
Abstract
Background
Nursing workload is largely studied but poorly explored under physical, mental, and emotional dimensions. Currently, only a limited number of variables have been linked to nursing workload and work contexts.
Purpose
The study aimed to investigate whether it is feasible to identify variables that consistently correlate with nursing workload and others that are specific to the context.
Methods
We employed a descriptive correlational analysis and a cross-sectional design. Data were collected through a survey distributed to registered nurses working across Italy, at the conclusion of randomly assigned morning or afternoon shifts.
Results
We received 456 surveys from 195 shifts, collected from nurses in four public and two private hospitals. Commonly associated variables with nursing workload dimensions included patient complexity of care, admission/discharge or transfer, informing patients/relatives, contacting physicians, and unscheduled activities. Variables categorized as setting-specific were patient isolation and specialties, nurse-to-patient ratio, adequacy of staff in the shift, peer collaboration, healthcare documentation, educating others, and medical urgency.
Conclusions
In summary, certain variables consistently correlate with nursing workload across settings, while others are specific to the context of care. It is imperative for nurses and nurse managers to measure the nursing workload in various dimensions, enabling the prompt implementation of improvement actions.
Keywords
Introduction
In recent years, healthcare organizations have been facing various challenges related to the complexity of care, including the growth of chronic and communicable diseases, technological advancements, resource shortages, and staff retention issues (WHO, 2020). The challenges require continuous transformations, leading organizations to strike a balance between cost savings and the delivery of high-quality care (WHO, 2018). Organizational decisions and ongoing transformations significantly impact healthcare professionals’ work activities, specifically putting nurses under noteworthy pressure to fulfill their caring roles (Navajas-Romero et al., 2020; Van den Oetelaar et al., 2021).
Working conditions are the major drivers of employment attractiveness, performance, productivity, and retention of the health workforce (WHO, 2021). Therefore, in an era of nursing shortage and expanding nursing scopes of practice, it is necessary to empower the present nursing workforce and uphold decent working environments to guarantee acceptable workloads (Ivziku, Ferramosca, et al., 2022), productivity, and quality of care (WHO, 2018), as well as improve the patient experience (Gualandi et al., 2021).
Review of the Literature
For more than four decades, scholars have persistently studied nursing workload and attempted to identify classification systems to measure it (Hoogendoorn et al., 2020). Despite the great variation of nurses’ work activities in hospital settings, some common factors have been thoroughly explored in nursing research, seeking to understand their influence on nursing workload. However, the findings are of moderate validity and reliability (Hoogendoorn et al., 2020) and nursing workload remains a critical topic in nursing literature (Ivziku, Ferramosca, et al., 2022).
Nursing workload is defined as ‘the amount of time and care that a nurse devotes (directly and indirectly) to patients, the workplace, and professional development’ (Alghamdi, 2016). Increased nursing workloads have been associated with reduced quality of care and patient satisfaction, as well as omitted care and higher patient safety risks (Alrabae et al., 2021; Copanitsanou et al., 2017; Pereira Lima Silva et al., 2020). Nursing workloads also have negative effects on nurses’ well-being, such as increased stress, emotional exhaustion, and absenteeism (Copanitsanou et al., 2017; Pereira Lima Silva et al., 2020). Additionally, they can lead to reduced job satisfaction, performance, and engagement, while also increasing turnover intentions among nurses (Copanitsanou et al., 2017; MacPhee et al., 2017; Pereira Lima Silva et al., 2020).
Among the factors that affect nursing work and increase workloads in acute care settings, multiple demands of patient care (Aiken et al., 2021; Ivziku, De Maria, et al., 2022), the quality and quantity of human resources (Ivziku, De Maria, et al., 2022; Jones et al., 2015; Moloney et al., 2020; Pereira Lima Silva et al., 2020), poor working environments (Ferramosca et al., 2023; Pereira Lima Silva et al., 2020), disorganized workplaces (Ferramosca et al., 2023; Jennings et al., 2022), and time and task allocation (Michel et al., 2021) were determined. Identifying and correcting disturbances in nurses’ work and leveraging stress factors can help buffer the negative work experience and workloads in nurses (Moloney et al., 2020). Therefore, further studies that continue to document challenges in nurses’ work and provide strong evidence on the determining factors are needed.
With the intention of contributing to increased knowledge on nursing workload in acute care settings, this research team is exploring the phenomenon and trying to identify antecedents of general (Ivziku, Ferramosca, et al., 2022), as well as physical, mental, and emotional dimensions of workload in nurses working in medical and surgical wards (Ferramosca et al., 2023; Ivziku, De Maria, et al., 2022). Present findings indicate that in work contexts, aspects related to nursing staffing and skill-mix, patient complexity, number of specialties, or nurse-to-patient ratio, as well as work process aspects regarding work organization and workflow, unscheduled activities, healthcare documentation, or patient isolation may influence nurses’ perceptions regarding shift workloads (Ferramosca et al., 2023; Ivziku, Ferramosca, et al., 2022; Ivziku, De Maria, et al., 2022). What is not yet clear in the literature is whether there is a definitive set of determinants of nursing workload, which are common across different work settings or specific to the context of care.
Therefore, in this study, the authors aim to describe aspects associated with physical, mental, and emotional nursing workloads that are distinguished for specific work settings and identify common factors across them.
Materials and Methods
Design
In this study, a cross-sectional descriptive design was used. The descriptive design is well suited for an initial understanding of commonalities or differences between work settings and nurse perceptions regarding dimensions of workload and identifies relationships to explore in future research on the phenomenon. The research followed the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) Guidelines for observational studies (von Elm et al., 2014)
Theoretical Framework
The guiding theory for this study was the job demand-resources (Bakker & Demerouti, 2017). Job demands encompass factors such as time pressure, exposure to stressful or traumatic situations, conflicting demands from clients or teams, adverse environments, or staffing constraints. These aspects require sustained effort and are linked to physiological and psychological effects. Job resources encompass supportive work environments, access to essential equipment and technology, support from supervisors and coworkers, well-organized work tasks, opportunities for high-quality work, autonomy in decision-making, recognition for achievements, and professional development opportunities. These resources assist workers in managing job demands and fostering psychological well-being. When job resources surpass job demands, employees are prone to experiencing positive outcomes like job satisfaction, engagement, and commitment to their work. Conversely, an imbalance where job demands surpass available resources can result in stress, burnout, and decreased job performance (Bakker & Demerouti, 2017).
The JD-R theory has been applied across a range of healthcare work settings and in nursing (Broetje et al., 2020; Van Veldhoven et al., 2015). By evaluating demands and resources not only at the individual level but also at the team and organizational levels, healthcare organizations can use this theory to identify areas for improvement within their work environments and implement interventions to support employee well-being and job satisfaction.
