
Abstract
Introduction
While practice guidelines support clinical decision-making for optimal patient outcomes, there is often nonadherence to practice guidelines in implementing evidence-based interventions.
Objectives
This article aimed to assess adherence to practice guidelines in emergency obstetric and newborn care (EmONC) and the outcome of pregnancy in cases of obstetric complications in referral hospitals.
Method
The study employed a descriptive design. A purposive sampling technique was used to select the three tertiary hospitals and six out of nine state hospitals in Osun State. A data extraction form developed based on a fidelity framework was used to collect data on Adherence from 264 cases of obstetric complications. Descriptive statistics, such as frequency and percentage, and inferential statistics, such as chi-square, were done with the significance level set as p < .05.
Results
Findings showed low adherence to practice guidelines in 70.8% of hemorrhage care, 52.0% of fetal distress care, 60.0% of prolonged obstructed labor care, and 44.4% of preeclampsia/eclampsia care. The study's findings also showed that 64.3% of cases of prolonged/obstructed labor, 54.9% of cases of fetal distress, and 46.7% of all cases of obstetric complications were referred out at the state hospitals. Neonatal mortality in state and tertiary hospitals was 3.7% and 21.7%, respectively, which was significantly different (p < .001).
Conclusion
There was low adherence to practice guidelines for the implementation of EmONC in state and tertiary hospitals, and a significant number of cases of obstetric complications were referred out in the state hospitals. The low adherence to practice guidelines and numerous referrals truncate the successful implementation of EmONC and hinder women and newborns from receiving optimal care for obstetric complications. There is a need to develop strategies that promote adherence to practice guidelines in implementing EmONC.
Keywords
Introduction
In Nigeria, many women and neonates face negative health outcomes and are dying from obstetric complications. Nigeria presently has one of the worst neonatal mortality rates in the world, with 38 newborn deaths per 1,000 births (National Population Commission (NPC) [Nigeria] and ICF International, 2019). Nigeria also accounts for 23% of global maternal mortality, with an estimated maternal mortality ratio of 917 maternal deaths per 100,000 live births (World Health Organization, 2019). Many of these deaths resulting from obstetric complications are unpredictable but can be prevented with Emergency obstetric and newborn care (EmONC) provided by skilled birth attendants (Hussein et al., 2012).
While practice guidelines are evidence-based recommendations to guide healthcare providers in providing care, and support clinical decision-making to ensure quality care and optimal patient outcomes, they are often not followed in practice (Barth et al., 2016). Adherence to practice guidelines results in intervention success, and sub-standard care indicates ineffective implementation of evidence-based interventions (Muntinga et al., 2015; Visser et al., 2018). The high maternal and newborn mortality in Nigeria may be related to EmONC implementation for the management of obstetric complications in healthcare facilities. Measuring adherence to practice guidelines is essential in providing valuable information on whether high maternal and newborn mortality despite EmONC implementation is due to failure to implement EmONC as intended.
Review of Literature
In Nigeria, many women and newborns die from obstetric complications and lack of EmONC (Ewere & Eke, 2020). Many newborn deaths result from preterm birth, sepsis, and asphyxia. Also, over 70% of maternal deaths result from five obstetric complications: hemorrhage (antepartum and postpartum hemorrhage), severe preeclampsia and eclampsia, peripartum sepsis, prolonged/obstructed labor, and unsafe abortion with hemorrhage as the leading cause of direct maternal mortality in Nigeria (Ayenew, 2021; Izugbara et al., 2017). Research shows that about 40% of newborn deaths and many maternal deaths could be averted with EmONC (Hou et al., 2022).
