolution of the field, these interventions were delivered through a range of modalities, spanning from traditional face-to-face instruction and interactive educational materials in earlier studies (Shojafard et al., 2009; Tung et al., 2013) to modern digital platforms (Al-Sutari & Ahmad, 2017; Dinh et al., 2018; Liou et al., 2015; Ramadan et al., 2024; Siabani et al., 2016).
Specific intervention models showed sustained efficacy over the review period. Hybrid models, digital education, nurse-led self-management programs, and motivational interviewing techniques were particularly effective in supporting self-care. This effectiveness was evident in foundational nurse-led research (Otsu & Moriyama, 2011) and was further corroborated in subsequent studies utilizing motivational and digital strategies (Dalir et al., 2016; Navidian et al., 2017; Wonggom et al., 2018).
Other studies emphasized the benefits of integrated approaches. For instance, Arredondo Holguín et al. (2012) demonstrated that a combination of group education, home visits, and telenursing significantly improved patients’ skills related to medication management and help-seeking. Similarly, more recent remote interventions that included direct provider support were also effective in enhancing patient engagement and symptom recognition (Chen et al., 2018).
Conversely, mixed outcomes were also reported regarding specific endpoints. For instance, while telenursing improved self-care behaviors in the study by Heidari et al. (2017), it had no significant influence on exercise tolerance. Additionally, regarding advanced technologies, Wonggom et al. (2020) observed that while avatar-based education enhanced knowledge, the resulting behavioral changes were inconsistent. Likewise, Gheiasi et al. (2017) found that family-involved education improved self-care, though results varied depending on individual patient engagement.
Theme3: Effect on Hospital Readmissions and Mortality Rates
Fewer studies directly addressed the effects of educational interventions on hospital readmissions and mortality, and their findings were heterogeneous. Some studies showed promising results; for example, digital education was associated with reduced hospital visits (Wonggom et al., 2018). However, other interventions demonstrated limited impact. Peyman et al. (2020) found that while a self-efficacy-based educational approach improved adherence, it did not significantly influence long-term hospitalization rates.
Similarly, Loghmani and Monfared (2018) concluded that while Orem's self-care model increased patient knowledge, its impact on hospital readmission rates remained inconclusive. The primary reason for this finding was the study's short duration (limited to one month of follow-up), which was insufficient to detect changes in long-term outcomes such as hospital readmissions. Furthermore, this underscores the complexity of HF management: readmission rates are influenced by multiple determinants—including disease progression, socioeconomic constraints, variable self-care adherence, and the lack of sustained clinical follow-up—which cannot be fully mitigated by education alone. Likewise, Liou et al. (2015) reported that video-assisted instruction coupled with telephone counseling improved self-care maintenance, yet no significant effect on hospitalization or mortality was observed.
Collectively, these findings suggest that while educational interventions are effective in improving self-care behaviors, their translation into reduced hospital readmissions and mortality may depend on factors such as intervention duration, follow-up intensity, and the personalization of content. Programs that incorporate continuous support mechanisms may be better positioned to achieve long-term clinical benefits.
Discussion
This integrative review evaluated the impact of educational programs on self-care behaviors among patients with HF, situating its findings within the Middle-Range Theory of Self-Care of Chronic Illness (Riegel et al., 2022). Consistent with this framework, structured educational interventions improve self-care maintenance, monitoring, and management, all critical components for optimal HF outcomes.
The findings align with recent systematic reviews that demonstrate the effectiveness of self-care interventions in improving adherence and reducing hospital readmissions among patients with HF (Vellone et al., 2022). Incorporating structured education into routine care can enhance patient confidence and disease management capabilities, reinforcing prior findings that self-care confidence may be more important than cognition in preserving functional status in HF patients (Riegel et al., 2022).
Notably, this review identified variability in educational program delivery methods, including traditional in-person sessions, group education, and emerging digital and telehealth interventions. While traditional methods remain effective, recent evidence highlights the significant potential of digital health solutions, such as telemonitoring and mobile health applications, to support, empower HF self-care management and reduced perceived hospitalization rates (Pons Riverola et al., 2023; Madujibeya et al., 2023; Liu et al., 2022). However, the successful implementation of these technologies requires addressing various barriers related to patient digital literacy, a poor internet connection, healthcare provider integration, and system-level readiness (Whitelaw et al., 2021).
