
Abstract
Introduction
Nurses who are at the forefront of the fight against Covid-19 have faced problems such as anxiety and stress due to the high contagiousness of this disease and the challenges of providing services to infected patients. Death anxiety and the resulting fear following the Covid-19 pandemic can affect caring behaviors and the quality of nursing care services.
Objective
The present study was conducted with the aim of determining the association between caring behaviors and death anxiety among Iranian nurses working in COVID-19 wards.
Methods
This cross-sectional study was conducted in 2021 in Tehran. The participants consisted of 233 nurses who were purposively selected from university hospitals in Iran. Data collection tools included Demographic Information Form, Death Anxiety Scale, and Caring Dimension Inventory (CDI-25). Data analysis was done using SPSS (version 16).
Results
Most of the participants were female (79.4%), had less than 5 years of work experience (50.6%), and had bachelor's degree (88.8%). Based on the results, the level of death anxiety among nurses was moderate (7.05 ± 3.85) and their caring behavior was at optimal level (103.03 ± 13.15). Among the subscales of caring behavior, physical-technical behaviors with mean of 46.43 ± 6.20 got the highest score, and unnecessary behaviors with mean of 4.39 ± 0.73 got the lowest score compared to other subscales. Based on data analysis findings, caring behavior and its dimensions had no significant correlation with nurses’ death anxiety (p = 0.111).
Conclusions
Our results showed that despite having a moderate level of anxiety, nurses try to provide good care behaviors to patients with covid-19. However, reducing nurses’ anxiety can improve caring behaviors.
Introduction
Coronavirus disease (COVID-19), as an infectious disease caused by severe acute respiratory syndrome (SARS-CoV-2), was declared as a pandemic by the World Health Organization (Yiğit & Acikgöz, 2021). It quickly affected various fields, including healthcare and economic systems (Haleem et al., 2020; Onyeaka et al., 2021). According to reports, more than 540 million people in the world have been infected with this disease and more than 6 million people have lost their lives because of the COVID-19 pandemic. In Iran, the number of infected people is more than 7 million and the number of deaths attributable to COVID-19 is estimated at around141 thousand people (WHO, 2022).
Nurses as the largest group of healthcare providers are at the top of the pyramid of the health system and making up the backbone of healthcare system. They are on the front line of fighting against Covid-19 diseases and responsible for providing holistic care to patients. In crises and epidemics such as COVID-19, the roles and responsibilities of nurses are doubled, preventing nurses from performing their duties optimally (Al Thobaity & Alshammari, 2020) and causing significant and destructive effects on their performance (Chan et al., 2021). This high stress and heavy workload leads to gaps and deficiencies in caring for patients (Bernacki et al., 2021; Masterson-Algar et al., 2021). In such a situation, caring behavior can be negatively affected by insufficient information about the disease, long and continuous care of affected patients, high workload, and constant exposure to death (Alagamy et al., 2022). Although the unfavorable caring behaviors of nurses (focusing on routine and technical aspects more than the social-emotional aspects) can be a contributing factor to client's unmet needs (Baljani et al., 2012), it was found that nurses’ caring behavior in the context of COVID-19 had been at a favorable level (Hajibabaee et al., 2022). Nevertheless, the nurse's attitude about death and dying process and the resulted death anxiety can adversely affect the quality of care provided by the nurse (Peters et al., 2013). In COVID-19 epidemic, where the importance of nurses’ caring behavior has doubled, it is necessary to discover factors affecting nurses’ caring behavior. Therefore, the present study was conducted with the aim of determining the association between caring behaviors and death anxiety among Iranian nurses working in COVID-19 wards.
Review of Literature
Providing care is a vital component of nursing services, and the responsibility of each nurse is to develop and improve nursing services by providing desirable care behaviors (Vujanic et al., 2020). Caring behaviors are all actions performed in relation to the client's well-being, such as understanding, consoling, listening, being honest, and unconditional acceptance of patient (Salimi & Azimpour, 2013). The importance of caring behaviors and nurse–patient interactions has been proven for everyone. If the implementation of interactive nurse–patient models developed based on the desired caring behaviors in the healthcare system, can improve nurses’ working environment, and the nurse–patient satisfaction level. As well as it can lead to a higher level of patient safety and enhance the quality of provided cares. However, not paying attention to the development and improvement caring relationships can have destructive effects on clients’ experiences (Modic et al., 2014).
