
Abstract
Background
The care of a child receiving chemotherapy has a significant impact on the parents and family structure, which has been explored in depth in a few studies in Saudi Arabia. The purpose of this study is to further explore the lived experiences of Saudi Arabian parents in caring for their children receiving chemotherapy.
Methodology
A qualitative descriptive design was used in this study with a sample of 17 parents of children receiving chemotherapy. The participants were recruited using the snow-balling technique throughout the community, as well as from the University Hospital, Pediatric Oncology Department. The data were collected via in-person and virtual methods using semi-structured, open-ended interviews and analyzed using thematic analysis.
Results
The findings of the study were placed into two main themes: family experience and stages of disease. Family experiences include the parents and siblings’ experiences. The stages of disease include three sub-themes: the pre-diagnosis phase, diagnosis phase, and treatment phase.
Conclusion
The cancer journey had a huge impact on the parents and siblings. The study revealed important findings related to the experiences during the stages of diseases and lived experiences of parents and siblings including psychological, physiological, social, and financial impacts.
Background
Cancer is the leading cause of deaths and illnesses in the world. It is a disease that can affect any part of the body as it is characterized by uncontrolled cell growth that can invade and spread to other parts of the body (WHO, 2021). As a result, cancer is now having a significant and growing global impact. This impact can clearly be observed in the youth population. According to the World Health Organization (WHO, 2021), an estimated 400,000 children in the world develop cancer per year. Within this demographic, globally, acute lymphoblastic leukemia is the most common type of childhood cancer. It accounts for approximately 19 percent of all pediatric cancers (WHO, 2021), constituting 34.6 percent of all cases in Saudi Arabia (Ministry of Health, 2020).
There are four main types of cancer treatment that can be implemented to deal with this growing global issue: surgery, radiation therapy, stem cell transplantation, and chemotherapy (Hockenberry et al., 2018). These treatment modalities can either consist of a single type of cancer treatment (unimodal) or a combination of cancer treatments. The first type is surgery, which involves taking biopsies and removing the tumor. Second, radiotherapy is combined with chemotherapy or surgery to achieve the best results in reducing the tumor's size. Stem cells are blood-forming cells obtained via transplant from a family member or volunteer (allogeneic) or the patient (autologous) to produce functional blood cells (Hockenberry et al., 2018). Among these treatments, chemotherapy is usually the first line of cancer treatment (Hockenberry et al., 2018).
Chemotherapy, as the literature shows (Sous et al., 2021), causes painful side effects on the skin, nails, and mucosa by quickly dividing tissue. A cross-sectional study revealed that 73.4 percent of pediatric patients reported dry mouth and 61.8 percent a change in taste as side effects of chemotherapy (García-Chías et al., 2019). In addition, a separate study on pediatric chemotherapy found that 52 percent reported fatigue, 43.7 percent mentioned lost appetite, and 42.3 percent had pain (Torres et al., 2019). Even though chemotherapy is highly efficient in the treatment of cancer, it has several significant side effects that can impact the child's health. Chemotherapy does not only have a severely detrimental effect on the physical health of individuals but also places strain on the family units.
Because childhood cancer treatment can last several years, it can have a significant impact on the siblings and family structure. Research has confirmed (Erker et al., 2018; Kahriman et al., 2020), the impact of having a child receiving chemotherapy on the parents and siblings, which may lead to consequences such as increased depression and a decrease in the siblings’ daily activities (Erker et al., 2018; Kahriman et al., 2020). Additionally, many studies have investigated the effects of a child's chemotherapy on parents, showing they face physical, psychological, social, and financial consequences (Al Qadire et al., 2020; Carlsson et al., 2019; Sercekus et al., 2014).
The treatment journey of a child with cancer includes several challenging stages including diagnoses, treatment, and relapse periods. Providing care at home to the children receiving chemotherapy can strain a family’s financial resources (Al Qadire et al., 2020). When dealing with these challenges, many families tend to hide their emotions to prevent the cancer patient from feeling overwhelmed because of their inability to deal with the patient's expressions. This leads to preventing discussion with the child and causing stress to build instead (Sercekus et al., 2014). Furthermore, most caregivers (usually parents) need to be in the hospital with the hospitalized child during the chemotherapy treatment, which means that parents may be unable to provide adequate care for other healthy siblings. As can be seen, the effects of chemotherapy often extend beyond the patient to the family unit.
