
Abstract
Introduction
For healthcare workers, good work-related well-being positively affects enthusiasm, efficiency, and job satisfaction. Conversely, poor well-being is associated with burnout and negative patient outcomes. During times of crises, it is difficult to balance professional responsibilities with well-being.
Objective
This study aimed to evaluate the degree of well-being among nurse practitioners in Israel who worked in COVID-19 units or allied units during the delta wave.
Methods
This was a web-based, cross-sectional study. Nurse practitioners who worked within the COVID-19 units in Israeli hospitals were asked to complete several questionnaires: a sociodemographic questionnaire, the Subjective Happiness Scale, the Mental Health Continuum-Short Form, and the Center for Epidemiologic Studies-Depression.
Results
Forty-nine nurse practitioners participated in the survey. Scores from the Subjective Happiness Scale and the Mental Health Continuum-Short Form indicate that most nurses have relatively positive mental health. Conversely, scores on the Center for Epidemiologic Studies indicated that participants are at risk for clinical depression. There was a positive moderate association between the number of years worked as a nurse practitioner and depression and a moderate negative association between the number of years worked as a nurse practitioner and happiness.
Conclusions
Understanding how nurses’ mental health is impacted during crises can provide healthcare systems with tools to prevent negative outcomes. This, in turn, may contribute to a lower burnout rate, higher satisfaction from work, and better patient outcomes.
Introduction
In the workplace, the balance between positive and negative affects plays a crucial role in employee well-being (Yoon et al., 2022). Well-being is a combination of a positive mental state that includes emotional stability, involvement, meaning, optimism, positive emotions, resilience, self-esteem, vitality, and access for basic resources. There are different types of well-being, such as subjective well-being, work well-being, social well-being, and psychological well-being (Brough & Pears, 2004; Diener et al., 2018; Keyes, 1998; Schulte & Vainio, 2010). The future of healthcare systems depends on the ability of healthcare professionals to cope with and adapt to crises, such as the shattering events (Institute of Medicine, 2011). As such, it is crucial to understand the factors that contribute to resilience, happiness, and well-being among these professionals.
Dodge et al. (2012) define well-being as “as the balance point between an individual's resource pool and the challenges faced” (p. 223). Scaria et al. (2020) define physician well-being as “The ability to appropriately respond to expected and unexpected stresses in order to be healthy, happy and prosperous in work and in life.” Both of these definitions highlight the fact that in order to maintain a state of well-being, an individual must have the appropriate resources to cope with challenges. If a person has more challenges than available resources, their well-being suffers. Studies on nurses and well-being demonstrated this concept by showing that nurses who reported a lower level of work–life balance also reported lower psychological well-being, higher rates of burnout, and lower self-reported health (Burke et al., 2012; Vallone et al., 2020).
Resilience is a multifaceted construct that encompasses various aspects of psychological, emotional, and social well-being (Atkinson, 2020). In the face of adversity, individuals who exhibit higher levels of resilience often engage in health-related behaviors and maintain a strong sense of spirituality, both of which are linked to improved psychological well-being (Bożek et al., 2020). Eiroa-Orosa (2020) posits that understanding psychosocial well-being in the context of complex and multidimensional problems requires a comprehensive approach, taking into account the interplay of individual, social, and environmental factors.
Happiness includes a variety of aspects, with resilience being a central component. In the healthcare system, the working environment often presents grim working conditions, a heavy workload, ineffective management policy, limited support, limited opportunities for promotion, and inadequate salaries (Rathnayake et al., 2021). Happiness is an essential component for many professions but is especially crucial for the nursing profession. Nurses come in direct contact with patients in various situations that require altruism, self-confidence, creativity, courtesy, and energy (Kakemam et al., 2019).