Death anxiety is a conscious or unconscious psychological state that is associated with feelings of insecurity, anxiety, or fear related to death or near-death experiences or it occurs when people feel the threat of death/dying (Zhang et al., 2019). Death anxiety and the resulted fear prevent the effective communication between nurses and patients and their families, hence negatively affecting the caring attitude. In addition, the impact of destructive factors such as reduced physical performance, stress and life's dissatisfaction, has led to the emergence of anxiety in nurses, which can be effective in managing the death process of patients in the workplace and have an adverse effect on the quality of nursing services (Karabag Aydin & Fidan, 2022; Sharifnia et al., 2016).
During COVID-19 pandemic, one of the most important concerns experienced by the nurses is death anxiety. In this epidemic, nurses showed a higher level of death anxiety than other healthcare workers (Karabag Aydin & Fidan, 2022). In this regard, Belash et al. (2021) reported that about 69% of nurses had severe death anxiety (Belash et al., 2021). Peters et al. (2013) concluded that death anxiety in nurses negatively affected their caring behavior and attitude towards care (Peters et al., 2013). Therefore, it seems that when nurses are aware of their thoughts and feelings about death, they can provide a higher quality care to patients and their families (Pehlivan et al., 2020). Nurses are more exposed to the tensions caused by COVID-19 pandemic crisis than any other group in the society, so more attention should be given to their mental health than other sections of the society, because this issue can directly affect the way of care, caring behaviors and quality of care provided by them.
Methods
Research Question
Are caring behaviors and death anxiety associated with each other among nurses working in the COVID-19 wards?
Design
This descriptive cross-sectional correlational study was conducted in 2021 in Tehran, Iran. After obtaining code of ethic and in coordination with the officials of Hospitals, the study was initiated. In order to access to the list of nurses working in the Covid-19 department, the researcher went to the relevant wards and during a short meeting with nurses, the objectives of the study were explained to all participants. They were assured that their participation in the study was voluntary and their information would be kept confidential and would be used for research purposes only. Due to COVID-19 pandemic and inhibiting face-to-face data collection, a link to the questionnaire was provided to the participants through WhatsApp Messenger. All of the participants voluntarily completed the consent form before entering the study. It should be noted that the questionnaires completion guide and the researcher's contact number to answer the possible questions of the participants were available at the beginning of the questionnaires.
Participants
The study population was composed of all the nurses working in the COVID-19 wards in Firozabadi, Firozgar, Hazrat Rasool, and Lulagar hospitals affiliated to Iran University of Medical Sciences. The inclusion criteria were working at COVID-19 ward for at least one month and having at least a bachelor's degree in nursing.
Sample
The continuous sampling method was performed. Considering 95% confidence interval and 80% test power, assuming 0.2 correlation coefficient between caring behavior and death anxiety to obtain statistically significant difference between variables, according to a study done by Cui et al. (2020), taking into account 10% participants dropout, and using the following formula, the sample size was calculated as 233 people.


Instruments
Data collection tools included demographic information form, Death Anxiety Scale, and Caregiving Dimension Inventory (CDI-25).
Demographic Information Form
This form included the variables of age, gender, marital status, work experience, and education level.
Templer Death Anxiety Scale
This questionnaire was designed by Templer in 1969 as a self-report scale consisting of fifteen yes-no items. One score is allocated for each positive (“yes”) answer and zero score for each negative (“No”) answer in items of 1, 4, 8, 9, 10, 11, 12, 13, and 14. Reversely, zero score is allocated for each positive (“yes”) answer and one score for each negative (“No”) answers in items of 2, 3, 5, 6, 7, and 15. Total score ranges from 0 to 15. It has a cut off score = 6–7, so that a higher score means more death anxiety. Templer reported that the validity of the total scale was 0.83 (Templer, 1970). In a study by Sharifnia et al. (2016), it was reported that the validity of 11 items of this scale was 0.87 and that of the next 4 items was 0.75. Using test–retest method, they also revealed that the validity of the whole scale was between 0.89 and 0.91 (Sharifnia et al., 2016).
