
Abstract
Introduction
The COVID-19 pandemic has resulted in an unanticipated shift in nursing practice to meet the sudden increase in demand for pandemic-related care, leaving nurses unable to provide acceptable services to patients in the way they were taught and expected to do. It put the nurses under more stress and most of them were dissatisfied with their work due to excessive burnout.
Objectives
The study determined the level of stress and burnout among front-line nurses working at the Ministry of Health Hospitals in Najran, Saudi Arabia during the COVID-19 pandemic.
Methods
A total of 1594 nurses were chosen using a convenience sampling approach. Google Forms were used to collect data from the nurses. COVID-19 stressors questionnaire and an abbreviated Maslach Burnout Inventory were used to assess stress and burnout among nurses.
Results
Our study reported that the majority of nurses experienced extreme levels of stress as their colleagues became ill; that they would spread COVID-19 infection to their family and friends; upsetting to see COVID-19 patients dying in front of them; not knowing when the COVID-19 pandemic will be under control; and emotional exhaustion and physical fatigue. A vast majority of nurses felt there were not adequate protective measures; there was a shortage of staff at times; were nervous and scared and thought of quitting their job; and they would quit their job if a COVID-19 outbreak recur and they would fall sick. Likewise, 41.9% of the nurses experienced a high level of burnout. A significant association was found between the area of working and the level of burnout among nurses.
Conclusion
As nurses experienced extreme levels of stress and severe burnout, it is vital to design regular programs to assist frontline nurses in maintaining their mental health.
Introduction/Background
Nurses are highly skilled and knowledgeable healthcare workers who provide holistic patient-centered care throughout the life span of an individual (Powers, 2021). Nursing has its reputation for being a demanding job by its very nature. Recently, the demand for nursing personnel has increased (Koh et al., 2015). The COVID-19 pandemic has increased the demand and visibility of nurses and emphasized that nurses are the backbone of and central to every healthcare service. Nurses are working on the frontline during this pandemic to prevent, treat, and manage conditions with care, compassion, creativity, resilience, and pronounced leadership skills (Smith et al., 2020). Unfortunately, many nurses worldwide have lost their lives during the pandemic. They have been working without sufficient protection, have been facing abuse and violence, have not been receiving decent salaries and incentives, and have been separated from their loved ones, consequently increasing their stress and burnout levels. Stress is an interactive situation between a job and the person working in that job, which leads to changes in the physiological and psychological statuses and affects job performance (Richardson & Rothstein, 2008). Burnout is a response to excessive stress at work, which is characterized by feelings of being emotionally drained and lacking emotional resources including emotional exhaustion, depersonalization, and reduced personal accomplishment (Maslach, 1998). Burnout in nurses causes serious health problems and adverse implications not only to nurses but also to patients and healthcare institutions (Kabunga & Okalo, 2021). This clearly shows that nurses worldwide are facing the most unprecedented public health crisis (Powers, 2021).
Nurses make up the majority of healthcare professionals and are at the forefront of the COVID-19 response (Ghanbari et al., 2020), and their clinical job necessitates direct contact with patients who may be asymptomatic, putting them at risk for COVID-19 infection (Huang et al., 2020; Jackson et al., 2020). Nurses working in high-risk units, specifically emergency units, critical care units, and medical and surgical units, are at risk of COVID-19 cross-infection owing to adjacent interaction with respiratory pathogens when carrying out aerosol procedures (Ng et al., 2020). Additionally, nurses in various regions worldwide are facing constraints in medical supplies, including personal protective equipment (PPE) such as masks, gloves, and gowns, while enthusiastically embracing the difficulties posed by COVID-19 (Jackson et al., 2020). The COVID-19 pandemic has also resulted in an unanticipated shift in nursing practice to meet the sudden increase in demand for pandemic-related care (Smith, 2020), leaving nurses unable to provide acceptable services to patients in the way they have been taught and are expected to do and putting them under more stress and dissatisfaction at work. All these factors pose nurses to experiencing stress and burnout in their day-to-day lives (McGrath et al., 1989).
Review of the Literature
While managing complex care and treatment processes, nurses are often confronted with difficult situations that yield emotional exhaustion, leading to stress (Schroeder et al., 2020). Working for lengthy periods, ambiguity in duties, shifting of nurses’ units or wards, and increased workload prompt nurses to experience stress more rapidly, especially during the pandemic (Clegg, 2001; Xu et al., 2021). Workplace stress has also been linked to higher degrees of exposure to potentially traumatic experiences among nurses (Drennan & Ross, 2019). Moreover, nurses working in Corona wards, married nurses (Jose et al., 2020), and nurses who suppress their emotional expression (Nadeem et al., 2021) experience more stress during the COVID-19 pandemic. Moderate to severe levels of stress have also been reported in the majority of nurses during this period (Aly et al., 2021; Lenzo et al., 2021). The other identified causes of stress during the pandemic include illness and death of others, self-exposure to infection, lack of PPE and other supplies, workplace, opinions and politics, fear of the unknown, and feelings of inadequacy and helplessness regarding patients and their treatment (Basit & Peni, 2021).
