
Abstract
Introduction
Sucrose is an evidence-based intervention used for short-term pain management and distress from minor procedures. Limited research exists on nurses’ knowledge and use of sucrose in Neonatal Intensive Care Units in Saudi Arabia.
Objective
To assess nurses’ knowledge and use of sucrose in Neonatal Intensive Care Units in Saudi Arabia.
Methods
A cross-sectional online survey was used to collect data from a convenience sample of 68 neonatal intensive care nurses in Saudi Arabia. A modified tool assessed the knowledge and use of sucrose. Logistic regression analysis was used to find the predictors for sucrose use.
Results
Most respondents never used sucrose for neonatal pain management and did not receive any training on sucrose. The mean knowledge of nurses regarding sucrose and its use was very low (38%): 16% had a high level of knowledge regarding sucrose, 13% moderate, 19% low, and 52% very low. Nurses who received training on sucrose use and nurses who read or heard about sucrose predicted the use of sucrose.
Conclusion
Nurses’ knowledge and use of sucrose were inadequate. Interventional programs are needed to enhance the nurses’ knowledge regarding sucrose and its use and to enhance the utilization of sucrose as a pain management intervention in the Neonatal Intensive Care Units in Saudi Arabia.
Introduction
Evidence from clinical research has demonstrated that newborns are more sensitive to pain than older babies. Newborn's procedural pain may be induced by various diagnostic and treatment procedures, including vitamin K injections, vaccinations, blood glucose checks, intravenous catheter insertion, and blood collection for diagnostic procedures (Stevens et al., 2018). Pain and discomfort associated with painful procedures are among the most common causes of pain in newborns. In the Neonatal Intensive Care Unit (NICU), it has been reported that a newborn has roughly 11 painful procedures daily (Roofthooft et al., 2014; Stevens et al., 2011). Heel sticks to get a small amount of blood for diagnostic purposes, for example, checking blood gas levels, is the most prevalent procedure performed on neonates, and it is often completed without analgesics (Hsieh et al., 2018).
Painful stimuli in newborns may elicit negative behavioral, physiological, and cognitive responses, which may affect the long-term neurodevelopmental consequences (Hsieh et al., 2018). Untreated pain in early infancy could lead to distress, increased pain sensitivity, decreased immune system functioning, increased avoidance behavior, and social hypervigilance (Valeri et al., 2018). Untreated pain in neonates is associated with a variety of long-term negative health consequences, including tissue damage and injury, as well as progressive changes in central nervous system (CNS) functions, which may impair the behavioral component of pain experienced later in life if left untreated (Hsieh et al., 2018). Therefore, procedure-related pain in newborns needs immediate treatment from the practitioner to avoid short- and long-term consequences in children.
Pharmacological and non-pharmacological interventions can be used to manage a newborn's pain. Pharmacological interventions include using medications such as morphine and paracetamol. Non-pharmacological interventions include using non-medication strategies to reduce or relieve pain, including breastfeeding, kangaroo care, and sweet-tasting solutions (Hsieh et al., 2018; Perry et al., 2018). Sweet-tasting solutions (e.g., sucrose 24%) have analgesic properties, and as a result, they are employed as analgesics in the treatment of newborn procedure-related discomfort (Gao et al., 2016; Harrison et al., 2012; Stevens et al., 2016).
Review of Literature
Sucrose Use
Sucrose 24% can be used for procedural pain when breastmilk is unavailable, and neonates can tolerate a small amount of oral intake (Velumula et al., 2022). Sucrose 24% can be administered by nurses without a physician's prescription, which may enhance and speed up the management of newborns’ pain (The Royal Children's Hospital Melbourne, 2021). It is also inexpensive and easy to administer. It could be administered 2 min before the minor painful procedures, for example, heel pricks. A small amount (from 0.05 mL if the infant is nil orally up to 0.25 mL) of sucrose 24% can be effective to reduce the neonatal from minor procedures. Sucrose 24% can be applied directly onto the infant's tongue or on a dummy. Sucrose 24% is used for short-term neonatal pain as its analgesic effect is short from 5 to 8 min. Sucrose 24% can be used as an adjunct to strong analgesics during procedures that may cause severe pain, for example, chest drain insertion (Harrison et al., 2012; Kassab et al., 2021; Stevens et al., 2018; The Royal Children's Hospital Melbourne, 2021; Valeri et al., 2018).