Mental illnesses, which include depression and anxiety disorders, negatively affect workplaces and can significantly affect the mental well-being of nurses, endanger patient care, and increase the risk (Heesakkers et al., 2021). Depression among healthcare workers has been defined as being affected mainly by stress, tension, strain, and weariness Moreover, during the COVID-19 pandemic, there was an additional layer of professional isolation added to uncertainty. Nurses reported a lack of clarity about their role and practice and were frightened of being caught between the world of medicine and nursing without proper tools (Wood et al., 2021).
Several factors affect the well-being and welfare of nurses (Bożek et al., 2020; Coppola et al., 2021; Gray et al., 2019). Specifically, there are three dimensions that influence work mental health (Gray et al., 2019). The first dimension is the scope of practice: high demand, low control, and balance between effort and rewards. The second is the organizational environment, such as obligatory shifts, job modifications, sense of security, and social support. Lastly, external factors such as personal boundaries, marital status, and surrounding network also affect workplace well-being. Higher work-related well-being positively affects enthusiasm, efficiency, and job satisfaction, while a low level is associated with leaving the profession and negative patient outcomes (Yoon et al., 2022).
In some cases, it is more difficult for the nurse to balance professional responsibilities with well-being. This is especially true during disasters and times of crises. Disaster contexts are diverse and multidimensional and include both natural phenomena, such as floods, droughts, and hurricanes, and anthropogenic crises, such as fires, wars, and disease outbreaks in susceptible areas. Regardless of the disaster's origin, the role of nurses as primary responders is pivotal in these dire situations (International Council of Nurses, n.d.). Each disaster type demands a distinct repertoire of skills or specialized training for effective management. It is imperative for healthcare practitioners, particularly nurses, to prioritize their safety and well-being while demonstrating proficiency in their professional responsibilities. Their preparedness and competence in disaster response cannot be overemphasized, as it facilitates efficient healthcare and safeguards the responders themselves (Rokkas et al., 2014). Moreover, it is sometimes difficult to make ethical decisions as a nursing professional, while being in a life-and-death situation.
Crisis situations are inevitable in today's complex world, affecting individuals, communities, and entire nations. These challenging times demand resilience, defined as the capacity to adapt positively to adversity, maintain or regain well-being, and continue to function effectively (Aburn et al., 2016). The COVID-19 pandemic, in particular, has brought to light the importance of understanding and promoting resilience, especially among healthcare professionals who have been at the forefront of the crisis response (Hall, 2020).
Nurse Practitioner in Israel: A New Role
The Institute of Medicine (2011) defines the role of the nurse practitioner (NP) in healthcare as a qualified nurse who works in an ever-changing healthcare landscape and for whom an essential element of their role is to improve care and promote access to care. The nurse practitioner is a new and growing role in the Israeli health sector, having been introduced a mere decade ago. Nurse practitioners who specialize in palliative care, geriatrics, and neonatal care were the first to be introduced to the healthcare system. The nurse practitioners have an essential role in the provision of quality care to patients, especially in light of growth of the older adult population (Institute of Medicine, 2011), need for a complex care, and physician shortage (Haron et al., 2019). However, due to the structure of and legislation related to the Israeli healthcare system, nurse practitioners are limited in their ability to practice their full scope of qualifications (Haron et al., 2019).
The COVID-19 Delta Wave in Israel
According to earlier studies on the outbreak of infections, healthcare workers are at higher risk for poor mental health during outbreaks. Three characteristics of the COVID-19 pandemic increased poor mental health among healthcare workers: (1) the scale of the victims, (2) change in individual practice settings, and (3) uncertainty regarding health guidelines (De Kock et al., 2021).
The first cases of the delta variant in Israel were confirmed on 16 April 2021, and it subsequently spread quickly through June 2021. This wave of morbidity was different from previous waves, in two ways. First, a significant majority of society in Israel was vaccinated. The absolute majority of the hospitalized patients in serious condition during this wave were people who had not been vaccinated (Ministry of Health, n.d.). Second, for the first time, vaccinated people got sick as well, although on a smaller scale. This resulted in the return of COVID-19-related restrictions, such as a limited gatherings and mask mandates (Lipsitch et al., 2022). By the end of September 2021, about 14% of Israel's population had been infected, of whom 7,800 had died (Weinreb, 2021).