The overall prevalence of stress during the COVID-19 pandemic ranges from 43% to 45% across different studies conducted worldwide (Al Maqbali et al., 2021; Arnetz et al., 2020). In China, 35% of healthcare personnel have been reported to experience moderate to severe posttraumatic stress symptoms 1 month after the COVID-19 pandemic (Salari et al., 2020). Posttraumatic stress is a psychiatric state caused by exposure to a traumatic event or an extreme stressor that is responded to with fear, helplessness, or horror (Mealer et al., 2009). Approximately 26% of healthcare professionals in Italy (Di Tella et al., 2020), 40% of nurses in the United Kingdom (Lai et al., 2020), and 64% of nurses in the United States (Krystal, 2020) have reported clinically significant levels of posttraumatic stress symptoms after the outbreak of COVID-19. Further, healthcare workers have experienced significant psychological distress during the first wave of the pandemic (Salmon & Morehead, 2019). Psychological distress is a state of emotional suffering characterized by symptoms of depression and anxiety, which are widely used as an indicator of mental health (Drapeau et al., 2012). Therefore, organizations must pay special attention to healthcare providers in the early detection and reduction of stress by organizing reflection sessions to identify their problems, increasing the number of nurses, and providing facilities to support them (Aly et al., 2021).
Nurses have also experienced significant degrees of burnout during the COVID-19 pandemic as they dealt with suffering, loss, and death every day (Rose et al., 2021) and as they were continuously exposed to stress and observed various negative outcomes in their patients, leading to insomnia, irritability, and incompatibility (Ruiz-Fernández et al., 2020). Further, younger nurses and nurses working longer shifts have expressed higher levels of burnout (Shirom, 2011). Factors related to the working environment, workload, shift work (Zhang et al., 2020a), and lack of PPE have contributed to burnout among clinical nurses during the pandemic (Bakhamis et al., 2019). In their systematic review and meta-analysis, Galanis et al. (2021) reported younger age, low family and colleague readiness to cope with the COVID-19 outbreak, decreased social support, working in hospitals with inadequate and insufficient materials and human resources, increased workload, lower level of specialized training regarding COVID-19, longer working time in quarantine areas, working in a high-risk environment, and increased perceived threat of COVID-19 as risk factors for burnout among nurses. Further, a recent study has found that burnout due to occupational circumstances negatively affected nurses’ quality of life during the pandemic (Meneguin et al., 2023).
Anxiety is a psychological and physiological state characterized by cognitive, somatic, emotional, and behavioral components manifesting as unpleasant feelings (e.g., uneasiness, apprehension, fear, or worry), sleep disturbances, and higher states of autonomic stimulation (Dagget et al., 2016). In a previous study, the levels of burnout and anxiety during the COVID-19 pandemic and the influencing factors for burnout were assessed among 1,011 nurses. The study showed that anxiety was positively associated with emotional exhaustion and cynicism and was negatively associated with personal accomplishment. Further, working experience of ≤ 5 years, working in a hospital dormitory, working time exceeding 9 h, and adequate knowledge on COVID-19 were found as protective factors for burnout. In contrast, having no siblings, living in hostels, working in isolation wards, doing three or more night shifts per week, and being surrounded by COVID-19-confirmed or -suspected medical staff were found as negative factors for burnout (Wan et al., 2022).
Good physical and mental health among nurses is essential to providing quality patient care. However, the uncertainties of COVID-19 may aggravate the stress and burnout among nurses providing care. An important step to prevent stress and burnout among nurses can be the early identification of stressors to help in designing strategies to minimize these conditions. This approach can provide nurses with better work experiences. To date, few studies have examined stress and burnout among nurses in Gulf countries. Therefore, the purpose of the present investigation was to examine stress and burnout among frontline nurses working in the Ministry of Health hospitals in Najran, Saudi Arabia. Specifically, the study sought to determine the factors contributing to stress and emotions and evaluate work-related burnout among nurses during the COVID-19 outbreak.
Methods
Study Design and Research Questions
A cross-sectional survey was conducted to evaluate stress and burnout among nurses during the COVID-19 pandemic.
Setting
The study was conducted in the Ministry of Health hospitals in Najran, Saudi Arabia, during the COVID-19 pandemic.