Sucrose Safety
Research reveals that sucrose 24% is safe with no or minimal adverse events for neonatal pain management (Gray et al., 2015; Li et al., 2022; Potana et al., 2015; Stevens et al., 2016; The Royal Children's Hospital Melbourne, 2021). As reported by a study in 2005, chocking and desaturation are potential harms of oral sucrose (Grabska et al., 2005). However, this may be applied to any oral intake, not only sucrose. More recent studies did not observe any chocking or desaturation after oral sucrose administration (Dilli et al., 2014). One study observed one mild episode of spitting up after oral sucrose (Tutag Lehr et al., 2015). Another research reported no episode feeding intolerance, high glucose level, or necrotizing enterocolitis post oral sucrose (Potana et al., 2015). Another study found no significant short-term neonatal neurobehavioral effects post-oral sucrose (Banga et al., 2016).
Factors Influencing Sucrose Use
There are many factors influencing the use of evidence-based practice interventions to manage neonatal pain including patients, healthcare professionals, and organizational factors (Alburaey et al., 2020; Cheng et al., 2017; Ismail, 2016; Neshat et al., 2021; Perry et al., 2018). Sucrose is no exception. These factors include the availability and trust in the evidence, the existence of a policy, the leader's support, staff awareness, knowledge and time, and training (Alburaey et al., 2020; Neshat et al., 2021; Perry et al., 2018). Neonatal nurses should be informed of the efficacy of various pain-management options and utilize evidence-based practice to choose the most suitable therapy for neonatal pain when dealing with a baby in distress (Kyololo et al., 2021). Nurses’ knowledge and perspective may have an impact on their care behavior (Kassab et al., 2021).
Sucrose Research in Saudi Arabia
Few studies conducted in Saudi Arabia with regard to sucrose use for neonatal pain. One study reported that sucrose was used for procedural neonatal pain management by only 16% of the NICU nurses in Saudi Arabia (Alburaey et al., 2020). Another study on sucrose conducted in Saudi Arabia found that sucrose 24% solution combined with pacifier produced significant reduction in pain scores in preterm neonates admitted to the NICU compared to water with pacifier (p < .05) (Elserafy et al., 2009). As the research is limited regarding the use and knowledge of NICU nurses of sucrose as a non-pharmacological intervention (within the scope of nursing practice to administer) in Saudi Arabia, it is worthy to assess the knowledge and use of sucrose by NICU nurses in Saudi Arabia.
Methods
Research Design
This research used a descriptive cross-sectional online survey to assess the knowledge and use of sucrose in NICU nurses of Saudi Arabia. Data collection took place between January and April 2023.
Sample and Setting
Neonatal intensive care nurses from three level III NICUs in Saudi Arabia (governmental, private, and military) were invited to complete an online survey. Participants had the chance to complete the survey when they were on duty or outside the work setting. The inclusion criteria were nurses working in level III NICU, minimal 6 months NICU experience, and able to read and write English as the study tool in English. The study link and QR code were shared by email and direct sharing to 120 nurses representing the total number of NICU nurses in the three hospitals.
Data Collection Tool
A previously published questionnaire on nurses’ knowledge management in neonates was modified with permission from the developer (Kassab et al., 2021). The modified instrument consisted of four parts. These included the Demographic Data Sheet, items related to sucrose use, items related to nurses’ knowledge of neonatal pain, and items related to nurses’ knowledge of oral sucrose as non-pharmacological pain management for neonates. The participants rated their responses on knowledge items on a three-point scale (1 = correct, 2 = don’t know, 3 = incorrect). Examples of the items for nurses’ knowledge of oral sucrose are “Oral sucrose as a pain management intervention is effective to manage neonatal pain” and “Oral sucrose with non-nutritive sucking (pacifier dipped in sucrose) is more effective to manage neonatal pain.” The content validity of the tool was established by a panel of six experts in nursing, research, NICU, and pain management. The content validity index was very good (0.82). The internal consistency reliability of the knowledge regarding neonatal pain and knowledge of sucrose was established using the Kuder-Richardson 20 (KR-20), which was high (0.93 for the knowledge regarding neonatal pain and 0.99 for the knowledge regarding sucrose use).