Setting and Participants
This study involved registered nurses working in thirteen medical-surgical wards across six teaching hospitals located in the southern, central, and northern regions of Italy. Hospitals were chosen based on convenience, and nurse executives from various hospitals were contacted and invited to participate in the research. To ensure the representativeness and diversity across the different hospitals and regions, each participating center was requested to designate one medical and one surgical ward for inclusion in the research. A purposive sampling strategy was used to select the wards. To be included in the study, the wards should assist major surgery and general medicine patients, while excluding wards dedicated to COVID-19 infected patients.
All registered nurses working in the included wards were invited to participate in the study. The research aimed to identify determinants of nursing workload. Therefore, only full-time registered nurses who were directly involved in patient care and had been working in the ward for at least 2 months were included in the study. Float nurses and nurses working extra time or additional shifts were excluded. The exclusion rationale is linked to the risk of bias in perceived workloads resulting from additional work. Float nurses were excluded because they may not be familiar with the ward characteristics, potentially leading to increased demands and searches for materials or questions regarding team communication. Among the 269 eligible nurses, 174 consented to participate in the study.
Data Collection
At the beginning, the researchers approached the nurse executives of the six hospitals and the nurse managers of the thirteen selected wards to explain the aims of the research and seek their approval for participation in the study. Subsequent meetings were conducted to reach all nurses working in the wards and explain the study's purpose and their potential involvement.
Specifically, registered nurses were invited to complete a self-administered survey about their workloads at the end of a randomly chosen working shift, either in the morning or afternoon, over three consecutive weeks during the period of February 2021-June 2023. Nurses received a Google Forms link in their institutional email. The survey platform was easily accessible via various devices and web browsers. The estimated completion time for the survey was 10–15 min, ensuring data security and confidentiality throughout the survey process. Each participant was assigned a unique numeric code for survey completion, and nurses had the freedom to decide whether or not to participate in the survey.
Instruments
Data were collected with an online survey composed of three sections: demographic data, shift dynamics information, and nursing perceptions regarding workload aspects.
In the first section of the survey, nurses were asked to provide general information about their sex, age, work experience, the ward they worked in, and the shift they worked, using both open-ended and multiple-choice items.
In the second section, to assess shift aspects influencing the nursing work, nurses were asked to provide information about the number of patients cared for during the shift, the different medical specialties, and number of patients in isolation taken care during the shift. These aspects were measured using open-ended items. Further shift-related aspects were explored including the patient complexity of care, the adequacy of staffing, skill-mix, and collaboration with colleagues during the shift, engagement in patient transport or admission/discharge, giving information to patients/relatives, searching for the physician, educating new nurses, students or other staff, unscheduled activities, medical urgency, and healthcare documentation. These aspects were measured with multiple-choice single items with a 4-point Likert scale, ranging from 0 (not appropriate/no engagement) to 4 (completely appropriate/high activity engagement). The use of single-item measurements is recommended in the literature when evaluating a specific construct (Williams & Smith, 2016).
In the third section, nurses were able to respond to questions regarding workload. To measure the general perception of workload perceived in the shift we asked nurses to report on a 5-point Likert scale from 0 (very high workload) to 4 (no workload) for the level of workload perceived during the shift worked.
To measure physical, mental, and emotional nursing workloads we used three scales from the Questionnaire on the Experience and Evaluation of Work (QEEW 2.0) © SKB questionnaire (Van Veldhoven et al., 2015).
The physical workload was measured with the Pace and Amount of Work scale, which consists of six items rated on a 4-point Likert scale from 0 (never) to 4 (always). Lower scores refer to lower physical workload. The scale demonstrated a good internal consistency (Rho 0.86) (Van Veldhoven et al., 2015) for one dimension.
The mental workload was measured with the Mental Workload scale, which has four items rated on a 4-point Likert scale from 0 (never) to 4 (always). It is unidimensional and has good internal consistency (Rho 0.81) (Van Veldhoven et al., 2015). Lower scores indicate a lower mental workload.
The emotional workload was measured with the Emotional Workload scale, which has five items rated on a 4-point Likert scale from 0 (never) to 4 (always). It is unidimensional and has good internal consistency (Rho 0.80) (Van Veldhoven et al., 2015). Lower scores indicate a lower emotional workload. These scales have previously been tested within the Italian population.
Ethical Considerations
The study received approval from all the local Ethics Committees. The researchers approached nurses individually and collected written informed consent. Those who refused to sign the informed consent were excluded from the study. Anonymity was ensured by assigning a unique numeric code to each participant (World Medical Association, 2013). Data access was restricted to the research team.
Data Analysis
Sample characteristics and variables studied were described by means, standard deviations (SD), frequencies, or percentages. To compare variables the chi square test or ANOVA test were applied. For verifying the relationship between the investigated variables, a bivariate Pearson product-moment correlation was launched. Effects were reported as positive or negative and for a correlation coefficient between 0–0.29 the correlation was determined as small, for 0.3–0.49 the effect was considered medium and for 0.5–1 the effect was considered large. Preliminary analyses were conducted to check for missing values, outliers, and to test for normality assumptions. Missing data of less than 1% for each variable will be deemed acceptable after confirming random missingness. Cases with missing data will be handled using available case analysis.
An estimation of the sample size was performed with G*Power 3.1. A sample size of 300 surveys was required to achieve a power level of 95%, a significance level (alpha) of 0.05, and effect sizes ranging from 0.1 to 0.3 for the two-sided analysis of Pearson's product-moment correlation coefficient (r). However, 456 surveys were collected for a more stable analysis.
Statistical tests were two-sided; p-values < 0.05 were considered significant. Preliminary and descriptive analyses were conducted in SPSS v. 26.0.
Results
Overall, 456 completed surveys were received from nurses working in 195 randomized shifts (275 surveys in morning and 181 in afternoon shifts). The overall survey response rate was 75% and the most frequently reported reason for nurses missing the survey was their shift workload. No missing data or outliers were recorded. Normal distribution and linearity were satisfactory.
The surveys were collected from nurses working in six hospitals, four public (hospital 2, 3, 4 and 6) and two private (hospital 1 and 5), located in the north (hospital 6), in the central (hospital 1, 3 and 4) and in the southern regions of Italy (hospital 2 and 5). The results were analyzed and presented on the hospital basis.
Socio-Demographic Descriptions
Regarding nurses’ characteristics (Table 1), in all six hospitals, the sample was composed mostly by females. In hospital 1 and 6, the nurses were the youngest, with an average age of 30.83 years (SD 6.47) and 32.07 (SD 9.01) respectively, unlike hospitals 2 (44.68 ± 9.32), 3 (38.28 ± 7.86), 4 (44.47 ± 10.90) and 5 (36.10 ± 10.62). The work experience of nurses working in hospitals 1, 3, 5 and 6 was lower than in hospitals 2 (19.05 ± 10.15) and 4 (18.00 ± 10.09). Adequacy of staff in the shift was perceived at an average level for hospitals 1, 4 and 5 and was reported as particularly critical in hospital 2 (66.7%) and hospital 6 (75.6%). Skill-mix reported in the shift was perceived as frequently adequate only in hospital 3, whereas in the other hospitals nurses reported an average score. For additional information, see Table 1.
