
Abstract
Introduction
Hospitals are required to implement patients safety incident (PSI) reporting, analysis, and problem-solving. Self-assessment is important for exploring gaps and strengthening PSI reporting and learning system.
Objectives
This study examined PSI reporting and learning systems through self-assessment based on WHO guidance, analysis of section scores by hospital class, and analysis of section relationships.
Method
This cross-sectional study was conducted on 193 health workers from 47 Indonesian non-profit private hospitals selected using non-probability sampling. Samples in each hospital consisted of seven hospital staff, including quality and patients’ safety committee, infectious diseases control committee, manager/head of nursing, as well as functional staff comprising doctors, nurses, pharmacists, and nutritionists. Six aspects based on WHO guidance were measured in this study namely 1) environment for reporting, 2) reporting rules and content, 3) analysis and investigation, 4) governance, 5) action and learning, as well as 6) patients’ and family engagement. The data obtained were analyzed using univariate and bivariate analysis.
Results
The results showed that the total average score was 64.7 ± 3.3, and the average score on all components of PSI reporting and learning system was minimum 59.3 and maximum 69.6 of a total score of 100. The lowest average score was found in patients’ and family engagement component at 59.3 ± 8.4. Class B hospitals had higher average scores on each component than class C and D hospitals, except on the action and learning and patients’ and family engagement section. There was a significant positive linear correlation between each section of PSI reporting and learning system (p-value < 0.01).
Conclusion
The PSI reporting and learning system in hospitals is in need of improvement across all aspects. One specific area that requires attention is the implementation of mechanisms for patient and family engagement, which can play an important role in promoting safety programs.
Background
Patients’ safety is a priority for health services because it could lead to serious public health problems (Card, 2014). However, endeavors in this situation have yielded mixed results in the reduction of preventable harms, errors, and adverse events (Lark et al., 2018). Patients Safety Incident (PSI) reporting is an effective strategy used to enhance patients’ safety and quality improvement in healthcare (Fukami et al., 2020). According to previous studies, insights into patients’ safety are affected by volume of data overload, poor specification report requirements, overinterpretation of incident analyses, selectivity and incompleteness of data, taxonomies and classifications that do not facilitate the identification of system weaknesses, as well as lack of investment in analysis compared to reporting
Furthermore, patients’ safety is still a priority issue for healthcare systems in both high and low resources countries (Kang et al., 2021).
Review of Literature
Based on previous literature, under-reporting of PSI is evident in Indonesia (Dhamanti, Leggat & Barraclough, 2019), and according to the data from the Indonesian Patients’ Safety Committee, PSI reporting at the national level is very low. In 2019, only 334 from a total of 2877 hospitals, or 12% reported PSI to the national level (Daud, 2020). The under-reporting is caused by hospital-related factors such as lack of understanding, knowledge, and responsibility for reporting, lack of leadership and institutional culture, as well as the perception of reporting as an additional burden. Meanwhile, non-hospital related factors include lack of feedback and training, lack of confidentiality mechanisms in the system, absence of policy safeguards to prevent any punitive measures against the reporting hospital, and lack of leadership (Dhamanti et al., 2022). There is a pressing need for the Indonesian Government to improve the system, by making specific regulations and creating a robust infrastructure at all levels to support incident reporting (Dhamanti, Leggat, Barraclough, et al., 2019).
In terms of regulation, Indonesian Ministry of Health in 2017 mentioned that reporting is performed by the unit to the leader who also conducts grading. When the grading is blue/green, the unit leader carries out a simple investigation and recommendation. However, when the grading is red/yellow, further analysis and investigation are conducted with the root cause analysis by the hospital patient safety team. Incident criteria are divided into four categories namely potential injury conditions, near-miss events, non-injury events, and unexpected/sentinel events which might lead to death or severe/permanent injury (Ministry of Health of Indonesia, 2017).