Emergency obstetric and newborn care is an effective strategy to reduce maternal and newborn morbidity and mortality resulting from obstetric complications. Emergency obstetric and newborn care is a package of seven to nine signal functions which include: the use of uterotonics, use of magnesium sulfate, use of parenteral antibiotics, manual removal of placenta, removal of retained products, assisted vaginal delivery, basic neonatal resuscitation, surgery (cesarean section), and blood transfusion. The first seven signal functions are referred to as Basic emergency obstetric and newborn care (BEmONC), which the BEmONC health facilities provide. The Comprehensive emergency obstetric and newborn care (CEmONC) comprises the seven signal functions in BEmONC and two additional signal functions, which are surgery (cesarean section) and blood transfusion, provided by the CEmONC health facilities (Geleto et al., 2018; Okonofua et al., 2019). These signal functions are implemented by skilled birth attendants in healthcare facilities as a timely intervention for obstetric complications. World Health Organization (WHO) recommends oxytocin as the first drug in the treatment of postpartum haemorrhage (PPH): The dosage of oxytocin is 10 international unit (IU) bolus injection. Also, magnesium sulfate is the recommended anticonvulsant drug for the management of eclampsia with a loading dose of 4 grams (g) intravenous and 5 g intramuscular in each buttock followed by a maintenance dose of 5 g intramuscular every 4 hrs in alternate buttocks. Emergency cesarean section is recommended in the management of obstructed labor, and management of prolonged labor is with oxytocin 5 IU in 500 milliliters (ml) of intravenous fluid. Positive pressure ventilation (PPV) initiated within 60 seconds of birth is recommended for fetal distress (World Health Organization et al., 2009). Further studies also affirmed that magnesium sulfate is recommended in the prevention and treatment of eclampsia (Berhan & Berhan, 2015; Souza et al., 2013).
Practice guidelines bridge the gap between evidence from research and practice to improve the outcomes of care (Barth et al., 2016; Fischer et al., 2016). The EmONC practice guidelines include the nine signal functions for comprehensive EmONC (World Health Organization et al., 2009). The guidelines can enhance quality care for the leading causes of maternal and newborn mortality and improve pregnancy outcomes. However, factors such as the availability of practice guidelines, availability of resources needed for the intervention, and healthcare providers’ competence (knowledge and skills) have been shown to determine adherence to practice guidelines and their impact on pregnancy outcomes. The study by Okonofua et al. (2017) shows that poor use of treatment protocol, lack of resources, and poor skills of the healthcare providers are causes of death in the facilities. Also, previous studies in Nigeria revealed the unavailability of EmONC practice guidelines in healthcare facilities (Komolafe et al., 2021; Okonofua et al., 2019), inadequate EmONC resources (Hussein et al., 2016; Komolafe et al., 2022), and healthcare providers’ lack of competence in newborn resuscitation (Exley et al., 2018).
Evidence across countries has shown up to 70% noncompliance to practice guidelines in the implementation of interventions in various disciplines (Barth et al., 2016). Research has shown that the variation in guideline implementation is a major barrier to quality care in hospitals (Nair et al., 2014). Also, previous studies have pointed out the association between the implementation of evidence-based intervention and quality of care (Ameh & Van Den Broek, 2015; Austin et al., 2014; Ebuehi et al., 2013). The poor quality of care in hospitals hinders women from seeking and accessing facility-based care (Bohren et al., 2017; Nesbitt et al., 2016).
Previous studies in Nigeria indicated the unavailability of EmONC practice guidelines in healthcare facilities (Komolafe et al., 2021; Okonofua et al., 2019), inadequate EmONC resources (Hussein et al., 2016; Komolafe et al., 2022), and poor quality of maternal and newborn care (Austin et al., 2014; Ebuehi et al., 2013). There is a need to know the extent to which the implementation of EmONC is according to practice guidelines in Nigeria. Moreover, measuring adherence allows the researchers to know whether a lack of success with efficacious interventions results from failure to effectively implement interventions as planned or intervention inadequacies (Grant et al., 2013; Muntinga et al., 2015). Therefore, this study assessed the adherence to practice guidelines in signal functions of EmONC in referral hospitals and the pregnancy outcome in cases of obstetric complications in referral hospitals.