Socio-demographic characteristics of the sample (N = 456).
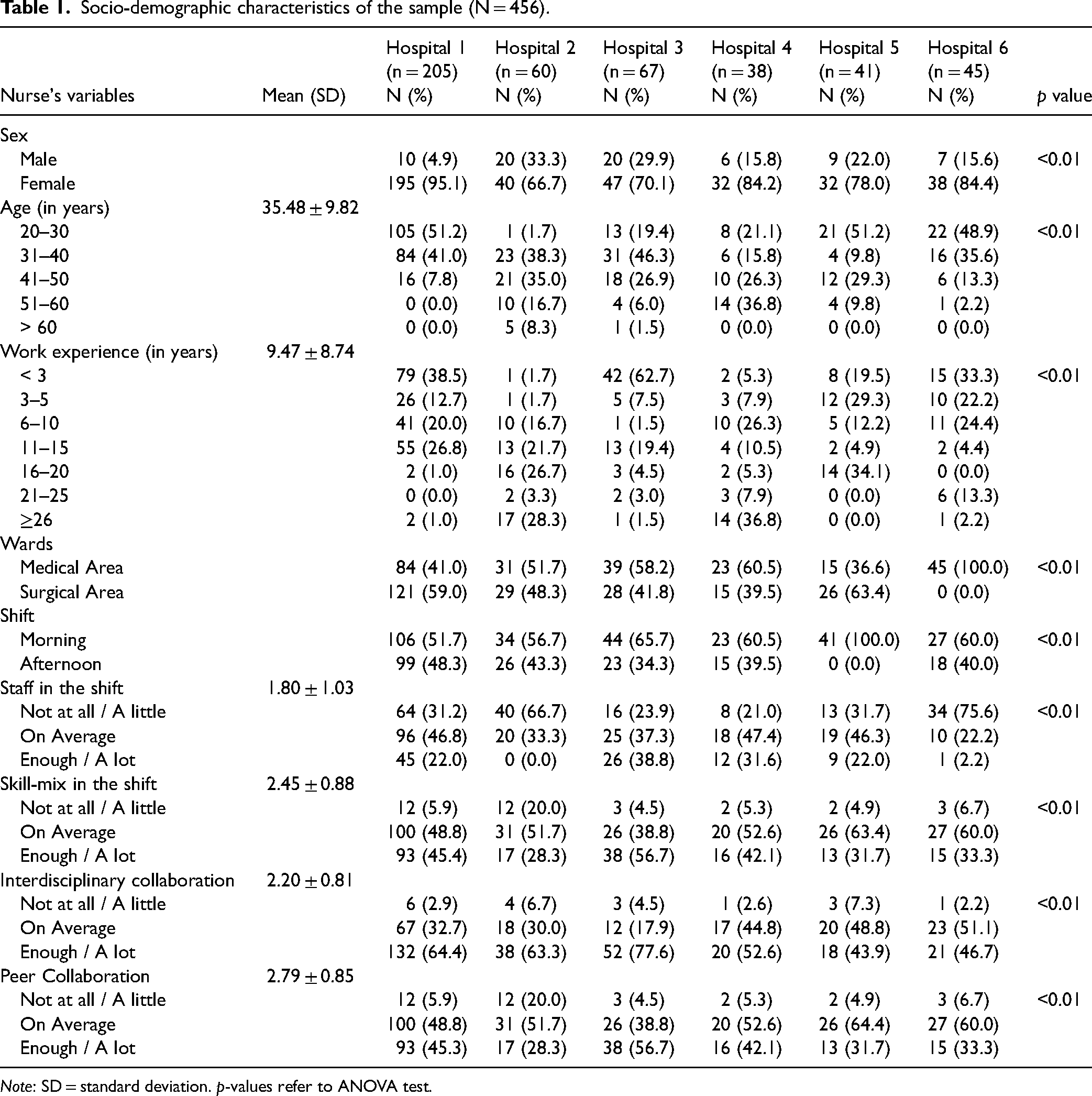
Note: SD = standard deviation. p-values refer to ANOVA test.
Regarding the patient's variables, the nurse-to-patient ratio was in average of 8.66 (SD 2.75). Only in hospital 4 and 5 the nurses reported a 1:3–7 ratio, in hospitals 1, 2, and 3 the frequently reported ratio was 1: 8–10 patients, whereas in hospital 6, nurses reported a critical ratio of 1:11–16 patients in the totality of answers (see Table 2). In all hospitals the nurses frequently reported to care for 1–2 patients in isolation (0.77 ± 1.13) and in hospital 5 36.6% of nurses reported to care for 3–4 isolated patients during the shift. Additionally nurses reported to take care of patients of up to two medical specialties more frequently.
Description of patient variables (N = 456).
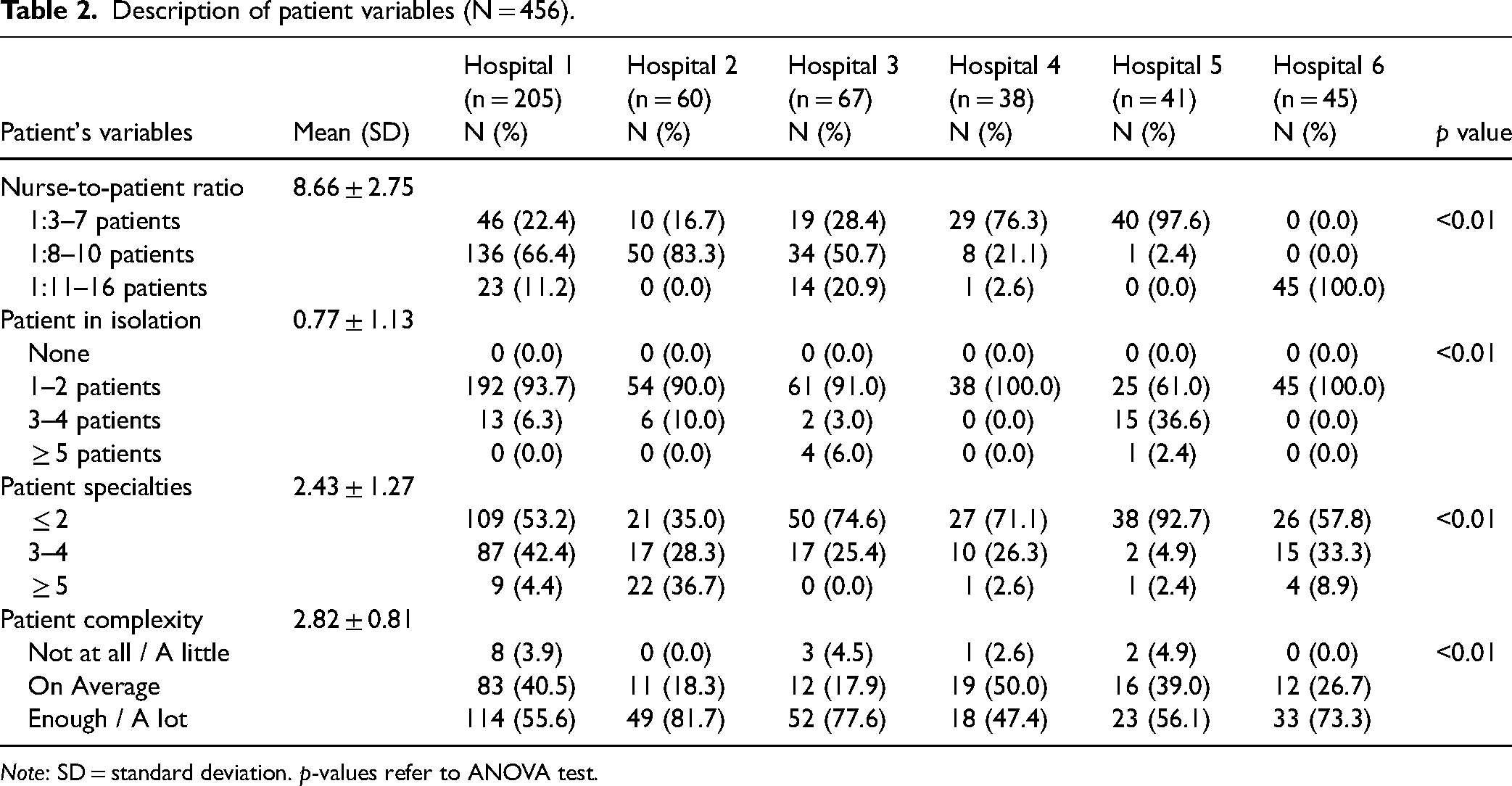
Note: SD = standard deviation. p-values refer to ANOVA test.