Literature Review
An electronic literature search was conducted in different databases including Ebsco, MIDLINE, OVIDSP, PubMed, and CINAHL. Searching strategy was employed with the keywords (“chemotherapy” AND “pediatric” AND “cancer” AND “parents”), and the search was limited to English articles published between 2016 and 2023. Twenty studies were deemed relevant based on their titles and abstracts. Following evaluation, nine articles were included while eleven were excluded for the following reasons: patients over the age of 18; reported patients received a treatment other than chemotherapy; and samples included children with multiple chronic illnesses.
This literature review presents the psychological, physiological, sociological, and financial challenges facing parents, caregivers, and siblings of a child undergoing chemotherapy. The disease and treatment journey can also greatly impact the marital relationship.
Having a child with cancer is a highly difficult experience for a family. The parents suffered emotional distress and fear of health deterioration of their child's health. A cross-sectional study of 192 biological parents in the United States found that parents are most anxious while waiting for a diagnosis and when the child begins chemotherapy (Wiener et al., 2017). A qualitative study (Hassankhani et al., 2019), in Iran of 21 caregivers for cancer patients found that stress can cause stomach and joint pain, insomnia, appetite changes, and weakened immunity. Another quantitative study of 62 parents exploring the association between socioeconomic and psychological experiences found similar results with most participants reporting depression, anxiety, and sleep deprivation (Okumu et al., 2017).
Marital relationships can also be adversely affected by the care of a child receiving chemotherapy. A cross-sectional study with 192 parents exploring the effect of having a child with cancer on the parents’ relationships (Wiener et al., 2017), revealed that parents felt less emotionally connected at the start of treatment and when they were separated for a long time during treatment (Wiener et al., 2017). This happened because both were dealing with stressful events, including changing roles and increased responsibilities (Wiener et al., 2017). However, a systematic review of couples functioning after a pediatric cancer diagnosis emphasized the importance of emotional closeness, marital support, satisfaction, and overall adjustment in successful adaptation (Van Schoors et al., 2017). A descriptive study conducted in Turkey with 65 families evaluated the changes that the parents experienced during care (Kahriman et al., 2020). It confirmed that supporting the parents is important to help them cope with their child's cancer experience (Kahriman et al., 2020).
Most caregivers of children undergoing chemotherapy face social and financial challenges due to their children's conditions. Cancer negatively impacts family function and well-being, including restrictions on social life and daily activities. For instance, family members may experience social isolation, family activities may be difficult to coordinate, and family members may begin to think about nothing but the illness and stay away from social activities (Kahriman et al., 2020). In addition, a parent may have to leave work to care for a sick child. This condition may lead to financial difficulties and deterioration of family connections.
A qualitative descriptive study in Turkey evaluated how the lives of families of children with cancer changed (Kahriman et al., 2020). The effects on siblings appeared in multiple aspects: physical, psychological, and social (Kahriman et al., 2020). Mothers stated that they did not feed their healthy children with their favorite meals as they used to, and the siblings became more apprehensive, unhappy, and angry and felt emotionally abandoned. They felt jealous because of the increasing parental concern for the child with cancer. The siblings also experienced social isolation and limitations on family activities resulting from increased time spent on hospitalization by parents to care for their child with cancer (Kahriman et al., 2020).
Parents adapt to their children’s illnesses in a variety of ways. The literature has mentioned some aspects of family coping with having a child with cancer. Parents frequently seek information about the illness and its treatment. Some parents get reassurance from family and friends. Socializing with other parents who experienced the same situation can help them emotionally, socially, and spiritually (Walubita et al., 2018). A parent may also turn to religion as a coping mechanism. They pray to God for help and for their child’s recovery (Walubita et al., 2018).
The effort necessary from parents when their child receives chemotherapy is intense and affects their roles as parents. However, there is a lack of literature examining the impact of the disease and treatment journey on the parents and siblings, siblings’ needs, family separation, and living arrangements during the hospitalization of the child receiving chemotherapy. There have been a few studies in Saudi Arabia that explore in depth the experiences of parents with children receiving chemotherapy. The purpose of this study is to further explore the experience of Saudi Arabian parents in caring for children receiving chemotherapy.