Caregiving Dimension Inventory (CDI-25)
This questionnaire was developed by Watson and Lea in 1977. It consists of 25 items whose purpose is to evaluate nurses’ caring behaviors from different dimensions, namely physical-technical behaviors (items of 1, 2, 5, 8, 9, 12, 14, 15, 18, 20, 25), psycho-social behaviors (items of 4,7,10,11,13,17,19,21,23, 24), professional behavior (item 6), and unnecessary behaviors (item 22). The items are scored on a 5-point Likert scale (completely agree (5), agree (4), have no opinion (3), disagree (2), and completely disagree (1)). Items 3 and 16 have reversed scoring. The range of total scores is between 25 and 125, and higher scores indicate more desirable caring behavior. The reliability of CDI in Watson et al.'s study was confirmed using Cronbach's alpha (α=0.97) (Watson & Lea, 1997). Salimi et al. also confirmed the reliability of CDI using the factor analysis method (0.86) (Salimi et al., 2014).
In the current study, the content validity of the questionnaires was confirmed by three faculty members of Nursing and Midwifery School of Iran University of Medical Sciences. Cronbach's alpha coefficient was used to measure the internal consistency of the questionnaire. The questionnaires were completed by 25 nurses working in the COVID-19 wards who were not part of the research samples but had similar characteristics. With running statistical tests, the internal consistencies of the questionnaires have calculated, and the results provided in the Table 1.
The Internal Consistency of the Questionnaires.

Ethical Consideration
In order to comply with research ethics and not to interfere with the patient care plan and considering the difficulty of high workload and heavy shifts during COVID-19 pandemic, no specific time limit was considered for completing the questionnaires.
Statistical Analysis
Data analysis was done using SPSS (version 16). Frequency distribution tables were used for qualitative variables and numerical measures of minimum, maximum, mean, and standard deviation were used for quantitative variables, such as death anxiety. Independent t-tests and one-way analysis of variance were run to investigate any correlations between death anxiety and demographic variables. Pearson's test was also used to discover the possible correlation between caring behavior and death anxiety. A p-value less than 0.05 were considered to be statistically significant.
Results
Sample Characteristics
In terms of demographic characteristics and according to Table 2, most of the participants were female (79.4%). About 43.8% of them were less than 30 years old and more than half of them (50.6%) had less than 5 years of work experience.
Frequency Distribution of Demographic Information among Nurses Working in COVID-19 Wards.

Research Question Results
According to Table 3, the mean score of death anxiety was 7.05 ± 3.85; given the score range (0 to 15) and the cutoff point, it was at the moderate level.
Numerical Indicators of Death Anxiety among Nurses Working in COVID-19 Wards.

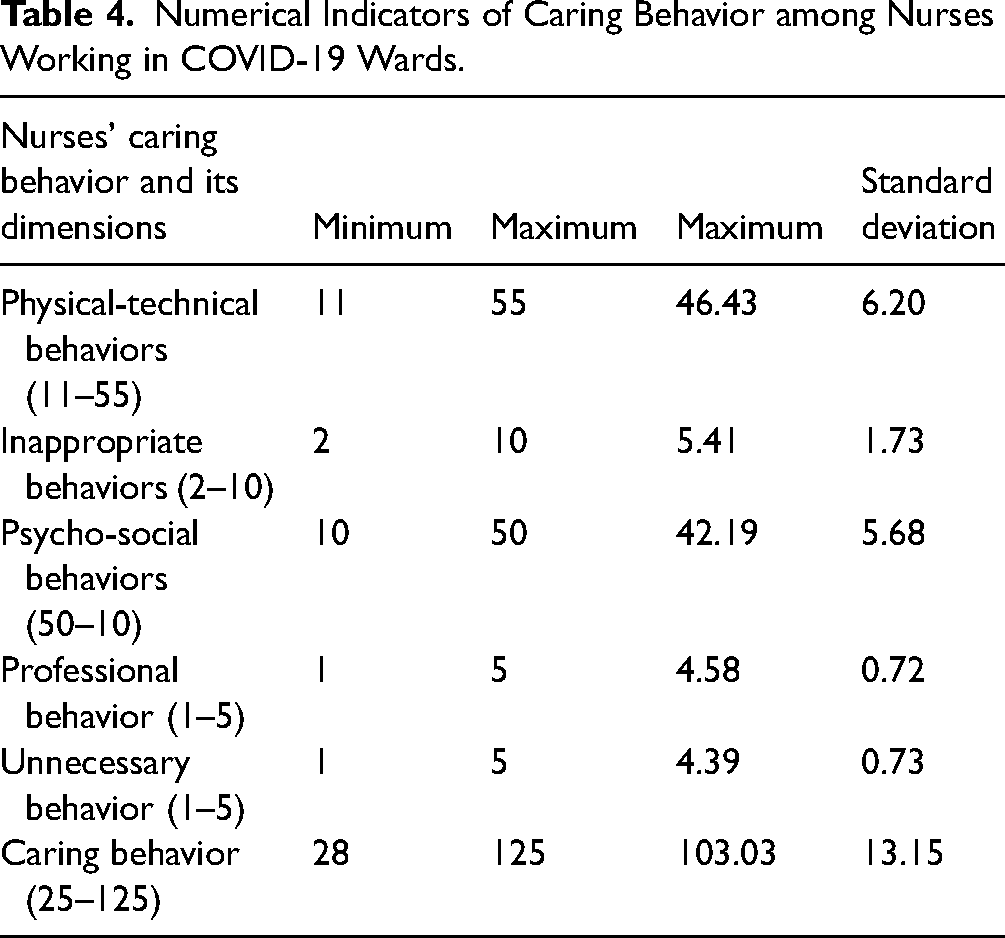
Table 4 shows the mean score of caring behavior (103.03 ± 13.15), which was higher than the median value of the scale. Among the subscales of caring behavior, physical-technical behaviors with mean of 46.43 ± 6.20 got the highest score and unnecessary behaviors with mean of 4.39 ± 0.73 got the lowest score compared to other subscales.