Despite promising results, the review highlights limited evidence regarding the long-term sustainability of educational interventions. Many studies lack the longitudinal follow-up necessary to evaluate the maintenance of self-care behaviors and their sustained impact on hospitalizations and mortality over extended periods (Madujibeya et al., 2023). Future research should prioritize longitudinal, theory-driven studies to assess the durability and effectiveness of educational interventions in diverse patient populations.
Furthermore, individualized and culturally tailored educational approaches, guided by theoretical frameworks such as the Middle-Range Theory of Self-Care, may significantly enhance patient engagement and adherence (Riegel et al., 2022). This personalization is crucial, especially when considering the variations in health literacy, socioeconomic status, and comorbid conditions that directly affect patients’ capacity to engage in effective self-care practices.
This integrative literature review clearly demonstrated that educational programs have a positive impact across multiple patient outcome domains for individuals living with HF. Regarding QoL, most of the reviewed studies reported significant improvements after participants engaged in educational interventions. For example, RCTs conducted in Iran (Khezerlou et al., 2025; Hosseini et al., 2023) and home-based programs (Widiastuti et al., 2025) all showed enhanced QoL among their participants. However, the sustainability of these gains was a bit more varied. Studies from places like Saudi Arabia (Alodhaib et al., 2025) and Vietnam (Nguyen et al., 2025) indicated that while initial improvements in QoL were seen, they weren't always consistently maintained over longer follow-up periods.
In terms of self-care management, educational interventions consistently boosted patient engagement in a range of self-care activities. These interventions were delivered in various ways—from traditional face-to-face sessions to modern digital and hybrid models. Interestingly, studies suggested that hybrid and nurse-led interventions (Mohamad, 2025; Longhini et al., 2023; Tao et al., 2023) were particularly effective at sustaining these behavioral changes. Approaches that incorporated motivational interviewing, involved family members, and offered direct support from providers were found to promote greater self-efficacy and confidence in self-care (Son et al., 2025; Dellafiore et al., 2023; Masterson Creber et al., 2023). Despite these positives, it was noticed that some mixed outcomes regarding the consistency of behavioral change; some interventions, for instance, improved knowledge but didn't always translate that knowledge into consistent lifestyle adjustments (Longhini et al., 2025; Tinoco et al., 2021).
The evidence on the impact of educational programs on hospital readmissions and mortality was more limited and showed greater heterogeneity (Vijaya Kumari et al., 2025). While some digital and self-efficacy-based interventions did demonstrate reductions in hospital visits (Oh et al., 2023; Huang & Chair, 2025), others showed only a limited influence on long-term hospitalization or mortality rates (Kinugasa et al., 2024; Hosseini et al., 2023). These inconsistencies suggest that while educational interventions were effective at enhancing self-care behaviors, translating that into reduced hospital readmissions and mortality might require longer intervention durations, more personalized content, and continuous follow-up support (e.g., telemedicine or mHealth monitoring) to sustain improvements and achieve those crucial long-term clinical benefits.
This integrative review extends existing knowledge on the care of patients with HF through offering a more nuanced synthesis that links methodological rigor with outcome variability and highlights the effectiveness of diverse educational strategies. Importantly, it draws attention to underexplored areas such as the sustainability of QoL improvements and implementing digital health solutions. By situating these findings within the Middle-Range Theory of Self-Care of Chronic Illness, this review not only reinforces existing evidence on the value of education but also advances it by emphasizing theory-driven, individualized approaches that provide a clear direction for future decisions.
Another important issue is to ensure equity and access that all the patients will have equal opportunity to benefit from the education and eliminating barriers to have access to the available resources taking into consideration their individual differences and abilities. These resources may include unbiased funding and support services to poor societies, thus promote a better educational arrangements for all (Naim, 2025). Equity in this context means addressing socioeconomic disparities, cultural and linguistic diversity, and varying levels of health literacy, so that no group is disadvantaged in receiving or applying self-care education. Access involves not only the physical availability of resources but also their affordability and adaptability to diverse patient needs. By prioritizing equity and access, healthcare systems can foster more effective and sustainable educational arrangements that empower all patients to engage in self-care.