Methodology
Research Design
A qualitative, descriptive design has been used to explore the experience of parents in caring for children receiving chemotherapy.
Study Setting
This research study was conducted in the Kingdom of Saudi Arabia (KSA). The participants were recruited through a flyer posted on social media (WhatsApp and Twitter), as well as from King Abdulaziz University Hospital, where there is a pediatric oncology unit.
Sample
A convenience sampling technique was used to recruit the participants. The sample of this research included parents of children receiving chemotherapy. The participants were recruited through the snow-balling sampling technique.
Inclusion criteria were the following: (a) the participants were parents (mother or father) or direct caregivers of the child; (b) the child was receiving chemotherapy for treatment of any kind of cancer; (c) the child was below 18 years old; and (d) the child was receiving chemotherapy sessions or completed the sessions no more than 6 months ago. The exclusion criteria were children diagnosed with other acute or chronic health conditions that required other treatment regimens other than chemotherapy.
Considering the inclusion criteria, 31 participants were invited to participate in this study. The recruitments and interviews continued till data saturation reached when no new information was added. The total sample size included in this study was 17 participants.
Instrumentation
Open-ended, semi-structured interviews were used. The questions in the interview were developed by reviewing the pertinent literature. An individual interview was conducted in person or virtually through Zoom, an online meeting application.
Data Collection Procedure
The researchers conducted in-depth semi-structured interviews either in-person or virtually using Zoom. The first and second authors were involved in all the interviews as they have previous experiences in qualitative research. The interviews lasted approximately 60 min. The interviews were recorded. The scheduled meetings through Zoom were secured with a password, and confidentiality was maintained throughout the closed meeting.
Data Analysis
The data were analyzed using thematic analysis. The data collection and data analysis were performed simultaneously. The investigators specifically analyzed the data to uncover common themes/subjects, concepts, and patterns of meaning (Polite & Beck, 2017).
In the first step of the thematic analysis, the audio was transcribed to text. The text was coded and paraphrased to abbreviated labels. Second, possible themes and sub-themes were created by merging multiple codes into a particular theme, and then the themes were reviewed by the researchers to ensure that the data were both relevant and accurate. The third step included identifying final themes and sub-themes (Polite & Beck, 2017).
Ethical Considerations
Ethical approval was obtained from King Abdulaziz University, the Faculty of Nursing (NREC Serial No: Ref No. 2B.13) prior to conducting this study. Additionally, ethical approval was obtained from the University Hospital (Reference No HA-02-J-008) before contacting the participants. Participation was completely voluntary. Informed consent was obtained from the participants upon the agreement to participate in the study and prior to the interview. Confidentiality was maintained throughout the research process. Personal data collected from the questions were kept private, by using the codes given to each participant. Furthermore, data were kept private and only the study team and supervisors could access it.
Results
Demographic Information
A total of 17 participants were included in this study. The sample involved one father (n = 1, 5.9 percent) and 16 mothers (n = 16, 94.1 percent). Six of them were from 20 to 30 years old (35.3 percent), nine 31 to 40 (n = 9, 52.9 percent), and two 41 and older (n = 2, 11.8 percent). The majority of them (n = 16, 94 percent) were married, had received a bachelor's degree (n = 9, 52.9 percent), were unemployed (n = 15, 88.2 percent) and had less than 3000SR income (n = 9, 52.9 percent) Children in the study had different types of cancer, including brain and spinal cord tumors (n = 2, 11.8 percent), leukemia (n = 9, 52.9 percent), and others. Demographic characteristics are shown in Table 1.
The main findings of the study were placed into two main themes: stages of disease and family experience (Figure 1 summarizes the study findings).