Numerical Indicators of Caring Behavior among Nurses Working in COVID-19 Wards.
As it is clear from Table 5, there was no significant correlation between caring behavior and death anxiety (p = 0.111, r = 0.105). No significant correlation was found between any dimensions of caring behavior and death anxiety, as well.
Correlation Between Caring Behavior and Death Anxiety among Nurses Working in COVID-19 Ward.

The results of the independent t-test showed that there was a statistically significant association between death anxiety and participants’ gender (p < 0.05). In addition, two-by-two comparison of Tukey showed that the mean score of death anxiety was higher in female participants than in male ones. The results of our study showed that the numerical indicators of death anxiety among nurses working in the COVID-19 ward can be affected by gender and this is felt more in women than in men (p = 0.044). However, numerical indicators of death anxiety among nurses working in the Covid-19 ward had no significant relationship with the age of the participants (p = 0.416). Also, no statistically significant relationship was found between other demographic characteristics and death anxiety (p < 0.05) (Table 6). Based on Table 7, there was no statistically significant association between demographic characteristics and participants’ caring behavior (p < 0.05).
Numerical Indicators of Death Anxiety among Nurses Working in COVID-19 Ward with Respect to Demographic Information - 2020.

Numerical Indicators of Caring Behaviors among Nurses Working in COVID-19 Ward with Respect to Demographic Information - 2020.

Discussion
The purpose of this study was to examine the connection between Death Anxiety and Caring Behavior among Iranian Nurses who work in Covid-19 Wards of hospitals affiliated with the Iran University of Medical Sciences. The high occurrence of COVID-19 has created a serious situation in society, and media coverage of the illness's mortality and death rates leads to psychological responses, particularly fear and anxiety about dying. Thoughts of one's own death or the death of others cause death anxiety, which has been shown to have negative impacts in various areas of people's lives. These impacts include pessimism, despair, a poor understanding of social support, and an insufficient perception of life (Çakar, 2020). The person is unable to process properly and experiences severe anxiety due to these stressful conditions. In general, it is necessary to take measures to improve the level of caring behavior and reduce as much as possible the level of death anxiety among nurses taking care of patients with COVID-19 (or any other contagious disease). These measures involve the regular assessment of nurses, especially psychological assessment, provision of targeted training in order to develop and promote the nurses’ resilience and support nurses psychologically when facing with patients’ death process and the resulted anxiety, and creating developing plans to improve nurses’ skills such as controlling emotions or strengthening motivation to do their best while caring for these patients.