Sample
Nurses working in nine Ministry of Health hospitals in Najran, Saudi Arabia, participated in the study. These nurses were providing care to patients with COVID-19 from June to August 2020. In total, 1,949 nurses were working in the COVID-19 units, emergency units, and intensive care units (ICUs) of the selected hospitals. However, the study sample included only 1,594 nurses who agreed to participate and met the study's inclusion criteria.
Inclusion/Exclusion Criteria
All male and female nurses who agreed to participate in the study and who were working in COVID-19 units, emergency units, and ICUs as well as nursing practitioners including nursing specialists, charge nurses, and head nurses were included in the study. In contrast, nurses who planned to resign, who extended their leave for more than 6 weeks during the study, who were working in administrative positions or in health centers, and who had missing data on the data collection instruments including the questionnaire were excluded from the study.
Ethical Considerations
The study was approved by the Institutional Review Board (IRB) with registration number KACST,KSA: H-11-N-081, in Najran, Saudi Arabia. All participants provided consent before participating in the study. Administrative permission was obtained to distribute Google Forms to the nurses. Voluntary involvement and data confidentiality were assured. Only the researchers had access to the data, which were stored in a password-protected file.
Data Collection Instruments
Part I
Sociodemographic characteristics and occupational history including age, sex, civil status, nationality, nursing tenure, area of work, average working hours per week, number of night duties per week, and provision of direct care to patients during the COVID-19 pandemic were evaluated.
Part II
COVID-19 stressors were assessed using the COVID-19 Stressors Questionnaire prepared by the researchers. The tool was prepared in reference to the MERS-CoV Staff Questionnaire (Khalid et al., 2016). The COVID-19 Stressors Questionnaire consists of 15 items scored on a 5-point Likert scale: 0 = never stressful to 4 = extremely stressful. The items are divided into two categories: (1) feelings of staff during the COVID-19 outbreak (six items) and (2) factors for stress among staff during the COVID-19 outbreak (nine items). The responses to each item on each subscale are scored and added up to obtain the total score, with higher scores indicating higher stress levels. The total score of all subscales is obtained to determine the level of COVID-19-associated stress. A total score of < 20 indicates a low level of COVID-19-associated stress; 21–40, a moderate level; and 41–60, a high level. The tool was tested for its reliability, revealing a Cronbach's alpha of .87.
Part III
The English version of the abbreviated Maslach Burnout Inventory (aMBI) (Maslach et al., 1997) was used to assess burnout among nurses. It is a nine-item scale designed for and widely used in the detection of nurses’ burnout. In a few previous studies, this tool specifically measured burnout among nurses during the COVID-19 pandemic (Elhadi et al., 2020; Ślusarz et al., 2022; Stodolska et al., 2023). There are three subscales in this scale: emotional exhaustion (emotional depletion because of employment demand and ongoing work-related obligations), depersonalization (measured answer to stress), and personal achievement (point of personal accomplishment, job satisfaction, and personal competence). There are three elements in each subscale. The responses are based on a 7-point Likert scale ranging from 0 (never) to 6 (every day). A higher score for emotional exhaustion and depersonalization suggests greater burnout, while a higher score for personal achievement indicates a better sense of success. Taken together, high emotional exhaustion and depersonalization scores and a low personal achievement score suggest increased burnout. The sum of the emotional exhaustion and depersonalization scores is used to calculate the total burnout score. Each subscale score ranges from 0 to 18. Burnout is defined as “no to low burnout” for emotional exhaustion and depersonalization and “moderate to severe burnout” for emotional exhaustion and depersonalization. Because higher personal achievement scores suggest less burnout, the definition is reversed for personal achievement. A score of 10 indicates significant burnout relative to personal achievement in the profession. The total score for each item is added up. The reliability of the aMBI is .99. The tool is available in the public domain.
Data Collection Procedure
As the study was performed during the COVID-19 pandemic, the isolation policy advocated for limiting face-to-face contact and avoiding large gatherings. Therefore, the researchers decided to collect the data via Google Forms. The form was shared through the nurses’ WhatsApp groups and email IDs. The email ID was requested in the form. Duplicate entries, which were identified using the email IDs, were removed.
Statistical Analysis
Data entry and statistical analysis were conducted using SPSS 21. The sample characteristics were described as frequencies and percentages. The chi-square test was used to determine the association of the level of burnout with the demographic variables.