Method
Study Design, Setting, and Population
A descriptive research design was used to assess adherence in the implementation of emergency obstetric and newborn care in the referral hospitals in Osun State, Nigeria. Osun State has 12 referral hospitals (two federal-funded tertiary hospitals, one state-funded tertiary hospital, and nine secondary hospitals [state hospitals] scattered in six administrative zones of the state). The state hospitals are owned and funded by the state government while most tertiary hospitals are owned and funded by the Federal government, although both are referral hospitals and provide comprehensive EmONC (Abimbola et al., 2015; Okpani & Abimbola, 2015). There were six to 12 beds in the labor and delivery room of tertiary hospitals and two to six beds in the labor and delivery room of state hospitals.
Sample Size and Technique
The purposive sampling technique was used to select the three tertiary hospitals and six out of nine state hospitals in the state, one from each of the six administrative zones. The sample size for the study was determined using the Cochran formula with a 15% prevalence of obstetric complications (Otolorin et al., 2015) and a 25% attrition rate. Thus, 264 records of cases of obstetric complications that were well documented from 1st January till 31st December 2018 in the nine referral hospitals were included in the study. The records of care and patient case files in the hospitals were paper-based.
Data Collection
Data on adherence was collected from the records of care and case files of women and newborns with obstetric complications using a data extraction form developed on the REDCap platform to ensure data quality. The admission and discharge registers for labor/delivery cases were reviewed to sort out the cases of obstetric complications and the case file numbers. The case file numbers were listed, and in the tertiary hospitals, a cover letter signed by the head of the department of health records was attached for access to extract relevant data from the case files. The available case files in the labor ward or maternity unit of the hospitals were reviewed on the ward or unit, while those available in the department of health records were reviewed there without taking any case files out of the ward, unit, or health records department. Other sources of information, like the nurses’ report book, were reviewed to complement data collection on adherence in the implementation of the EmONC signal function. There were only five cases of peripartum sepsis; one in state hospitals and four in tertiary hospitals, hence peripartum sepsis was not captured in this article for objectivity. According to the fidelity framework (Carroll et al., 2007), adherence was assessed based on the contents, dosage, frequency, and duration of signal function for obstetric complications.
Statistical Analysis
Data collected on adherence were coded and entered into Stata version 14. A score of 1 was allotted to “yes” when the content of the signal function was performed and 0 to “no” when it was not done. A score of 1 was allotted to “yes” when the correct dose was given, 0 to “no” when the dose was not correct, 1 to “yes” when the frequency was correct, and 0 to “no” when the frequency was not correct and 1 to “yes” when the duration was correct and 0 to “no” when the duration was not correct. The correct scores for the EmONC signal function for each obstetric complication were expressed as a composite score and brought to 100%. The extent of adherence in EmONC signal function was measured in percentage (%). Adherence scores below 70% were regarded as low adherence, while scores ranging from 70% to 100% were regarded as high adherence. The 70% threshold was based on the evidence of 70% noncompliance to practice guidelines in various disciplines, across countries (Barth et al., 2016). Data analysis was done using Stata version 14. Both descriptive statistics, such as frequency and percentage, and inferential statistics, such as chi-square, were done with the significance level set as p < .05.
The Strengthening the Report of Observational Studies in Epidemiology checklist for cross-sectional studies was used (Network Group Equator, 2021).
Results
Table 1 shows the four types of obstetric complications: hemorrhage; preeclampsia/eclampsia; prolonged/obstructed labor, and fetal distress in referral hospitals. The table shows that the highest percentage of obstetric complications in this study was prolonged/obstructed labor (36.0%).
Types of Obstetric Complications by Referral Hospitals.

Table 2 shows the adherence to practice guidelines in the EmONC signal functions. There was correct use of oxytocin in the treatment of postpartum hemorrhage (83.8%) but incorrect dose, rate, and frequency (100%) in the referral hospitals. The use of antibiotics was recorded in all cases (100%) of retained placenta and retained product of conception, however, the dose, rate, and frequency were correct in 80.8% of cases. Magnesium sulfate was correctly used for Eclampsia in 75.9% of cases of eclampsia but the dose, frequency, and duration were correct in about half of the cases. PPV was documented in 48.0% of cases of fetal distress and PPV within 1 minute of life was documented in 44.0% of the cases.