Data Collection Procedure
After obtaining ethical approvals for the study from Fakeeh College for Medical Sciences and from Ministry of Health, the Principal Investigator visited the three hospitals and introduced the study to the NICU nurses and managers including the study aim and expected outcomes. The survey link and QR code were shared with the participants directly and by email. The first page of the online survey ensured that participation was voluntary and anonymous. No identifications were collected. The consent was implied by agreeing to participate and completing the survey.
Data Analysis
The statistical package for the Social Sciences (SPSS, IBM Version 26) was used to analyze the data. Frequencies and percentages were used to summarize the categorical variables. Means and standard deviations were used to summarize the continuous variables. Multiple binary logistic regression analyses were used to identify the predictors for sucrose use. One of the independent variables in the model was the knowledge regarding sucrose and its use. This was used to identify if the knowledge regarding sucrose is a significant factor for the use of sucrose.
Ethical Considerations
Ethical approval was obtained from Fakeeh College for Medical Sciences (355/IRB/2022). Informed consent was implied by agreeing, completing, and submitting the survey. The study was anonymous and voluntary. No identifiers were collected from the participants. A secured platform (SurveyMonkey) was used to collect the data from the participants. Data were kept confidential; no one can access the data except the researcher. Data were stored using a password. Data will be destroyed by secure deletion after 5 years of results publication.
Results
A total of 68 NICU nurses completed the survey. The mean age of the participants was 32.9 (SD = 5.42). The mean years of experience in neonatal care was 6.6 years (SD = 4.82). Majority were female (82%). About 49% of the participants were single, 46% were married, and the remaining 5% were either widowed or had other marital statuses. The majority of participants (70.6%) were Saudi, while the remaining 29.4% were non-Saudi. Regarding education, the majority of the participants (79.4%) held a bachelor's degree in nursing, while 14.7% held a master's degree or higher, and the remaining 5.9% held a college diploma in nursing. Most of the participants worked in governmental hospitals (53%), followed by military hospitals (33.9%), and private hospitals (13.2%) (Table 1).
Participant Demographics.

The majority of respondents reported not having received any training on the use of sucrose for neonatal pain management (81%), 72% reported never used sucrose for neonatal pain management, and 59% reported having heard or read about the use and benefits of sucrose for neonatal pain management.
Mean knowledge regarding neonatal pain was high (mean = 83%, SD = 22%). The highest item that participants answered correctly was “neonates are capable of experiencing pain” (94%), and the lowest answered item was “neonatal pain has long-term adverse effects” (72%) (Table 2).
Knowledge of NICU nurses of neonatal pain.

For the knowledge level regarding neonatal pain classification, 79% had a high level of knowledge, 12% moderate, 3% low, and 6% very low (Figure 1).
