
Abstract
Background of the Study
Mammograms are sometimes met with issues of overdiagnosis and underdiagnosis; therefore, they are less reliable in identifying cancer in women with dense breasts. As a result, it is critical to be aware of other sensitive screening techniques for the early diagnosis of breast cancer.
Aim
The ultimate objective of this study was to assess the knowledge of nursing undergraduates regarding non-invasive biomarkers, such as volatile organic compounds in breath, nipple aspirate fluid, sweat, urine, and tears, for the early detection of breast cancer to help improve patient care, determine the risk factors, and encourage practice of breast self-examination.
Methods
Cross-sectional research was done in the Department of Nursing at Farasan campus using a self-structured questionnaire as the study tool. A total of 260 students willingly participated. The study tool had evaluation questions focused on the non-invasive biomarkers of breast cancer, risk factors, and breast self-examination practices to collect data. The data were subjected to descriptive and inferential statistics. The statistical significance was calculated at P < .05. Data analyses were done using Microsoft Excel (2013).
Results
A
Conclusions
Outcomes would help prioritize actions to help future nurses better understand breast cancer, allowing them to extend patient care in the best way possible.
Introduction
After lung cancer, breast cancer (BC) is the most common malignancy in women worldwide and the second-leading cause of cancer-related mortality in developed countries (WHO, 2012). In 2020, approximately 68,500 people died from breast cancer globally, and approximately 2.3 million women received diagnoses. By the end of 2020, BC had become the most common disease in the world, with 7.8 million women staying alive after being diagnosed with breast cancer in the preceding 5 years (WHO, 2021).
Breast cancer is very common, thereby putting a lot of strain on healthcare resources and significantly raising prices (Cocco et al., 2022). The financial burden of managing breast cancer in Saudi Arabia is high and dramatically escalates as the disease progresses. In 2018, an estimated $13.345 million USD was spent to treat breast cancer in Saudi Arabia, with Stage I patients paying an average of $14,249 USD and Stage IV patients paying an average of $81,489 USD. One of the major factors influencing the total healthcare costs was the price of medications, hospitalization, and diagnostic testing. The majority of trastuzumab-based regimens accounted for 67% of the overall cost of medications in the targeted therapy category (Alghamdi et al., 2021).
Early BC diagnosis programs, assessment of costly interventions, and consideration of non-invasive biomarkers of BC and biosimilars are some of the ways that could lead to cost savings (Cesarec et al., 2007). According to estimates, there were 3,629 cases of breast cancer in Saudi Arabia in 2018. By 2040, that number is expected to rise to 6,886 (Alghamdi et al., 2021). Additionally, it has been noted that the bulk of Saudi Arabian patients with breast cancer receives a diagnosis at an advanced stage, which could significantly raise resource consumption and cost (Alghamdi et al., 2021; Bcheraoui et al., 2015; Cesarec & Likić, 2017; Cocco et al., 2022; WHO, 2021). Age, family history of the disease, hormone problems, alcoholism, stress, and other factors are established risk factors for breast cancer development. However, it's crucial to remember that 75% of breast cancer cases in women have an unknown cause. Breast density genes may possibly be linked to an increased risk of breast cancer.
Breast cancer could happen to any woman, irrespective of her education, social, and cultural background. Therefore, a woman's awareness of breast cancer is crucial. The ability to identify the difference between normal and abnormal breasts, to know what to look for during breast self-examination (BSE) practices, and identify the appropriate time for breast cancer screening may help detect the early stage of breast cancer (Almuhlim et al., 2018; Yousuf, 2010). BSE increases women's awareness of their breast health, potentially resulting in the early diagnosis of breast cancer. BSE and adherence to this practice, at least on a monthly basis, are gateways to health promotion behaviors.
Mammograms have been one of the most effective screening methods and a crucial component of early breast cancer identification in recent years (Guide to Mammography and Breast Imaging, 2012; Ponraj et al., 2011). They also expose the breast to substantially lower radiation doses than previous devices (Rangayyan et al., 2006). However, mammography does not always offer a conclusive diagnosis regarding the existence or absence of cancer, particularly in situations with dense breast tissue, which is defined as the quantity of fibro-glandular tissue in the breast that is radiologically dense (Boyd et al., 2007; Johns, 1987). Therefore, mammographic screening is frequently unreliable in differentiating between people with breast cancer and healthy individuals, in addition to being costly, uncomfortable, and sometimes hazardous for sensitive patients.