Adherence to Practice Guidelines in EmONC Signal Functions in Referral Hospitals.

Table 3 shows high adherence in 29.6% and 28.6% of hemorrhage care in tertiary hospitals and state hospitals, respectively. There was high adherence in 83.3% and 15.4% of fetal distress care in tertiary and state hospitals, respectively. Also, there was high adherence in 56.6% and 19.1% of prolonged/obstructed care in tertiary and state hospitals, respectively. There was also high adherence in 66.7% and 33.3% of preeclampsia/eclampsia care in tertiary and state hospitals, respectively. Table 3 also shows higher adherence to care for obstetric complications in tertiary hospitals than in state hospitals.
Levels of Adherence by Type of Complications in the Referral Hospitals.

significant p-value.
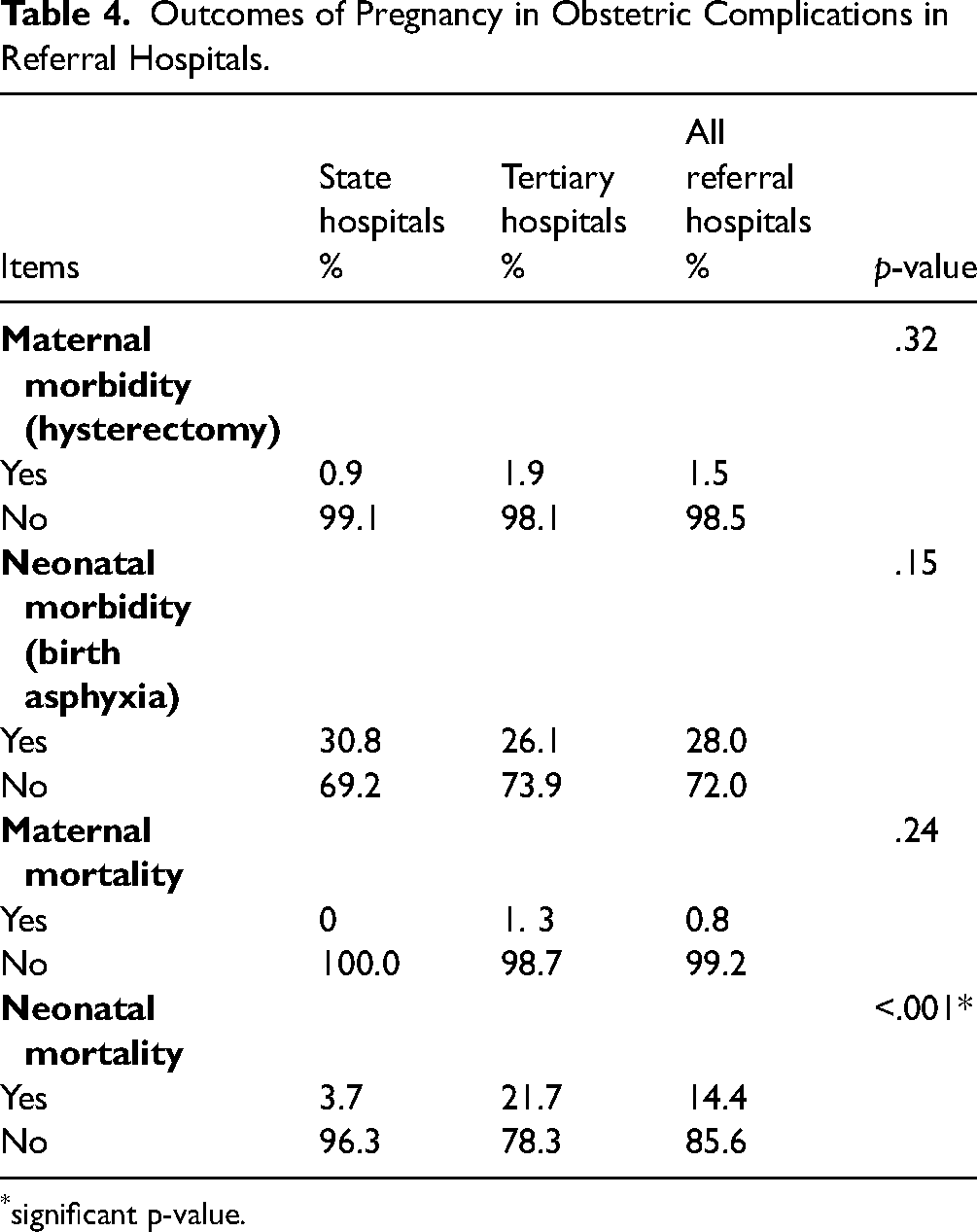
Table 4 shows that there was neonatal morbidity in 30.8% and 26.1% of obstetric complications in state hospitals and tertiary hospitals, respectively. There was also neonatal mortality in 3.7% and 21.7% of obstetric complications in state hospitals and tertiary hospitals, respectively, and this was significantly different in the referral hospitals (p ≤ .001).