Objectives
This is the first survey related to nurse practitioner well-being conducted in Israel during the COVID-19 delta wave. The overall aim of the study is to evaluate the degree of well-being among NPs in Israel who worked in COVID-19 units or allied units during the delta wave. Specifically:
To examine the level of happiness, sense of well-being, and depression among cohort of nurse practitioners in Israel during the COVID-19 delta wave, specifically the difference in well-being between NPs in COVID-19 units and those in allied units To examine the association between happiness, wellbeing, and depression and sociodemographic parameters To compare observed happiness, sense of well-being, and depression among Israeli NPs to the literature review
Methods
Design
This is a cross-sectional, descriptive study.
Research Question
Was the delta wave in Israel associated with poorer well-being (measured by the degree of reported happiness, resilience, and depression) among nurse practitioners working in COVID-19 or allied units in Israeli hospitals?
Sampling, Recruitment, and Sample Size
Forty-nine (36.0%) nurse practitioners participated in this study, out of 136 who worked in COVID-19 units or allied units.
Inclusion/Exclusion Criteria
Included in the study were nurse practitioners who hold a registered nurse certification, master's degree, and nurse practitioner certification; are fluent in Hebrew; provided informed consent; and were working in the COVID-19 units or allied units (units connected to COVID-19 units, such as the emergency department). The study population included nurses from health maintenance organizations, hospitals, and geriatric medical centers.
Measures
This research used three validated questionnaires and a sociodemographic questionnaire for data collection. The three validated questionnaires were:
Subjective Happiness Scale (SHS) Mental Health Continuum-Short Form (MHC-SF) Center for Epidemiologic Studies-Depression (CES-D)
The Subjective Happiness Scale
The Subjective Happiness Scale (SHS) is a four-item scale of global subjective happiness. Two items ask respondents to characterize themselves using both absolute ratings and ratings relative to peers, while the other two items offer brief descriptions of happy and unhappy individuals and ask respondents the extent to which each characterization describes them. The SHS Cronbach's alpha is 0.79 to 0.94 (M = 0.86). Higher scores indicate high levels of happiness and x = 5.3- less than the average (Lyubomirsky & Lepper, 1999).
Mental Health Continuum-Short Form (MHC-SF)
The MHC-SF is a scale measuring well-being. Each of the 14 items on the MHC-SF can be scored in Likert scale between 0 and 5, with the total score on the scale ranging from 0 to 70 points. Higher scores indicate a higher level of emotional well-being. In addition to the overall score, the MHC-SF can determine if someone is flourishing and languishing or has a moderate mental health. Cronbach's alpha is 0.89 for the entire questionnaire and ranging from 0.74 to 0.93 for each section.
Center for Epidemiologic Studies-Depression (CES-D)
The CES-D scale is a brief, self-reported scale designed to measure self-reported symptoms associated with depression experienced in the past week. The scale includes 20 items reflecting major facets of depression: depressed mood, feelings of guilt and worthlessness, feelings of helplessness and hopelessness, psychomotor retardation, loss of appetite, and sleep disturbance (Radloff, 1977). Score ranges from 0 to 60, with high scores indicating greater depressive symptoms. CES-D with cutoff 16 and up are able to identify individuals that are at risk for clinical depression.
Additionally, we collected sociodemographic characteristics via a questionnaire: age, sex, average monthly income, and seniority in nursing. The income level variable had three options, above average, average, and below average, based on the relation to the Israeli average income.