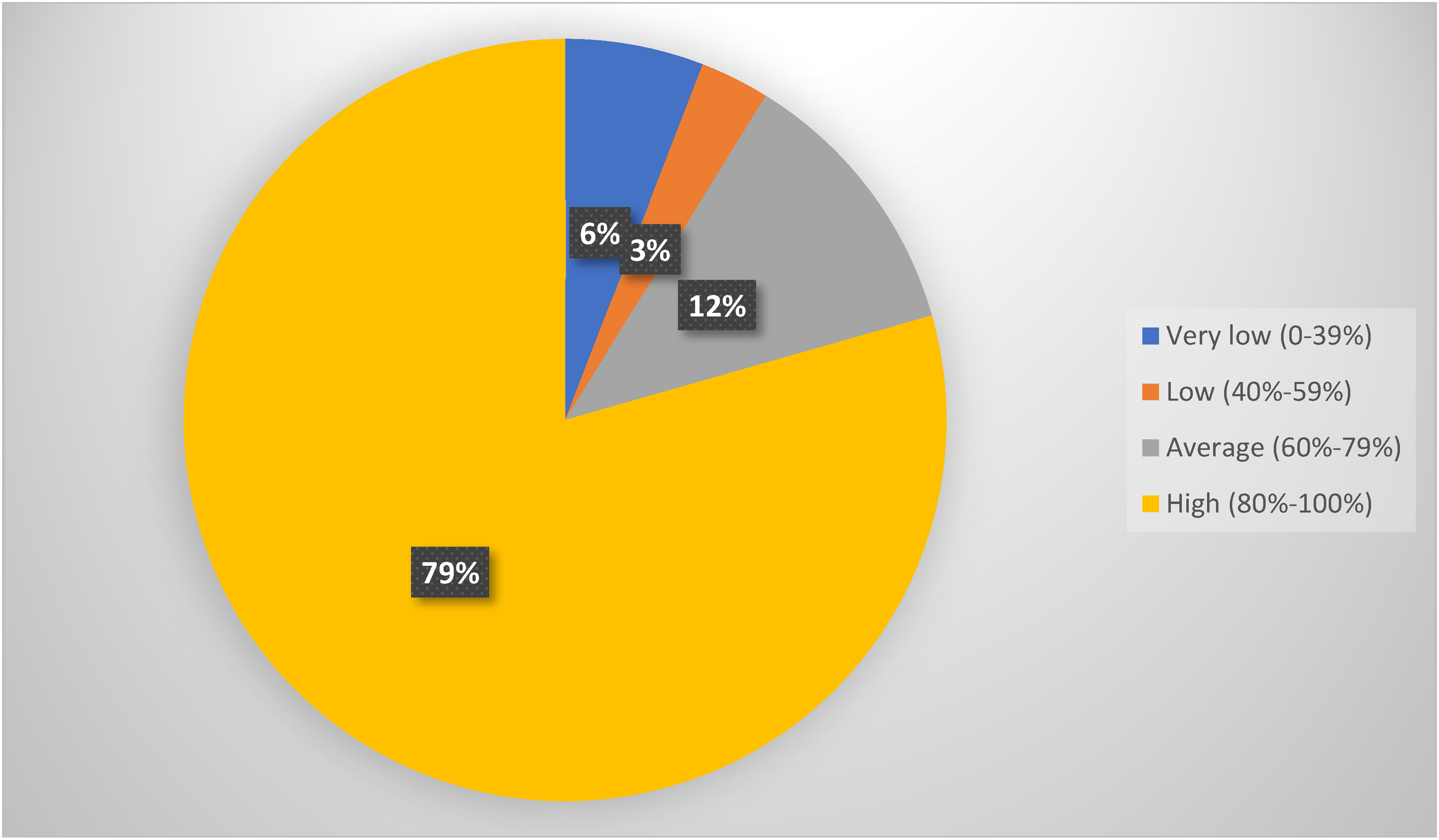
NICU nurses knowledge level of neonatal pain.
The mean knowledge of NICU nurses regarding sucrose use was very low (38%, SD = 0.30). The mean answers in the majority of the items were low or very low (Table 3).
Knowledge of NICU nurses regarding sucrose use.

For the knowledge level regarding sucrose use, 16% had a high level of knowledge, 13% moderate, 19% low, and 52% very low (Figure 2).

NICU nurses knowledge level of sucrose use for neonatal pain.