Stages of disease
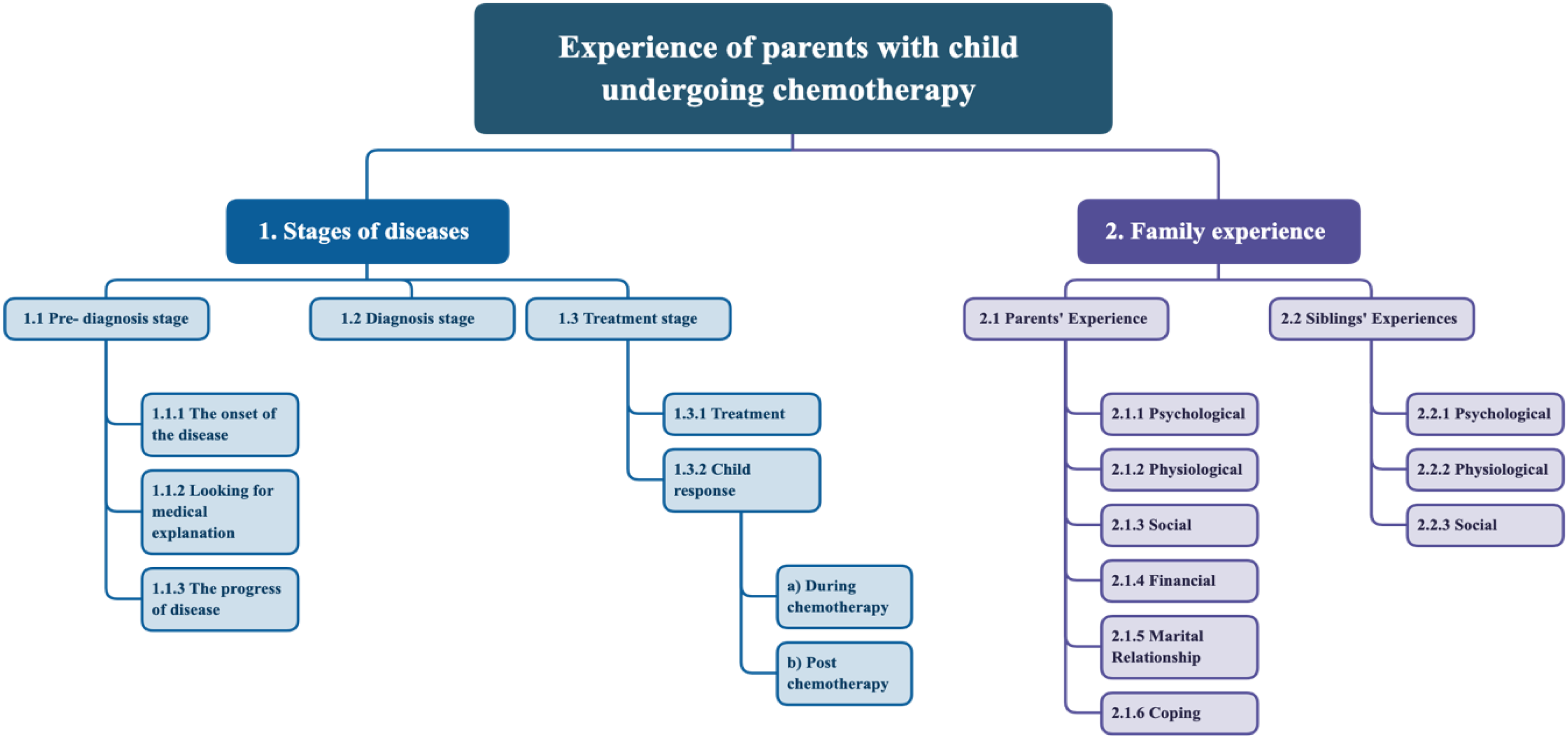
Graph illustrating the thematic analysis results.
The stages of disease include three sub-themes: pre-diagnosis phase, diagnosis phase, and the treatment phase.