Outcomes of Pregnancy in Obstetric Complications in Referral Hospitals.
significant p-value.
Figure 1 shows that 64.3% of cases of obstructed labor were referred out of state hospitals. Also, 53.9% of fetal distress and 46.7% of all cases of obstetric complications were referred out of the state hospitals.

Percentage distribution of referrals by type of obstetric complications at state hospitals.
Discussion
The study assessed adherence in the implementation of signal functions of EmONC in referral hospitals. EmONC signal functions for four major obstetric complications, hemorrhage, preeclampsia/eclampsia, prolonged/obstructed labor, and fetal distress, which were major contributors to maternal and neonatal mortality in Nigeria, were assessed. Assessment of adherence in the implementation of EmONC is necessary to identify gaps and potential solutions to ensure the intervention is implemented as intended by protocols to optimally realize the benefits of averting maternal and newborn deaths from obstetric complications.
Adherence to Practice Guidelines in Care of Hemorrhage
The results of this study established low adherence to EmONC practice guidelines in EmONC signal functions for hemorrhage care in the referral hospitals. As reported by Izugbara et al. (2017), hemorrhage is the leading cause of direct maternal mortality in Nigeria. A sizeable number of women in Nigeria die, and many more experience serious and life-threatening morbidities due to bleeding during the perinatal period. Thus, efforts to reduce maternal morbidity and mortality in Nigeria must target the implementation of EmONC for the management of various causes of antepartum and postpartum hemorrhage.
Adherence to Practice Guidelines in Care of Prolonged/Obstructed Labor
Findings from this study show that prolonged/obstructed labor is the most common obstetric complication in referral centers. Adherence to practice guidelines was low in state hospitals. Although there is a dearth of studies on the adherence of healthcare providers in the implementation of the EmONC signal functions for prolonged and obstructed labor as the basis of discussion of results from this study, the use of partograph in hospitals, as reported by a recent study in Nigeria (Ojong et al., 2021) might have helped in the prompt diagnosis of prolonged and obstructed labor. In tertiary hospitals, Adherence to implementing the EmONC signal function for prolonged obstructed labor was high. This may be related to the availability of obstetrics specialists and resident doctors capable of carrying out cesarean sections in tertiary hospitals.
Adherence to Practice Guidelines in Care of Fetal Distress
Though PPV was used in state hospitals, the use was not initiated within the first 60 seconds of life. As pointed out by the study of Exley et al. (2018), many healthcare providers lack competence in newborn resuscitation. The lack of competence may be the basis for nonadherence to the practice guidelines for newborn resuscitation and a contributory factor to the stagnancy in neonatal mortality rate in Nigeria. There is still much to be done to reduce the neonatal mortality rate with regard to newborn resuscitation to avert preventable deaths from fetal distress and birth asphyxia.