Strengths and Limitations
This review has several significant strengths that make it a rigorous and valuable academic work. The methodological approach was grounded in established best practices, rigorously guided by the JBI and PRISMA standards. This ensured a systematic and reproducible process from the initial research development of the questions to the final synthesis of the findings. The commitment to transparency is further demonstrated by the review's registration with the OSF, a practice that enables public scrutiny and verification of the methodology. Another strength of this review lies in its integration with a theoretical framework. Using the Middle-Range Theory of Self-Care as a conceptual lens allowed for a meaningful synthesis of the findings, providing a deeper understanding of the mechanisms through which educational programs influence patient behavior. Furthermore, the comprehensive nature of the search strategy served as a key strength, allowing for the inclusion of a wide range of studies and providing a broad, encompassing overview of the available evidence on self-care education for patients with HF.
Despite these strengths, certain limitations warrant consideration. The search strategy did not include studies on the education of family members, which is a crucial aspect of self-care behavior due to the significant influence of family support in chronic conditions such as HF. where patients often rely on relatives for emotional support, daily management, and decision-making. Excluding this factor may have overlooked valuable insights into how education directed at family members can enhance patient outcomes. By not incorporating this body of evidence, the review may have provided only a partial understanding of the broader context of self-care
Additionally, the overall comprehensiveness of this review may be impacted by several methodological constraints. These include the exclusion of some full-text studies due to unavailable access, the reliance on English-only literature, and the inherent heterogeneity of the interventions and outcome measures. Furthermore, the predominance of moderate-quality studies and the potential for publication bias (where positive findings are more likely to be published) warrant caution in interpreting the results.
Conclusion and Implication for Practice
This review highlights that knowledge gaps and behavioral challenges remain major barriers to effective self-care in patients with HF. Tailored educational interventions—particularly nurse-led programs—are essential to strengthen patients’ confidence, adherence, and symptom management, ultimately reducing hospitalizations and mortality.
Collectively, the findings offer relevant evidence for healthcare providers, policymakers, and those developing patient education programs that enhance self-care practices among patients with HF. Particularly, nurse-led interventions are encouraged to design strategies through utilizing their expertise to teach patients with HF self-care management techniques in different health care facilities. These interventions may include innovative approaches and services aim at empowering patients’ abilities and confidence to improve health outcomes. In this regard, it is recommended to establish the creation of nurse-led units in each hospital to carry out these interventions mainly early discharge planning programs.
Overall, ensuring equity and access across diverse settings requires interdisciplinary collaboration and policy support. Future research should build stronger evidence for nurse-led units and innovative educational strategies that empower patients and sustain long-term health outcomes.
Supplemental Material
sj-docx-1-son-10.1177_23779608251410981 - Supplemental material for The Effect of Educational Programs on Self-Care Behaviors Among Patients with Heart Failure: An Integrative Literature Review
Supplemental material, sj-docx-1-son-10.1177_23779608251410981 for The Effect of Educational Programs on Self-Care Behaviors Among Patients with Heart Failure: An Integrative Literature Review by Nedal F. Abu Jasser, Ferial A. Hayajneh and Maysoon S. Abdalrahim in SAGE Open Nursing
Supplemental Material
sj-docx-2-son-10.1177_23779608251410981 - Supplemental material for The Effect of Educational Programs on Self-Care Behaviors Among Patients with Heart Failure: An Integrative Literature Review
Supplemental material, sj-docx-2-son-10.1177_23779608251410981 for The Effect of Educational Programs on Self-Care Behaviors Among Patients with Heart Failure: An Integrative Literature Review by Nedal F. Abu Jasser, Ferial A. Hayajneh and Maysoon S. Abdalrahim in SAGE Open Nursing
Footnotes
Acknowledgment
The authors would like to thank the University of Jordan for providing resources such as e-Library and access to full-text articles.
Ethical Approval and Informed Consent Statements
Ethical approval and informed consent were not required for this study, as it is an Integrative literature review of previously published literature.
Authors Contributions
All authors contributed to the study conception and design. Material preparation and data collection were performed by NA, Data analysis and results were performed by MA and FH. Writing the manuscript first draft and shared in the analysis and discussion were performed by MA and NA. The final version of the manuscript was written by NA. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data available when required from the journal.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.