The search for disease markers in unconventional bodily fluids is becoming increasingly popular as biomarker identification methods continue to progress. Breast cancer-associated biomarkers have been identified in urine (Beretov et al., 2015), nipple fluid aspirate (Shaheed et al., 2018), and breast milk (Aslebagh et al., 2022). The knowledge of breast cancer markers in fluids other than those traditionally associated with cancer diagnosis could improve nurses’ ability to identify the disease and create community awareness for diagnosis. Tears also contain hundreds of proteins/peptides, lipids, glycoproteins, hormones, and small-molecule metabolites (Barmada & Shippy, 2020). The changing expression levels of ocular proteins in response to systemic disease have been well established in the literature. In a study conducted by Daily et al. (2022), ocular proteomes were examined to identify protein biomarkers with altered expression levels in women diagnosed with breast cancer.
Tears, sweat, urine, nipple aspirates, and exhaled breath are examples of circulatory, non-invasive biomarkers that may be used to detect therapeutically relevant mutations and tumor features. These non-invasive biomarkers may also offer important insights regarding the course of the disease and its response to treatment (Barmada and Shippy, 2020; Bohm et al., 2012; Chen et al., 2016; Deutscher et al., 2010; Erbes et al., 2015; Hanna et al., 2019; Hermann et al., 2018; Li et al., 2020; Patel & Shah, 2022). Compared to imaging or tissue samples, these non-invasive biomarkers can be gathered at a higher frequency, which may enable more intelligent early diagnoses and management of the disease (Barmada and Shippy, 2020; Bohm et al., 2012; Chen et al., 2016; Deutscher et al., 2010; Erbes et al., 2015; Hanna et al., 2019; Hermann et al., 2018; Li et al., 2020; Patel & Shah, 2022).
Literature Review
Global Incidence
The patterns and trends of breast cancer vary in different countries. There were approximately 2.3 million new breast cancer cases and 685,000 breast cancer deaths worldwide in 2020 (Lei et al., 2021). Its incidence and mortality vary among countries, with the age-standardized incidence ranging from the highest of 112.3 per 100,000 of the population in Belgium to the lowest of 35.8 per 100,000 of the population in Iran and the age-standardized mortality from the highest of 41.0 per 100,000 of the population in Fiji to the lowest of 6.4 per 100,000 of the population in South Korea. Breast cancer is the most common type of cancer in women in the United States (Yıldırım et al., 2022). As per the estimates of the American Cancer Society, approximately 4 million women in the country had a history of breast cancer as of early 2019 (DeSantis et al., 2019). Additionally, approximately 50,000 women in the US receive a diagnosis of breast ductal carcinoma in situ (DCIS), one of the most common precancers in all tissues (American Cancer Society, Breast Cancer Facts & Figures, 2019). In several Asian and African nations, the peak age of breast cancer is more than 10 years younger than in European or American nations (Sung et al., 2021).
The incidence of breast cancer is significantly higher in developed countries than in developing nations. This is because of a long-standing higher prevalence of risk factors, including decreased fertility rates, a high percentage of oral contraceptive or hormonal menopausal therapy use, shorter breastfeeding durations, and higher body weights (Cancer CGoHFiB, 2002; Hu et al., 2013; Kim et al., 2019; Møller et al., 2002; Nguyen et al., 2020; Pfeiffer et al., 2018; Zhang et al., 2012).
National Incidence
In 2018, breast cancer was the most commonly diagnosed type of cancer and the second-leading cause of death after leukemia in Saudi Arabia (Alqahtani et al., 2020). In recent years, the KSA has seen an increase in the incidence of breast cancer, with instances rising from 1,152 per 100,000 people in 2008 to 1,473 per 100,000 people in 2010 and 1.826 per 100,000 people in 2014 (Alothaibi, 2018; Basudan, 2022). According to the KSA Health Council's 2014 cancer registry, breast cancer accounts for 28.7% of all cancer cases in women. However, a different study found that breast cancer causes 13.08% of all cancer-related fatalities, with 98% of cases affecting women and 12% affecting males (Alothaibi, 2018). Scientific studies from different regions in the KSA have reported the prevalence of breast cancer among females (Alothaibi et al., 2018; Heena et al., 2019; Yakout et al., 2014), with three to eight confirmed cases of breast cancer per 1,000 patients from 2010 to 2017. Moreover, the highest incidence rates of breast cancer were reported in 2017.