WHO launched the self-assessment guideline for PSI reporting and learning system. This aims to provide a way for healthcare organizations, health systems, clinical departments and teams to undertake a broad assessment of patients’ safety to explore gaps and further develop the system. This self-assessment contained six sections, namely 1) environment for reporting including culture in which reports are promoted and valued, while staff are also praised for participating, 2) reporting rules and content regarding criteria of incident, 3) analysis process of incident and further investigation, 4) governance or management of the reporting system and the use of technology for support, 5) analysis for action and learning from the incident, 6) patients’ and family support as well as their engagement for learning (World Health Organization, 2020). The use of self-assessment to study patients’ safety is still rare, specifically in private hospitals in Indonesia. Therefore, this study aims to explore PSI reporting and learning system through self-assessment in non-profit private hospitals in Indonesia, compare the score of each section of PSI reporting and learning system based on hospital class and analysis of the relationship between sections in the PSI reporting and learning system.
Methods
Study Design and Setting
This quantitative study was conducted at a non-profit private hospital affiliated with a socio-religious organization called Muhammadiyah that manages 199 hospitals spread in Indonesia (Samsudin & Prabowo, 2022). To select the participants, a letter was sent to hospital management and 47 hospitals participated in the survey. The hospitals were located in Java Island, namely Central Java, East Java, DI Yogyakarta, DKI Jakarta, Lampung, and West Java. The hospitals come from various classes of hospitals. In the Indonesian hospital context, hospital classes D, C, and B have a minimum of 50 beds, 100 beds, and 200 beds, respectively. Moreover, according to previous regulation, hospital categorization was also based on several aspects such as availability of specialist services, equipment, human resources, and infrastructures or buildings. Hospitals class B have more complete services and facilities than class C and D hospitals.
Population and Sample
This study measured the learning and reporting system of PSI through self-assessment by seven staff in the Muhammadiyah-'Aisyiyah hospital. These include the Infection control and prevention unit management staff, patients’ safety and quality unit management staff, nursing manager, as well as functional medical doctor, nurses, and pharmacist/nutritionist. This cross-sectional study was conducted on 193 health workers from 47 Indonesian non-profit hospitals.
The samples were selected using a voluntary non-probability sampling method where seven aforementioned staff who volunteer to participate in the study were recruited in this study (Setia, 2016).
Research Instrument
The instrument used was created based on WHO PSI reporting and learning system namely Technical report and Guidance (World Health Organization, 2020). It was designed as a tool for exploration and discussion to identify gaps, support, and further develop systems. In addition, this tool can be used by health care services with or without an existing system in place (World Health Organization, 2020). There are six aspects measured in this study with 7, 11, 13, 5, 2 and 6 questions respectively. These include 1) environment for reporting, 2) reporting rules and content, 3) analysis and investigation, 4) governance, 5) action and learning, 6) patients’ and family engagement. There were also 5 Likert scale answers to each question from strongly disagree to strongly agree. Furthermore, the measurement instrument measured the socio-demographic characteristics of the respondents covering age, gender, educational background, position, and the hospitals where they worked. The pre-test measurement had been done on 30 health workers in hospitals before the study was performed. A reliability test showed a Cronbach alpha value of 0.924, indicating that the instrument is reliable and has internal consistency (Taber, 2018).
Data Collection and Ethical Consideration
Data were collected through an online method and the invitation to participate in this study was sent through an e-mail to the hospital e-mail and WhatsApp group of patients’ safety and quality improvement unit forum. There was neither forced consent nor sanctions against the respondents who declined to participate during the data collection. Phone credit or electronic money within the amount of IDR 20,000/USD 1.32 was given to appreciate the respondents’ participation. Besides, anonymity and confidentiality were maintained in the study process. Ethical clearance was obtained before data collection from the Ethics Committee of the Universitas Muhammadiyah Prof. Dr. Hamka, Indonesia, with number 03/22.06/01781.
Data Analysis
Data analysis was carried out using Microsoft Excel and the results were presented descriptively by displaying the quantity as well as the percentage of respondents’ socio-demographic characteristics and the average score on the six components measured. In each section, the minimum score was 0 and the maximum was 100. Moreover, the Kruskal-Wallis test was employed in order to examine the difference in each section's score based on hospital class using statistical analysis software. Spearman rank correlation also has been performed to analysis relationship between section of PSI reporting and learning system. An association with p < 0.05 was considered significant. Correlation score: 0.30 to 0.50 shows low correlation, 0.50 to 0.70 shows moderate correlation, 0.70 to 0.90 shows high correlation and 0.90 to 1.00 shows very high correlation (Mukaka, 2012).