Data Collection
The researchers shared the web-based survey composed of the four questionnaires in WhatsApp chat groups and email lists of registered NPs working in COVID-19 or allied units between October 2021 and February 2022. The survey was sent to all nurses who completed the academic program for nurse practitioners at the Jerusalem College of Technology or through the Ministry of Health program. Collected data was anonymous. From 136 questionnaires sent out, 49 responses were collected for a response rate of 36%.
Ethical Considerations
Ethical approval for this study was obtained from the Jerusalem College of Technology Ethics Committee (approval no.: 21_014). Introduction to the study and the provision of informed consent were on the first page of the survey. Completion of the electronic questionnaire was voluntary; participants could choose to answer yes or no on the consent form. A participant who refused to participate could select no, and the survey ended. In that case, no personal information was collected.
Statistical Analysis
Categorical variables presented as frequencies with percentages. Univariate analyses included chi-square and a one-way analysis of variance (ANOVA) followed by Tukey's post hoc tests to determine the nurse practitioner specialty in which professional is differed significantly. The level of significance was set at a p-value of 0.05. The data were normally distributed without outliers or missing values. Pearson's correlation coefficient analysis was used to investigate the relationships among depression happiness satisfaction and occupational well-being. The Statistical Package for the Social Sciences version 27 (SPSS Inc., Chicago, Illinois) was used for all data analyses.
Results
Sample Characteristics
A total of 49 nurse practitioners completed the survey. The majority of participants were women (89.8%), were married or with a partner (77.6%), were Jewish (89.8%), and had a graduate degree (91.8%). More than half of the participants defined themselves as secular (57.1%). The ages of the nurse practitioners ranged between 33 and 66, with the average age of the participants of 49.8 years. The average number of years worked as a nurse among the participants is 24.7, while the average number of years as a nurse practitioner is 4.5. The most common specialty was geriatrics (53.1%), and almost three-quarters of the respondents currently work as nurse practitioners (73.5%) within the COVID-19 units and 26.5% worked in allied units. The majority (67.4%) work in a full-time position, and close to half (46.9%) work in general hospitals. Other participant characteristics are shown in Table 1.