Two distinct patterns of breast cancer were also observed, with the most common type being ductal carcinoma with an incidence percentage of 81.80%, followed by lobular carcinoma with a 3.40% incidence rate (Asiri et al., 2020). These data indicate that further steps are still needed to identify breast cancer at an early stage.
Opportunities for Control and Intervention
One of the most successful programs that have been implemented by the Saudi government is the breast cancer screening program that offers mammography, which is provided for free at all government facilities, and malls. Despite this, the incidence remains high. Sometimes, extensive mammogram use may also lead to high incidence rates of breast cancer. Mammography screening is the best way to discover breast cancer early, but it can also lead to overdiagnosis, which can increase the incidence of breast cancer. The rate of overdiagnosis varies from 5% to 50% (Srivastava et al., 2019).
The Center for Disease Control stated that early detection is the best defense against the morbidity and mortality of breast cancer (Srivastava et al., 2019). In line with this, the best way to reduce incidence is to know the non-invasive biomarkers of breast cancer, identify the risk factors, and encourage the practice of breast self-examination (BSE) that may help in the early detection of breast cancer.
Significance of the Study
Nurses comprise the largest proportion of the Saudi health care system (MOH, 2014). Female nurses can positively impact the attitudes and beliefs of female patients. They are also the first point of contact for female patients and their families/friends. In order to do this, it would be crucial to make sure that these young nurses have the necessary knowledge to share with their patients, family members, and friends.
Breast cancer awareness includes knowledge of the risk factors, signs, symptoms, and screening methods for breast cancer. Knowledge and awareness play a vital role in the early detection and optimal treatment of breast cancer. Creating awareness among female health workers could go a long way in enhancing awareness and early diagnosis of breast cancer. Identification of breast cancer at an early stage is the best way to prevent it and is of utmost importance in saving lives and improving the quality of life. These non-invasive methods of breast cancer detection using tears, sweat, and nipple aspirates are relatively convenient, simple, inexpensive, and free from risk or harm; hence, nurses should have the relevant knowledge and skills, such that they may create awareness at the community level. Studies on the knowledge of non-invasive breast cancer biomarkers, risk factors, and BSE practice in future nursing professionals in the age group of 18 to 23 years old are not yet available, despite the fact that numerous studies about breast cancer knowledge and BSE practice in female university students have already been presented (Hadi et al., 2010; Nemenqani et al., 2014; Yousuf, 2010). To assess the level of knowledge and skills among nursing students, KAP studies are required. The present study was conducted to assess KAP of nursing undergraduates about the non-invasive biomarkers of breast cancer in view of the increasing incidence of breast cancer in KSA.
The knowledge of nurses on the non-invasive biomarkers of breast cancer, such as nipple aspirates, breath, tears, and urine, are important determinants for the early diagnosis of breast cancer and for the reduction of the economic burden of the disease on the health care system.
Overdiagnosis leads to overtreatment due to mammographic screening in the case of dense breasts and inflicts considerable physical, psychological, and economic harm on many women (Autier & Boniol, 2018). The dense breast tissue is linked to a markedly reduced mammographic sensitivity and a higher interval cancer rate (Boyd et al., 2007; Bodewes, 2022; Kerlikowski 2007; Mandelson et al., 2000); thus, an increased understanding of breast cancer with relation to knowledge on non-invasive biomarkers, risk factors, and breast self-examination (BSE) practices is important to enable future nurses to extend better patient care and disease management by helping them in the early diagnosis of breast cancer and may reduce the mortality rate globally. To the best of our knowledge and based on a PubMed search, this is the first study dealing with the above mentioned issue in the XXX and XXX provinces in Saudi Arabia. Therefore, the present study was undertaken to assess the knowledge of non-invasive biomarkers of breast cancer, associated risk factors, and attitudes toward BSE among nursing undergraduates.