Results
Demographic Variables of the Participants
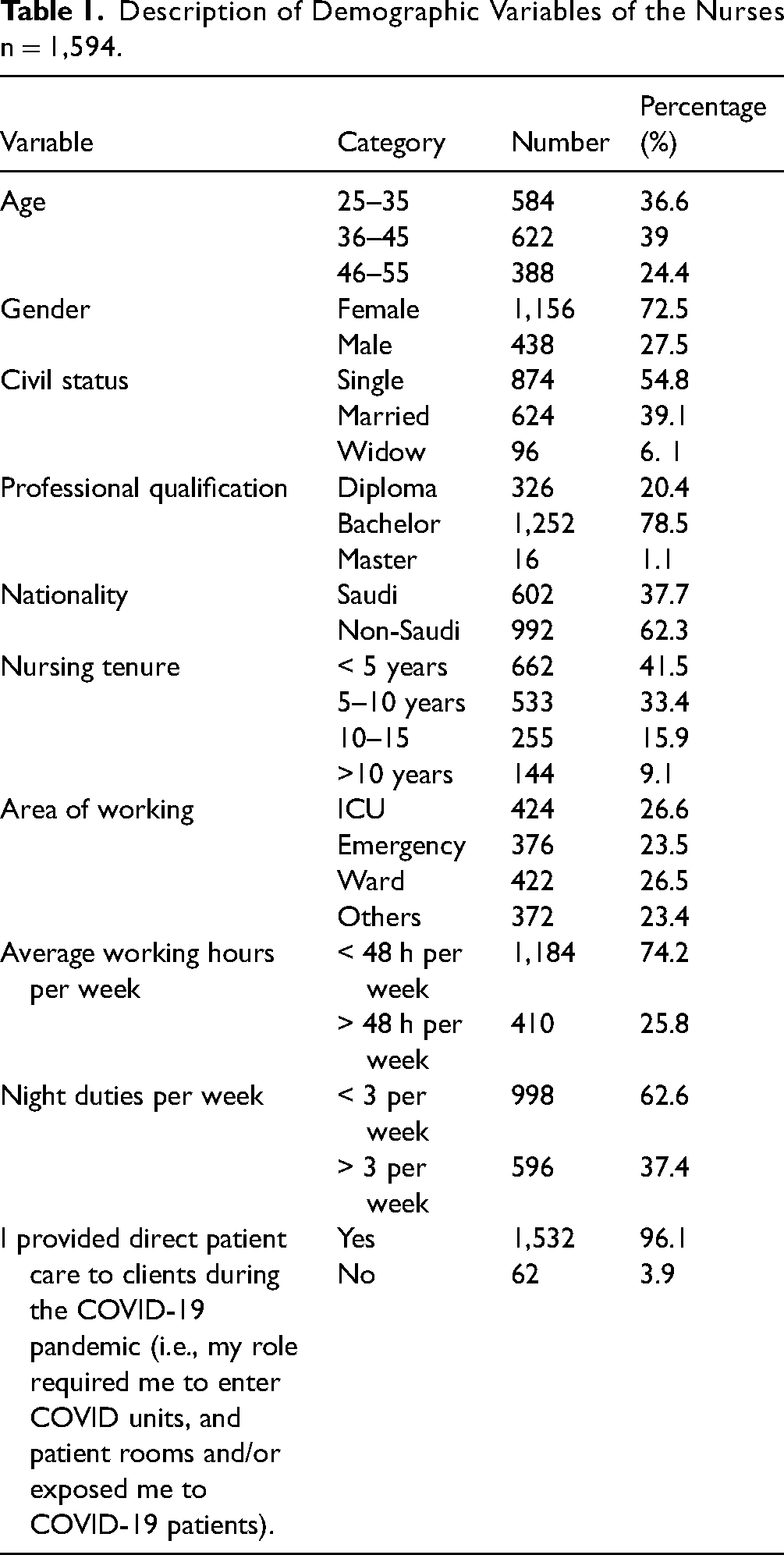
Table 1 shows the demographic variables of the participants. The majority of the participants were aged from 36 to 45 years (n = 622; 39.0%); were women (n = 1,156; 72.5%); were single (n = 874; 54.8%); had a bachelor's degree (n = 1,252; 78.5%); were non-Saudis (n = 992; 62.3%); had ≥ 5 years of nursing work experience (n = 662; 41.5%); worked in ICUs (n = 424; 26.6%); worked for an average of 48 h per week (n = 1,184; 74.2%); worked three night shifts per week (n = 998; 62.6%); and provided direct care to patients during the COVID-19 pandemic (n = 1,532; 96.1%).
Description of Demographic Variables of the Nurses n = 1,594.