Nurses play a crucial role in the treatment team and are on the frontlines in the battle against the COVID-19 pandemic. They experience long-term and constant stress, which can pose a threat to their health, particularly for those working in COVID-19-related wards such as intensive care units. This stress can also lead to the development of psychological disorders (Liu et al., 2020). The findings of this study showed the death anxiety of nurses was at an average level, which was in line with the studies done by Tavakkoli et al. (2021) and Karabağ Aydın and Fidan (2022); However, in contrast to our findings, Yiğit and Acikgöz (2021) and Farokhnezhad Afshar et al. (2021) reported high level of death anxiety among the studied samples (Farokhnezhad Afshar et al., 2021; Yiğit & Acikgöz, 2021). This high level of death anxiety reported by these studies can be attributed to long working hours or constant exposure to anxiety, which imposing negative consequences on all aspects of individuals’ health.
Based on our findings, there was no statistically significant relationship between death anxiety and any of the participants’ demographic variables except for gender (more prevalent in females than in males). Align with our study, Farokhnezhad Afshar et al. (2021) stated that there was no statistically significant relationship between death anxiety and demographic variables except for the gender, reporting that it was more common in females (Farokhnezhad Afshar et al., 2021). Similarly, Tavakkoli et al. (2021) found no significant relationship between general/demographic variables and death anxiety (Tavakkoli et al., 2021). In their study conducted on the general population in Turkey, Kavakli et al. (2020) also concluded that female participants had a higher level of perceived risk of getting infected with COVID-19 and death anxiety compared to male participants (Kavakli et al., 2020). The levels of emotional intelligence can vary among professionals in different fields, particularly among healthcare professionals. In addition, some components of emotional intelligence are individual-centered (Alonazi, 2020). To effectively manage and work with one's emotions, it is possible to teach and practice emotional intelligence. Goleman argues that it should be a major focus in professional development initiatives. He believes that having expertise specific to a job is not enough to improve performance. Instead, individuals need to have higher levels of emotional intelligence in order to effectively utilize new skills. Improving emotional intelligence can lead to balanced improvements in both professional success and social performance (Coetzee & Harry, 2014; Goleman et al., 2013). The absence of a significant relationship between death anxiety and demographic variables of the participants except for gender could be due to the different emotional intelligence of the participants. However, further studies are necessary to understand these issues.
In return, Belash et al. (2021) reported a significant relationship between death anxiety and demographic variables (i.e., age, weekly working hours, having children, end-of-life care, participation in resuscitation, observing the death of patients, and satisfaction with personal protective equipment) (p < 0.05). They also stated that this relationship was independent of the participants’ gender (Belash et al., 2021). Although Yiğit and Acikgöz (2021) found a significant difference between death anxiety level and demographic variables (i.e., gender, marital status, childbearing status, family structure, income level, and smoking and alcohol consumption) (p < 0.05), they detected no significant relationship between nurses’ age, suffering from a chronic disease, and being diagnosed with mental illness and different levels of death anxiety and anxiety (p > 0.05). In addition, they yielded that the level of anxiety might be different depending on individual and demographic characteristics, personal habits, and the individual's health status (Yiğit & Acikgöz, 2021). The relationship between gender, age, and death anxiety can vary among individuals in the general population and nurses. It's important to note that these relationships are complex and influenced by a wide range of factors, including cultural, social, and individual differences. It's important to recognize that individual differences play a significant role in these relationships. Not everyone in a specific gender or age group will experience death anxiety in the same way. Additionally, cultural and personal beliefs, prior experiences with death, and the specific caregiving context can all influence the relationship between gender, age, and death anxiety. It seems that evaluating the relationship between gender/age and death anxiety in nurses working in the COVID-19 ward with the general population or other care could highlight important issues. As a result, it seems necessary to evaluate the relationship between emotional intelligence and death anxiety in different groups (nurses or general population).
The mean score of caring behavior of nurses revealed a high and optimal level of caring behavior. Similarly, Kusuma et al. (2021) and Hajibabaee et al. (2022) reported that nurses’ caring behavior was at a good level (Hajibabaee et al., 2022; Kusuma et al., 2021). In addition, Asadi et al. (2020) demonstrated that the level of caring behavior was optimal among personnel working in COVID-19 wards (Asadi et al., 2020). In contrast, Zabolypour et al. (2016) revealed a moderate level of caring behavior (Zabolypour et al., 2016). The reason for this disparity can be due to the difference between the research community of the study in question investigated patients and not nurses, because the views of nurses and patients on caring behaviors and how to perform them leading to the improvement of the quality of care and increasing patient and nurse satisfaction are different.