Methodology
Setting
Department of Nursing, Farasan Island.
Study design
A descriptive cross-sectional study.
Study sample
Female nursing undergraduates of the Department of Nursing.
Sampling procedure
Simple random sampling.
Study tool
A questionnaire was used as the research tool for data collection from the study participants.
There were nine sections in the questionnaire:
Section 1: Demographic Information. It included eight items (i.e., age, gender, marital status, residence, living with parents, study year, family's educational background, and family history of breast cancer)
Section 2: The Knowledge Evaluation Questions included 16 items.
Section 3: The domain for knowledge regarding non-invasive biomarkers of breast cancer had seven evaluation items.
Section 4: The domain for Awareness of Risk Factors had 12 items.
Section 5: Source of Information on Breast Cancer had six evaluation questions
Section 6: BSE practices and barriers to breast self-examination had three evaluation questions.
Section 7: Lifestyle characteristics had eight items.
Section 8 had six evaluation questions on the Knowledge of Treatment.
Section 9 had three items on knowledge regarding incidence rates and expenditures on breast cancer in KSA.
Ethical considerations
Sufficient research information was provided to the participants with the help of full informed consent. This was achieved via a consent form attached to the questionnaire. Full confidentiality was ensured. The rights of the participants were protected by the Helsinki Code of Ethics. The study was approved by the Head of Ethics Committee of the College (No. 1/1/1444H, 2022).
Data collection procedure
Formal approval was used to conduct this research. Consent was obtained from all the participants, and a free hand was given to the participants to participate in the study or refuse to participate.
Study timeline
Data collection was conducted from February to March 2022.
Inclusion and exclusion criteria
Regular students enrolled with a university during the academic year 2021–2022, and those who were not willing to participate, were excluded from the study.
Definitions
Breast self-examination
One's self-examination of her breasts to identify any changes.
Breast self-Examination performed
BSE done at least once within the duration of 12 months.
Sample size and sampling procedure
A sample size of 260 students was determined using Cochran's formula (1964): n = z2pq/e2, where p is the proportion of knowledge on breast cancer among female students (22%); e is the desired level of precision (5%); and z = 1.95 at CI 95% (Cochran, 1963). The calculation also included a 5% non-response rate. Simple random sampling was done. Reliability was calculated to check the internal consistency among items of the questionnaire using Cronbach's alpha (α) and was 0.875, which was considered within the acceptable range.
Data analyses
Data analyses were done using Microsoft Excel software. Descriptive statistics were used to summarize the data, which were then displayed in the tables and figures. The study's hypothesis was either accepted or rejected using inferential analysis and the t-test. Based on prior research on breast cancer risk factors, the most important risk factors for breast cancer were found to be breast density, obesity, age, menarche and menopause at different times, lifestyle, and diet (Engin, 2017). The current study used these risk factors to determine the participants’ knowledge of breast cancer and the risk factors. Correct responses were summed up to get the total knowledge scores for each participant. The connections between the sociodemographic characteristics of the participants and their understanding of the most significant risk factors for breast cancer were examined using Pearson's Chi-squared test. The threshold for significance was established at a P-value < .05.
Results
Demographic Features of the Study Participants
The participants were first- to fourth-year female nursing undergraduates, the majority of which constituted third-year study groups, followed by fourth-year study groups. The participants’ mean age was 21 years (SD = 21.3 ± 3.2; ranging from 18 to 25 years). Eighty seven percent of the study participants were unmarried, and 1% reported having a family history of breast cancer (Table 1).
Study Samples’ Distribution According to Their Demography, Knowledge, Lifestyle, and Dietary Habits (N = 260).

Significant at P value < .05; *Significant at P value < .05 based on Chi-squared test.
General Knowledge of Breast Cancer
General knowledge of breast cancer was significantly high (P < .05) among the respondents. Table 2 shows a comparison of the knowledge regarding the signs and symptoms of breast cancer among the participants. The participants belonging to higher study years were found to have more knowledge of breast cancer symptoms than those in the lower study years. The participants were found to be well-aware of the breast pain symptom (63.1%). A higher number of the study participants also recognized change in breast shape (88.8%) and painless lumps (55.8%) as breast cancer symptoms. However, some respondents were still unaware of nipple discharge (42.1%) and inverted nipples (16.9%) as breast cancer symptoms (Table 2). There was a strong correlation among the knowledge, study year, and marital status of the study participants (Table 3).