Participant Demographics.
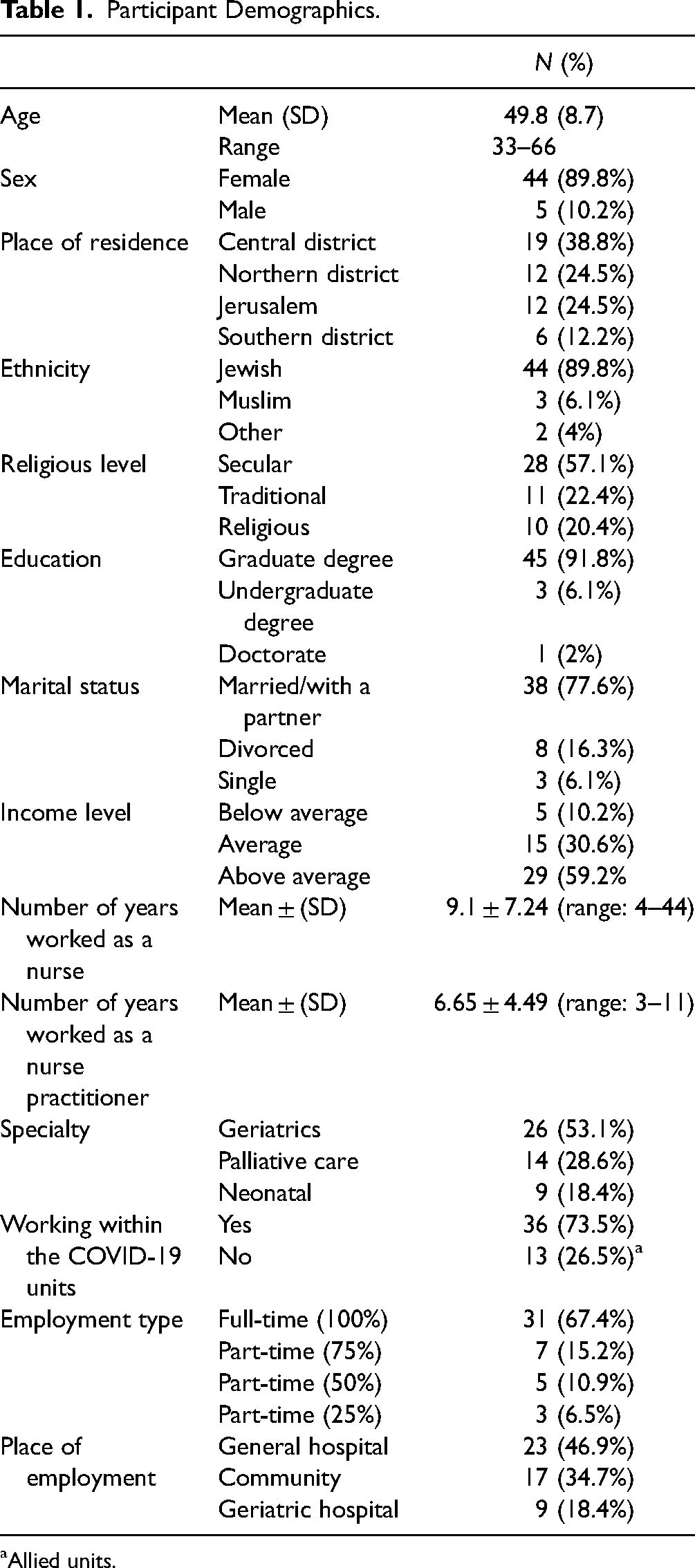
Allied units.
Scale Results
Almost half of the respondents (48.9%) reported having 17 or more depressive symptoms, according to the CES-D measure. Table 2 is a summary of the mean scores of all the scales and subscales among the entire study population. Scale total scores are in bold.
Summary of Means, Standard Deviation for All Scales and Subscales (SHS, MHC-SF, CES-D) (N = 49).

Note: Overall scores by specialty are in bold.
When stratifying the SHS scores by nurse practitioner specialty, no statistically significant difference was found among the three groups (geriatric, palliative care, neonatal) (F(2,46) = 0.319, p = 0.729). No statistically significant difference among the three groups was found for well-being in the MHC-SF scale (F(2,46) = 0.52, p = 0.598) or for any of the subscales (emotional well-being: F(2,46) = 0.085, p = 0.919; social well-being: F(2,46) = 1.083, p = 0.347; psychological well-being: F(2,46) = 0.196, p = 0.823). Additionally, there was no statistically significant difference in levels of depression among the three nurse practitioner groups, according to CES-D scale (F(2,46) = 0.432, p = 0.652). Nor were any statistically significant differences among any of the four subscales (depressive affect: F(2,46) = 0.546, p = 0.538; positive affect: F(2,46) = 0.292, p = 0.748; somatic and retarded activity: F(2,46) = 0.355, p = 0.703; interpersonal: F(2,46) = 0.223, p = 0.801) (Table 3).
Relative and Absolute Happiness SHS, MHC-SF, and CES-D (Mean, Standard Deviation, One-Way ANOVA) Between the Three Nurse Practitioner Specialties.

Note: Overall scores by specialty are in bold.
Additional Findings
There were no statistical differences in the levels of happiness, well-being, and depression by level of average monthly income (below average, average, and above average) (F(2,46) = 2.93, p = 0.063). For the MHC psychological well-being index, there was a significant difference in well-being levels between households with less than average income and those with average income (mean difference = 0.7, p = 0.106). However, there were no statistically significant differences in well-being levels between households with average income and those with more than average income. For the CES-D depressive affect, CES-D positive affect, CES-D somatic and retarded activity, and CES-D interpersonal scales, there were no significant differences in well-being levels between different levels of household income.