Factors Contributing to the Nurses’ Stress During the COVID-19 Outbreak
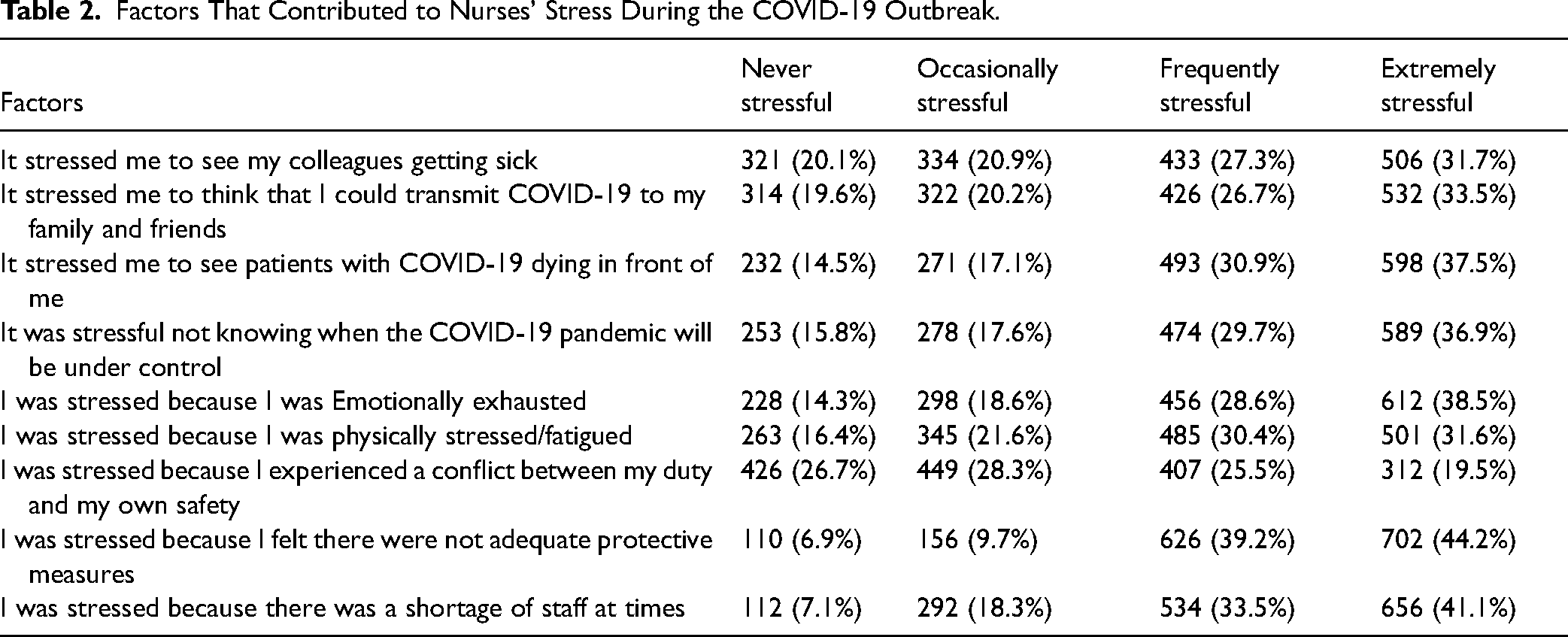
Table 2 displays the factors that contributed to the nurses’ stress during the COVID-19 outbreak. A total of 506 (31.7%) nurses stated that they experienced extreme stress to see their colleagues getting sick. Several nurses (n = 532; 33.5%) experienced extreme stress thinking about the possibility of spreading COVID-19 to their family and friends. Approximately 36.9% (n = 589) of the nurses indicated that it was upsetting for them to see patients with COVID-19 dying in front of them. With regard to not knowing when the COVID-19 pandemic will be under control, 589 (36.9%) nurses showed an extreme level of stress. Furthermore, 612 (38.5%) nurses were extremely stressed because they were emotionally exhausted. A major proportion of the nurses (n = 501; 31.6%) were extremely stressed because they were physically stressed/fatigued. Most participants (n = 449; 28.3%) said that they were occasionally stressed as they experienced conflict between their duty and their own safety. With respect to protective measures, the majority of the participants (n = 702; 44.2%) reported that they lacked supplies to protect them. Meanwhile, 656 (41.1%) participants showed an extreme level of stress about the shortage of nurses.
Factors That Contributed to Nurses’ Stress During the COVID-19 Outbreak.