Adherence to Practice Guidelines in Care of Preeclampsia/Eclampsia
Adherence to the implementation of preeclampsia/eclampsia guidelines was high in tertiary hospitals and low in state hospitals. Magnesium sulfate is the recommended anticonvulsant drug for preventing and treating eclampsia and severe preeclampsia (Berhan & Berhan, 2015; Souza et al., 2013). Anecdotal observation during data collection revealed that the protocol for magnesium sulfate use for the management of preeclampsia/eclampsia was posted in labor wards of the teaching hospitals. Availability of the protocol might be a facilitating factor in the adherence to the signal function of this obstetric complication. However, a systematic review of the provision of emergency obstetric care in Nigeria revealed that the unavailability of magnesium sulfate contributes to maternal mortality (Hussein et al., 2016).
Adherence to Practice Guidelines in State and Tertiary Hospitals
Adherence to practice guidelines was worse in the state hospitals. This might be related to the lack of EmONC guidelines in many state hospitals. Previous studies affirmed the lack of EmONC guidelines in many hospitals (Komolafe et al., 2021; Okonofua et al., 2019). This finding implies that the quality of care is compromised, and the benefits of averting maternal and newborn mortality from obstetric complications promised by implementing EmONC are jeopardized. Also, reports from previous studies have shown that variation in the implementation of practice guidelines is a barrier to the provision of quality, and lack of resources as well as healthcare providers’ poor skills increase mortality in hospitals (Nair et al., 2014; Okonofua et al., 2017).
The adherence to practice guidelines in the implementation of EmONC signal functions for obstetric complications differs at the state hospitals and tertiary hospitals. State hospitals, though expected to have the surgical capacity and blood transfusion facilities to implement comprehensive EmONC hospitals, are lagging behind and thus refer patients to tertiary hospitals. The referral of women and newborns with obstetric complications from state hospitals to tertiary hospitals is a sheer betrayal of the women's trust in facility-based care. The weak context in EmONC implementation in state hospitals, which was linked to inadequate resources and funding may be responsible for the referrals (Komolafe et al., 2022). To a large extent, the survival of women and newborns with obstetric complications may depend on facility-based delivery and the type of healthcare facility, state, or tertiary. Although maternal morbidity, mortality, and newborn mortality were low in State hospitals compared with tertiary hospitals, it may be because many of the cases of obstetric complications were referred out to the tertiary hospitals, thereby transferring morbidity and mortality that could have happened in the state hospitals to the tertiary hospitals. Research shows that a woman who delivers in a tertiary hospital is less likely to die than when she delivers in a state hospital (Ntoimo et al., 2018). While delivering a baby in a state hospital may be a misadventure, resulting in life-threatening disabilities or death of the woman and newborn, peradventure obstetric complications set in, the same case may be a near-miss if it happens in tertiary hospitals. Although it may be impossible for all births to occur in the few tertiary hospitals in Nigeria, efforts to reduce maternal and newborn morbidity and mortality should focus on quality improvement to upgrade state hospitals to safe hospitals for women to deliver their babies. Effective funding of the state hospitals to ensure adequate resources in terms of material and human is necessary for quality healthcare and safe delivery in state hospitals.
The findings on adherence in the implementation of EmONC reflect the quality of care available for women and newborns with obstetric complications. Evidence has shown that poor quality of care in maternal and newborn care is associated with poor implementation of evidence-based intervention (Ameh & Van Den Broek, 2015). The poor quality of maternal and newborn care reported by previous studies in Nigeria (Austin et al., 2014; Ebuehi et al., 2013) can be related to poor implementation of EmONC, which hinders the provision of adequate and appropriate care for women with obstetric complications in the hospitals. As pointed out by previous studies, the poor quality of care in hospitals may hinder women with obstetric complications from seeking and accessing facility-based care (Bohren et al., 2017; Nesbitt et al., 2016). The experience of referral from state hospitals for cases that should have been handled in state hospitals may negatively impact the willingness of women to seek facility-based care for subsequent pregnancies and result in severe morbidity or mortality for them and their newborn babies.