No statistically significant differences were observed for well-being (F(2,46) = 1.624, p = 0.208). When looking at each of the subscales separately, no statistically significant differences were found (emotional well-being: F(2,46) = 0.698, p = 0.503; social well-being: F(2,46) = 0.648, p = 0.528; psychological well-being: F(2,46) = 2.442, p = 0.098). Furthermore, no statistically significant differences were observed in levels of depression among the three income groups (F(2,46) = 0.314, p = 0.458). Additionally, no statistically significant differences were observed in the four subscales among the three groups (depressive affect: F(2,46) = 0.314, p = 0.732; positive affect: F(2,46) = 0.739, p = 0.438; somatic and retarded activity: F(2,46) = 0.878, p = 0.422; interpersonal: F(2,46) = 1.396, p = 0.258) (Table 4).
MHC-SF, SHS, and CES-D (Mean, Standard Deviation, One-Way ANOVA) of All Three Income Groups.

Note: Overall scores by specialty are in bold.
Table 5 shows no significant association between the level of seniority as a nurse (in years worked) and happiness, mental health, and depression. Conversely, there was a positive moderate association between the number of years worked as an nurse practitioner and depression (r(49) = 0.341, p = 0.019) and a moderate negative association between the number of years worked as an nurse practitioner and happiness (r(49)= −0.345, p = 0.017).
Matrix of Pearson's Correlation Coefficient Between the Dependent Variables and Number of Years Worked (N = 49).
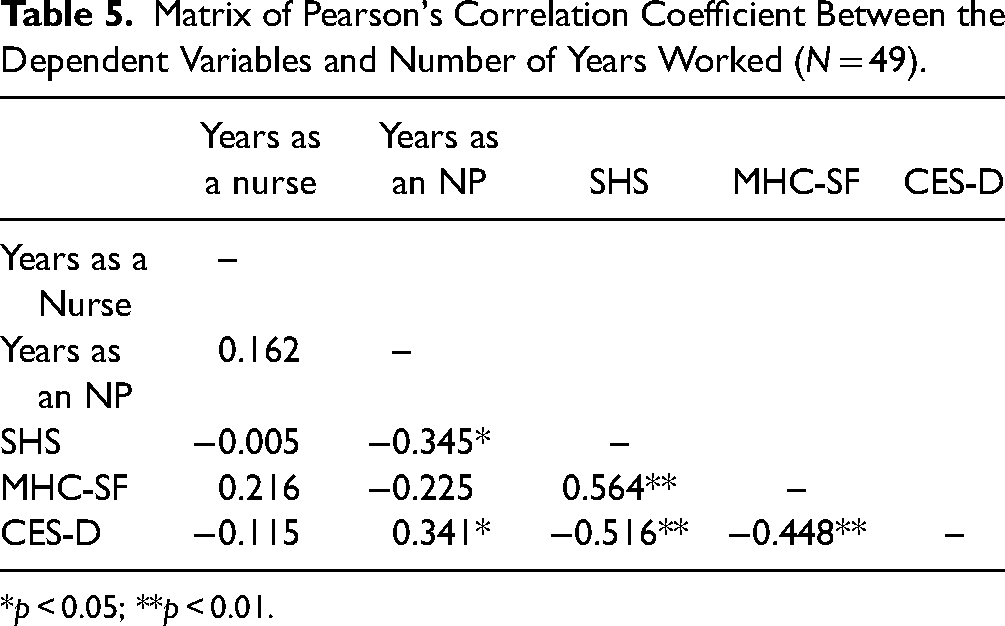
*p < 0.05; **p < 0.01.
Discussion
The aim of this study was to evaluate the emotional and professional well-being of three different Israeli nurse practitioner subgroups including geriatric, palliative care, and neonatology nurse practitioners. Previous studies have demonstrated the strong association between well-being and work conditions among nurses particularly that a weak work–life balance has a negative effect on the overall well-being of nurses and other healthcare workers (Burke et al., 2012; Vallone et al., 2020). The COVID-19 delta wave was particularly challenging as nurses (and other healthcare workers) had already been coping with the COVID-19 pandemic during the previous year, and it was believed (at first) that once the majority of the population was vaccinated, the Israeli healthcare system would no longer be in a state of crisis.