Regarding workflow variables, nurses were asked to report which activity impacted more in their work during the shift. Patient admissions/discharges frequently impacted the work of nurses in hospital 1, 2 and 4, whereas a lower impact was reported in hospitals 3, 5, and 6 (Table 3). Similarly, in hospital 2 (55%) and 4 (42.2%) nurses reported a higher involvement in the shift with patient transport. Responses of nurses regarding the impact in the shift related to search or contact of physicians was very different among hospitals, and nurses in hospital 5 reported less problems. Regarding work programs and unscheduled activities, nurses in hospitals 1, 4, 5, and 6 frequently reported a low impact, differently from hospitals 2 and 3 that reported a 40% and 43.3% high impact respectively. Additionally, nurses in all hospitals reported a high impact in the shift work regarding healthcare documentation. For additional information, see Table 3.
Description of Workflow Variables (N = 456).
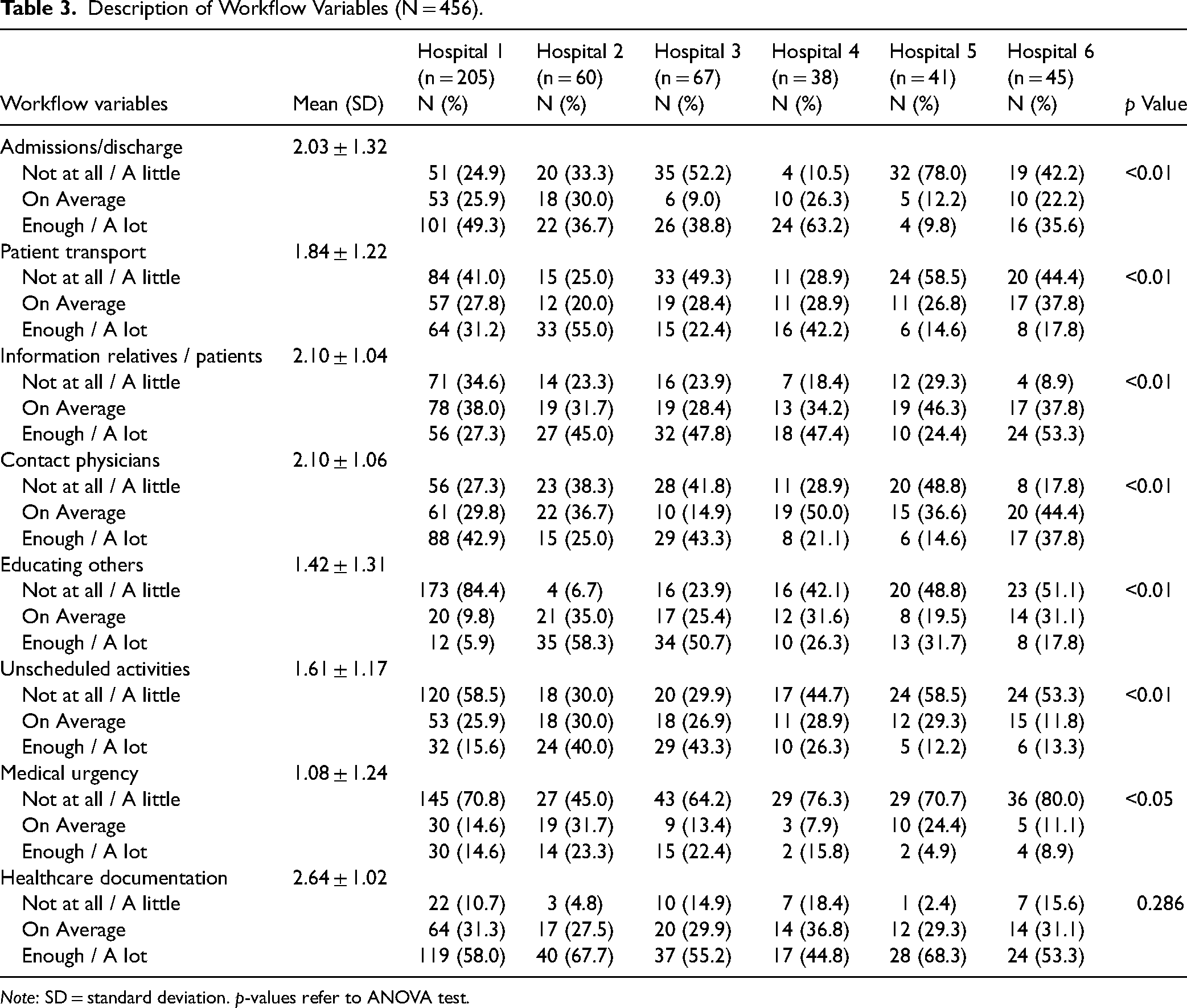
Note: SD = standard deviation. p-values refer to ANOVA test.