1.1 Pre-diagnosis 1.1.1 Onset of the symptoms started with parents’ recognizing a problem with their child. They noticed several and sequential symptoms that suddenly happened. Symptoms included but are not limited to fever, loss of appetite, difficulty in movement, abdominal pain, and swelling. Also, unusual symptoms such as lips bleeding and a hematoma behind the ear appeared. One of the participants stated about her daughter:Suddenly something changed in her stomach, she was complaining about her stomach, she went to play, and she came again complaining about her stomach. 1.1.2 Looking for a medical explanation for these symptoms, the parents brought their child to healthcare professionals to figure out the diagnosis. A participant said,She complains about her hand so much she can’t move it . . . I wanted to know so I referred to a doctor and went to more than one doctor . . . So, they did a biopsy that took about two days, it wasn't long . . . They told us that she actually had leukemia . . . it was not shown in the lab tests before. 1.1.3 Progress of disease includes the stages of disease becoming worse and the child's health deteriorating. Five of the children included in this study experienced problems with movement such as inability to walk or stand. As one parent said, “After that, my daughter fell to the ground several times and could not walk at all, and suffered from prolonged and persistent headaches and the inability to eat or drink.” They then spoke about the disease's progress, saying, “He suffered from a headache all the time. He says my head hurts from headache.” Another said, “We entered the emergency; her health was deteriorating; she did not eat or drink.” 1.2 Diagnosis phase 1.3 Treatment stage
The pre-diagnosis stage includes the onset of the disease, looking for a medical explanation, and the progress of the disease.
Another added, “He started losing weight very quickly.” Another participant pointed out that there were unusual symptoms: “He has symptoms at home, such as this, he was lethargic, and then . . . his lips start to bleed.”
During this phase, the parents spent a long time back and forth between the hospitals to find an accurate diagnosis. There were several differential diagnoses for their children and frequent lab investigations or diagnostic procedures.
When the diagnosis was confirmed, the parents experienced denial and shock. In addition, they struggled to process the information regarding the disease and its treatment. However, one participant mentioned that their child underwent multiple tests to confirm the diagnosis, and when the diagnosis was confirmed, they felt relieved rather than anxious. The following statement was echoed by various participants, “The diagnosis felt like torture, and when we were informed that cancer had been confirmed, we felt relieved.”
Most of the participants stated that the treatment period started within an average of 1 month after the confirmed diagnosis. Some of the participants stated that it consisted of a variety of treatment options such as chemotherapy, surgical procedures, and radiation. As one of the participants said, “When the eradication stage comes, we will do an operation and remove the tumor, but we will continue on the chemo, meaning we will not stop.”
Some of the participants stated that the treatment stage was characterized by frequent hospitalization and continuity of chemotherapy, which improved the patient's condition: Four days later, we go back to taking a dose in day care, which is the light dose . . ., we go home, and then we go back to the hospital and take a dose in day care, which is taken in the morning at noon, and we go out.
Some participants stated that their children's conditions deteriorated as the disease progressed during treatment. They stated that the cancer had spread to all parts of the body. Eye blindness, seizures, disturbances in urination, sodium alteration, and dehydration were all reported by different participants as the disease progressed during the chemotherapy. The following statements by the participants illustrated the physiological changes during chemotherapy: “A disturbance in the urination hormone, and the sodium was high and sometimes it went down,” and “Now she can't see with her left eye.”
1.3.1 The child's response to chemotherapy sessions was classified into two groups: during chemotherapy sessions and post-chemotherapy sessions. (a) During the chemotherapy sessions: Most of the participants mentioned that their children displayed various symptoms during the chemotherapy sessions. These symptoms are classified into early and late chemotherapy sessions.
Early chemotherapy session: Some parents stated that their children were showing early negative symptoms during the initial doses, but the majority of the participants emphasized that their children's symptoms and moods had improved during the early chemotherapy sessions. In addition, two of the caregivers stated that their children were optimistic, and one said that their child educated himself and them about the disease and was patient during the sessions. As the participant said, “Before he was taken, he had severe symptoms, but after the chemotherapy began, glory be to God, the fever subsided, and the pain went away.”
Some of the participants stated that their children experienced pain and tiredness during early sessions in addition to having some behavioral symptoms such as fighting and resistance to the treatment. Also, one of the participants explained that her child refused the treatment and was feeling extreme fear from the injection: “A lot of tightening, he was moving in the bed and the needle moved out and blood began to fall.”
Last chemotherapy sessions: Three of the participants stated that their children showed decreasing severity and improved appetite to eat. Two of the caregivers stated that their children were requesting outside food and were not liking the hospital food. One participant mentioned the food desire of her hospitalized child as: “I want to go home. I want to go . . . I want my dad to get me food from somewhere else. I don't like this food.”