In this cross-sectional study, nurse practitioners working in COVID-19 units or allied units in hospitals were surveyed. Data was collected via an online, anonymous survey sent out to nurse practitioner WhatsApp groups and email lists. All groups surveyed were actively working in the profession during the recent COVID-19 delta wave period, either in COVID-19 units or in allied units. The above comparison enabled us to isolate the effect of direct COVID-19 patient care imposed on nurse practitioners as opposed to other factors such as demographics, seniority in the nursing profession, and more specifically seniority as a nurse practitioner. The results indicate that the only parameter related to decreased well-being and higher depression scores was seniority as a nurse practitioner. No difference was demonstrated between COVID-19 treatment group nurse practitioners (geriatric, palliative care) and the non-COVID-19 treatment nurse practitioners (neonatology). Neither did overall seniority as a nurse have any impact on well-being, happiness, or depression score.
The COVID-19 pandemic has caused physiological, emotional, and economical strain globally, negatively affecting the well-being of healthcare workers (Scaria et al., 2020). The delta wave, in particular, exposed the vulnerability of the healthcare workers, when even vaccinated health workers could be infected and transmit the virus to others. Healthcare providers saw more patients during each shift, were exposed to increased crisis and escalating life and death situations, and felt isolated inside the COVID-19 unit (this feeling was prevalent among both staff and patients). They also expressed fear of the unknown and were required to learn new skills and responsibilities that were not part of their own scope of practice (Rathnayake et al., 2021).
Nurses’ well-being is inherently tied to their work, as demonstrated in several studies (Burke et al., 2012; Vallone et al., 2020). Oncology nurses, for example, are exposed to constant emotional strain due to frequent exposure to patient death and suffering (Rezaee et al., 2019). Similarly to oncology nurses, studies found that during the COVID-19 delta, palliative care nurses reported frequently about exhaustion, fatigue, and increase emotional distress (Diehl et al., 2020). Nursing as a profession is tangled between patient care responsibilities, low wages, and hard-working conditions, which are linked to additional emotional distress (Davey et al., 2019). The COVID-19 pandemic added an extra layer of unpredictable health situations and lack of confidence related to scope of practice (Wood et al., 2021).
Geriatric NPs had the highest scores on the MHC-SF, with the highest sub-score for psychological well-being. Additionally, no significant difference among the three groups was found for well-being in the MHC-SF scale. According to Eiroa-Orosa (2020), psychosocial well-being should be seen as being influenced by internal variables (sex, ethnicity, self-balance) and external variables (economy, society), which during a time of crisis can be unbalanced. Rozanski et al. (2019) stated there is no decisive factor that influences psychosocial well-being. This is because socioeconomic status as education and income influence both health and psychological well-being. Furthermore, these studies suggest that life satisfaction, meaning optimism in life, can be a safeguard against life-threatening events.
However, nearly half of the respondents (48.9%) reported having 17 or more depressive symptoms on the CES-D measure. The cutoff point for the CES-D measure is 16, with a score of 16 or higher reflecting individuals at risk for clinical depression (Radloff, 1977). Additionally, there was no significant difference in levels of depression among the three nurse practitioner groups, according to CES-D scale. Previous research by Hall (2020) and Heesakkers et al. (2021) during COVID-19 waves found high levels of anxiety, depression, and exhaustion among all nursing professional who were exposed to COVID-19 patients and particularly among nurses who worked in the intensive care units. Most nurses described fear, sleep deprivation, anxiety, and repeated stress.