Overall all nurses reported high workload in the shift in general, in all hospitals. Regarding physical workload the mean score was 43.66 ± 23.93 indicating a moderate level. Nevertheless, in hospital 2 33% of nurses reported high scores differently from nurses in the other hospitals. The mental workload was reported to be high, with a mean score of 86.59 ± 18.03 with small variations among hospitals. The emotional workload was medium, with a mean of 55.07 ± 17.43 with little differences in all hospitals except in hospital 5 where 36.6% of nurses reported high scores (see Table 4).
Description of Workload (N = 456).
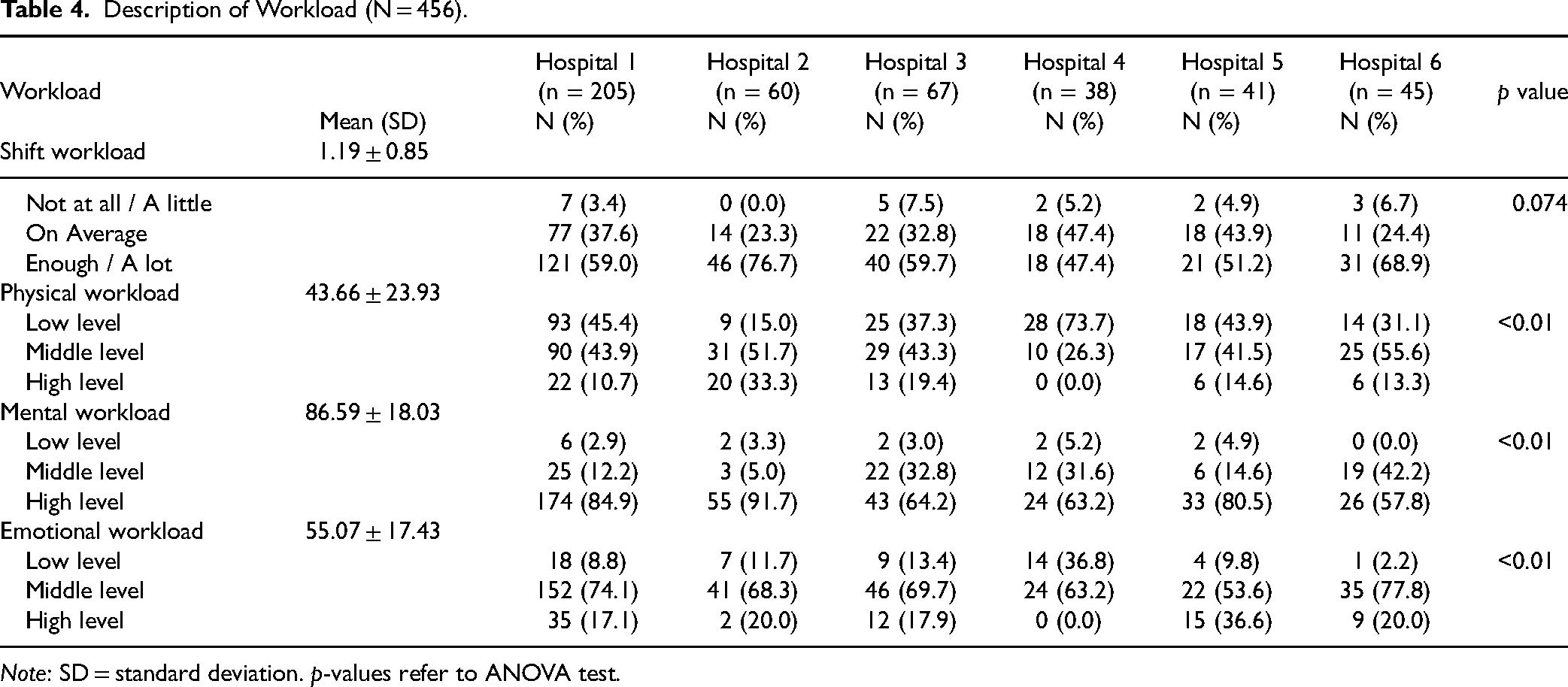
Note: SD = standard deviation. p-values refer to ANOVA test.
Description of Relations Between Included Variables and Workload Dimensions
In Table 5 are presented, entire sample correlations between nurse, patient and workflow variables with physical, emotional and mental workload dimensions. The bivariate correlations are expressed with the Pearson product-moment coefficient.
Variables of Pearson Correlation with Workload Dimensions (N = 456).

**Correlation is significant at the 0.01 level (2-tailed); *Correlation is significant at the 0.05 level (2-tailed).
Regarding the physical workload, positive and negative correlations of small, medium and large effects were evidenced. Among the positive correlations, large effects were observed only for the patient complexity of care (r = 0.501) and the general workload of the shift (r = −0.620 inverse scoring). The correlation was positive and showed medium effect for the adequacy of staff in the shift, unscheduled activities, medical urgency and healthcare documentation (see Table 5). For additional correlations, see Table 5. Finally, the physical workload was found to be positively and significantly correlated with emotional and mental workload.
Regarding the emotional workload (see Table 5), significantly negative correlations with the ward in which the nurse worked, the number of staff on the shift, the degree of interdisciplinary collaboration, and the workload of the shift (all inverse scored) were observed. Other positive small effect correlations were observed for patient complexity, isolation, and specialties and workflow variables related to unscheduled activities, medical urgency, and healthcare documentation. For additional correlations, see Table 5. Finally, the emotional workload correlated positively and significantly with the physical (medium effect), mental and general workload (small effect).
The mental workload was found to be positively correlated with the degree of interdisciplinary and peer collaboration, patient complexity, isolation, specialties, admission/discharge, transport, as well as with workflow variables related to contacting physicians, medical urgency and healthcare documentation (small effects). Finally, the mental workload was positively correlated with physical, emotional, and general shift workloads (small effects) (see Table 5).
Description of Common or Context Specific Relations Between Variables and Workload Dimensions
In the supplemental material Table S1 we present Pearson product-moment bivariate correlations among variables explored and workload dimensions based on the specific hospital data. When a correlation was statistically significant between a variable explored and at least one dimension of the workload, we included it among present effects for that hospital. When the variables presented statistically significant correlations in at least four hospitals we considered it as a common effect variable, whereas when the significant effect was found in up to three hospitals, we considered it setting specific. The classification of relationships as common or setting specific is presented in Table 6. Our data suggest that the patient complexity of care, admission/discharge, transport, information to patient/relatives, unscheduled activities together with contacting physicians, interdisciplinary collaboration and skill-mix in the shift are variables related to nurses’ workloads, in general and on specific dimensions. Additionally, the ward where nurses work has an effect on their perceptions of the workload.
Description of Relations Between Common and Setting Specific Variables and Workload Dimensions.

Note: x refers to significant Pearson correlations observed across hospitals between the variables and the dimensions of workload.
Discussion
This study aims to describe aspects associated with physical, mental, and emotional nursing workloads that are distinguished for specific work settings and identify factors that are common across them. Nurses working in six hospitals (4 public and 2 private) in Italy with different organizational characteristics have been enrolled in the present study.