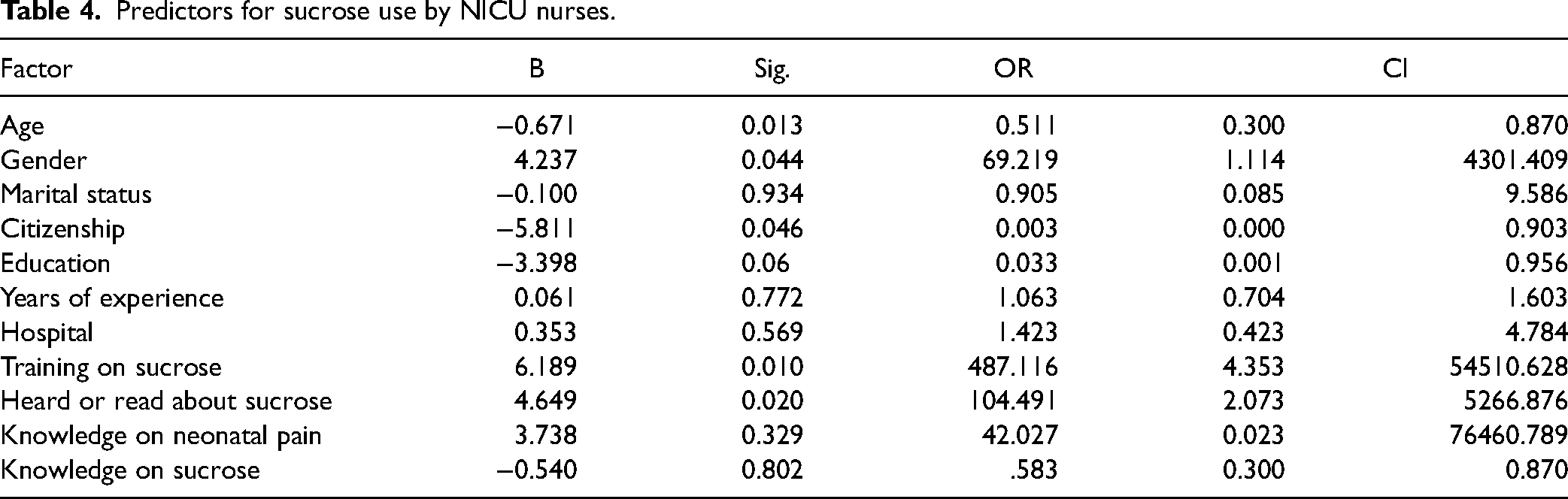
Predictors for sucrose use were younger nurses, male nurses, Saudi nurses, nurses who received training on sucrose use, and nurses who read or heard about sucrose (p ≤ .05). Knowledge regarding neonatal pain and knowledge regarding sucrose were not significant predictors of sucrose use (Table 4).
Predictors for sucrose use by NICU nurses.
Discussion
The majority of respondents never used sucrose for neonatal pain management and did not receive any training on sucrose. Although the mean knowledge of NICU nurses regarding neonatal pain was high, the mean knowledge regarding sucrose use was very low. Nurses who received training on sucrose use and nurses who read or heard about sucrose predicted the use of sucrose.
The findings of the study showed that most of the respondents have never used sucrose for the management of neonatal pain despite the fact most of NICU nurses have come across the benefits of sucrose in the management of pain neonatal. The results of this study are consistent with a recent study conducted in Saudi Arabia that indicated that the majority of doctors and nurses did not use sucrose for pain relief in the NICU in Saudi Arabia despite having adequate knowledge on neonatal pain. One of the reasons might be most of the participants have not received the training on neonatal pain management (Alburaey et al., 2020). However, the benefits of sucrose in managing neonatal pain have been described by several studies (Harrison et al., 2012, 2017; Stevens et al., 2016, 2018).
The knowledge of NICU nurses regarding neonatal pain was high. The results of this study indicated that nurses were aware that neonates experience pain, minor procedures can cause pain to neonates, preterm neonates are at greater risk of neurodevelopmental impairment due to repeated painful procedures, and that neonates, especially preterm infants, are more sensitive to pain than older children and adults. The results of this study are consistent with previous research. A study from Brazil found that most NICU nurses were aware that premature infants and newborns can experience pain (Costa et al., 2017). Another study from Jordan found that the majority of NICU nurses believe that neonates experience pain and they are at a greater risk for neurodevelopmental impairment because of repeated painful procedures (Kassab et al., 2021).