According to our findings, there was no significant relationship between demographic variables and caring behavior. Align with our study, Asadi et al. (2020) and Kartini & Putri (2019) reported that nurses’ personal characteristics (i.e., age, gender, and education level) did not affect their caring behaviors (Asadi et al., 2020; Kartini & Putri, 2019), while emotional intelligence had a significant effect on their caring behaviors (Kartini & Putri, 2019).
The results showed no significant correlation between caring behavior and its dimensions and death anxiety among nurses. Although no study investigating the same variables was found, our findings were in agreement with the results of the study done by Asadi et al. (2020) on the association between COVID-19 anxiety and nurses’ caring behaviors. Based on the aforementioned study, there was no significant relationship between these two variables (Asadi et al., 2020). This finding can be related to the ability of nurses to adapt and choose appropriate coping strategies, which ultimately determines their caring behavior (Kusuma et al., 2021).
Strength and Limitations
One of the limitations of this study was performing the study in hospitals affiliated to one university (Iran University of Medical Sciences) and involving only nurses, which preclude the generalization of the results to the larger populations. The other limitation was related to the virtual data collection, which limited the researcher's communication with the participants and might have influenced the understanding of the content and the completion of the questionnaires.
Implications for Practice
We demonstrated that the caring behaviors and death anxiety are not related to each other. In fact, the moderate level of death anxiety could not effect on caring behaviors of nurses. Nurses who worked in COVID-19 wards, despite of encountering with high level of stress of providing care for patients, showed a high level of caring behaviors. These results showed that they had received good training for probable stressful situation. Therefore, it is highly recommended that these policies continue to promote awareness and skills of nurses. Future studies should have more emphasis on promoting and maintenance of mental health of nurses as key members of medical team. Implementing comprehensive interventions for early diagnosis and management of depression, anxiety, and stress symptoms among nurses can prevent severe consequences, enhance the quality of nursing care, and improve patient satisfaction. Healthcare authorities and policymakers are advised to utilize effective interventions to identify nurses who are at risk for mental health issues and offer them psychiatric counseling services and stress management education to enhance their mental well-being. To facilitate the effective results of the relationship between caring behavior and death anxiety in healthcare organizations, it may be considered in the future to investigate between caring behavior and death anxiety during crisis epidemics, from other healthcare providers and patients at different stages.
Conclusions
COVID-19 epidemic has affected the health of people both physically and psychologically, especially the personnel who are working on the frontlines of the fight against COVID-19. Caring behaviors, if properly supported (especially psychologically), can reduce the impact of negative factors on the care process, meet the expectations of patients, and increase the quality of the provided care.
This study showed that caring behavior had no significant correlation with the death anxiety in nurses. In other words, we found that nurses had a favorable caring behavior despite having a moderate level of death anxiety. These findings revealed that nurses tried to provide good caring behaviors, as the most basic nursing role, while caring for patients with COVID-19 despite having a moderate level of anxiety. More studies are necessary to investigate the difference in understanding of emotional intelligence of the participants in future studies.
Footnotes
Acknowledgement
The authors would like to give their thanks to the Vice Chancellor for Research of the Iran University of Medical Sciences, and the officials of all those hospitals for providing the facilities and their cooperation in accessing the research samples. As well as the authors express their gratitude to all those nurses who attended to this study to achieve its goals.
Authors’ Contributions
N.S. conceived the paper and planned the program to implementing. Z.A. and Z.S.M.K. implemented and supervised the program, and R.B. wrote the main manuscript. All authors interpreted the data, reviewed successive versions of the paper and approved the final version to be published.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement
All methods followed the ethical principles for medical research and the study was approved by Ethics Committee of Iran University of Medical Sciences (approval No. IR.IUMS.REC.1399.1118).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received a financial support for the research, and authorship of this article from Iran University of Medical Science (design, collection, analysis, and interpretation of the data). (Grant number IR.IUMS.REC.1399.1118).