Overall, there is no statistically significant difference among hospitals regarding the perception of general workload but the differences become statistically significant on specific dimensions of workload. In fact, when nurses were asked in general regarding workload in the shift their answers were mostly grouped as enough or a lot. When they were specifying in what dimensions they perceived the impact they reported higher scores on mental workload, followed by scores on emotional and physical loads. These results confirm previous findings from this research team (Ferramosca et al., 2023; Ivziku, Ferramosca, et al., 2022; Ivziku, De Maria, et al., 2022) and support the reasoning that irrespective of the setting, nurses’ work generates loads on the physical, mental and emotional dimensions.
Exploring further associations among variables, it is observed that some of them were correlated significantly with nursing workload dimensions in more than four hospitals, whereas others were significant only in a few hospitals. In an attempt to better determine the aspects that generate workload on nursing work, the work settings were explored looking for variables related to nurses, patients and workflow and their relationships with dimensions of workload. In the following paragraphs, common and context-specific relationships found in this study are described.
Common Variables Associated with Nursing Workload Dimensions
The variables that were frequently correlated with workload dimensions in more than four hospitals were: patient complexity of care, admission/discharge, patient transport, information to patient/relatives, skill-mix in the shift, interdisciplinary collaboration, contact physicians, unscheduled activities, and ward.
Regarding patient complexity of care, relationships with the three dimensions of workload were evidenced. Indeed, the highest frequency of correlations among hospitals was observed on the physical workload but in two hospitals relationships with emotional and mental loads were also found. The patient complexity of care is related to patient needs for nursing care and as the complexity increases, nursing tasks increase leading to time pressure (Qureshi et al., 2020). Moreover, augmented concentration on the work and recurrent communication with the patient and healthcare professionals induce higher mental and emotional workloads (Arsenault Knudsen et al., 2018; Van der Heijden et al., 2020; Yanchus et al., 2017).
Additionally, the admission/discharge of patients and their transportation within and among care settings was frequently correlated with physical and mental or physical, emotional and mental workloads, respectively. Previous literature reported that the increased patient turnover intensifies the nursing workload and creates unstable work environments (Blay et al., 2017; Yanchus et al., 2017). Moreover, the patient turnover and patient movements within hospitals are burdensome for nurses because they are time-consuming and disrupt the workflow (VanFosson et al., 2017; Yanchus et al., 2017) requiring not only physical energies but also higher concentration and emotional equilibrium of nurses.
One essential part of the nursing work is the education and information of patients and relatives regarding care (Chan et al., 2013). However, when nurses are overwhelmed with activities during the shift, despite trying to find snippets of time for communication with patients and families, they frequently report interruptions of work (Myny et al., 2012). In turn, this causes disturbances in nurses’ work leading to increased physical, emotional and mental loads on nurses (Navajas-Romero et al., 2020). This is confirmed in the data since correlations with the three dimensions were observed.
With reference to variables related to nurses, skill-mix in the shift in this study was correlated with physical, emotional and mental workloads. In previous studies, this variable was associated with unfinished care, work stress and emotional workload (Duffield et al., 2011; Van den Oetelaar et al., 2021; Yanchus et al., 2017). Nevertheless, studies observing relationships between the skill-mix in the shift and workload are few and further research is needed.
In addition to the skill-mix, the quality of interdisciplinary collaboration was recurrently correlated with emotional and mental workloads. Difficulties in interdisciplinary collaboration can interfere with nursing activities making the tasks to be carried out heavier and more stressful. When collaboration and teamwork are perceived of good quality they support nursing decision-making and hinder nurses’ workload estimation (Arsenault Knudsen et al., 2018; Van den Oetelaar et al., 2021; Yanchus et al., 2017). Collaboration at work was often considered a protective factor for balancing the workload, coping with stressful working conditions, engaging in patient care, and remaining in the nursing profession (Van Bogaert & Clarke, 2018).
Workflow aspects related to unexpected activities and contacting physicians were correlated with different dimensions of workload. This can be explained by disruptions in nursing work generated by these variables and consequently increased time issues (Fagerström & Vainikainen, 2014), increased physical requests (Mohammadi et al., 2016), and augmented mental and cognitive demands (Jennings et al., 2022). Considering that nurses spend a lot of time during the shift away from the patient (Congdon et al., 2020) it is crucial to explore and intervene on context factors to improve the workflow.
Additionally, the data suggest that nurses working in medical wards report higher physical and emotional workloads. The literature reports that patients in medical wards present multiple and complex care needs (Bakhshi et al., 2019) which require high-level skills and care-time of nurses (Michel et al., 2021). When nurses work in shifts with reduced human resources, increased patient care needs and repeated workflow interruptions they will report increased physical and emotional workloads, as is the case with this study data.
What has been described so far are common factors found to be correlated with workload dimensions across different medical and surgical ward settings in Italy. Similar studies will be helpful to support the literature on this topic.
Context Specific Variables Associated with Nursing Workload Dimensions
Some variables explored were correlated with workload dimensions in three or fewer hospitals. This was the criteria chosen to define a context-specific association.
For example, the nurse-to-patient ratio was associated specifically with the physical dimension of workload only in hospitals 1 and 5, both being private. The nurses working in these two hospitals reported a different percentage in the nurse-to-patient rates, nevertheless, the correlation effects were significant with the workload. In the nursing literature, the nurse-to-patient ratio was commonly used as an indicator of the nursing workload (Griffiths et al., 2020). In fact, some literature reports that the number of patients cared for (Nasirizad Moghadam et al., 2021), and direct patient care (Van den Oetelaar et al., 2021) increase nurses’ physical workloads, limit nurse–patient contact, increase care left undone, and intensify time pressure on nurses and concerns about patient outcomes (Yanchus et al., 2017). This study’s findings add to the literature that confirms the opposite theory (Oppel & Mohr, 2021; Qureshi et al., 2020), supporting that it is not the number but rather the complexity of patient care that determines an increased perception of workload among nurses. It seems logical that the specific context can determine the number of patients admitted in a ward, the environmental organization of areas of care as well as the patient specialties or the policies for staffing and these aspects will contribute in determining the perceived workload among nurses.
Caring for patients of different medical specialties was found to correlate with physical and/or emotional nurse workload. The mix of medical specialties within a ward is determined by the hospital policies. A high number of patients from different specialties cared for by a nurse during the shift, will determine an increased need for communication with different physician teams (Duffield et al., 2011), which can result in workflow disruption (VanFosson et al., 2017), reduced work efficiency (Congdon et al., 2020), and undoubtedly an increase in the perception of the nursing workload (Duffield et al., 2011), physical and emotional.