Results
Respondents and Hospitals Characteristics
The majority of respondents were aged less than 40 years (n = 112, 58.0%) with an average age of 37.9 years, a minimum of 24.0 years, and a maximum of 55.0 years. Moreover, they were mostly females (n = 152, 78.8%) and worked as nurses (n = 86, 44.6%). The respondents came from the infection control and prevention unit, patients’ safety and quality unit, nursing manager and functional medical doctor, pharmacist, nutritionist and nurses. In addition, some respondents came from non-Java Island such as Lampung, South Kalimantan, and South Sumatra. The hospitals represented different types including general and specialist, such as mother and child, as well as mental hospitals. The majority of respondents were from class C hospitals (n = 105, 54.4%), as shown in Table 1.
Respondents’ Characteristics.
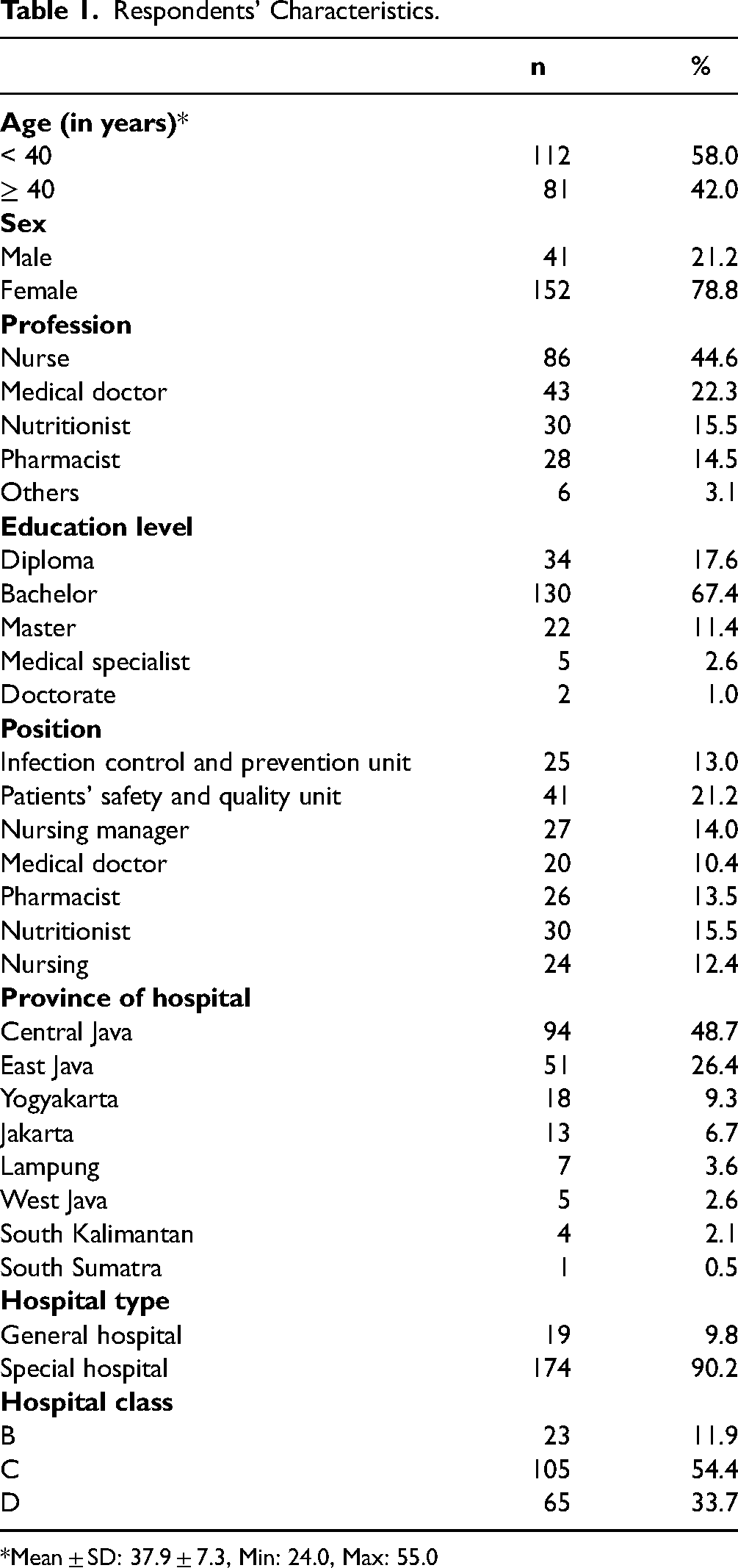
*Mean ± SD: 37.9 ± 7.3, Min: 24.0, Max: 55.0
PSI Reporting and Learning System Scores Each Section and its Difference Based on Hospital Class
Table 2 shows PSI reporting and learning system component WHO scores which are grouped by the hospital class. The lowest component was found in patients’ and family engagement component of 59.3 ± 8.4, followed by analysis and investigation of 64.1 ± 9.5. While the highest section of the PSI reporting and learning system is action and learning section (69.6 ± 15.1). Additionally, class B hospitals have higher scores on each component than class C and D, except on the action and learning and patients’ and family engagement section.
Difference of Patient Safety Incident Reporting and Learning System Score According to WHO Based on Hospital Class.
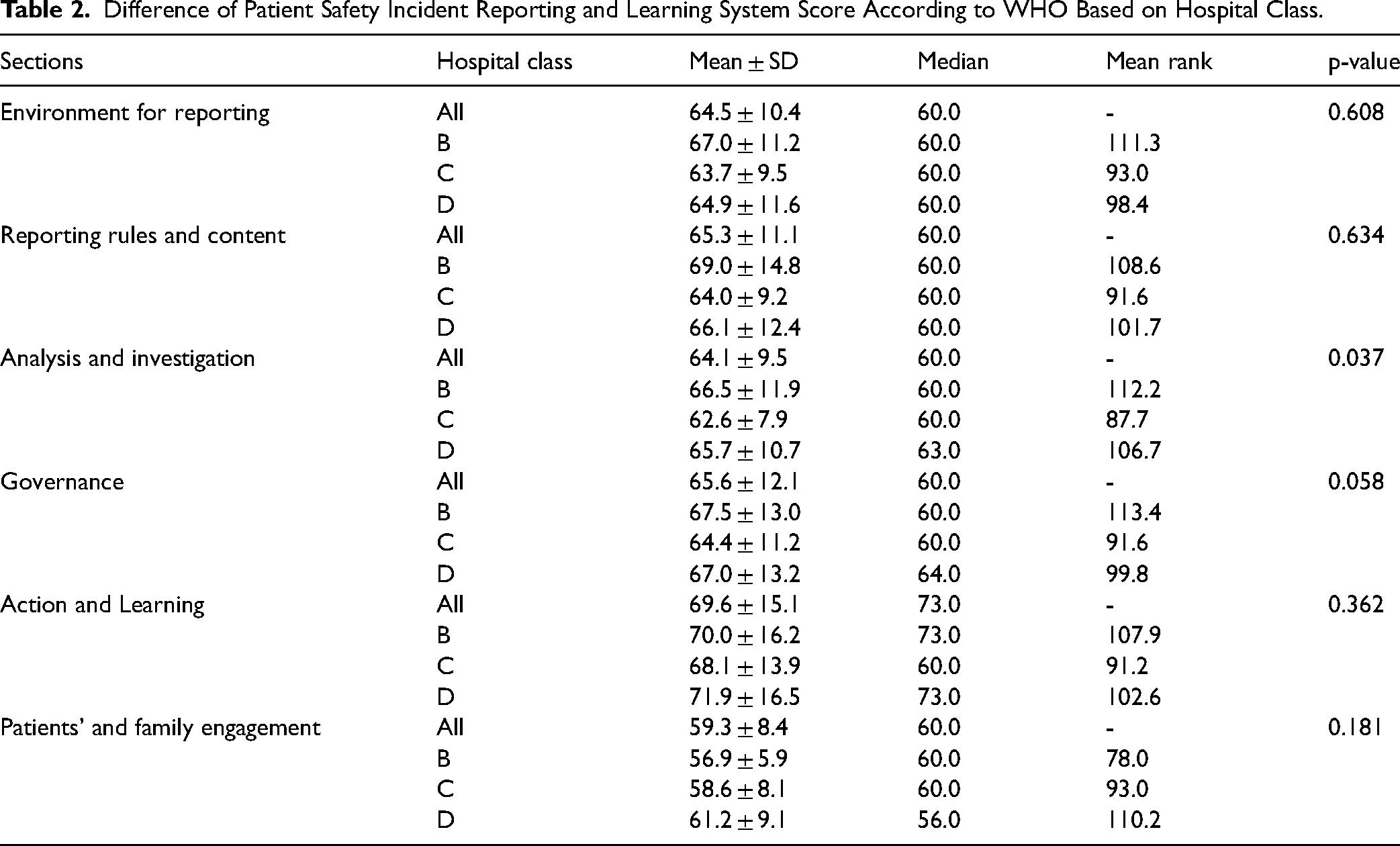