The findings on adherence to EmONC practice guidelines underscore the importance of the availability and use of practice guidelines in referral hospitals. Previous studies pointed out the major factors determining adherence to practice guidelines (Exley et al., 2018; Hussein et al., 2016; Komolafe et al., 2021, 2022; Okonofua et al., 2019). Hence, EmONC training for healthcare providers, the use of EmONC practice guidelines as well as availability of EmONC resources in healthcare facilities might ensure adherence to EmONC practice guidelines in the implementation of EmONC signal functions in the referral hospitals.
Strengths and Limitations of the Study
The study was conducted in both state and tertiary hospitals, which are referral centers, allowing tracking and comparing adherence in the referral hospitals. Also, the inclusion of all the tertiary hospitals in the state and one state hospital from each of the six administrative zones in the state contributes to making the findings generalizable to Osun State. To an appreciable extent, this study has provided empirical data on the cause of high maternal mortality in Nigeria and provided actionable information that policymakers can act upon to improve maternal and newborn health. The study also provided a basis for future research on quality improvement in EmONC for obstetric complications in healthcare facilities.
The retrospective nature of the study, which involved the extraction of data from patients’ records of care, could be a limitation considering the challenge with the quality of perinatal data capture. However, the researcher mitigated this challenge by using well-documented records of care.
Implication for Practice
The low adherence in this study has implications for maternal and child health nursing. The failure to follow practice guidelines to implement EmONC as intended may negatively impact pregnancy outcomes, and medical litigations may ensue from maternal and newborn mortality and morbidity. Also, low adherence to practice guidelines may make correlating data on the effectiveness of EmONC across regions and nations impossible, and quality improvement efforts may be jeopardized.
There is a need for qualitative research to explore the reasons for low adherence to practice guidelines to inform evidence-based interventions for improving adherence to practice guidelines in the implementation of EmONC in Nigeria.
Conclusion
The findings of the study showed low adherence to EmONC guidelines in state and tertiary hospitals in the study setting. Although adherence to EmONC guidelines was higher in tertiary hospitals, the perinatal outcomes such as maternal mortality and morbidity, and newborn mortality were lower in state hospitals compared with tertiary hospitals. This may be because of several unnecessary referrals of obstetric complications, which should have been treated in state hospitals to tertiary hospitals, thus transferring maternal and newborn morbidities and mortalities to tertiary hospitals. Again, the numerous unnecessary referral of cases in state hospitals shows that EmONC has not been successfully implemented in state hospitals. The study pointed to the need to intensify efforts in adherence to EmONC guidelines and the implementation of EmONC to ensure women and newborns with obstetric complications get adequate and appropriate care when they arrive at the state and tertiary hospitals.
Footnotes
Acknowledgments
We appreciate women and newborns, both dead and alive, whose records of care contribute to this research.
Authors’ Contributions
AOK conceptualized the study, collected, analyzed, and interpreted data; AEO and OOI contributed to the conceptualization, interpretation of data, and writing of the manuscript, and AOO, AOI, and OBO contributed to the first draft of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Considerations
Ethical approval for the study was obtained from the Health Research Ethics Committee (HREC) of the Institute of Public Health, Obafemi Awolowo University, Ile-Ife (IPHOAU/12/1098) and Research Ethics Committees of the tertiary hospitals (LTH/EC/2019/06/419 and ERC/2018/12/11). Permission to collect data was also obtained from the Ministry of Health, Osun State. Ethical principles of confidentiality and anonymity were maintained as identifiers were removed from the data obtained.
Funding
This research was supported by the Consortium for Advanced Research Training in Africa (CARTA). CARTA is jointly led by the African Population and Health Research Center and the University of the Witwatersrand and funded by the Carnegie Corporation of New York (Grant No. G-19-57145), Sida (Grant No. 54100113), Uppsala Monitoring Center, Norwegian Agency for Development Cooperation (Norad), and by the Wellcome Trust (reference no. 107768/Z/15/Z) and the U.K. Foreign, Commonwealth and Development Office, with support from the Developing Excellence in Leadership, Training and Science in Africa (DELTAS Africa) program. The statements made and views expressed are solely the responsibility of the Fellow.