Participants’ Responses in Relation to Signs and Symptoms of Breast Cancer (n = 260).
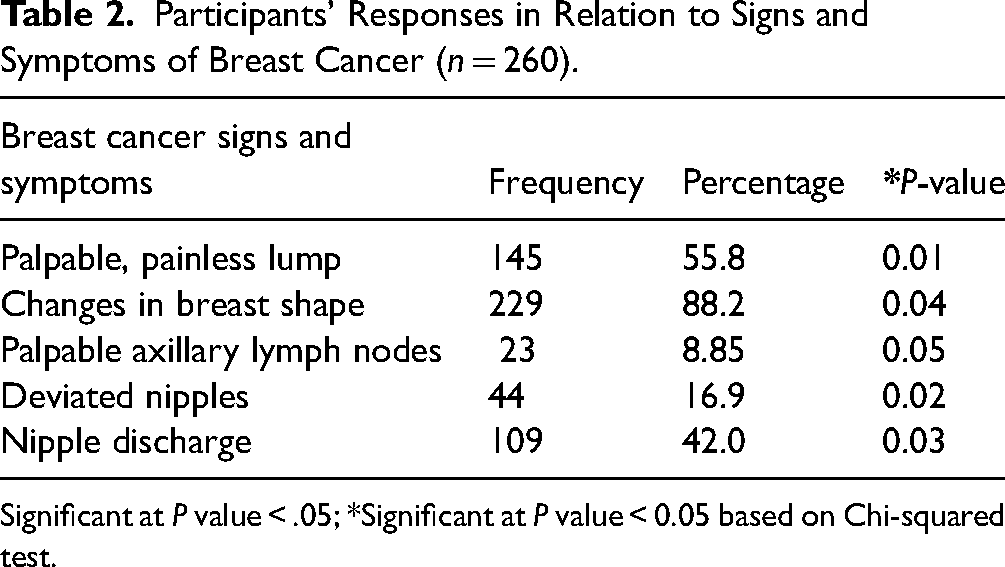
Significant at P value < .05; *Significant at P value < 0.05 based on Chi-squared test.
Correlation Between Study Years in the Program, Age, Marital Status, and Level of Knowledge of Study Participants (n = 260).

Significant at P value < .05; *Significant at P value < .05 based on the Chi-squared test.
General Breast Density Knowledge and Importance
Most participants were unaware that having dense breasts raises a woman's risk of breast cancer and can conceal tumors on mammograms (65%). The other risk factors mostly recognized by the study participants were advanced age (76.2%), genetic mutation (66.9%), smoking (86.9%), alcoholism (88.1%), stress (69%), obesity (47.7%), and early or late onset of menstruation and menopause (48.1%). The participants were unaware that breast cancer can happen at a young age and has the worst prognosis (12.3%).
Knowledge Regarding Non-Invasive Biomarkers
The knowledge of the study participants about non-invasive biomarkers was significantly low (P < .05) as a very low percentage of the study participants (27%) responded that they were aware of these non-invasive biomarkers (Figure 1). The majority of the participants marked this as ‘No’ and were found to be confused. They marked it ‘Maybe’ as a response to these evaluation questions.

Participant for Knowledge of Non-invasive biomarkers of Non-blood origin.
Knowledge Regarding Risk Factors
The majority of the participants (78.5%) were not aware of breast density as a risk factor for breast cancer. However, the study participants identified alcohol containing perfumes (89.1%), excessive alcohol consumption (88.1%), genetic mutation and positive family history of breast cancer (66.9%), and waist circumference/obesity (61.2%) as established and most important risk factors of breast cancer. The participants also identified stress, poor dietary habits, and fewer physical activities as the major modifiable risk factors. Accordingly, 47.7% of the participants identified no breastfeeding as one of the significant risk factors for breast cancer. However, their knowledge of the other associated risk factors of breast cancer was poor.