Upon a deeper examination of the scores per item in each section, it is discovered that certain items still have lower scores. Some of these items are the mechanism for patients and family to make PSI reporting (2.9 ± 0.7), the regular public disclosure of aggregated data with appropriate interpretative commentary (2.8 ± 0.7), incidents always being disclosed to victims of harm and their families (2.7 ± 0.7), patients and family who have suffered harm being involved in designing action to reduce the likelihood of a recurrence (if they so wish) (2.9 ± 0.7), and patients and family who have suffered harm playing a major role in education and training of students and healthcare staff (2.8 ± 0.7) (Appendix 1).
In terms of mean rank score, the results showed that hospital class B had a higher score than class C and D on all sections except the patients’ and family engagement section. However, there was no significant difference in the scores of each section between hospitals except for the analysis and investigation sections (p-value: 0.037) (Table 2).
Correlation Between Each Section of PSI Reporting and Learning System
Spearman rank correlation showed significant positive linear correlations between each section of PSI reporting and learning system (Table 3). The results of the study show that there is a significant strong positive correlation between the reporting rules content section and the investigative analysis section (r: 0.720, p-value < 0.01). The study also shows that most of the correlation between sections is moderate.
Correlation of Each Section of PSI Reporting and Learning System.

**Correlation is significant at the 0.01 level (2-tailed)
Discussion