Among patient variables, patient isolation was found to correlate with physical, mental or emotional workload, differently for the hospital settings. It is logical that this variable is setting-specific, considering that within a medicine and surgery department, the number of isolated patients may differ in time or even may be higher in some departments than in others. The wards included in this study were not dedicated to infectious diseases and were not Covid-19 dedicated units. Despite this, caring for an infected patient requires more time for the nurse for prophylactic measures to prevent or contain the spread of infection. This leads nurses to ration the remaining working time for the care of other patients, generating a psychological and physical burden on nurses and an increased workload (Duffield et al., 2011; Navajas-Romero et al., 2020).
The perceived adequacy of staffing in the shift was correlated in three hospitals mostly with physical and emotional workload dimensions and in one hospital with the mental load. Even this variable is very much connected to the specific hospital setting based on staffing resource investments of the hospital’s top management. Previous research provided contradictory findings. In one research a relationship with the physical load was documented (Oppel & Mohr, 2021) while in another no effects were evidenced (Wang et al., 2021). This study adds to the present knowledge information regarding relationships with emotional and mental workloads. Restricted staffing resources lead nurses to reduce collaboration and contact with colleagues and patients and increased number of nursing activities, which requires a higher concentration at work and increased psychological demands of nurses. A recent scoping review (van der Mark et al., 2021) reports that the perceived adequacy of staffing by nurses could potentially be an available measure for staffing requirements. Therefore, as in Oppel & Mohr (Oppel & Mohr, 2021), the perception of staffing resources adequacy is probably a better indicator than the nurse-to-patient ratio for measuring nurse workload and staffing needs.
Peer collaboration in the shift was correlated to the mental and emotional workload. This variable as well is classified as setting-specific. Staff collaboration during a shift can be determined by various aspects like the quality of relationships among nursing team members and the ward nurse manager's leadership style. When collaboration is not optimal, this can increase the workload of the nurse. Good collaboration can generate good teamwork, a protective factor for balancing the workload and coping with stressful working conditions (Van Bogaert & Clarke, 2018).
Among workflow variables, the education of others was confirmed to be correlated with physical and emotional workloads. This variable as well is considered to be setting-specific. Although all included hospitals where teaching hospitals, at the moment of the data collection only in three hospitals nurses reported a high load in this variable. It may happen that in some months and in specific departments, there are no students or contrarily there is an over boarding of students and new comer nurses. Educating others (new nurses, students, new physicians, etc) is part of nursing activities, an important component of building workplace cohesiveness, and preparing new generations of nurses (Sassaki et al., 2019). Studies considering the effect of educating others on the workload so far are very few. Previous studies reported that educating others is time-consuming (Campos et al., 2018) and impacts the workflow or work-planning (Myny et al., 2012) leading to an increased physical workload (Mohammadi et al., 2016) and emotional strain. Further research is recommended to explore these relationships.
Medical urgency as well confirmed to be setting specific and to have effects on physical, emotional and mental workload in two hospitals. In fact, in the two hospitals where these correlations were confirmed, nurses reported a 22–23% high impact in their responses. Medical urgency is not very common, but when a patient presents clinical instability or medical urgency, it disrupts nurses’ work and requires them to think and act quickly and to maintain emotional stability. Previous literature report the pressure perceived by nurses related to the time factor; working quickly and with a great variability of activities determines even greater perception of both physical and emotional workloads (Pedroso et al., 2020) and, during a medical urgency nurses should increase their concentration and decision making which leads to a higher mental load.
In nursing practice, nurses among other activities must devote time to healthcare documentation, an extremely important activity. The results of this study show that healthcare documentation correlates with the physical workload in three hospitals and with all the three dimensions of workload in one hospital. In this particular setting, the documentation was paper-based and particularly detailed on the patient assessment. In recent years, the volume of nurse's documentation increased, due in part to increased patient turnover (Blay et al., 2017) or to multiple paper-based or electronic recording systems (Shihundla et al., 2016). Different studies confirm that this is a time-consuming activity (Campos et al., 2018; Duffield et al., 2011), frequently associated with increased workloads (Moore et al., 2020; Myny et al., 2012). In addition, when a patient's documentation is unavailable, or incomplete, this gives rise to additional nursing time, amplifying an already persistent workload (Shihundla et al., 2016). Documentation continues to contribute largely to nurses’ workloads, constituting 15% of a nurse's shift working time (Campos et al., 2018). The most time-consuming documentation tasks are head-to-toe assessments, admission hires, and vital charting, which account for the majority of the documentation time (70%) (Munyisia et al., 2011). Nurses look forward to interventions that reduce the documentation time (like for e.g., nursing scribes, device integration, and artificial intelligence to help with documentation). Without strategic interventions, nurses’ documentation burden is unlikely to be fully alleviated.
Final Discussion on Nursing Workload Dimensions
The nursing workload has been articulated in physical, mental and emotional dimensions only in a few studies. In this research, the focus was on variables identified as significant for the nursing workload, measured from a general perspective in prior qualitative or quantitative studies. This study aimed to explore the correlation effects of these variables with the specific dimensions of workload. The findings confirm that these variables have distinct effects on the explored workload dimensions. For example, the variable “interdisciplinary collaboration”, which was classified as having a common effect on the nursing workload, was perceived differently by nurses in various hospitals. In one hospital it was seen as affecting physical and emotional dimensions of nursing workload, whereas in others, effects were perceived only on the emotional or mental dimension. This suggests that, despite organizational factors, the impact of work aspects and contexts on nurses is highly personal and individualized.
The Job Demand-Resources theory (Bakker & Demerouti, 2017) suggests that personal resources can act as a buffer against job demands. To enable nurses to better manage their workload, strengthening personal resources can contribute to their overall well-being. Some individual aspects that influence how people perceive their workload are: time management and priority setting (Goldsby et al., 2020); effective coping mechanisms (Lee et al., 2016); effective communication skills including communication of their needs, delegating tasks, or seeking support (Goh et al., 2020); work-life balancing (Holland et al., 2019); individual personality traits, such as conscientiousness, strong personal values and ethics of care (Waterfield & Barnason, 2022), resilience (Lanz & Bruk-Lee, 2017), and health (physical and mental).
Considering these individual factors in addition to patient variables, nursing resources and workflow aspects discussed in this research, it is essential for healthcare organizations and nurses themselves to understand the nursing workload and address it effectively. Nurses play an active role in observing how the work conditions are influencing their job performance and in acting proactively to create a supportive and conducive work environment. Tailoring interventions based on these aspects can contribute to a healthier and more balanced working environment.
Strengths and Limits
This study makes significant contributions to the research in the field of nursing workload. In contrast to many other previous studies, this research focused on the perceived workload of nurses during specific shifts, asking them to report concrete factors that impacted their shift work. This approach enables a more objective measurement of workload. Additionally, this study documented that work-related aspects, including those involving nurses, patients and workflow, impact nurses across various dimensions—physical, mental, and emotional. Additionally, recognizing that perceptions may vary among individuals or working environments, the study sought to enhance variability by including the perspectives of nurses working in six hospitals—both public and private—and across different wards. Despite the inherent variability, the study successfully identified variables that exhibit a consistent relationship with dimensions of nursing workload, along others that were more context specific. This will lay the groundwork for future studies aiming to delve into the relationships further.