One finding from the study that is not supported by the literature is the lack of statistical differences in the levels of happiness, well-being, and depression by level of average monthly income. This may be due to the unique nature of a pandemic and the fact that its effect is felt across the entire population, regardless of the income level. A moderate positive association was found between the number of years worked as a nurse practitioner and depression, and a moderate negative association was found between the number of years worked as a nurse practitioner and happiness. These associations may be due to previous feelings of stress and burnout among nurse practitioners who had been working longer that were only compounded with the COVID-19 pandemic (Ge et al., 2023).
Strengths and Limitations
Strengths
This study has a number of strengths. First, it contributes to the understanding of well-being among nurses during times of crises. This topic is of utmost importance, as nurses and other healthcare workers are on the frontline during health crises. Second, in order to collect data for the degree of resilience, happiness, and depression, validated, reliable scales that had been used in numerous previous studies were utilized. Third, the researchers were able to identify all nurse practitioners in Israel who worked in COVID-19 or allied units during the delta wave and invite them to participate in the study.
Limitations
This study has several limitations that should be considered when interpreting the results. Firstly, the sample size was relatively small and only included nurse practitioners from three specific areas of healthcare. As a result, the generalizability of the findings may be limited. It is also important to note that the nurse practitioner role is still relatively new in the Israeli healthcare system and that nurse practitioners are limited to a specific specialty, accounting for less than 1% of the overall nursing sector. Additionally, the study was conducted during the COVID-19 pandemic, and nurses and healthcare workers were overwhelmed with web-based surveys for numerous COVID-19-related studies, which may have contributed to the low number of participants.
Another limitation of the study is the use of self-reported measures to assess emotional well-being, which can be susceptible to bias and may contribute to systematic misinterpretation. Moreover, the study did not investigate other factors that could affect emotional well-being, such as intensive news and media exposure, ethical distress, and separation from families.
Lastly, this study is the first to investigate well-being among Israeli nurse practitioners, and there are no previous data with which to compare. Future studies with larger sample sizes and diverse populations are needed to confirm and expand on the findings of this study. Overall, despite these limitations, this study provides important insights into the emotional well-being of Israeli nurse practitioners in specific healthcare areas during the COVID-19 pandemic.
Implications for Practice
Preserving well-being for healthcare workers, especially during times of health crises is of utmost importance, in order to maintain a healthcare workforce that can cope with a crisis. Advanced nursing education must ensure that nurses are equipped with the necessary personal resources needed to handle challenges while providing care, and healthcare settings management should provide resources, such as enabling a healthy work–life balance, providing counseling after a crises has been managed, and offering continuing medical education that also addresses coping strategies during medical and nursing challenges. Furthermore, previous research has highlighted a significant discrepancy between the theoretical knowledge and practical skills acquired by Israeli NPs during their training and their actual implementation in the field (Haron et al., 2019; Romem et al., 2023). This discrepancy can result in frustration, disappointment, decreased professional well-being, and heightened depression scores among these healthcare professionals.
Conclusions
This study is the first to explore the well-being of Israeli nurse practitioners during the delta wave of the COVID-19 pandemic. The findings indicate that the nurse practitioners reported good emotional well-being during the delta wave of the pandemic, despite the global crisis and unpredictable circumstances. The extensive and broad training that Israeli nurse practitioners receive equips them to deal with complex and uncertain situations such as those encountered during the COVID-19 pandemic. As well-being is defined as the equilibrium of resources to cope with challenges faced, this training is likely a significant factor that helped them maintain a state of well-being. To further enhance the well-being of nurse practitioners and prevent burnout, health promotion strategies such as providing more information on crisis management, promoting self-care during stressful events, and encouraging regular supportive activities like mindfulness or physical training can be helpful.
Future studies could expand the sample size to include a wider range of healthcare professionals and investigate differences in psychological well-being and depression between different types of healthcare professionals. This would allow for a more comprehensive understanding of the emotional health of healthcare professionals during times of crisis, which could inform targeted interventions to support their well-being.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.