Based on the results, the average score in the PSI reporting component and learning system is 64.7 (of a total of 100), with a minimum and maximum scores of 59.3 and 69.6, respectively. Moreover, the patient and family engagement aspect have the lowest score compared to the other sections. A previous study conducted in Indonesia showed that barriers such as low health literacy led to patients’ unwillingness to participate in patients’ safety program (Listiowati et al., 2023). This is because patients felt they did not have knowledge related to the care. Besides, health workers were also unwilling to involve patients in the program (Listiowati et al., 2023). A study carried out in Iran found several barriers related to patients, healthcare providers, as well as health system in patients’ and family engagement during patients’ safety program (Sarkhosh et al., 2022).
The item with the lowest score in patients’ and family engagement section is “incidents are always disclosed to victims of harm and their families”. A previous study conducted in Korea showed that disclosure of PSI was not common (Kim & Lee, 2021). It is often difficult for medical staff to perform DPSI in actual clinical practice (Ock et al., 2016; Pyo et al., 2020). This is due to several issues such as fear of loss of relationship with patients, loss of reputation or damage to career progression, and lack of institutional support to challenges in disclosing PSI (Kim & Lee, 2020; O’Connor et al., 2010). Disclosure practice can be improved by strengthening policy and supporting healthcare professionals in disclosing adverse events. Increased openness and honesty following adverse events will improve provider–patient relationships (O’Connor et al., 2010). Moreover, at an organizational level, patients and family should be engaged in the design or development of patient-centred processes and systems, for example as members of advisory committees (Frampton et al., 2009).