However, the current study does have some limitations. The utilization of a self-assessment questionnaire may introduce a response bias toward social desirability. To mitigate this, the researchers attempted to address the issue by incorporating variability in participant numbers, observed shifts, unit types, and hospitals from diverse regions, encompassing both public and private settings. An additional limitation is the cross-sectional design of the study, which precludes the ability to establish cause-and-effect relationships.
Future research could enhance the current knowledge by incorporating job resources and investigating their impact on workload dimensions. Moreover, researchers might consider exploring additional variables not covered in this study and testing their relationships with nurse-workload dimensions, taking into account the specificity of the work context or generalizability. Longitudinal studies are also recommended to identify causal relationships between the explored variables and workload dimensions.
Implication for Practice
The findings of this study suggest the need for interventions on the variables explored. Interventions should be multidimensional and take into account all the sources of stressors in the nursing work. Some interventions that may help nurses afford the pressure and stress associated with high physical, emotional and mental workloads can be: training programs on strengthening self-efficacy (Molero et al., 2018), building resilience and adaptability skills to handle uncertainty (Lanz & Bruk-Lee, 2017), increasing mindfulness, meditation, and other well-being activities (Melnyk et al., 2020), strengthening emotional intelligence to manage better emotions (Lartey et al., 2021), empowering nurses with professional governance to enhance control over their tasks, decision-making, and work processes (Porter-O’Grady & Clavelle, 2020), creating a flexible work environment through flexible scheduling, and support for personal time and work-life balance (Pyle & Roesch, 2022), encouraging a supportive work culture and social support, fostering team cohesion and promoting open communication (Velando-Soriano et al., 2020), reorganization of work processes and rearrangement of environments to reduce disruptions (Ferramosca et al., 2023), adjusting staffing resources based on recurrent evaluations of patient complexity and turnover, and staff skill-mix in the ward.
Organizations should explore innovative approaches to support and provide relief to fatigued nursing staff (Moloney et al., 2020). Creating conducive work environments is crucial for retaining the nursing workforce. Therefore, organizations need to monitor levels of physical, emotional and mental workloads among nurses to prevent negative outcomes on their staff and on the quality of care. Persistent high physical workloads among nurses lead to work-related musculoskeletal disorders (Zare et al., 2021) or injuries (Bagheri Hosseinabadi et al., 2019), sick leave and absenteeism (Van der Heijden et al., 2020) consequently leading to a further reduction in the staff available on shifts. The mental workload negatively impacts the performance of nurses (Yuan et al., 2023), resulting in increased vulnerability to errors (Nasirizad Moghadam et al., 2021), frustration and dissatisfaction (MacPhee et al., 2017) ultimately leading to burnout (Clari et al., 2022). The emotional load contributes to heightened perceptions of workload, increased tendency to leave the job (Van der Heijden et al., 2020), elevated stress levels (Yen et al., 2019) and a greater risk of burnout (Clari et al., 2022). Furthermore, these diverse facets of workload, each displaying distinct characteristics, can impact one another (Ferramosca et al., 2023), contributing to escalating workloads.
Conclusions
In conclusion, work contexts significantly influence the well-being of nurses, impacting their physical, emotional, and mental states. Certain variables consistently affect the nursing workload across various work settings, while others are context-specific. Moreover, the effects on perceived workload dimensions are individualized. Both nurse managers and nurses play an active role in exploring and addressing determinants associated with nursing workload dimensions, emphasizing the importance of personalized strategies in fostering a supportive work environment.
Supplemental Material
sj-docx-1-son-10.1177_23779608241258564 - Supplemental material for Decoding Nursing Job Demands: A Multicenter Cross-Sectional Descriptive Study Assessing Nursing Workload in Hospital Medical-Surgical Wards
Supplemental material, sj-docx-1-son-10.1177_23779608241258564 for Decoding Nursing Job Demands: A Multicenter Cross-Sectional Descriptive Study Assessing Nursing Workload in Hospital Medical-Surgical Wards by Dhurata Ivziku, PhD, RN, Raffaella Gualandi, PhD, RN, Federica Maria Pia Ferramosca, PhD, RN, Marzia Lommi, PhD, RN, Maria Ymelda Tolentino Diaz, PhD, RN, Barbara Raffaele, PhD, RN, Graziella Montini, MNS, RN, Barbara Porcelli, MNS, RN, Alessandro Stievano, PhD, RN, Gennaro Rocco, PhD, RN, Ippolito Notarnicola, PhD, RN , Roberto Latina, PhD, RN, Anna De Benedictis, PhD, RN and Daniela Tartaglini, PhD, RN in SAGE Open Nursing
Footnotes
Acknowledgments
The authors want to acknowledge all nurses and nurse managers of the wards involved in this study.
Author Contributions
Conceptualization: D.I. and DT.; methodology: D.I., M.L., and R.G.; software: D.I., M.L., and I.N.; validation: B.R, M.Y.T.D., G.M., and B.P.; formal analysis: D.I., M.L., and I.N.; investigation: D.I, M.L., B.R., M.Y.T.D, and F.M.P.F; resources: D.I, M.L., B.R., M.Y.T.D, and F.M.P.F; data curation: D.I., M.L., and F.M.P.F.; writing—original draft preparation: D.I., M.L., F.M.P.F., and M.Y.T.D; writing—review and editing: D.I., M.L., G.R., A.S., A.D.B., R.G., R.L., and D.T.; visualization: B.R, M.Y.T.D., G.R., A.S., A.D.B., G.M. and B.P.; supervision: DT. and R.G.; project administration: D.I. and DT; funding acquisition: D.I. and DT. All authors have read and agreed to the published version of the manuscript.
Data Availability Statement
The data are available from the first author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Centre of Excellence for Nursing Scholarship (CECRI), Order of Nurses of Rome, Italy (grant reference 3.21.4). Additionally, the authors want to acknowledge the Italian Scientific Society for the Direction and Management of Nursing (SIDMI) for the support and sponsorship of the study.
Informed Consent Statement
Written informed consent was obtained from all the participants involved in the study.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. The study was approved by the Ethics Committee of University Campus Bio-Medico of Rome on 9 November 2020 with the protocol number: Prot.: 95/20 OSS ComEt CBM; the Ethics Committee of ASL Lecce on 14 May 2021 with the protocol number: Verbale N. 62; the Ethics Committee “LAZIO 2” on 9 June 2021 with the protocol number N. 0116717/2021, the Ethics Committee “IRCCS ISMETT” on 21 September 2022 with the protocol number IRRB/13/22; the Ethics Committee “INSUBRIA” on 11 October 2022 with the verbal number N. 105
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.