Some participants stated that their children were feeling tired and bored from hospitalization during the chemotherapy sessions. Also, the participants mentioned that their children missed home and felt homesick. Other participants mentioned that their children experienced weak immunity and bleeding, as one explained, he was “bleeding from his nose, from lips, bleeding into the urine.”
(b) Post-chemotherapy session: The majority of respondents mentioned that their child experienced post-chemotherapy symptoms, which are divided into psychological, physical, and behavioral symptoms.
Psychological symptoms: Some caregivers reported that their children were exhibiting psychological symptoms such as tiredness, unacceptance, and body image disruption. One participant said, “He was not accepting of others. He did not accept himself and beat me. He beat his brothers and my mother. I mean, his psychological state was once devastating.”
Physical symptoms: Most participants reported that their children experienced physical symptoms after receiving chemotherapy, such as fever, diarrhea, fatigue, hair loss, and appetite loss. One participant stated that her child's vision had changed as a result of chemotherapy. Two participants stated that their children's hearing had deteriorated and become weaker. One participant said, “Hearing was much weaker, much weaker, meaning with a hearing aid.”
One of the participants indicated that the pandemic had affected them negatively. Their child was infected with COVID-19 due to weakened immunity, and he suffered from vomiting blood, hyperthermia, and isolation in the hospital: “He contracted COVID after receiving chemotherapy. He was in isolation in the hospital. He was vomiting blood, and his immunity was very weak, and his temperature was high.”
Behavior symptoms: Most respondents stated that their children became more aggressive with siblings, parents, and relatives. As one of the participants mentioned, “He just beats me and beats his sibling and my mother.”
Furthermore, the caregiver mentioned that her child consistently blames her for being in the hospital and losing their hair. This participant shared what her child said to her: “You are the one who did this to me, why did you make them shave my hair, Mama, why did we go back to the hospital? I don't want the hospital.”
Social symptoms: Three of the caregivers mentioned that their children expressed missing their siblings. The following statement was echoed by the participants, “She missed her sibling.”
2. Family Experience
2.1 The Experience of Parents 2.1.1 Physiological: Participants stated experiencing sleep disturbances and an inability to sleep peacefully due to their constant worry and fear for their sick child and siblings. One of the participants revealed that they had hyperglycemia as a result of their grief. Another respondent stated that despite their loss of appetite, they forced themselves to eat in order to gain the energy necessary to care for their sick child. One of the participants said, “A lot of tension from the day she got sick until today, constant tension and fear and lack of sleep. I'm afraid for her while she is in bed.” 2.1.2 Psychological: While caring for the child, participants reported that they were experiencing feelings of sadness, prolonged fear, anxiety, and stress. They had entered a period of uncertainty in terms of making decisions about the child's treatment. Regarding the child's condition, another participant expressed pessimism and worry about losing the child. Some participants reported crying and shouting during the initial chemotherapy session. One of the participants expressed happiness at the slightest improvement in their child's laboratory results and condition. A participant explained:It made me crazy when I knew that he would take chemotherapy the next day and after, I don’t know, I swear I felt like my soul is coming out of me, for real I felt like my heart is coming out of me, I don’t know, I talked to my siblings—that's it, take me out, I don’t want the hospital. 2.1.3 Social: Participants stated that they avoid interacting with friends and family out of concern for the child's potential exposure to infection. Because they were so busy caring for their child with cancer, their relationships with others have changed. Five participants reported feeling separated from a family member while hospitalized. Due to grief, some participants isolated themselves from their family. One of the participants stated that they would displace their emotions onto the other siblings of the sick child. One of the participants said, “Because the immunity is low and so I was afraid, we usually don't go to visits.” 2.1.4 Financial: The participants reported an increase in monthly expenses due to the need for additional supplies to care for the child. Participants reported having financial difficulties and being unemployed. The results revealed that the child's illness and prolonged hospital admissions caused some parents to lose their jobs; other participants stated that they could no longer commute to work because they are caring for their sick child. One of the participants said, “Our circumstances are a little difficult in terms of finances; my husband doesn’t have a job.” 2.1.5 The effect on marital relationships: Some participants reported that their relationship had improved since the child's diagnosis. Another participant stated that at the beginning of their cancer journey, their relationship was difficult because the wife changed and the husband became harder, but after acclimatization, their relationship returned to normal. One of the parents stated that they developed a mutual understanding while caring for their child. The parent said, “I argued with him. ‘That's it, you left us.’ He was saying, ‘The first time you told me I left you, I didn't leave you.'” 2.1.6 Ability to cope: The participants coped with the circumstances by accepting the disease and comparing their experiences to those of others. They coped spiritually by praying for the child's health to improve. One of the participants explained that because she is an optimistic person, she instilled optimism in her children, which led them to view the experience as a difficult period that would pass eventually: “I am always optimistic, and I try to adopt in my children that everything will be fine, and so on, even though it is a difficult time for me and them, and even though the entire house is affected, I am not alone, thank God.” 2.2 The Experience of Siblings 2.2.1 Physiological effects: The participants reported that the siblings of their child receiving chemotherapy suffered physical problems such as loss of appetite and fatigue: “My daughter no longer wants to eat.” 2.2.2 Psychological effects: Participants mentioned that the child's siblings experienced jealousy, fear (from sickness, hospitalization, or regarding the sick child), crying, depression, worry about re-admission, sadness for their sick sister or brother, and tiredness due to separation. One participant stated that her daughter competes for attention and becomes more sensitive when her father treated her brother differently. Some children were separated from their siblings, which had a psychological influence on them, causing sadness, blaming of the mother, secrecy, and signs of regression. 2.2.3 Social effects: Most of the participants stated that the siblings of their child receiving chemotherapy suffered from isolation (refusing to leave the house) and feelings of separation or family disintegration and a need for parents or the sibling who has cancer. According to their statements, because some participants failed to adequately care for their children due to the burden associated with providing care, their other children had to drop out or postpone school: “My daughter's studies were affected a lot as she was late for her semester.”
Parents’ experiences were divided into six subcategories: physiological, psychological, social, financial, effect on marital relationship, and ability to cope.
The results indicated that most of the participants were not affected by the COVID-19 pandemic, but they became afraid for their child with cancer due to weak immunity. Some of the participants indicated that the pandemic affected them positively, that the family became closer with each other than before: “Frankly, we benefited from these days because we returned home, and the family gathered more.”
The effects on siblings were placed into three categories: physiological, psychological, and social.
In some cases, the patient's siblings wanted to sleep with the mother more and be more attached to her. One participant reported that her child (the sibling) experienced nocturnal enuresis, was nervous, and was aggressive: “Their psychology was affected to the point that my son suffers from bed wetting.”
Most of the participants indicated that their healthy children (the siblings) stayed with their father at home. Three of the participants indicated that their children stayed in another city. Furthermore, some of them said that their children stayed with the family of the father. One indicated that their two daughters stayed with neighbors. Finally, one participant said her children stayed at home alone: “I am in the hospital and their father is at work, and they are alone at home.”
Discussion
This qualitative study explored the experiences of caregivers in caring for children receiving chemotherapy and its impact on the children's siblings. Two main themes resulted from this research: disease stages and family experience. To determine the cause of their child's symptoms, the parents underwent an attempt at diagnosis; during this procedure, they expressed stress and anxiety (Pedersen et al., 2020). Furthermore, the family experienced a variety of physical and mental difficulties due to the side effects of chemotherapy, hospitalization, and the drastic changing of their lives (Carlsson et al., 2019; Hassankhani et al., 2019; Torres et al., 2019). Similarly, a study in Iran with 21 caregivers found that most parents experienced emotional stress (Hassankhani et al., 2019).
The findings from this study regarding pre-diagnosis and diagnosis phases were similar to those of related studies (Faruqui et al., 2019; Pedersen et al., 2020), in which the children reported general and worsening symptoms such as flu-like symptoms, difficulty in movement, loss of appetite, and severe non-specific symptoms such as bleeding. These symptoms place parents in difficult situations, and they are persistent in obtaining the diagnosis (Faruqui et al., 2019; Pedersen et al., 2020). Time intervals from the onset of symptoms to the final diagnosis are influenced by a variety of visits to healthcare professionals, receiving differential diagnoses, and frequent investigations (Faruqui et al., 2019; Pedersen et al., 2020). At the time of receiving a confirmed cancer diagnosis, parents in this study experienced denial, shock, confusion, or a sense of relief consistent with findings from other studies (Faruqui et al., 2019). These findings emphasize the importance of early detection of cancer symptoms to improve prognosis and reduce the burden on parents (Faruqui et al., 2019).