Another item with a very low score is the existence of a mechanism for patients and family to make PSI reporting. Regarding this matter, the policy issued by Indonesian Ministry of Health in 2017 did not emphasize PSI reporting mechanism that can be conducted by patients (Ministry of Health of Indonesia, 2017). Although physicians have the advantage of medical knowledge, nonphysician patients and family members have also alerted physicians and nurses to various potential sentinel events (Roberg, 2001). Several challenges such as fear of reprisal, lack of knowledge, and blind faith could lead to the unwillingness to engage in patients’ safety (Chegini et al., 2021). The item “involvement of patients and family who have suffered harm in designing action to reduce the likelihood of a recurrence” also had a very low score. Additionally, patients’ reluctance to participate in safety programs due to their cultural condition can be a significant barrier (Listiowati et al., 2023). A study conducted in Iran showed that factors such as low levels of health literacy, ineffective education, unwillingness, and culture can be a significant barrier to patient engagement in the delivery of safer care (Chegini et al., 2020).
This study found that the PSI reporting and learning system sections have a significant positive correlation. This indicates that systemic improvement efforts are required to enhance the PSI reporting and learning system's performance. In this context, increasing the involvement of patients and patient families can be accomplished by creating a positive environment to good reporting, specifically by establishing a mechanism for patients and families to report patient safety incidents. Moreover, a previous study showed that there is a relationship between patient and family engagement and analysis and investigation process of the incident (Kok et al., 2018).
Strengths and Limitations
This study only involved participants from one group of non-profit private hospitals, hence, the results cannot be generalized to depict all types of hospitals in Indonesia. The present study involved 47 hospitals. We expected 7 respondents from each hospital to do self-assessment. However, only 18 out of 47 hospitals could participate as expected. We only received 3 to 6 respondents from the remaining 29 hospitals. Nevertheless, we consider the respondents’ assessments involved in the present study have reflected the present situation of the hospital's patient safety incident reporting and learning system. Moreover, this is the first study in the Indonesian context that examined PSI reporting and learning system in line with WHO patient safety incident reporting and learning systems self-assessment guidance. Therefore, further studies are needed to evaluate the incident reporting and learning system in other types of hospitals in Indonesia such as government hospital. Exploration related to patients’ and family engagement in safety program particularly in Indonesia should be conducted to explore deeper the challenges and possible strategies.
Implications for Practice
This study found that patients’ and family engagement in PSI reporting and learning system is still lacking, and some practices should be performed on practical, organizational, and broad policy levels. Several possible practices include educating patients on their important role in maintaining safety, establishing patient-centered care, and building a strong policy to enable a mechanism for engaging patients and their family in PSI reporting and learning system (Bombard et al., 2018). Moreover, there is a need to improve patients’ safety culture through the transformational leadership of hospital leaders and the awareness of doctors, nurses, and other healthcare workers (Rachmawati, 2011). Regular monitoring is significant step in order to maintain the good performance for patient safety incident reporting (El-Sayed Aly et al., 2022).
Conclusion
All aspects of PSI reporting and learning system are yet to reach optimal values, with patients’ and family engagement having the lowest score among others. Several improvements can be made, such as creating mechanisms as well as implementing patients’ and family incident reporting, increasing transparency in disclosing PSI, and involving patients with family in designing actions to improve safety. Furthermore, patients should be educated, specifically regarding the importance of their role in safety program to improve awareness and engagement (Bombard et al., 2018).
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical clearance was obtained before data collection from the Ethics Committee of the Universitas Muhammadiyah Prof. Dr. Hamka, Indonesia, with number 03/22.06/01781.
Funding
This study was funded by Universitas Muhammadiyah Prof. Dr. Hamka with grant number: 380/F.03.07/2021.
Universitas Muhammadiyah Prof. Dr. Hamka, (grant number 03/22.06/01781).
{kind=link}
{kind=link}