Factors Contributing to the Nurses’ Emotions During the COVID-19 Outbreak
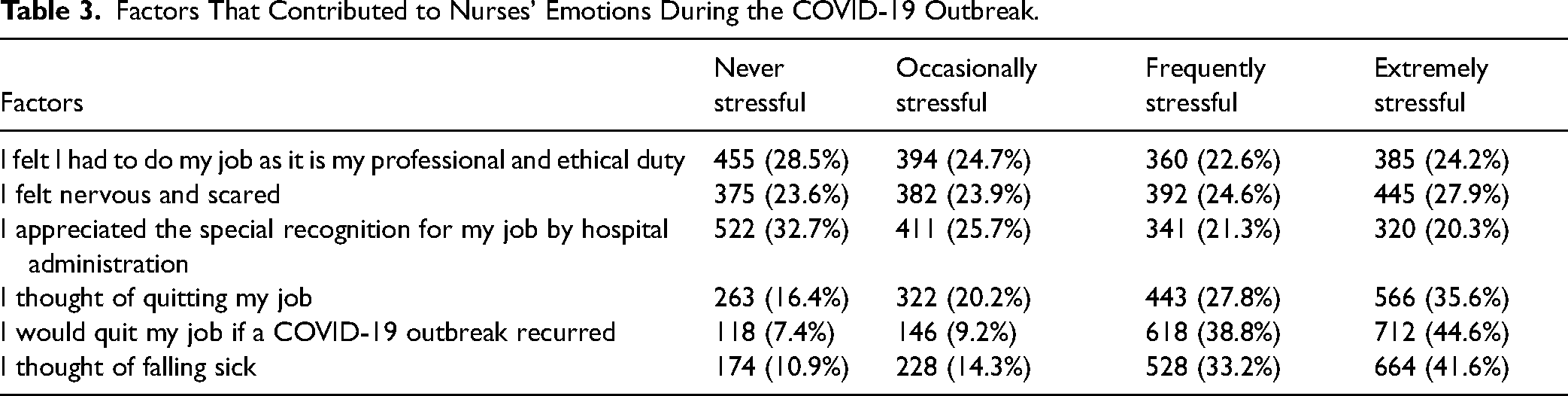
Table 3 shows that the majority of the respondents (n = 455; 28.5%) were rarely stressed about their job because they felt that it was their professional and ethical responsibility. Approximately 27.9% (n = 445) of the nurses mentioned that they were nervous and scared. Most participants (n = 522; 32.7%) stated that they were appreciated and recognized by the hospital administration for their work. Several nurses reported that they thought of quitting their job (n = 566; 35.6%) and that they would quit their job if the COVID-19 outbreak recurs (n = 712; 44.6%). Lastly, nearly half of the nurses (n = 712; 44.6%) mentioned that they thought of falling sick.
Factors That Contributed to Nurses’ Emotions During the COVID-19 Outbreak.
Work-Related Burnout Among the Nurses During the COVID-19 Outbreak
Pareto charts were created to rank the burnout experienced by nurses during the COVID-19 pandemic. Emotional exhaustion was experienced by 66.4% of the nurses. Several nurses (n = 1,091; 68.4%) mentioned: “I feel emotionally exhausted from my work.” A major proportion of the nurses (n = 1,062; 66.7%) expressed “I feel fatigued when I get up in the morning and have to face another day on the job.” The majority (n = 1,024; 64.3%) agreed that they were working with people all day. Depersonalization was perceived by 56.6% of the nurses. A total of 924 (58.2%) nurses experiencing burnout stated that they felt that they treated some patients like impersonal objects, while 892 (56%) stated that they had become more callous toward people since starting their profession. Some nurses (n = 839; 55.4%) mentioned: “I genuinely don’t care what happens to some patients.” The personal accomplishment was expressed by 48.4% of the participants. Most participants agreed with the following statements: “I feel I’m positively influencing other people's lives through my profession” (n = 771; 48.4%) and “I feel thrilled after working closely with my patients” (n = 701; 44.4%) (Figure 1). Figure 2 shows that 668 (41.9%) nurses reported that they were experiencing high levels of burnout; 522 (32.8%), moderate levels of burnout; and 404 (25.3%), low levels of burnout.

Pareto chart showing burnout among nurses during the COVID-19 outbreak.

Burnout scores of the nurses according to the abbreviated Maslach Burnout Inventory.
Association Between the Levels of Burnout During the COVID-19 Pandemic With the Demographic Variables of the Nurses
The area of work was significantly related to the level of burnout among the nurses during the COVID-19 pandemic at a 0.0572 level; in contrast, the other demographic variables such as age, sex, and civil status had no significant relationship with the level of burnout among the nurses (Table 4).
Association Between the Level of Burnout During the COVID-19 Outbreak Among Nurses With Their Selected Demographic Variables.