Majority of the study participants (69.7%) identified age as the major non-modifiable risk factor for breast cancer. However, very few participants were aware of the risk of breast cancer due to disruption in biological clock like early menarche, late menopause, and hormonal therapy. It was also found that their knowledge of the modifiable and non-modifiable risk factors was unsatisfactory.
Knowledge of BSE Practices
The study participants had less knowledge about BSE practices, with the majority responding that they did not know how to perform BSE (77.3%). In fact, 52.7% of the participants responded that they had never done BSE (Table 4). There was a significant correlation between breast self-examination practice and age (P < .05) as those few students (22.7%) who were doing breast self-examination practices every 2–4 months belonged to a higher study year.
Examination Practice Among Study Participants (n = 260).

Barriers of BSE Practices
The study participants cited “Not knowing how to perform breast self-examination” as the most common reason for not performing the breast self-examination (45.4%, Table 1), fear of a positive diagnosis (27.3%), thinking they were not at risk as all were in their teens and hence not required (27.3%), and lack of time (11.54%).
Knowledge of Source of Information Regarding Breast Cancer
Regarding the source of information, the majority of the participants identified the internet as the major source of information, followed by government health programs.
Knowledge of Global and National Incidence Rates and Epidemiology of BC
The majority of the participants did not have sufficient knowledge regarding the epidemiology, incidence, and current trends of breast cancer at the global and national levels (Table 5). Furthermore, knowledge regarding the incidence rates and health care expenditure by the government on breast cancer was also significantly low (P < .05).
Knowledge Regarding Incidence Rates and Expenditure on Breast Cancer in the KSA (n = 260).

Significant at P value < .05; *Significant at P value < .05 based on the Chi-squared test.
Discussion
The high incidence rates of breast cancer could be caused by a number of factors, including an aging population, an increase in risk factors, the widespread use of mammography screening (Srivastava et al., 2019) for detection, age (Britt et al., 2020; NCD, 2017), and changes in population and epidemiology (Blüher, 2019; Hu et al., 2013; Møller et al., 2002; NCD, 2017; Zhang et al., 2012). The most crucial steps to reducing breast cancer-related mortality are acquiring knowledge and performing skill-based interventions required for early diagnosis.
Nevertheless, mammography has certain drawbacks, one of which is its inability to identify breast cancer. The range of mammographic sensitivity for identifying breast cancer in a randomized, controlled mammography screening experiment was 71% to 96% (Humphrey et al., 2002). Mammographic sensitivity decreased even further in patients with dense breast tissue, that is, from 48% to 70% (Humphrey et al., 2002; Pisano et al., 2005). For women with thick breasts, ultrasonography is more sensitive than mammography in identifying lesions (Skaane, 1999; Zonderland et al., 1999). Nevertheless, the majority of microcalcifications, which are characteristic findings in ductal carcinoma in situ, are also missed by ultrasonography. Ductal carcinoma in situ accounts for 75% of the tumors that ultrasonography misses, while invasive carcinomas account for 25% (Nemec et al., 2007).
In the KSA, despite the healthcare facilities being free of charge with widespread screening services, even in shopping malls, as community service activities, the utilization of breast cancer screening methods, including mammography, and screening rates is not optimal and are very low, respectively, with one study reporting that for women 50 years of age or older, 89% reported not having a clinical breast examination, and 92% reported never having a mammogram in the past year (Bcheraoui et al., 2015).
Studies have reported that ease of collection, high protein concentration, and lower complexity of the tear fluid compared to blood make tears an ideal diagnostic fluid (Ponzini et al., 2022; Ravishankar & Daily, 2022; Zhou & Beuerman, 2017). Additionally, low-molecular weight proteins are easily accessible in tear fluids and can aid in identifying crucial cancer biomarkers (Hagan et al., 2016). The study conducted by Leemans et al. (2022) demonstrated that volatile organic compounds in sweat differ between healthy individuals and breast cancer patients, suggesting the possibility of using these compounds as novel breast cancer biomarkers in non-invasive screening tools.