Most oncology patients recover eventually as a result of the various cancer treatments. The children's moods and symptoms improved after treatment; they were more optimistic, patient, and knowledgeable about the disease. Family support played a significant role in patients’ coping. In the study, the most common symptoms after chemotherapy were physiological side effects, homesickness, and hospital boredom. Consistent with findings from previous studies, it was documented that immediately after receiving chemotherapy, most pediatric children had irritability, weariness, pain, hair loss, and a lack of appetite (Al Qadire et al., 2020; Obaid, 2015; Torres et al., 2019). The patient was under stress and pain due to physical changes in their appearance and mood. This study found that most children who underwent chemotherapy became aggressive and developed behavioral issues. Chemotherapy enrages children, who blame their parents for being in the hospital. As a result, it is recommended that a psychologist follow up on the psychological state of a child and assist him or her in overcoming the ordeal.
The constant worry and fear for their child's life, as well as their responsibility to their other children, cause physical, mental, and social issues for parents in this study. Similarly, Sercekus et al., 2014 discovered that parents experience decreased appetite, insomnia, and fatigue. During chemotherapy, caregivers feel upset and avoid socializing for fear of infecting their child. Another study with a sample of 15 caregivers had a similar result, stating that prayer was the most prevalent cultural coping mechanism (Walubita et al., 2018). The parents in this study were struggling financially; despite the government's free treatment, their income was inadequate to care for their child at home. Similarly, research from Jordan with a sample of 264 parents found that 79.2 percent of the participants had financial problems (Al Qadire et al., 2020). Consistent with the findings from this study, research indicated that parents’ relationships are stronger during and before a cancer diagnosis (Wiener et al., 2017). Therefore, healthcare providers should counsel caregivers by actively listening to their concerns and encouraging them to verbalize their burdens.
According to the study, siblings may be worried about the sick child or become jealous. Furthermore, healthy siblings who are left with neighbors, friends, or other family during hospitalization may feel anger and insecurity. Parents may neglect the needs of their healthy children because their sick child consumes most of their time and energy. This situation has been connected to school troubles, enuresis, unhappiness, and antisocial tendencies in healthy children. The literature has consistently revealed that siblings of children receiving chemotherapy experienced despair, anger, anxiety, guilt, social isolation, and limited family activities as the unhappiest and most emotionally neglected family members (Kahriman et al., 2020) It is important to enhance the social support of siblings from parents and relatives to strengthen family relationships.
In this study, parents expressed concerns that their child may be infected with COVID-19. Families have consequently become more socially isolated and concerned about their children's weak immune systems. In accordance with the literature (Darlington et al., 2021), they have lost contact with their support network despite the availability of technology to facilitate communication.
Strengths and Limitations
The research sample was diverse because it included parents from a variety of cities and cultural backgrounds; however, the sample size was relatively small, which may limit the findings’ applicability to a wider population. Furthermore, the participants’ experiences may vary according to the type of cancer and age of the child as well as their individual disease prognosis.
Implications for Practice
The results of this study could contribute to improving the understanding of the parents’ experiences. Healthcare providers may use these findings to build a trusting relationship with the family to improve the quality of the family's experience and provide holistic care to the whole family. The future research may use the findings of this study and build upon to expand the understanding of the parents experience specific to different types of cancer.
Conclusion
The findings of this study revealed the psychological, physiological, social, and financial effects on the family and siblings. It is recommended that healthcare providers provide support and resources for the family throughout the stages of the disease. Furthermore, findings from this study lay the foundation for interventions that may support parents of children receiving chemotherapy.
Ethical Considerations
Ethical approval was obtained from the Faculty of Nursing, King Abdulaziz University (NREC Serial No: Ref No 2B.13) prior to conducting this study. Additionally, ethical approval was obtained from King Abdulaziz University Hospital (Reference No153-22) before contacting the participants. Participation was completely voluntary. Informed consent was obtained from the participants upon the agreement to participate in the study and prior to the interview. Confidentiality was maintained throughout the research process.
Demographic Characteristics of the Participants (N = 17).

Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.