Discussion
Work-related stress (WRS) is a major issue for both workers and organizations in the healthcare sector (Lim et al., 2019). It exists in every profession, but nurses experience higher levels of stress than do any other healthcare workers (d’Ettorre et al., 2019). Nurses are exposed to a variety of physical, psychological, and social stressors in their workplace, the levels of which are much higher among frontline nurses caring for patients with COVID-19 (Dagget et al., 2016). In our study, 63.8% of the nurses experienced extreme levels of stress. Of these nurses, 72.5% were women. Similarly, d’Ettorre et al. (2019) and Yada et al. (2014) reported a high level of stress among female healthcare workers and a lack of social support as a determinant for extreme stress (Zakeri et al., 2021). Zhang et al. (2020b) also pointed out that female nurses experienced psychological distress during the COVID-19 pandemic. On the contrary, Lee and Cho (2016) and Diale et al. (2020) showed that male nurses experienced more stress than did female nurses. Therefore, further studies are recommended to explore these contradictory study findings.
The factors that contributed to the nurses’ stress during the COVID-19 outbreak were also explored in our study. The majority of the participants were extremely stressed about the shortage of nurses. In nursing shortage, the demand for nurses exceeds the supply (Calman & Buchan, 2004) owing to the aging nursing workforce and changing demographics of the human population (Buerhaus et al., 2000). A shortage of nurses leads to stress, burnout, and job dissatisfaction among nurses (Toh et al., 2012). Similar to our study findings, Faraji et al. (2019) and Sharma et al. (2014) reported role overload as an important indicator for moderate to high levels of stress among nurses. Therefore, to reduce stress among nurses, organizations should customize their strategies for effective recruitment and retention of nurses. Additionally, hospital managers should initiate strategies to minimize occupational stress and should provide support to nurses to manage their stress.
Our study found that several nurses were extremely stressed about their fear of spreading COVID-19 to their family and friends. Consistent with this finding, Moussa et al. (2021) and Mohsin et al. (2021) found that Saudi nurses reported fear of COVID-19. This finding was also noted among Jordanian nurses in another study. Accordingly, sufficient information and support should be provided to alleviate fear among nurses. In addition, assessing the level of fear among nurses caring for patients with COVID-19 should be the priority of healthcare administrators to prevent psychological injury in nurses.
The nurses in our study were emotionally exhausted and physically stressed/fatigued. The COVID-19 pandemic has significantly impacted the physical and mental well-being of healthcare workers. During the pandemic, healthcare workers were anxious and depressed and experienced sleep disturbances (Lin & Zheng, 2021). Further, moderate to severe anxiety, stress, and depression were reported among nurses who experienced social rejection, who watched the television, who had temporary contracts, and who had financial hardships (Fathiariani & Nassimbwa, 2021). As the pandemic has posed a significant threat among healthcare workers worldwide, their physical and psychological stresses must be managed with efficient measures. Organizations and healthcare providers must pay more attention toward the early detection and reduction of stress by providing recreational facilities, conducting regular meetings to facilitate reflection on problems, and increasing the number of nurses (Mohsin et al., 2021).
Our participants expressed that it was upsetting for them to see patients with COVID-19 dying in front of them. Similar to this finding, nurses in another study expressed that the worst part of the pandemic was watching patients die without anyone nearby: Their families were not able to see them in their last moments, and they died without their loved ones by their side (Robinson & Stinson, 2021). Moreover, end-of-life care during the COVID-19 pandemic was less appreciated in hospitals. Thus, it is recommended to optimize care, especially in nursing homes and hospitals. Visits by relatives to some level are also a key component (Onwuteaka-Philipsen et al., 2021). The nurses in our study were also stressed about not knowing when the COVID-19 pandemic will be under control. The COVID-19 pandemic has effected unsettling changes for years now. It has disrupted societies worldwide and caused long-term unpredictable and uncontrollable situations (Sharma et al., 2020). Therefore, different types of uncertainty and their antecedents and outcomes should be identified to mitigate their impact.
In our study, most participants were occasionally stressed as they experienced conflict between their duty and their own safety. Similarly, Alyahya et al. (2021) found role conflict and ambiguity as factors causing stress among nurses during the COVID-19 pandemic. Therefore, consistent scheduling of duties is essential, and modifiable factors in the hospital should be considered to reduce stress among nurses (Malinowska-Lipień et al., 2022). Lastly, the lack of supplies for protection was another factor causing stress among the nurses in our study. Razu et al. (2021) also reported a shortage of quality PPE as a challenge faced by nurses in their study. These findings imply the need to provide adequate quality supplies and safety kits and protocols to enhance the physical and psychological well-being of nurses.
A major proportion of the nurses in our study were nervous and scared during the pandemic. Similarly, Abid et al. (2021) reported a predictive association between fear of COVID-19 and emotional distress among nurses. Maslakçı et al. (2021) showed that fear of COVID-19 affected the quality of work life of nurses. Strategies to manage stress and reduce fear can help nurses to overcome emotional distress, thereby increasing their productivity. Moreover, enhancing the psychological well-being of nurses can reduce the negative effects of the fear of COVID-19.