Phillips et al. (2003), Peng et al. (2010), Phillips et al. (2010), and Patterson et al. (2011) reported that breath analysis exhibits potential in cancer screening and early diagnosis because it is an easy, safe, painless, and non-invasive procedure that poses no risks to patients. Increased oxidative stress and the induction of cytochrome P450 enzymes are associated with BC. This leads to the lipid peroxidation of polyunsaturated fatty acids in cell membranes, which increases the production of volatile alkanes and alkane derivatives in the breath and ultimately affects the amount of volatile organic compounds in exhaled breath (Patterson et al., 2011; Peng et al., 2010; Phillips et al., 2003, 2010). Peng et al. (2010) also demonstrated that women with breast cancer have increased levels of 3,3-dimethyl pentane in their breath. However, the participants of this study had very little knowledge about the typical changes in breath odor in breast cancer patients.
Human urine is also one of the most useful biofluids of non-blood origin, which serves as an important biomarker of various diseases, including breast cancer. Studies have demonstrated increases in phosphotidylcholine and phosphotidylethanolamine in the urine samples of breast cancer patients (Beretov et al., 2015). Fifty-nine urinary proteins were differentially detected in breast cancer patients (Beretov et al., 2015). Furthermore, the biomarkers in nipple aspirate fluids could also be a better source for the identification of breast cancer as they contain exfoliated breast epithelial cells from which breast cancer originates (Sauter et al., 1997).
However, the study participants, who are future nursing professionals, had almost negligible knowledge regarding these noninvasive biomarkers that could be utilized as sensitive tools for creating awareness, which could help in early diagnosis and reduce the severity and mortality due to knowledge gaps.
Moreover, the participants reported breast cancer risk factors that were almost similar to those reported in various previous studies, such as older age, high body mass index or obesity, exposure to tobacco, physical inactivity, high-fat diets, early-age menarche, late age at first full-term pregnancy, shorter breastfeeding periods, use of hormonal menopausal therapy or oral contraceptives, breast density, and family history of breast cancer (Kushi et al., 2012).
Most of the research participants were unaware that dense breasts have a masking effect on mammographic screening, increasing their intrinsic risk of developing breast cancer. Therefore, more work has to be done to increase the students’ understanding of the various types of breast tissue and the increased risks of breast cancer.
The study participants were also almost unaware of the severity of breast cancer at such a young age. Several studies have shown that breast cancer arising at a young age is linked with a worse prognosis. Various studies have suggested that BC at a young stage is enriched with more aggressive breast cancer subtypes, particularly triple-negative or basal-like tumors (Azim & Partridge, 2014; Azim et al., 2020). In the study of Heena et al. (2019) among health professionals, the study participants were also found to have less knowledge and awareness about breast cancer, screening, and attitude.
The inadequate breast cancer knowledge determined in this study is in line with the results obtained for a study conducted among female university students in Saudi Arabia, which reported that only 4.2% of the study participants have adequate knowledge about BSEs (Albeshan et al., 2023). In another study conducted among Palestinian females by Jobran et al. (2023), the majority of females (68.7%) scored poorly on their knowledge of BC considering possible risk, methods of detection, methods of diagnosis, methods of treatment, signs and symptoms, information about mammography, and other knowledge questions. Only 31.7% scored well.
In contrast to this, the study conducted on female university students in Gambia by Kinteh et al. (2023) revealed that they had good knowledge regarding breast cancer screening. Abo Al-Shiekh et al. (2021), in their study on female university students in Gaza, found that the majority of students (80.2%) had acquired previous information about breast cancer from different sources, including university studies (57%), the internet (45%), and social media (41%). Findings showed good scores (≥70%) for the signs and symptoms and risk factors of breast cancer. Roughly, all students (96.5%) have heard about BSE, and 69.8% knew the time to do BSE; however, only 31.4% of them practice it regularly.
Similar to our study, the work of Abo Al-Shiekh et al. (2021) also reported that the three main barriers to BSE practice were students who do not have a breast problem (39.7%), do not know how to do it (37.9%), and are busy (31%). More than three-quarters (76.6%) of the respondents had never practiced any form of breast cancer screening. Kinteh et al. (2023) revealed almost similar results, where more than three-quarters (76.6%) of the respondents had never practiced any form of breast cancer screening. Alotaibi et al. (2018) reported that most of the participating students had never performed BSE (82%). Other researchers, however, who investigated the reasons for not practicing BSE, found that a lack of knowledge was the main reason. Alzabadi et al. (2017), Birhane et al. (2017), and Hassan et al. (2017), for example, reported that most students did not perform BSE because of insufficient information and skills about its steps. Findings of our study on reasons for the majority of the study participants not doing BSE practices also corresponded to the results of these studies.