The knowledge of the NICU nurses regarding sucrose was low. Majority of the participants did not identify the recommended dose, frequency, and painful procedures that require oral sucrose. Research shows that a small amount of 24% oral sucrose (0.1 ml) is effective to manage neonatal pain during painful procedures (Bueno et al., 2023; Gao et al., 2016; Stevens et al., 2018). Sucrose can be administered 2 min prior to the procedure and repeated if moderate to severe distress observed (Bueno et al., 2023). Majority of the NICU nurses in this study did not know that analgesic effect of oral sucrose can last for few minutes and the need for repeated doses. It was reported in many guidelines and research that sucrose analgesic effects last from 5 to 8 min (Harrison et al., 2012; The Royal Children's Hospital Melbourne, 2021). Majority of the NICU nurses in this study also were not aware that oral sucrose is more effective when combined with non-nutritive sucking. Previous research shows that sucrose in combination with non-nutritive sucking, for example, pacifier provides more effective analgesic effect than sucrose alone (Stevens et al., 2016).
Multivariate analysis showed some factors were associated with more sucrose use for neonatal pain. These include young, male, Saudi nurses, previous training, and previous exposure to knowledge regarding sucrose. Previous research shows many factors influencing the use evidence-based interventions among neonates including patients, healthcare professionals, and organizational factors (Cheng et al., 2017; Ismail, 2016). For example, a study from China found that clinical experience of healthcare professionals, culture of work, leadership characteristics, existence of evaluation and facilitation processes have impact on the implementation of evidence-based interventions such as interventions related to neonatal pain management (Yue et al., 2022). Even though the use of oral sucrose 24% is considered standard practice in many countries, NICU nurses in Saudi Arabia reported minimal use of sucrose. More research is needed to know why sucrose is not being used by NICU nurses in Saudi Arabia. These factors may include the availability of sucrose, the existence of a policy, the leader's support and training. Neonatal nurses should be informed of the efficacy of various pain-management options and utilize evidence-based practice to choose the most suitable therapy for neonatal pain when dealing with a baby in distress (Kyololo et al., 2021). Interventional programs including training and policy development are needed to enhance the use of sucrose 24%. Nurse administrators and decision makers should adopt evidence-based practice regarding sucrose 24% use in the NICU.
Limitations
There were several limitations to this study that compromise its generalizability beyond the settings where the study conducted. The first limitation is that the study used a self-administered questionnaire during data collection, and therefore bias in answering the questions. Observational studies may provide alternative method especially when assessing the practice. The second limitation of this study is that this study recruited small sample. Therefore, future research should recruit more sample from many areas in Saudi Arabia especially when using multivariate analysis which require large sample size.
Implications for Practice
As the use of sucrose was inadequate, NICU nurses should increase the use of sucrose 24% for painful procedures. Oral sucrose 24% is an evidence-based practice within the scope of nurses who can promptly apply to manage neonatal pain during painful procedures, which in turn relieving unnecessary pain that neonates experience. However, sucrose use depends on the availability of the product, policy supporting its use, and training on its use. Therefore, nurse administrators and decision makers should adopt such evidence-based practice, develop policy to regulate the practice, provide the product, and training sessions on sucrose use.
Conclusion
Neonatal ICU nurses in Saudi Arabia had adequate knowledge regarding neonatal pain, but they had inadequate knowledge regarding sucrose and its use for pain management. Sucrose was not adequately used by the NICU nurses in Saudi Arabia. Interventional programs are needed to enhance the NICU nurses’ knowledge and use of sucrose 24% for neonatal pain management. These programs should mitigate the modifiable factors identified by this study by providing training on sucrose 24% and its use in the NICU in Saudi Arabia.
Footnotes
Acknowledgments
The authors extend their sincere thanks to all NICU nurses who participated in this study.
Author Contribution
A.I.: conceptualization, supervision, data collection, analysis, and writing the manuscript. S.F.: conceptualization, data collection, and writing the manuscript. A.H.: writing the discussion and original draft preparation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Considerations
Ethical approval was obtained from Fakeeh College for Medical Sciences (355/IRB/2022). Informed consent was implied by agreeing, completing, and submitting the survey. The study was anonymous and voluntary. No identifiers were collected from the participants. A secured platform (SurveyMonkey) was used to collect the data from the participants. Data were kept confidential; no one can access the data except the researcher. Data were stored using a password.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.