Several nurses in our study also reported that they thought of quitting their job and that they would quit their job if the COVID-19 outbreak recurs. In their systematic review of 15 articles, Ayalew et al. (2021) demonstrated that a pooled proportion of nurses had the intention to leave their job during the COVID-19 pandemic. Similarly, Falatah (2021) found that nurses’ turnover intention increased significantly after the pandemic. Thus, the reasons for quitting the job among nurses should be identified, and strategies, policies, and programs should be designed to reduce the negative impact of COVID-19 on the retention of nurses. Lastly, nearly half of the nurses in our study mentioned that they thought of falling sick. The COVID-19 pandemic has inflicted a significant burden of mortality and morbidity among healthcare workers. In a previous study, sickness-related absence was reported among 9.1% of healthcare workers. A high level of sickness was seen in adult and pediatric emergency departments (Khorasanee et al., 2021). Accordingly, further studies are required to understand the frequency and causes of sickness among frontline nurses during the COVID-19 pandemic.
Burnout is a self-reported state of care- or work-related physical and mental stresses that cause emotional exhaustion, depersonalization, and reduced personal accomplishment (Rodrigues et al., 2018). In our study, 41.9% of the nurses showed high burnout levels. Emotional exhaustion was experienced by 66.4% of the nurses; depersonalization, by 56.6%; and personal accomplishment, by 48.4%. Similar to our study findings, Khasne et al. (2020) found a significant prevalence of burnout among healthcare workers and a higher prevalence among women. In the recent study conducted by Aranda-Reneo et al. (2021), nurses working in primary care centers experienced high levels of burnout. A systematic review that assessed job burnout among nurses during the pandemic revealed that 57.14% and 42.86% of nurses experienced moderate and high levels of burnout, respectively (Zareei et al., 2022).
In another study published in 2022, nurses experienced severe symptoms of burnout and moderate levels of resilience. The domains of emotional exhaustion and personal accomplishment had a significantly negative correlation with resilience. The study further found the type of hospital, type of ward, sex, and working overtime as the major predictors of burnout (Jamebozorgi et al., 2022). Similarly, burnout was frequent in nurses who were younger and those with fewer years of experience. Being around a person infected with COVID-19, working for longer hours, being assigned to treat patients with COVID-19, experiencing verbal and physical abuse from patients, and having fewer sleeping hours also contributed to severe burnout among nurses (AlJhani et al., 2021).
As nurses are exposed to physical and mental exhaustion due to the pain of losing patients and their colleagues, fear of transmitting the infection to themselves and their families, and other work-related factors, healthcare administrators should be proactive in providing a supportive environment and improving working conditions to minimize the consequences of excessive burnout. Strategies at the individual level, including balanced diet, physical activity, good sleep hygiene, family support, reflective practice, and meaningful relationship, should be encouraged. At the organizational level, multi-disciplinary psychosocial support, adequate time planning, blame-free working environment, involvement in management decisions, social support, and other strategies to avoid stressful situations should be provided. At the cultural level, healthcare workers should be involved in the development, testing, and evaluation of measures against burnout (Leo et al., 2021). Taken together, the key recommendation is to address the challenges experienced by nurses to consequently improve public health systems.
Strengths and Limitations of the Study
This study outlined WRS and burnout among nurses working in a Middle Eastern country. However, further studies are recommended to be conducted worldwide to find a solution to mitigate stress and burnout among nurses.
The present study has a number of limitations. First, the study used a cross-sectional research design, limiting the ability to evaluate stress and burnout among nurses in the long term. Second, the survey was performed online with voluntary participation, which might have led to selection bias. Third, the study was conducted only in the Ministry of Health hospitals in Najran, Saudi Arabia, limiting the generalizability of the study findings.
Implications for Practice
Personalized interventions can be implemented to assist frontline nurses in maintaining their mental health and to improve their quality of life. Stress and burnout can be regularly evaluated among nurses to predict their quality of life. Moreover, the influencing factors of stress and burnout can be identified to design strategies to minimize these conditions.
Conclusion
Nurses caring for patients with COVID-19 experience high levels of stress and burnout. It is critical to recognize the extent of stress and burnout among nurses, especially given the length of the pandemic. Moreover, it is important to monitor the emotional well-being of nurses. Regular programs should also be organized to support nursing staff, and strategies should be designed to enhance their overall psychological well-being. Maintaining the psychological well-being of nurses requires real-time information and solutions for reducing WRS and its associated negative impacts.
Footnotes
Acknowledgements
The authors thank the nurses who actively participated in the study.
Ethical Considerations
The study was approved by the Institutional Review Board (IRB) with registration number KACST, KSA: H-11-N-081, in Najran, Saudi Arabia.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.