None of the studies investigated the specific knowledge of the non-invasive biomarkers of breast cancer among female nursing undergraduates. The results of the present study revealed inadequate knowledge of the non-invasive biomarkers of BC, such as sweat, urine, breath odor, and nipple aspirates, for breast cancer detection.
The study findings confirmed that the study population had inadequate knowledge of the non-invasive biomarkers of breast cancer at baseline. A training program should be implemented to increase the level of knowledge about the non-invasive biomarkers of BC and BSE practice because, when educated youth are well aware of the disease and its early diagnosis procedures, they can create community awareness about the easy and early diagnosis of breast cancer using breath, sweat, and other non-invasive biomarkers discussed in this study. The outcomes of this study could be useful for policymakers to chalk out policies by focusing more on knowledge-building measures about the non-invasive biomarkers of breast cancer and knowledge of the breast self-examination technique, which would help in controlling the incidence of the disease and preventing its adverse outcomes on the quality of life.
Conclusion and Recommendations
In summary, there appears to be a broad general awareness about breast cancer among the study participants. However, only a small portion have a thorough understanding and knowledge of breast cancer, despite the fact that most of them have heard of the disease. Programs for educating nursing professionals about breast cancer symptoms, non-invasive biomarkers, and prevention should be launched, especially at the university level.
Knowledge- and skill-based interventions are required for early diagnosis using sensitive non-invasive biomarkers, such as changes in the smell of sweat, breath, or discharge from the nipples. This would help in better managing the disease, reducing the psychological load, and improving the quality of life of affected people. In view of the lesser percentage of study participants with knowledge of BSE practice, it is advisable that BSE knowledge and practice be incorporated into the nursing program.
Limitations
The main limitation of the study was the small sample size. A cross-sectional study sample should be large so as to get accurate findings from the study participants.
The self-report questions for the young nurses were another limitation of this study because of their bias.
Strength
The published data on breast cancer knowledge among nursing undergraduates are totally lacking from this very important island, which is now registered under UNESCO for its immense underwater wealth; hence, the study outcomes will advance our understanding of the existing knowledge on breast cancer and will add to the global efforts of the WHO to better understand and manage the disease.
Footnotes
Acknowledgments
The authors are highly grateful to the dean of the college, Dr. Afaf Mohammad Babeeir, for providing the necessary facilities for the electronic submission of the manuscript and providing a highly conducive work environment. The authors gratefully acknowledge the Writefull Tool from Hindawi, which was used for language check/editing prior to the submission of the manuscript. The authors are also grateful to the dean of the main campus’ College of Nursing, Dr. Mohammad Arishi, for promoting research and development activities for the nursing program. Thanks are also due to the participants who willingly participated in the study. They highly appreciate the active participation of Ms. Samar Ageely and Ms. Mead, the graduates of the Department of Nursing, Farasan Campus, Jazan University in the KSA in the data collection.
Authors’ Contributions
Dr. Shabihul Fatma Sayed conceptualized and designed the study and performed sampling and analyses, statistical analyses of the data, and manuscript writing. Dr. Hamad G. Dailah and Dr. Sumathi Nagarajan participated in data analyses and manuscript reviews. Dr. Siddig Ibrahim Abdelwahab and Dr. Shaived Shabeehul Hasan Abadi took part of the statistical analyses and manuscript writing. The manuscript was critically reviewed by Dr. Shabihul Fatma Sayed. All authors have given final approval of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Considerations
The study has been conducted in full accordance with the ethical guidelines of Jazan University, and has been approved by the College Ethical Committee (No. 1/1/1444H, 2022). Sufficient research information was provided to the participants with the help of full informed consent, and this was achieved via a consent form attached to the questionnaire. Full confidentiality was ensured. The rights of the participants, were protected by the Helsinki Code of Ethics.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.